Embed Size (px)
Citation preview

Introduction
Instructor :MSc Ikhlas Jarrar

Pharmacology
• Science that study study of drug action• Has two main areas – Pharmacodynamics – Pharmacokinetics – Phamacotherapeutics
• Pharmacology has many divisions :

Drug
• Chemical or biological agent that affect the biological systems
• May be used to :– treat, cure, prevention, diagnosis of disease ,and
enhance physical or mental well-being• Drug may be derived fro natural sources or
may be synthetic

Every drug have 3 names chemical,generic and trade name
• Chemical name describes the atomic molecular structure(seldom used
• Generic name =scientific name– The best used to avoid confusion
• Trade name =brand name – may differ according to company– Followed by symbol R means registered and
restricted

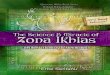
How is the drug developed
Clinical study Animal testingIn vitro study
marketing
Gen
eric
s av
aila
bl
Phas
e 4
Phas
e 3
Phas
e 2
Phas
e 1
New
dru
g ap
plic
ation
0 2 4 8-9 20 yr

Clinical study
• On human• Composed of 4 phases
1. Phase I Small number of normal people Pharmacokinetic of the drug is studied
2. Phase II Moderate number of normal and ill patients The goal is to see whether the drug works in the ill
patients

Clinical study
3. Phase III Larger number of people
4. Phase IV After marketing Study of toxicity of the drugs

Areas of pharmacology
• Pharmacokinetic– What the body do to the drug– ADME
• Pharmacodynamics – What the drug do to the body

Pharmacokinetic
• Action of the body on the drug• Composed of:– Absorption (A)– Distribution (D)– Metabolism (M)– Elemenation (E)


Absorption
• Rate and extent to which the drug moves from its site of administration

What does the rate and efficacy of absorption depend on?
1. Route of administration2. Blood flow3. Surface area available4. Solubility of a drug5. Drug-drug interactions6. pH

Routes of administration
• The path by which a drug, fluid, poison, or other substance is taken into the body
• 4 types:1. Enteral2. Parentral 3. Inhalation 4. Others

1.enteral
• Desired effect is systemic,administration through GIT .Includes:
1. Oral The most common Include tablet,capsule syrup,suspension
What is the difference btw them? Advantage :
1. Good patient cmpliance2. Easy to take
Disadvantage :1. First pass metabolism

1.Alimentary
2. Buccal Between gum and cheeks Advantage:
1. Avoid first pass metabolism by passing directly into superior vena cava
Disadvantage :1. Not all drugs can formulated as it

1.Alimentary
3. Sublingual Under the tongue Advantage:
1. Avoid first pass metabolism by passing directly into superior vena cava
Disadvantage :1. Not all drugs can formulated as sublingual

1.Alimentary
4. Rectal Suppository ,fleet enema Advantage :
1. Useful when oral route is unavailable due to vomiting2. Less first pass effect than oral
Disadvantage :1. Patient compliance2. Inconvenient when patient has diarrhea

Routes of administration
1. Enteral 2. Parentral 3. Topical 4. Others

2. Parentral
• Desired effect is systemic, substance is given by routes other than the digestive tract
1. Intravenous Direct injection into the vascular system Advantage:
1. Rapid effect2. Potent 3. No first pass effect bec. 100% of the drug enter circulation
Disadvantage 1. Need specialized persons like you2. Painful

2. Parentral
2. Intramuscular (IM) Usually given in gluteus maximus Advantage :
1. More rapid than PO and less rapid than IV2. No first pass metabolism
Disadvantage :1. Painful

2. Parentral
3. Subcutaneous (SC) Like insulin injections


2. Parentral
4. Intrathecal Injection into the spinal subarachnoid space Advantage :
1. In cases of acute CNS infection and spinal anesthesia2. Avoid first pass metabolism
Disadvantage :1. Personal error may lead to disablity to walk

2. Parentral
5. Epidural injection– Injection of drugs through a catheter placed into
the epidural space– In your opinion which is safer epidural or
intrathecal?


Epidural injection

Routes of administration
1. Enteral 2. Parentral 3. Topical4. Others

Topical
• Substance is applied directly where its action is desired
• Like:– Inhalation – Ear drops – Eye drops – Creams – Ointments

Inhalation
• Commonly drugs that affect lung but there are exceptions
• Inhalers and nebulizers

5. Transdermal
• Medicated adhesive patch that is placed on the skin to deliver a specific dose of medication through the skin and into the bloodstream.

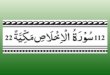
In what way does the pH of a drug affect the charge?
• Drugs are either weak acids or bases• Acidic drug are uncharged when protonated
HA H+ A-
NOT ABSORBED

In what way does the pH of a drug affect the charge?
• Basic drugs are charged when protonated
BH+ H+ B
NOT ABSORBED

CHARGE =
Not pass through site of administration
الحدود تعبر ال

pH 3 4 5 6 7 8 9 10 11
pH less than pKa pH more than pKa
Deprotonated forms A- and B predominate
Protonated forms HA and
BH+ predominate
pH=pKaHA=A-BH+=B

Bioavailability (BA)
• Fraction of administered drug that reach its site of action
• BA for IV =100%• BA for for a medication given as tablet is less
100%

Factors affect bioavailability
1. First –pass metabolism2. All factors that affect absorption

First pass metabolism
• Biotransformation that occurs before the drug reaches its site action
• Commonly occurs in liver• Also happens in other sites but to a lesser
extent like:1. Small intestine 2. Kidney

Bioequivalence
• the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of drug action when administered at the same molar dose under similar conditions in an appropriately designed study
• Panadol and sedamol are not bioeqivalent.what does that mean?

Distribution
• Process by which the drug leaves the bloodstream and enters the interstitium or the cells of the tissues

Types of transport
Transport
1-Passive transport
I-Simple diffusion
II-Facilitated diffusion
III-Filtration
IV-osmosis
2-Active transport

How the drug absorbed into the cells?
1. Simple diffusion– Concentration gradient• High conc. Low conc.
– No energy consumed– Most common mode of drug transport
2. Facilitated diffusion– Transport by special carrier proteins– No energy consumed
3. Active transport1. Need of protein2. Need energy ATP

Factors affect distribution
1. Blood flow 2. Capillary permeability3. Binding to plasma protein– Acidic drugs binds to albumin more efficiently than
basic ones – Ex:aminglycoside are basic drugs so their binding to
albumin is……………………
4. Drug structure– Lipophilic drugs cross cell membrane– Polar molecule doesn’t cross cell membrane

Biotransformation
• Lipophilic molecules modified to more polar molecule to enhance their elemination
• May activate or inactivate drugs• Composed of 2 phases– Phase I– Phase II

Phase I
lipophilic molecule
Polar molecule
OxidationReductionhydrolysis
May be active or inactive

Phase II
• Formation of covalent linkage between functional groups on the parent drug and another substrate
• Glucoronate , acetic acid ,glutathione,sulfate are major groups added
• Usually the drug become inactive

What is the main site of biotransformation?
• Liver
• Small intestine ,kidney play a little role


Where do these reaction occurs on a cellular level?
• Phase I reaction in cytochrome P450 system• Phase II reaction occurs in cytosol by group of
enzymes called transferases

Do phase II always follow phase I?
• Usually yes • There are few cases the drug will go through
phase II first like isoniazide

Factors affect biotransformation?
• Genetic difference• Induction of cytochrome P450 • Inhibition of cytochrome P450• Disease especially of the liver• Age and gender

Excretion
• Process by which a drug or metabolite is removed from body
• Major routes of excretion1. Renal » The most common routes of elemination» Acidification of urine enhance excretion of weak bases» What is the benefit?
2. Fecal 3. Respiration» Primarily for anesthetic gases and vapors
4. Breast milk» So not all drugs can be given to lactating women
5. Skin

What is the half life?
• Time needed to get rid of about one half of the drug
• Give us an indication about how many times the drug should be administered

Pharmacodynamics
• Action of the drug on body• Include:
1. Principles of receptor interaction2. Mechanisms of therapeutic and toxic action3. Dose-response relationship

Receptor interactions
• Receptor : Macromolecule typically made of proteins that interact with ligand or drug to make a physiological or pharmacological effect

Receptor families
G protein coupled
receptor
Enzyme linked
receptors
Ligand gated ion channel
Intracellular receptors
Spare receptors

Cell Surface Receptor Types:
1) Ligand-gated ion channel

Cell Surface Receptor Types:
2) G-Protein Coupled Receptor

Cell Surface Receptor Types:
3) Enzyme-linked Receptor eg Growth Factor Receptors

Drugs
Agonist Partial agonist Antagonist
Competitive Non-competitive

What is an agonist?
• Drug binds to and activates receptor– Scopolamine = muscuranic agonist
• Partial agonist– A drug which does not produce maximal effect
even when all of the receptors are occupied– Clomiphene partial agonist to estrogen receptors

What is antagonist?
• Antagonist– Inhibit or block responses caused by agonists– Atenolol is B1 blocker
• Competitive antagonist– Competes with an agonist for receptors– High doses of an agonist can generally overcome
antagonist

• Noncompetitive antagonist– Binds to a site other than the agonist-binding
domain– Induces a conformation change in the receptor
such that the agonist no longer “recognizes” the agonist binding site.
– High doses of an agonist do not overcome the antagonist in this situation

• Irreversible Antagonist– Bind permanently to the receptor binding site
therefore they can not be overcome with agonist

Dose response relationship

Dose response relationship
Graded
Efficacy Potency
Quantal
Effective dose Toxic dose Therapeutic
index

1. Graded dose response relationship
• As the concentration of the drug increases the magnitude of pharmacologic effect also increases
• The response is graded effect– Means that the response is continuous and gradual– The opposite of quantal which means all or nothing
response • The graph of this relationship is drawn by
blotting the magnitude of response against concentration of the drug

Rectangular hyperbola curve
Drug concentration
Biological effect

Graded response relationship determines two important properties :
1. Efficacy– Degree to which a drug is able to produce the
desired response– More efficacy=more therapeutically beneficial
2. Potency– Amount of drug required to produce 50% of the
maximal response the drug is capable of inducing– Used to compare compounds within classes of
drugs

Example

2-Quantal dose response relationship
• It describes the relationship btw the magnitude of the dose on the portion of population that responds
• It is all or none response– Patient may have response or not
• Useful in determining doses to most the population responds
• We determine 4 properties from it:– ED50– TD50– LD50– TI

Definitions• Effective Concentration 50% (ED50)– Concentration of the drug which induces a specified
clinical effect in 50% of subjects
• Lethal Dose 50% (LD50)– Concentration of the drug which induces death in 50%
of subjects– Used only in clinical studies on animals
• Toxic dose 50%(TD50)– Concentration of the drug which induces toxic effects in
50% of subjects

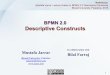
Definitions• Therapeutic Index–Measure of the safety of a drug –Calculation: TD50/ED50
• The larger TI the safer the drug
• The smaller TI the the more toxic

Dose-Response Relationship
• Drug induced responses are not an “all or none” phenomenon
• Increase in dose may:– Increase therapeutic response– Increase risk of toxicity

Therapeutic index
Drug concentration
Percentage of pts

Determining therapeutic index PE
RCEN
TAG
E O
F PA
TIEN
TS
LOG Drug concentration in plasma
TD50=10

• Drug A has Therapeutic index <1 is it safe ?

Examples :High therapeutic index drugs Low therapeutic index drugs
NSAID’s:Paracetamol,Ibuprofen Digoxin
Most antibiotics :penicillin Theophyllin
Beta blockers Warfarin
Multivitamins (except vit A ) Aminoglycosides
Immunosuppresive patients
Phenytoin ,phenobarbital

What must we do for these drugs having low therapeutic index?
• We must do therapeutic drug monitoring

REMEMBERNo drug produces a
single effect!!!