Embed Size (px)
Citation preview

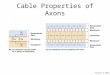
IntroductionMultiple Sclerosis (MS) is a chronic inflammatory disease characterized by the demyelization of axons within the central nervous system (CNS). Up to 75% of MS patients are reported to experience cognitive impairment (Pierson & Griffith, 2006), with the most commonly affected domains being processing speed, memory, and attention (Wallin, Wilken, & Kane, 2006). The 3-second version of the Paced Auditory Serial Addition Task (PASAT) was included as the lone measure of cognition within the Multiple Sclerosis Functional Composite (Snyder, Cappelleri, Archibald, & Fisk, 2001; Fischer, Jak, Kniker, Rudick, & Cutter, 2001). The PASAT is generally recognized as a measure of processing speed, working memory, and sustained auditory attention.
The PASAT has been shown to be highly accurate in identifying cognitive impairment in individuals with MS (Rosti, Hamalaien, Koivisto, & Hokkanen, 2007). However, the PASAT has been criticized as being a “highly sensitive but non-specific test” that has notable potential to identify non-impaired individuals as cognitively impaired, potentially due to “the wide network of neural systems (the anterior cingulate, frontal, superior temporal, and parietal cortices, cerebellum, and white matter tracts connecting them) shown to be activated during the PASAT performance” (Rosti, Hämäläinen, Koivisto, & Hokkanen, 2007, p. 109). The PASAT also may put individuals with speech or language impairment at a disadvantage, may penalize individuals who speak slowly for any reason, and is influenced by IQ (Tombaugh, 2006). An additional criticism of the PASAT is that mathematical ability may strongly influence PASAT scores (Chronicle & MacGregor, 1998; Rosti et al., 2007; Tombaugh, 2006).
The purpose of the current study was to examine the validity of the PASAT by comparing test scores to the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Randolph, 1998).
Results and SummaryCorrelations among the two measures of the PASAT and RBANS composites ranged from .141 to .490. The two and three second versions of the PASAT were significantly correlated with the Attention composite of the RBANS (.353 and .490). The two-second version of the PASAT was also positively correlated with the RBANS Delayed Memory and Total Scale composites. Linear regression indicated the 3-second version of the PASAT predicted a significant proportion of the variance in the Attention composite (R2=.125; p=.017).
The RBANS has been shown to identify cognitive impairments in patients with MS (Davis et al., 2007) and is a well-validated measure. Although questions have been raised about the PASAT’s utility and validity for working with patients with MS, the results of the current study suggest that both the 2 and 3 second version provide a good measure of attention. Analysis of the subtests which comprise the RBANS index suggested that Coding was more responsible for the correlation with both versions of the PASAT as compared to Digit Span; this was unexpected as the PASAT and Digit Span are both measures of auditory attention. Perhaps the increased complexity of the Coding subtest (e.g., also measures incidental learning) is more reflective of the cognitive load of the PASAT. Interestingly, the 3-second version seems to also be a measure of delayed memory which stands to reason given the more complex nature of the task and the higher demand placed on the memory systems. However, as multiple studies have suggested that long-term memory may be impaired in patients with MS (e.g., Davis et al., 2007) caution should be exercised when interpreting the 3-second version of the PASAT as solely a measure of attention. The results of this study further suggest that long-term memory should be thoroughly assessed in this population especially when attention deficits are present.
Future studies should investigate this relationship in other clinical populations as well as healthy individuals.
ReferencesChronicle, E. P. & MacGregor, N. A. (1998). Are PASAT scores related to mathematical ability?. Neuropsychological Rehabilitation, 8(3), 273-282.
Davis, A. S., Finch, W. H., Williams, R. N., Gupta, A. S., Randolph, C., Pass, L. A., & Whited, R. (May, 2007). Classification and regression tree analysis of neurocognitive functioning in patients with and without multiple sclerosis . Poster presented at the 21st Annual Meeting of the Consortium of Multiple Sclerosis Centers, Washington, D. C.
Fischer, J. S., Jak, A. J., Kniker, J. E., Rudick, R. A., & Cutter, G. (2001). Multiple Sclerosis Functional Composite: Interpretation and scoring manual. Retrieved from: http://www.nationalmssociety.org/for-professionals/researchers/clinical-study-measures/msfc/download.aspx?id=259
Pierson, S. H. & Griffith, N. (2006). Treatment of cognitive impairment in multiple sclerosis. Behavioral Neuropsychology, 17, 53-67.
Randolph, C., Tierney, M. C., Mohr, E., & Chase, T. N. (1998). The repeatable battery for the assessment of neuropsychological status (RBANS): Preliminary clinical validity. Journal of Clinical and Experimental Neuropsychology, 20(3), 310-319.
Rosti, E., Hämäläinen, P., Koivisto, K., & Hokkanen, L. (2007). PASAT in detecting cognitive impairment in relapsing-remitting MS. Applied Neuropsychology, 14(2), 101-112.
Snyder, P. J., Cappelleri, J. C., Archibald, C. J., & Fisk, J. D. (2001). Improved detection of differential information-processing speed deficits between two disease-course types of multiple sclerosis. Neuropsychology, 4, 617-625.
Tombaugh, T. N. (2006). A comprehensive review of the Paced Auditory Serial Addition Task (PASAT). Archives of Clinical Neuropsychology, 21, 53-76. doi: 10.1016/j.acn.2005.07.006
Wallin, M. T., Wilken, J. A., & Kane, R. (2006). Cognitive dysfunction in multiple sclerosis: Assessment, imaging, and risk factors. Journal of Rehabilitation Research and Development, 43(1), 63-72. doi: 10.1682/JRRD.2004.09.0120
Presented at the 29th Annual Conference of the National Academy of Neuropsychology
Contact for Correspondence: [email protected]
MethodologyParticipants were 45 patients diagnosed with MS (mean age 44.58 years, SD = 8.69 years). Mean time since diagnosis was 7.16 years (SD=7.06). Mean EDSS score was 2.86 (SD=1.70). Participants completed the PASAT and Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) as part of a comprehensive neuropsychological assessment.
Correlations
* Significant at the .01 level
RBANS Composite
3-s PASAT 2-s PASAT
Immediate Memory
.239 .279
Visual-Spatial/ Construction
.257 .141
Language .245 .213
Attention .490* .353*
Delayed Memory
.314* .167
Total Score .402* .260
Mean S.D.
3-s PASAT 38.33 10.36
2-s PASAT 27.73 8.46
Immediate Memory
87.67 16.56
Visual-Spatial/ Construction
93.96 14.24
Language 92.84 9.60
Attention 83.16 19.17
Delayed Memory 87.62 18.09
Total Score 85.18 15.25