Embed Size (px)
Citation preview

Intra-aortic Balloon Pump Counterpulsation
and Mechanical Circulatory Support

•
• Arrow Intra-Aortic Balloon Pump
• Cardiac Assist technology with proven reliability and performance, effectively decreases the workload of a weary heart
Decreases oxygen consumption
Increases cardiac output, perfusion, pressure and volume to Coronary Artries
Made in U.S.A. with over 35 years of proven technology

• Counterpulsation: A technique that synchronizes the external pumping of blood with the heart's cycle to assist the circulation and decreasing the work of the heart. Counterpulsation pumps when the heart is resting to increase blood flow and oxygen to the heart. Counterpulsation stops pumping when the heart is working to decrease the heart's workload and lessen oxygen demand
• Intra-Aortic Balloon Pump (IABP) - A device used to reduce left ventricular systolic work, left ventricular end-diastolic pressure, and wall tension.
• It is inserted into the descending aorta via the femoral artery either percutaneously or by surgical cut-down.
• The balloon rapidly deflates just before ventricular systole to reduce the impedance (A measure of the total opposition to current flow in an alternating current circuit) to left ventricular ejection.

• It then rapidly inflates immediately following aortic valve closure to augment (To make (something already developed or well under way) greater, as in size, extent) diastolic coronary perfusion pressure.

Intra-aortic Balloon Counter Pulsation Pump (IABP)

• The balloon is inflated during diastole in sync with the closure of the aortic valve.
• The blood in the aortic arch above the level of the balloon is pushed backward providing increased coronary artery blood flow and increased myocardial oxygen supply.

• The balloon is deflated just before systole which helps to decrease afterload.
• The space where the balloon was inflated creates an empty space where the blood doesn't have to flow against any resistance.

• IABP support is used until the heart function is improved enough to work on its own.
• The patient is gradually weaned from the IABP by reducing the pumping rate from 1:1 (augmentation (the amount by which something increases) with every beat) to 1:2 (augmentation with every other beat) to 1:4 (augmentation with every fourth beat).
• Cardiac function is assessed at each stage and IABP is removed if heart function is satisfactory.

• Intra-aortic balloon pump (IABP)• If a patient is unable to be weaned from CPB
(Cardiopulmonary bypass (CPB) is a technique that temporarily takes over the function of the heart and lungs during surgery), an intra-aortic balloon pump can be used to decrease afterload and increase myocardial blood flow.
• Harken and colleagues of Boston originally described the concept of counterpulsation in 1958 when, in an attempt to increase coronary artery perfusion, they used femoral access to remove blood during systole and replace it during diastole.
• Intra-aortic balloon pump (IABP) counterpulsation was first introduced clinically by Kantrowitz and associates in 1967.

• This therapeutic approach was instituted for treatment of two patients with left ventricular failure after AMI.
• Since that time, IABP has become a standard treatment for medical and surgical patients with acute left ventricular failure that is unresponsive to pharmacological and volume therapy
• Therapeutic goals are directed toward increasing oxygensupply to the myocardium, decreasing left ventricular work,and improving cardiac output.
• Before IABP, no single therapeutic agent was capable of meeting these three goals.
• IABP counterpulsation is designed to increase coronaryartery perfusion pressure and blood flow during thediastolic phase of the cardiac cycle by inflation of a balloon in the thoracic aorta.
• Deflation of the balloon, just before systolic ejection, decreases the impedance (The total opposition that a circuit offers to the flow of alternating current or any other varying current at a particular frequency) to ejection (afterload) and thus left ventricular work, with subsequent decreased myocardial oxygen consumption.
• Inflation and deflation counterpulse (To move or
act in opposition to; oppose) each heart beat.
• With improved blood flow and effective reduction in left ventricular work, the desired results are increased coronary artery perfusion and decreased afterload with subsequent increase in cardiac output.

• Physiological Principles• Greater work is required to maintain
cardiac output in the failing heart.
• With this added work requirement, oxygen demand increases.
• These circumstances may occur at a time when the myocardium already is ischemic and coronary artery perfusion is unable to meet the oxygen demands.
• As a result, left ventricular performance diminishes even further, resulting in decreased cardiac output.
• A vicious cycle ensues (To follow as a consequence or result) that is difficult to interrupt. Without interruption of the cycle, cardiogenic shock may be imminent (close in time; about to occur).

• This cycle can be broken with IABP therapy byincreasing aortic root pressure during diastole throughinflation of the balloon.
• With increased aortic root pressure, the perfusion pressure of the coronary arteries is increased.
• Effective therapy for the patient in left ventricular failure also involves decreasing myocardial oxygen demand.
• Four major determinants of myocardial oxygen demandare afterload, preload, contractility, and heart rate.

• IABP counterpulsation therapy can have an effect on all these factors.
• It decreases afterload directly and affects the other three determinants indirectly as cardiac function improves.
• Because IABP therapy assists the left heart, only the left ventricle is discussed here.

• AFTERLOAD AND PRELOAD
• The greatest amount of oxygen required during the cardiac cycle is for the development of afterload
• With greater impedance to ejection, afterload increases,thus resulting in increased myocardial oxygen demand.

• Impedance to ejection is caused by the aortic valve, aortic end-diastolic pressure, and vascular resistance.
• Greater aortic end-diastolic pressures require higher afterload to overcome impedance and ejection.
• Vascular resistance increases impedance when vessels become vasoconstricted.
• Vasodilation or lower vascular resistance
decreases afterload by decreasing impedance to ejection.
• Deflation of the balloon in the aorta just
before ventricular systole lowers aortic end-diastolic pressure.

• This decreases impedance to ejection and decreases left ventricular workload.
• In this way, IABP can effectively decrease the oxygen demand of the heart.
• A person in acute left ventricular failure has increased volume in the ventricle at end-diastole (preload) as a result of the heart’s inability to pump effectively.

• This excessive increase in preload increases the workload of the heart.
• IABP therapy helps to decrease
excessive preload by decreasing impedance to ejection.
• With decreased impedance, there is
more effective forward flow of blood and more efficient emptying of the left ventricle.
• CONTRACTILITY• Contractility refers to the velocity and
vigor of contraction during systole.• Although vigorous contractility requires
more oxygen, it is a benefit to cardiac function because it ensures good, efficient pumping, which increases cardiac output.
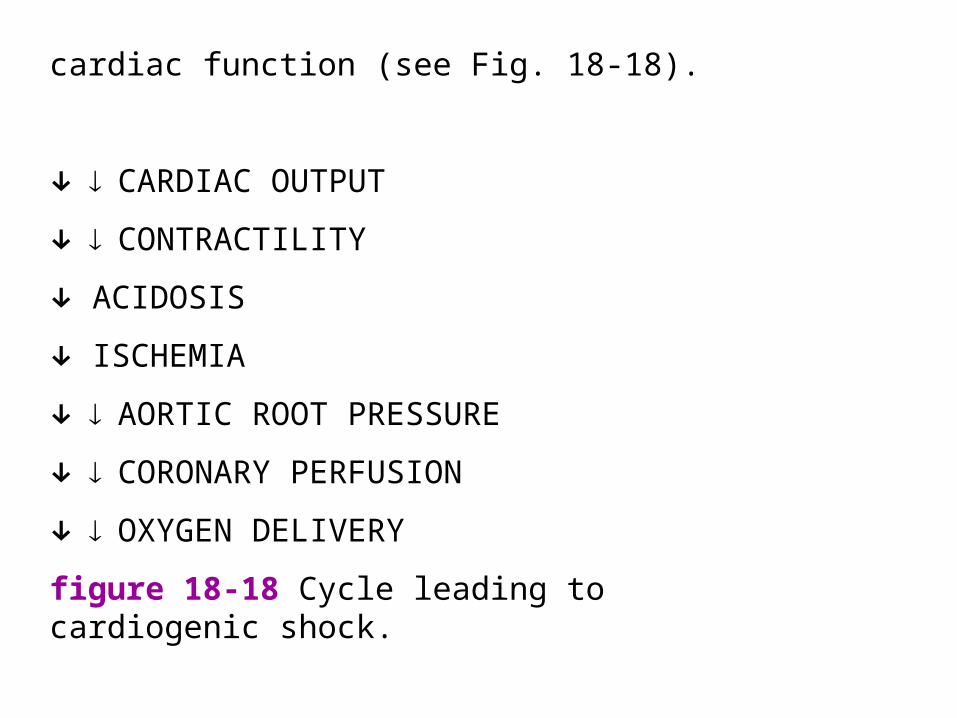
cardiac function (see Fig. 18-18).
↓CARDIAC OUTPUT
↓CONTRACTILITY
↓ ACIDOSIS
↓ ISCHEMIA
↓AORTIC ROOT PRESSURE
↓CORONARY PERFUSION
↓OXYGEN DELIVERY
figure 18-18 Cycle leading to cardiogenic shock.

• In failure, contractility is depressed.
• The biochemical status of the myocardium directly affects contractility.
• Contractility is depressed when calcium levels are low, catecholamine levels are low, and ischemia is present with resultant acidosis.

• IABP counterpulsation can increase oxygen supply, thereby decreasing ischemia and acidosis.
• In this way, IABP therapy contributes to improved contractility and better cardiac function

• HEART RATE• Heart rate is a major determinant of oxygen
demand because the rate determines the number of times per minute the high pressures must be generated during systole.
• Normally, myocardial perfusion takes place during diastole. Coronary artery perfusion pressure is determined by the gradient between aortic diastolic pressure and myocardial wall tension
• It can be expressed by the following equation:
Coronary perfusion pressure aortic diastolic pressure -myocardial wall tension
• Tension in the muscle retards blood flow, which is why approximately 80% of coronary artery perfusion occurs during diastole.
• With faster heart rates, diastolic time
becomes shortened, with very little change occurring in systolic time.
• A rapid heart rate not only increases oxygen demand but decreases the time available for oxygen delivery.

• In acute ventricular failure, a person may not be able to maintain cardiac output by increasing the volume of blood pumped with each beat (stroke volume) because contractility is depressed.
• Cardiac output is a function of both
stroke volume and heart rate:Cardiac output stroke volume heart rate

• If stroke volume cannot be increased, heart rate must increase to maintain cardiac output.
• This is very costly in terms of oxygen
demand.
• By improving contractility, IABP therapy helps improve myocardial pumping and the ability to increase stroke volume.
• Decreasing afterload also increases pumping efficiency.

• With improved myocardial function and cardiac output, the need for compensatory tachycardia diminishes.
• IABP counterpulsation increases coronary artery perfusion pressure by increasing aortic diastolic pressure during inflation of the balloon, resulting in improved blood flow and oxygen delivery to the myocardium.
• The physiological effects of IABP therapy are summarized in Box 18-14.
• Proper inflation of the balloon increases oxygen supply, and proper deflation of the balloon decreases oxygen demand.
• Timing of inflation and deflation is crucial and must coincide with the cardiac cycle.

• Direct Physiological Effects of IABP Therapy
• Inflation Aortic diastolic pressure Aortic root pressure Coronary perfusion pressure Oxygen supply• Deflation Aortic end-diastolic pressure Impedance to ejection Afterload Oxygen demand
• Equipment Features• The intra-aortic balloon catheter and the balloon mounted
on the end are constructed of a biocompatible polyurethane material.
• Filling of the balloon is achieved with a pressurizedgas that enters through the catheter.
• Because of its low molecular weight, helium is the pressurized gas of choice.
• Balloon size should be determined by the patient’s physical stature (An achieved level; status) to optimize counterpulsation (Table 18-11).
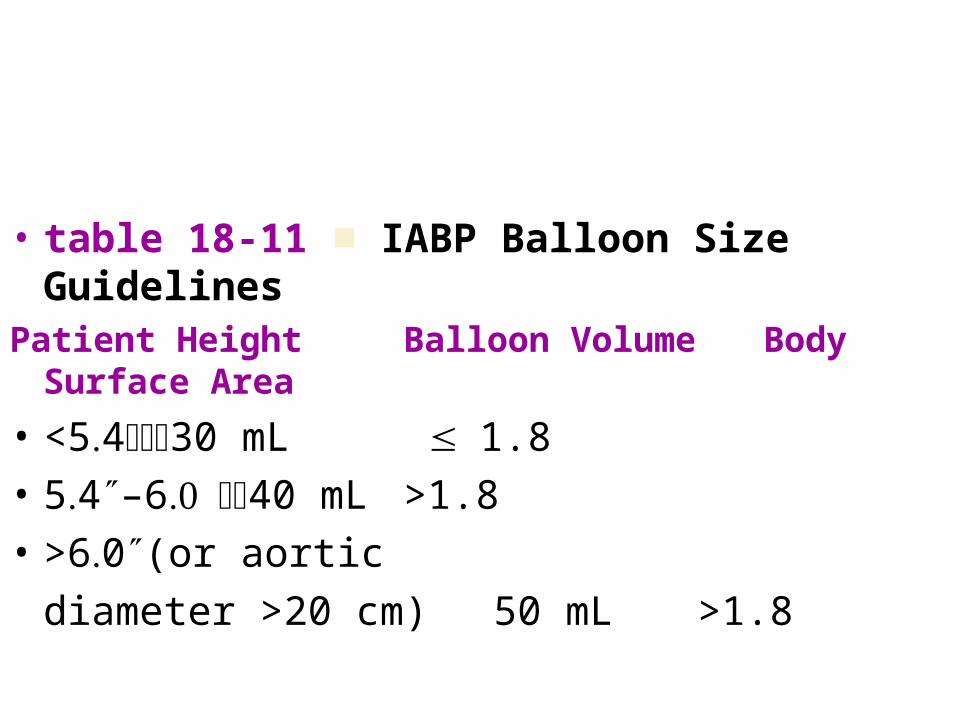
• table 18-11 ■ IABP Balloon Size Guidelines
Patient Height Balloon Volume Body Surface Area
• <5430 mL 1.8• 54″–640 mL >1.8• >60″(or aortic
diameter >20 cm) 50 mL >1.8
• With inflation, the addition of the balloon volume into the aorta acutely increases aortic pressure and retrograde blood flow back toward the aortic valve.
• With deflation, the sudden evacuation of the balloon volume acutely decreases aortic pressure.
• Catheters have a central lumen with which aortic pressure can be measured from the tip of the balloon.

• Indications for Intra-aortic BalloonPump Counterpulsation• Two major applications of IABP therapy
are for treatment of cardiogenic shock after myocardial infarction and for acute left ventricular failure after cardiac surgery.
• Other applications of IABP therapy for patients with cardiac pathophysiological conditions are noted in Box 18-15.

• box 18-15• Indications for IABP Therapy■ Cardiogenic shock after acute infarction■ Left ventricular failure in the postoperative
cardiacsurgery patient■ Severe unstable angina■ Postinfarction ventricular septal defect or mitralregurgitation■ Short-term bridge to cardiac transplantation

• CARDIOGENIC SHOCK• Treatment of cardiogenic shock is
complicated, and the mortality rate remains high.
• Cardiogenic shock develops in
approximately 15% of patients with myocardial infarction.
• Patients initially are treated with various inotropic drugs, vasopressors, and volume.

• A lack of, or minimal response in, cardiac output, arterial pressure, urine output, and mental status after this therapy indicates a need for assisted circulation with IABP therapy.
• Once hypotension is present, the self-perpetuating (To prolong the existence)
process of injury is in effect.
• Control of further injury and improvement in survival require early reversal of the shock state.
• Once IABP therapy is instituted, improvement shouldbe observed within 1 to 2 hours.
• At this time, steady improvement should be seen in cardiac output, peripheral perfusion, urine output, mental status, and pulmonary congestion.
• With improved cardiac function, a decrease in central venous pressure and PAWP also should be seen.
• Average peak effect should be achieved within 24 to 48 hours.

• box 18-15Indications for IABP Therapy■ Cardiogenic shock after acute infarction■ Left ventricular failure in the postoperative
cardiacsurgery patient
■ Severe unstable angina■ Postinfarction ventricular septal defect or
mitralregurgitation
■ Short-term bridge to cardiac transplantation
• POSTOPERATIVE LEFT VENTRICULAR FAILURE• Although the best outcomes result when IABP
counterpulsation is initiated at least 2 hours before cardiac surgery, a successful reduction in the mortality rate has been achieved by using IABP therapy for patients with acute left ventricular failure after cardiac surgery.
• Two major conditions might lead to postoperative pump failure: severe preoperative left ventricular dysfunction and intraoperative myocardial injury.

• IABP counterpulsation therapy can be used to weanpatients from cardiopulmonary bypass and to provide postoperative circulatory assistance until left ventricular recovery occurs.
• In these situations, early recognition of failure is evidenced by the heart’s inability to support circulation after cardiopulmonary bypass.
• Early recognition and treatment are crucial if left ventricular failure is to be reversed.

• UNSTABLE ANGINA• IABP counterpulsation therapy may be used
during PCI (percutaneous coronary intervention (angioplasty or stent placement) for patients with unstable angina or mechanical problems.
In this situation, PCI procedures usually are followed byemergency cardiac surgery.
• Patients in this category include those with unstable angina, postinfarction angina and postinfarction ventricular septal defects, or mitral regurgitation from papillary muscle injury with resultant cardiac failure.

• IABP counterpulsation therapy has been used successfully to control the severity of angina in patients in whom previous medical therapy has failed.

• The use of IABP therapy for patients with cardiac failure after ventricular septal rupture or mitral valve incompetence aids in the promotion of forward blood flow, which decreases shunting through the septal defect and decreases the amount of mitral regurgitation.
• Contraindications to Intra-aorticBalloon Pump Counterpulsation• There are few contraindications to the use of IABP
therapy.
• A competent aortic valve is necessary if the patient isto benefit from IABP therapy.
• With aortic insufficiency, balloon inflation would only increase aortic regurgitation and offer little, if any, augmentation of coronary artery perfusion pressure.
• In fact, the patient’s heart failure could be expected to become worse.

• Severe peripheral vascular occlusive disease also is a relative contraindication to the use of IABP therapy.
• Occlusive disease would make insertion of the catheter difficult and possibly interrupt blood flow to the distal extremity or cause dislodgement of plaque formation along the vessel wall, resulting in potential emboli.

• In patients who absolutely require IABP therapy, insertion can be achieved through the thoracic aorta, thus bypassing diseased peripheral vessels.
• Any previous aortofemoral or aortoiliac bypass graft contraindicates femoral artery insertion.
• The presence of an aortic aneurysm also is a contraindication to the use of IABP therapy.
• A pulsating balloon against an aneurysm may predispose the patient to dislodgement of aneurysmal debris with resultant emboli.
• A more serious complication is rupture of the aneurysm; it is possible for the catheter to perforate the wall of the aneurysm during insertion.

• Procedure• INSERTION• Proper positioning of the balloon is in the
thoracic aorta just distal to the left subclavian artery and proximal to the renal arteries (Fig. 18-19).
• The most commonly used method of catheter placement is percutaneous insertion using a Seldinger technique, although other approaches have been described.

• The most common alternative is direct insertion into the thoracic aorta.
• Because this requires a median sternotomy incision, it is restricted to cardiac surgical patients whose chests have been opened for the surgery.

• Once in place, the catheter is attached to a machine console (A cabinet for a radio, television set, or phonograph, designed to stand on the floor) that has three basic components: a monitoring system, an electronic trigger mechanism, and a drive system that moves gas in and out of the balloon.
• Monitoring systems have the capability of displaying the patient’s ECG and an arterial waveform showing the effect of balloon inflation– deflation.
• Consoles also are capable of displaying a balloon waveform that illustrates the inflation and deflation of the balloon itself.
• The standard trigger mechanism for the balloon pump is the R wave that is sensed from the patient’s ECG.

• This trigger signals the beginning of each cardiaccycle for the drive system.
• Other possible triggers include systolic arterial pressure or pacemaker spikes on the ECG.
• Adjustment of exact timing is controlled on the machineconsole.
• The drive system is the actual mechanism that drives gas into and out of the balloon by alternating pressure and vacuum.

• TIMING• Two methods of timing can be used
with IABP therapy:
• conventional timing and real timing. • Conventional timing uses the arterial
waveform as the triggering mechanism to determine both inflation and deflation of the balloon.

• Real timing uses the same point of reference (the dicrotic (A condition in which the pulse is felt as two beats per single heartbeat) notch on the arterial waveform) for balloon inflation but uses the ECG signal as the trigger for balloon deflation.
• Real timing is discussed briefly after conventional timing.
• Conventional Timing• The first step to proper timing of the balloon
pumpusing conventional timing is the identification of the beginning of systole and diastole on the arterial waveform.
• Systole begins when left ventricular pressure exceeds left atrial pressure, forcing the mitral valve closed.

• There are two phases of systole: isovolumetric contractionand ejection.
• Once the mitral valve is closed, isovolumetriccontraction begins and continues until enoughpressure is generated to overcome impedance to ejection.
• When ventricular pressure exceeds aortic pressure, theaortic valve is forced open, initiating ejection, or phase two.
• Ejection continues until pressure in the left ventricle fallsbelow pressure in the aorta. At this point, the aortic valve closes, and diastole begins.

• Closing of the aortic valve creates an artifact (something designed and created to serve a particular function) on the arterial waveform that is called the dicrotic notch.
• The dicrotic notch is used as a timing reference to determine when balloon inflation should occur.
• Inflation should not occur before the notch (a V-
shaped indentation [the act of cutting into an edge with toothlike notches or angular incisions]) because systole has not been completed.

• After aortic valve closure, two phases of diastole begin:
• isovolumic relaxation and ventricular filling.
• After aortic valve closure, there is a period in which neither the aortic nor mitral valve is open.
• The mitral valve remains closed because left ventricular pressure still is higher than left atrial pressure.
• This phase is isovolumic relaxation.

• When left ventricular pressure falls below left atrial pressure, the mitral valve is forced open by the higher pressure in the left atrium.
• This begins the filling phase of diastole.
• Balloon inflation should continue throughout diastole.
• Deflation should be timed to occur at end-diastole, just before the next sharp systolic upstroke on the arterial waveform.

• Figure 18-20 illustrates the cardiac cycle with left atrial, left ventricular, and aortic pressures superimposed on one another.
• Figure 18-21 illustrates a radial artery waveformwith the beginning of systole and diastole marked.

• Real Timing• The main difference between the two timing
methods is balloon deflation and the triggering mechanism used.
• Real timing uses the ECG as the trigger signal for balloon deflation.
• The QRS complex is recognized as the onset of ventricular systole, and balloon deflation occurs at this time.
• Triggering off of the R wave allows for balloon deflation to occur at the time of systolic ejection and not before (as with conventional timing).
• This timing mechanism is more effectivein patients with irregular heart rhythms because balloondeflation occurs on recognition of the R wave (systolic ejection).
• It does not need to be approximated by the operatoror an algorithm, as in conventional timing.

• Both a rapid deflation mechanism and a reliable ECG signal are necessary for IABP using real timing to augment blood pressure effectively.
• Balloon inflation with real timing occurs at theonset of diastole as triggered by the dicrotic notch on an arterial waveform, just as in conventional timing.
• Interpretation of Results• WAVEFORM ASSESSMENT• Analysis of the arterial pressure
waveform and the effectiveness of IABP therapy is an important nursing function.
• Nurses must be able to recognize and correct problems in balloon pump timing.

• Step 1• The first step in timing assessment is the ability
to recognize the beginnings of systole and diastole on the arterial waveform, as shown in Figure 18-21.
• Systole begins at point A, where the sharp upstroke begins.
• Point B marks the dicrotic notch, which represents aortic valve closure.
• At this point, diastole begins and the balloon should be inflated. Balloon deflation occurs just before point A, at end-diastole.
• Box 18-16 lists five criteria that can be used to measure the effectiveness of IABP therapy on the arterial pressure waveform.
• To evaluate the waveform effectively, the patient’s unassisted pressure tracing must be viewed alongside the assisted pressure tracing.
• This can be accomplished through adjustment of the console so that the balloon inflates and deflates on every other beat (i.e., a 1:2 assist ratio).
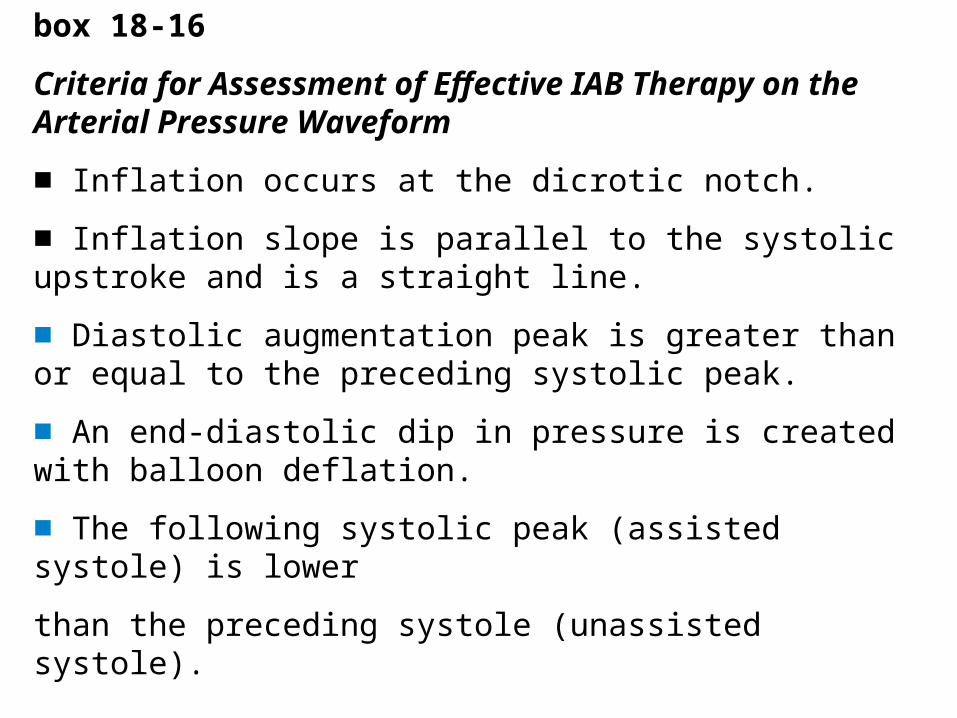
box 18-16
Criteria for Assessment of Effective IAB Therapy on the Arterial Pressure Waveform
■ Inflation occurs at the dicrotic notch.
■ Inflation slope is parallel to the systolic upstroke and is a straight line.
■ Diastolic augmentation peak is greater than or equal to the preceding systolic peak.
■ An end-diastolic dip in pressure is created with balloon deflation.
■ The following systolic peak (assisted systole) is lower
than the preceding systole (unassisted systole).
• Most patients tolerate this well for a brief period of time.
• Machine consoles are capable of freezing the waveform on the console monitor so that it would be necessary to assist at a 1:2 ratio only for one screen.
• Another alternative would be to obtain a strip recording of the 1:2 assistance for analysis.

• Step 2• After identification of the patient’s dicrotic notch,
a comparison is made with the assisted tracing to see that inflation occurs at the point of the dicrotic notch.
• Inflation before the dicrotic notch shortens systole abruptly and increases ventricular volume as ejection is interrupted.
• Late inflation, past the dicrotic notch, does not raise coronary artery perfusion pressure.
• The peak-diastolic pressure may not be as high as it would be with proper timing.
• Step 3• Next, the slopes of systolic upstroke and
diastolic augmentation should be compared.
• The diastolic slope should be sharp and parallel the systolic upstroke.
• The slope always should be a straight line.
• The greater the peak in diastolic pressure, the greater the increase in aortic root pressure.
• For this reason, balloon assistance is adjusted until the highest peak possible is achieved.
• Step 4• Deflation should occur just before systole,
causing an acute drop in aortic end-diastolic pressure.
• This quick deflation displaces approximately 40 mL of volume.
• The result is an end-diastolic dip in pressure that reduces the impedance to the next systolic ejection.

• The end-diastolic pressure without the balloon assistance should be compared with the end-diastolic pressure with the dip created by balloon deflation.
• Optimally, a pressure difference of at least 10 mm Hg should be obtained.
• Better afterload reduction is achieved with the lowest possible end-diastolic dip.
• The point of deflation also is crucial. Deflation that is too early allows pressure to rise to normal end-diastolic levels preceding systole.
• In this situation, there is no decrease in afterload.
• Late deflation encroaches (advance beyond the usual limit) on the next systole and actually increases afterload owing to greater impedance to ejection from the presence of the still-inflated balloon during systolic ejection.

• Step 5• Finally, if afterload has been reduced, the
next systolic pressure peak will be lower than the unassisted systolic pressure peak.
• This implies that the ventricle did not have to generate as great a pressure to overcome impedance to ejection.
• This may not always be seen because the systolic pressure peak also represents the compliance of the vasculature.
• If the vasculature is noncompliant due to atherosclerotic disease, the systolic peak may not change very much.
• Figure 18-22 illustrates the five points that are assessed on the waveform,
• whereas Figure 18-23 demonstrates possible errors in timing.

• Balloon Fit• The fit of the balloon to any particular patient’s
aorta determines how well these criteria are met.
• Ideally, approximately 80% of the aorta is occluded with balloon inflation.
• In a dilated aorta, in which less than 80% occlusion occurs, the effect of inflation and deflation is not as dramatic on the waveform.
• When a patient is hypotensive or hypovolemic, the balloon does not have as pronounced an effect on the waveform because there is less volume displacement as the balloon inflates or deflates.
• Assessment and ManagementPatients requiring IABP are managed much like any othercritically ill patient in cardiogenic shock or acute left ventricular failure.
• SYSTEM MONITORING• Cardiovascular System• Monitoring the cardiovascular system is extremely
important in determining the effectiveness of balloon pump
therapy. • The basis for this assessment includes vital signs,
cardiac output, heart rhythm and regularity, urine output, color, perfusion, and mentation.
• Vital Signs. Three important vital signs with respect to IABP therapy are heart rate, mean arterial pressure (MAP), and PAWP.
• Effective IABP therapy causes a decrease in all three parameters.
• Acute changes in the MAP may indicate volume depletion.
• Critically ill patients tolerate little change in their volume status.
• The PAWP is an important parameter for monitoring volume and provides the clinician with an
early indication of volume depletion or overload.
• Blood pressure readings require special consideration.
• Because the balloon inflates during diastole, peak-diastolic pressure may be higher than peak-systolic pressure.
• Most IABP consoles have monitoring systems capable of distinguishing systole from peak diastole; however, some monitoring equipment can distinguish only peak pressures from low-point pressures.
• For this reason, a monitor’s digital display of systolic pressure actually may represent peak-diastolic pressure.
• It is advisable to record blood pressure as systolic, peak-diastolic, and end-diastolic— that is, 100/110/60.
• These pressures can be read from a strip recording of the arterial waveform.
• Heart Rhythm and Regularity. Heart rhythm and regularity are important considerations.
• Early recognition and treatment of dysrhythmias are crucial for effective IABP support.
• Irregular dysrhythmias may inhibit efficient IABP therapy with some types of consoles because timing is set by the regular R-R interval on the ECG.
• A safety feature of all balloon pump consoles is automatic deflation of the balloon for premature QRS complexes.
• One particular IABP model tracks real time versus any average of beats so it more effectively tracks dysrhythmias.

• If the dysrhythmia persists and timing is ineffective, another alternative might be use of the systolic peak on the arterial waveform as the trigger mechanism for balloon inflation.
• The primary goal in dysrhythmias is to treat the dysrhythmia.

• Other Observations. Urine output, color, perfusion, and mentation all are important assessment parameters for determining the adequacy of cardiac output.
• All should improve in patients responsive to IABP therapy.
• Any deterioration in these signs also might indicate a fall in cardiac output.
• Cardiac output measurement is indicated when deterioration is evident, when a major change in volume or pharmacological therapy has been instituted, and during weaning from IABP support.

• The left radial pulse and the cannulated extremity should be frequently assessed.
• A decrease, absence, or change in character of the left radial pulse may indicate that the balloon has advanced up the aorta and may be partially obstructing or has advanced into the left subclavian artery.
• The presence of the balloon catheter in the femoral or iliac artery predisposes the patient to impaired circulation of the involved extremity.
• The affected extremity needs to be kept relatively immobile. Because flexion of the hip may kink the catheter and impair balloon pumping, it may be helpful to use a knee immobilizer to remind the patient to avoid hip flexion.

• The head of the bed also should not be elevated more than 30 degrees.
• Hip flexion also contributes to decreased perfusion to the distal extremity.
• Extremities should be checked hourly for pulses, color, and sensation.
• Any deterioration in the affected extremity should be reported to the physician.
• Severe arterial insufficiency necessitates removal of the catheter.

• Physicians advocate the use of heparin therapy to prevent possible thrombus formation around the catheter and vascular insufficiency, especially in medical patients.
• Each physician will determine whether the risks of anticoagulation outweigh the benefits for the specific patient.
• Low–molecular-weight dextran is another possible choice of therapy to prevent thrombus formation.

• This agent impairs platelet function and prevents triggering of the coagulation cascade.
• It is usually preferred in the cardiac surgical patient for the first 24 hours
• Pulmonary System• Many patients on IABP therapy require intubation and• ventilatory assistance. Some of these patients may have• respiratory insufficiency secondary to fluid overload
associated• with CHF. The immobile, intubated patient is• always at risk for respiratory infections and the
development• of atelectasis. Turning the patient is appropriate• provided modifications are implemented to keep the
extremity• cannulated by the balloon catheter straight. Daily• chest roentgenograms are needed to follow pulmonary• status and to inspect IV catheter placement. The position• of the balloon catheter also can be determined in this• manner.
• Renal System• Patients in cardiogenic shock or severe
left ventricular• failure are at risk for the development
of acute renal failure.• In the shock state, the kidneys suffer
the consequences of• hypoperfusion; therefore, urine output
and quality should

• be monitored closely. Serum BUN, creatinine, and creatinine
• clearance should be monitored daily to assess renal
• function. Creatinine clearance indicates renal dysfunction
• and possible failure much earlier than elevated serum creatinine.
• Any acute, dramatic drop in urine output might be
• an indication that the catheter has slipped down the aorta
• and is obstructing the renal arteries.


• WEANING• Indications for Weaning• Weaning patients from balloon
assistance usually can• begin 24 to 72 hours after
insertion. Some patients require• longer periods of support. Weaning
can begin when there• is evidence of hemodynamic
stability that does not require

• excessive vasopressor support. Ideally, vasopressor support
• is minimal when weaning begins. After the balloon
• is removed, it is much easier to increase vasopressor support
• than to reinsert a balloon catheter for hemodynamic
• support

• The patient should exhibit signs of adequate cardiac function,
• demonstrated by good peripheral pulses, adequate
• urine output, absence of pulmonary edema, and improved
• mentation. Good coronary artery perfusion will be evidenced
• by an absence of ventricular ectopy and no evidence of
• ischemia or injury on the ECG.• Complications may require ab
• Complications may require abrupt cessation of IABP.
• This may or may not result in reinsertion of another balloon
• catheter. Severe arterial insufficiency evidenced by a

• loss of pulses in the distal extremity, pain, and pallor is definitely
• an indication to remove the balloon catheter from• that particular insertion site. Any balloon that develops a• leak also requires removal. The physician may choose to• reinsert the balloon catheter in another extremity or to• replace the faulty balloon if the patient is
hemodynamically• unstable. Depending on the philosophy of the institution• and physician, a deteriorating, irreversible situation• also might be an indication for weaning or discontinuing• balloon pump support. Box 18-18 lists major indications• for weaning from IABP therapy.
• Approaches to Weaning• Weaning is commonly achieved by
decreasing the assist• ratio from 1:1 to 1:2 and so on until the
minimum assist• ratio is achieved on any particular
console. A patient might• be assisted at the first decrease for up
to 4 to 6 hours. The• minimum amount of time should be 30
minutes. During• this time, the patient must be assessed
for any change in• hemodynamic status.

• An increase in heart rate, a decrease• in blood pressure, and a decrease in cardiac output
indicate• a deterioration in hemodynamic status. Weaning
should be• discontinued temporarily and therapy should be
adjusted• before another weaning attempt. If the first decrease
in• assist ratio is tolerated, the assist ratio is decreased to
minimum,• with 1 to 4 hours allowed for each new assist ratio.• The patient must be assessed continually for any
indications• of intolerance to the process. Although less common,
weaning• can also occur by decreasing balloon volume, which in• many models is controlled from the console.

• From IABP• ■ Hemodynamic stability• Cardiac index >2 L/min• PAWP <20 mm Hg• Systolic blood pressure >100 mm Hg• ■ Minimal requirements for vasopressor support• ■ Evidence of adequate cardiac function• Good peripheral pulses• Adequate urine output• Absence of pulmonary edema• Improved mentation• ■ Evidence of good coronary perfusion• Absence of ventricular ectopy• Absence of ischemia on the ECG• ■ Severe vascular insufficiency• ■ Balloon leakage• ■ Deteriorating, irreversible condition

• Complications Specific to Intra-aortic• Balloon Pump Therapy• Patients with IABP counterpulsation need to
be monitored• for development of poor blood flow to the
cannulated• extremity, which could lead to compartment
syndrome. It• may occur within the first 24 hours of
support or not until• several days after catheter insertion.
Compartment syndrome• is caused by a rise in the tissue pressure in
one of
• the compartments of the affected lower extremity. Bone,
• muscle, nerve tissue, and blood vessels all are enclosed by a
• fibrous membrane called the fascia, and this enclosed space
• is called a compartment. It is nonyielding, so a rise in volume
• in the compartment increases the pressure in the compartment.
• The patient with IABP in whom limb ischemia develops
• from decreased capillary flow can suffer cellular and
• capillary damage that leads to increased capillary permeability.

• The resultant transudation of fluid into the closed
• compartment space increases tissue pressure to a level that
• can interfere with capillary blood flow. When this degree of
• tissue pressure is reached, tissue viability may be threatened.
• Treatment is directed at improving blood flow. Pressure
• release by fasciotomy may be needed to prevent tissue death.
• Decreased circulating platelets in the first 24 hours of• IABP therapy and a minimal decrease in red blood cell• count have been reported; however, they are not
thought to• be significant problems. There is a low incidence of
balloon• leakage and rupture. These complications might
result• from balloon inflation against a calcific,
atherosclerotic• plaque in the aorta.

• This disruption in the balloon surface• may be as small as a pinhole or may be
a large tear. The• associated danger is gas embolism. In
addition, the risk of• entrapment is minimal but still exists.
Table 18-12 provides• additional details about injury
secondary to balloons.

• Insertion of the catheter in the face of severe atherosclerotic
• vascular disease might result in arterial perforation or
• occlusion. Any leak is an indication for immediate balloon
• removal. Iatrogenic dissection of the aorta is rare but has
• been reported.

• Arterial insufficiency is the most common
• complication of IABP therapy. Arterial insufficiency may be
• permanent, or it may be relieved by aortofemoral or ileofemoral
• bypass grafting. Neuropathy in the catheterized
• extremity is another reported complication.





























