Embed Size (px)
Citation preview
Intrauterine Growth Restriction
Eric H. Dellinger, MD
Greenville Hospital System

IUGR: Introduction
• IUGR 2nd leading contributor to PNM rate• PNM rate increased 6-10 fold• PNM rate 8/1000 background:
– 120/1000 for all IUGR– 60-80/1000 when anomalies excluded
IUGR: Introduction
• 40% of stillbirths have IUGR– 53% of preterm stillbirths– 26% of term stillbirths
• Intrapartum asphyxia reported in up to 50% of IUGR fetuses
• > 60% of IUGR fetuses with FHR tracing abnormalities have hypoxia/acidosis
• Pardi, NEJM 328:692, 1993
When is small, too small? Defining IUGR
IUGR: Definition
• Birth weight < 10th percentile used to define growth restriction at birth
• Definition carried over to fetuses using ultrasound measurements (+/- 15%)
• Using 10th percentile, 70% will be constitutionally small (no increase risk)
• Two SD = less than 3rd percentile• AC < 2.5th percentile has 95% sensitivity
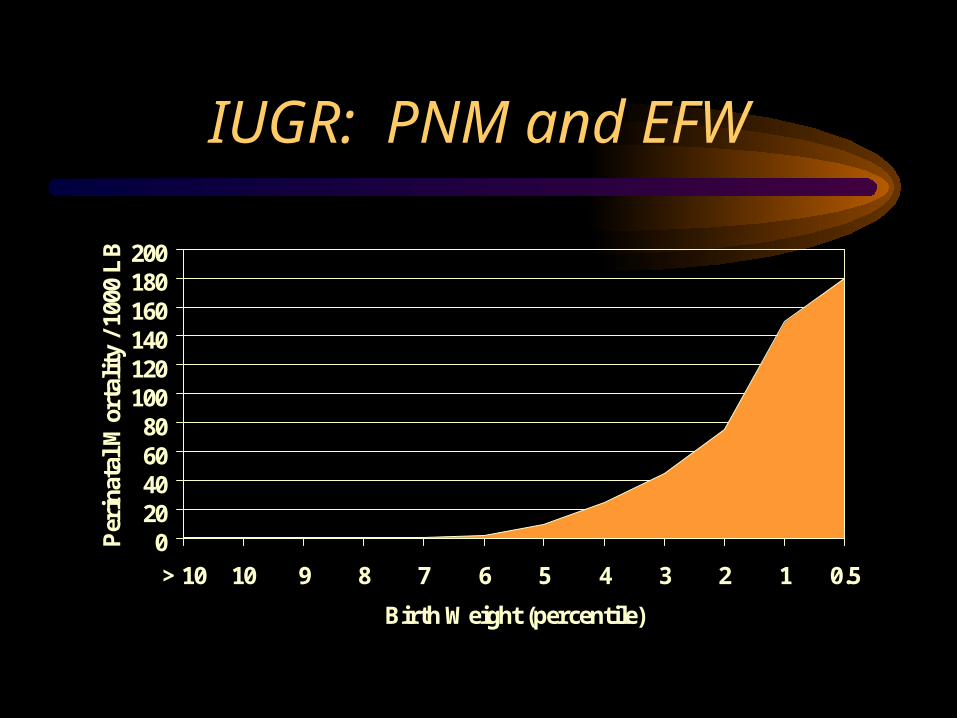
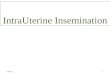
IUGR: PNM and EFW
020406080
100120140160180200
> 10 10 9 8 7 6 5 4 3 2 1 0.5
Birth Weight (percentile)
Per
inat
al M
orta
lity
/ 10
00 L
B
Background Information
Normal Versus Abnormal
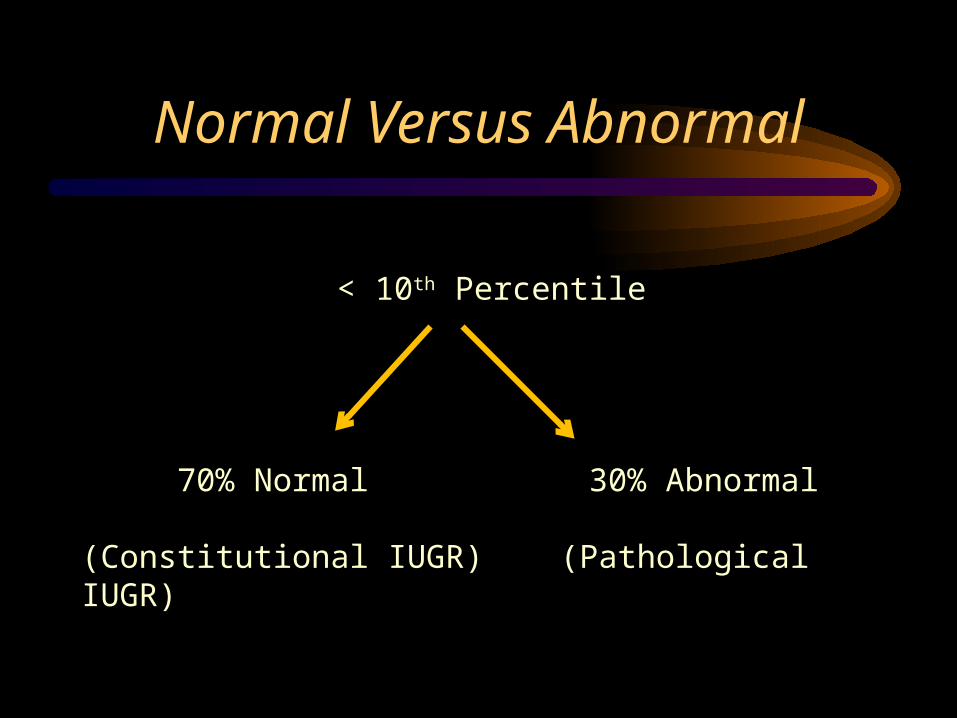
Normal Versus Abnormal
< 10th Percentile
70% Normal 30% Abnormal
(Constitutional IUGR) (Pathological IUGR)
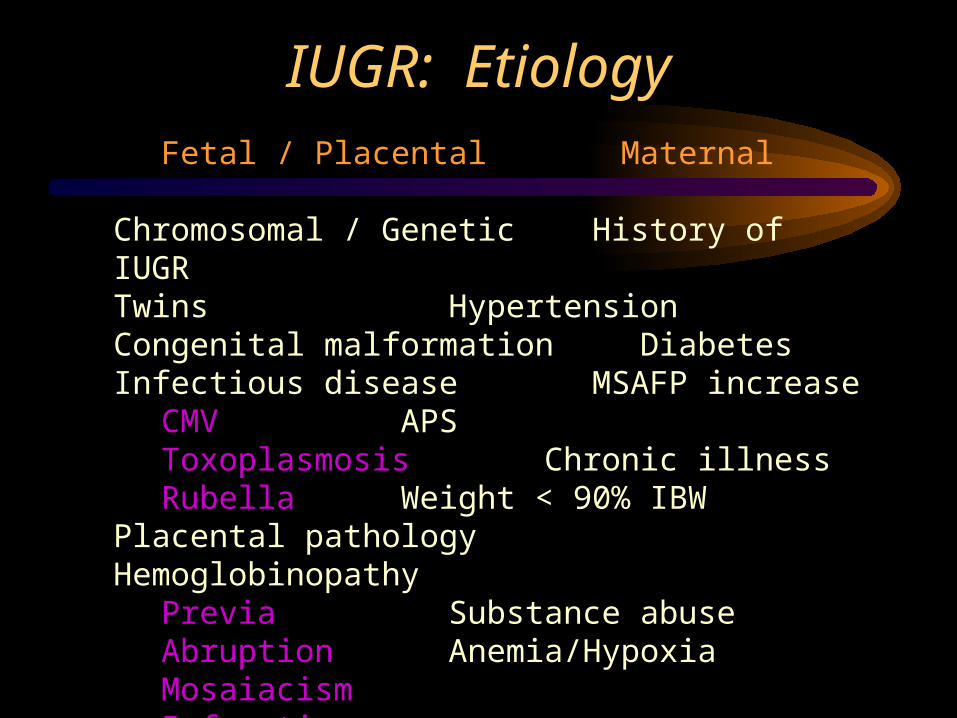
IUGR: EtiologyFetal / Placental Maternal
Chromosomal / Genetic History of IUGRTwins HypertensionCongenital malformation DiabetesInfectious disease MSAFP increase
CMV APSToxoplasmosis Chronic illnessRubella Weight < 90% IBW
Placental pathology HemoglobinopathyPrevia Substance abuseAbruption Anemia/HypoxiaMosaiacismInfarction
Past History of IUGR
• Prior history #1 risk factor for subsequent IUGR
• 1 prior episode: 25% recurrence• 2 episodes: Fourfold increase• 1/3 population “at risk”: 2/3 IUGR babies• 2/3 population “low risk”: 1/3 of the IUGR
babies, but most are constitutional
IUGR: Diagnosis
• The Fundal Height Myth:– best from 20-32 weeks: lightening– lag of 4 cm suspicious– Sensitivity of 27%, PPV of 18%
• Fundal height of limited value– risk factors more predictive
IUGR: Fetal Measurements
• Have you weighed a fetus lately?– EFW derived indirectly
• “Normal” growth curves difficult to establish• PTL strongly associated with IUGR
– BW derived charts inaccurate
• U/S growth curves more accurate over preterm age ranges
IUGR: Fetal Growth Patterns
When did you last watch a fetus grow?
Strategy
Strategy
• Normal versus abnormal• Symmetric versus asymmetric• Fetal causes
– Anomalies, arrhythmias, infection
• Placental problems• Amniotic fluid• Dopplers• Fetal surveillance
HC/AC Ratios
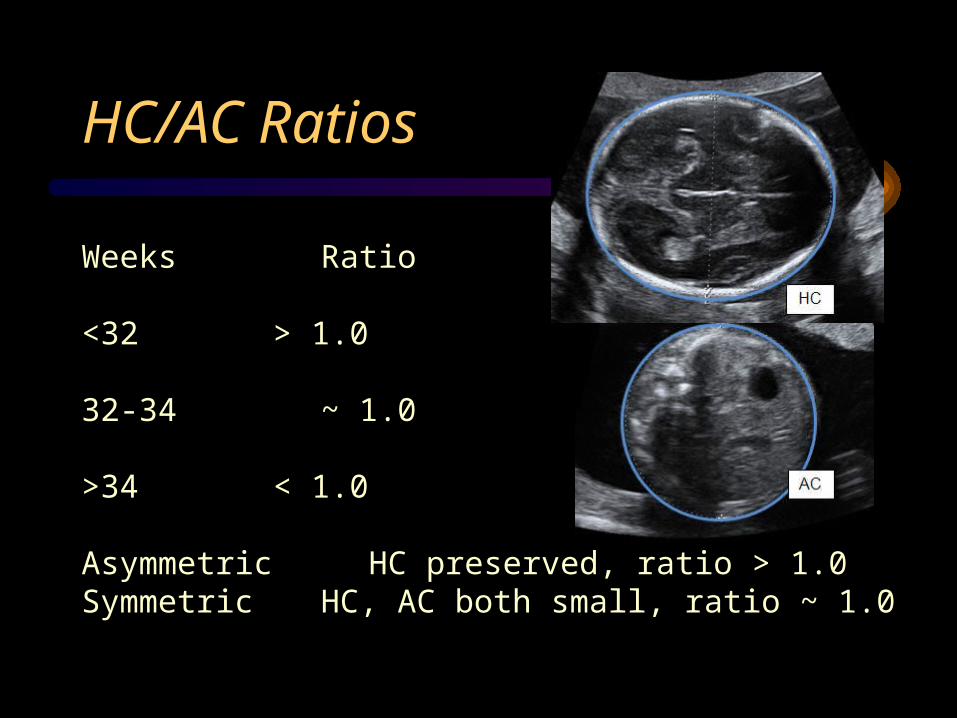
Weeks Ratio
<32 > 1.0
32-34 ~ 1.0
>34 < 1.0
Asymmetric HC preserved, ratio > 1.0Symmetric HC, AC both small, ratio ~ 1.0
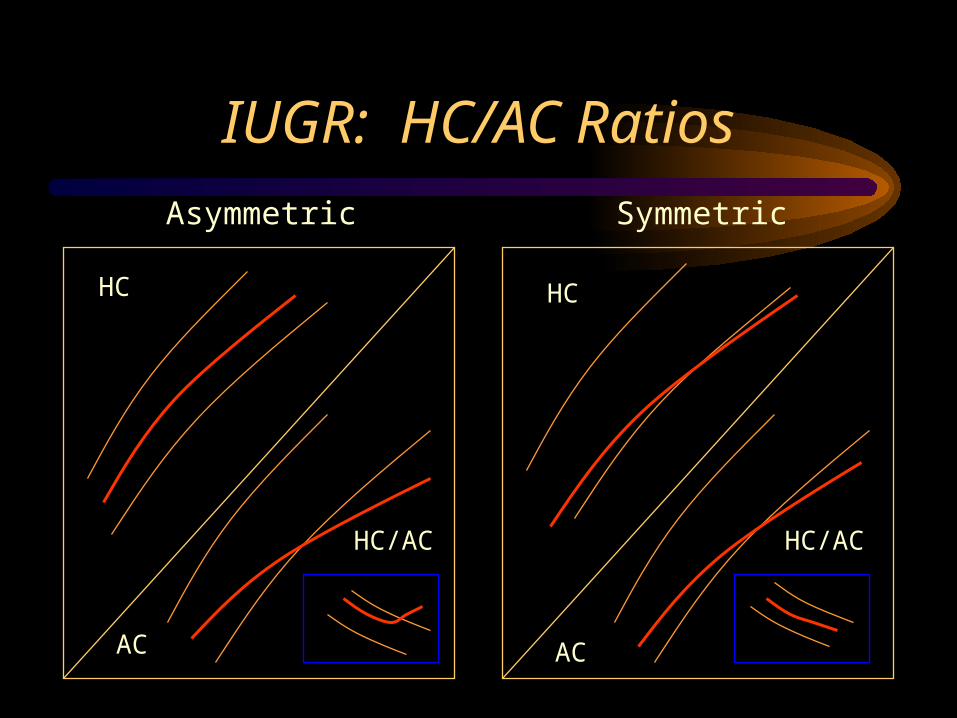
IUGR: HC/AC Ratios
Asymmetric Symmetric
HC HC
AC AC
HC/AC HC/AC
Asymmetric vs. Symmetric
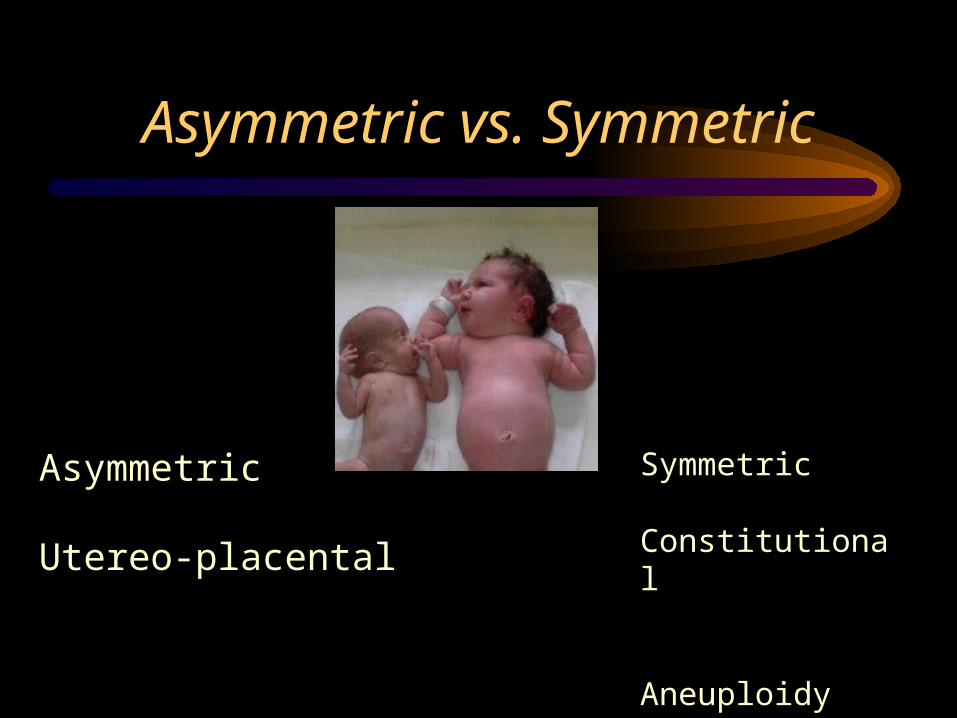
Asymmetric
Utereo-placental
Symmetric
Constitutional
Aneuploidy Infection
Fetal Causes
• Aneuploidy• Anomalies• Arrhythmias• Infection
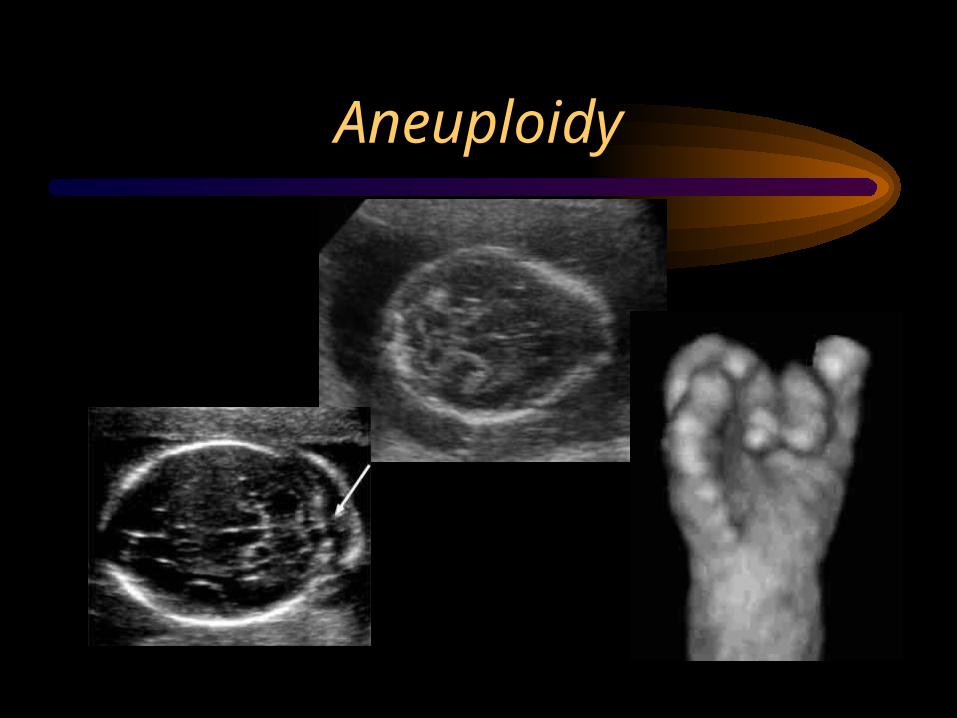
Aneuploidy
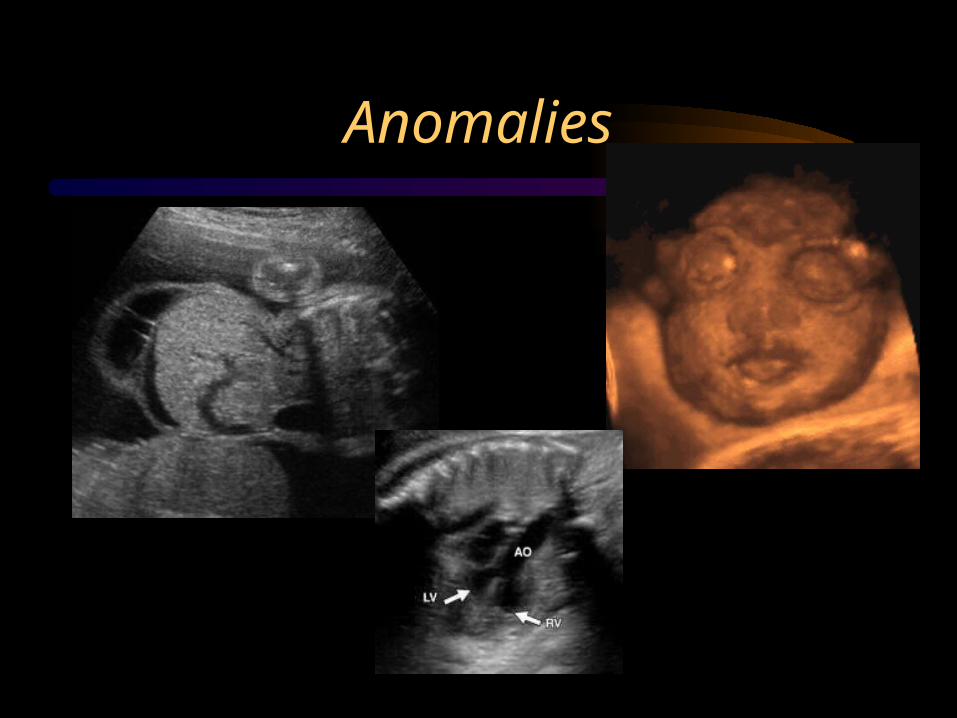
Anomalies
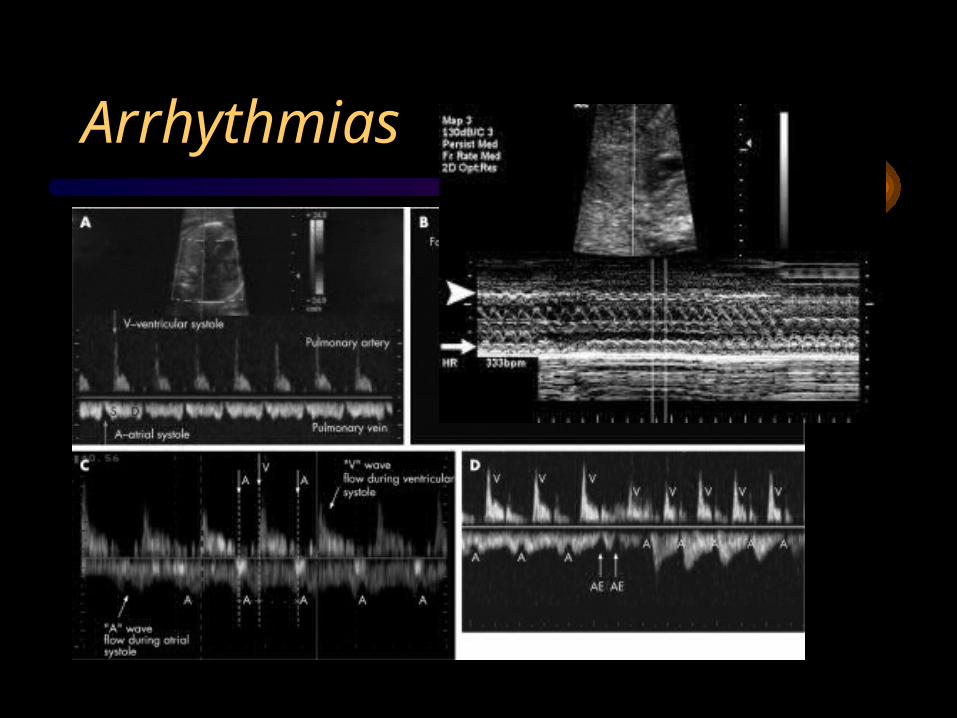
Arrhythmias

Infection
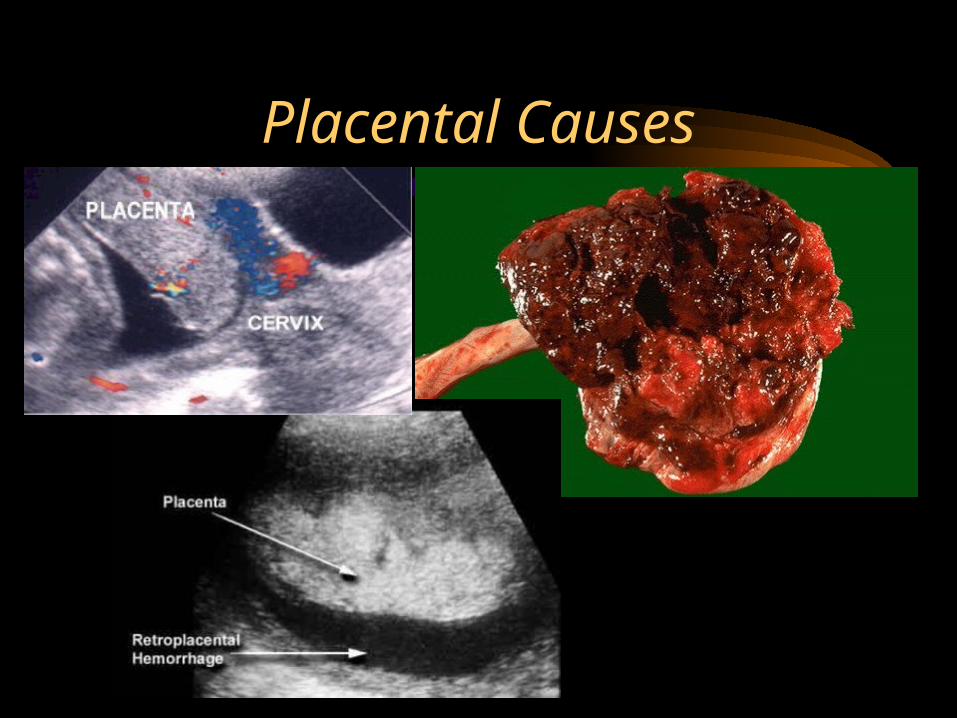
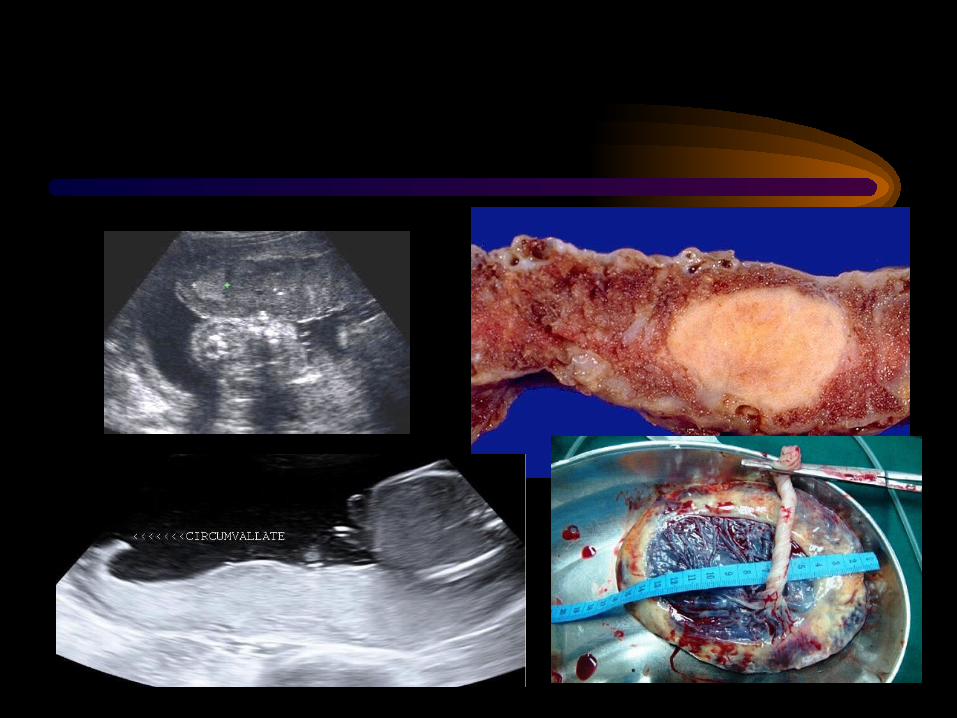
Placental Causes

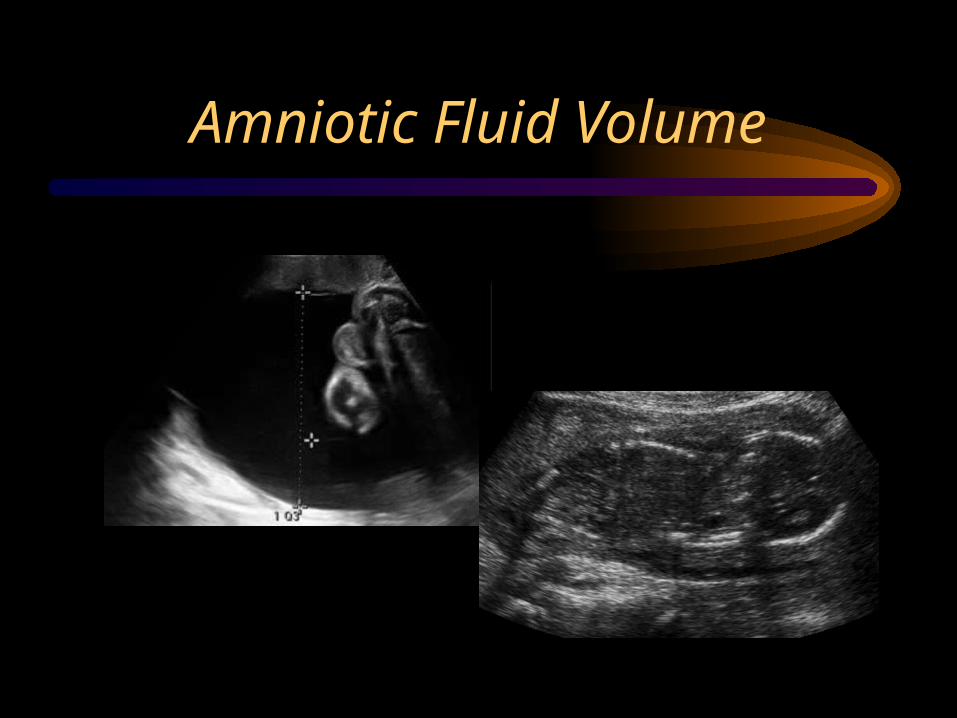
Amniotic Fluid Volume
IUGR: Oligohydramnios
• Initial harbinger of doom– IUGR, preeclampsia– may precede abnormal HC/AC
• Fluid pocket of BPP:– >2 cm 6% IUGR– 1-2 cm 20% IUGR– <1 cm 39% IUGR– also predicts intrapartum distress
![Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://img.pdfslide.net/doc/110x75/5b63022f7f8b9ade588b8aac/early-intrauterine-development-of-mixed-giant-early-intrauterine-development.jpg)