Embed Size (px)
Citation preview

Introduction to Chronic PainDefinitions and Pathophysiology
Rachael Rzasa Lynn, MD4 November 2015

Definition of Chronic Pain
• Pain that persists past the normal time of healing– Variable: less than 1 month to more than
6 months• Typically use 3 months as the point of
transition from acute to chronic pain – Six months is more often used in research
IASP Classification of Chronic Pain, Second Edition (Revised), http://www.iasp-pain.org/files/Content/ContentFolders/Publications2/ClassificationofChronicPain/Introduction.pdf

Pathogenesis of Chronic Pain
Marcus DA. Am Fam Physician. 2000; 61:1331-8)

Nociceptive and Acute Pain
• Reflects actual or imminent tissue injury• Can result in hypersensitivity as part of the
normal healing process in order to promote guarding/protection of the injured tissue
eg, sunburn• This pain can become more persistent and
chronic via both peripheral and central mechanisms

Nociceptors• Neurons that detect intense stimuli
– Mechanical– Thermal– Chemical Transduced into electrical signals
• Most are polymodal
• 2 major classes– Aδ-fibers
• Medium-diameter, myelinated detect well-localized, first, fast pain
– C-fibers• Small-diameter, unmyelinated
poorly localized, second, “slow” pain
• Pseudounipolar = Bidirectional• Ca++-dependent release of transmitters at the central terminal• Ca++-dependent release of neurogenic inflammatory molecules (CGRP, Substance P) that influence the peripheral tissue milieu
– Only peripheral terminal can respond to mechanical/temperature, but both terminals can respond to endogenous chemical signals
– Different fiber types project to distinct lamina within the spinal cord dorsal horn (DH)• lamina I & II receive primarily nociceptive input via Aδ and C-fibers of different sub-classes• lamina III & IV receive non-nociceptive, innocuous input via Aβ fibers• lamina V contains the Wide Dynamic Response (WDR) neurons that receive input from a variety of classes such that they respond to
a wide variety of stimulus intensities ranging from innocuous to noxious via Aβ, Aδ and C-fiber input– These also commonly receive visceral input, which likely contributes to referred pain (injury to visceral tissue is referred to somatic location)
Basbaum et al. Cell 2009; 139: 267-284

Supraspinal pathways in nociception
• Involves multiple levels of of brain structures:• brainstem (medulla, pons, midbrain)• diencephalon (thalamus, hypothalamus)• primary and secondary somatosensory
cortices• fronto-limbic circuits (prefrontal cortex [PFC],
anterior cingulate cortex, insula, amygdala, hippocampus)

Nociceptive Pathways
• Spinothalamic tract important for discriminitive aspects of pain– Where, how intense
• Spinoreticulothalamic tract more relevant for poorly localized pain
• Parabrachial region of the pons communicates with amygdala
= affective experience of pain
Basbaum et al. Cell 2009; 139: 267-284

Reduced descending inhibition• Midbrain and medullary structures control nociception (↑ & ↓)
– Periaqueductal gray (PAG) receives inputs from higher brain centers descending, inhibitory, analgesic effect• Via endogenous opioids
– Rostroventromedial medulla (RVM) can enhance or inhibit nociceptive input• Connects with PAG• inputs from the thalamus, parabrachial region and locus coeruleus
(norepinephrine)– LC and pontine nuclei exert descending inhibitor NE signals on dorsal horn– Activating spinal α2 adrenergic receptors is analgesic
• Includes nucleus raphe magnus (serotonin), the nucleus reticularis gigantocellularis-pars alpha and the nucleus paragiganto-cellularis lateralis (serotonin)
• Dysregulation of this inhibitory input may promote chronic pain
Ossipov MH et al. Curr Opin Support Palliat Care. 2014;8:143-51

Supraspinal changes in pain
• Chronic pain states can be associated with cortical changes. – Supraspinal regions involved
(either increased excitation or↓d gray matter) in chronic pain/plasticity include: • somatosensory cortex, PFC
(particularly dorsolateral prefrontal cortex), insula, thalamus and the cingulate cortex

TRP: Transient receptor potential channel (many subtypes)
TRPA1=cold (<15°C) in injury (not normal, acute cold), menthol
TRPM8=cold(<25°C), mentholTRPV1=heat (>43°C), capsaicin
ASICs: Acid-sensing ion channelsKCNK: Potassium channel subtypesNav: Voltage-gated sodium channel isoformsAlso Voltage-gated Calcium channels (N- and T-type);
α2δ subunit ↑’d after injuryMechanical transduction may occur via TRP,
ASIC and/or KCNK channelsGrace PM, et al. Nat Rev Immunol. 2014; 14: 217-231Basbaum et al. Cell 2009; 139: 267-284

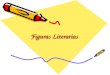
Mechanistic Stratification of Medications Used to Treat Neuropathic Pain
Fig. 4. Mechanistic stratification of antineuralgic agents. PNS = peripheral nervous system; CBZ = carbamazepine; OXC = oxcarbazepine; PHT = phenytoin; TPM = topiramate; LTG = lamotrigine; TCA = tricyclic antidepressant; NE = norepinephrine; SSRI = selective serotonin re-uptake inhibitor; SNRI = serotonin and norepinephrine re-uptake inhibitor; GBP = gabapentin; LVT = levetiracetam; NMDA = N-methyl-D-aspartate; NSAID = nonsteroidal anti-inflammatory drug.
Beydouna & Backonja M. J Pain Symptom Manage. 2003;25:S18-30

Persistent Pain: Sensitization• The differences between acute and chronic pain reflect neuronal plasticity• Usually due to inflammatory changes in the neuron environment
– Tissue damage accumulation of endogenous factors released by activated nociceptors or non-neural cells (eg, mast cells, basophils, platelets, Mθ, PMNs, endothelial cells, keratinocytes, fibroblasts)• neurotransmitters• peptides (substance P, CGRP, bradykinin)• eicosinoids and lipids such as prostaglandins, thromboxanes, leukotrienes, endocannabinoids• Neurotrophins (eg, NGF)• cytokines (such as IL-1β, IL-6 and TNF-α) and chemokines• Proteases• H+
– Nociceptors have receptors for these molecules (TRPA1, TRPV1, TrkA, ASICs, etc.) increased excitability pro-inflammatory and pro-algesic!• Targeting these receptors should reduce pathological (inflammatory) pain without inhibiting normal nociception
• Sensitization is a unique feature of nociceptors– Increase in nociceptor excitability = increased response to stimulus– Reduced threshold for activation and sometimes development of spontaneous activity– Responsible for primary hyperalgesia (eg, sunburn)– Triggers increased excitability in central neurons within the pain pathway= Central Sensitization
Basbaum et al. Cell 2009; 139: 267-284

Central Sensitization
• 3 major proposed pathways– Glutamate/NMDA-mediated hypersensitivity– Loss of inhibitory controls– Glia-neuron interactions• Microglia and astrocytes

Central Sensitization: Glutamate/NMDA
• Glu = excitatory neurotransmitter (NT)– Released from central terminal of nociceptors to
stimulate 2nd order dorsal horn neuron• Primarily AMPA & kainate Glu receptors (ion channels)
– Summation of many inputs results in action potential
• NMDA normally quiet BUT– In tissue injury, increased neurotransmitter release results in
depolarization that activates NMDA receptors Ca++ influx strengthened connection btwn nociceptor and pain-transmitting DH neuron heightened response to noxious stimuli = hyperalgesia» Also, innocuous inputs around the site of injury become painful =
allodynia• Now Aβ (normally light touch) activate pain transmission
circuits

Central Sensitization:Loss of Inhibitory Control
• GABA and glycine (gly) = inhibitory NT– Normally tonically active• When experimentally blocked hypersensitivity
behavior• Decreased activity with peripheral injury thus
enhanced excitation of spinal 2nd order neurons increased activity in response to both painful (hyperalgesia) and non-painful (allodynia) stimuli

Central Sensitization:Glia-Neuron Interaction
• Microglia are MΘ resident within CNS– Signal injury or infection within CNS
– Immune activity involved in sickness response (lethargy, depression, anxiety) associated with illness and also chronic pain
– Following peripheral nerve injury (but NOT inflammatory tissue injury) they accumulate in the superficial DH where the injured nerve terminates (and also surround and damage adjacent motorneurons)• Activated release inflammatory signals (TNF-α, IL-1β, IL-6) sensitization of central neurons and maintenance of pain
Grace PM, et al. Nat Rev Immunol. 2014; 14: 217-231
Basbaum et al. Cell 2009; 139: 267-284

Central Sensitization:Glia-Neuron Interaction
• Physical damage of peripheral afferent results in release of signals detected by microglia– ATP microglial P2-purinergic receptors (P2Xn)
• May ultimately result in decreased GABA-ergic inhibition and thus increased excitability
– Other neuronally released cytokines and chemokines (eg, CX3CL1) that activate the microglia when their receptors (CX3CR1) are bound• May be part of a positive-feedback loop
» microglia produce the protein that frees CX3CL1 from neuronal cell surface
– Glia are activated not just in spinal cord but also in the brainstem, contributing to facilitation of pain processing at supraspinal levels
Grace PM, et al. Nat Rev Immunol. 2014; 14: 217-231
Basbaum et al. Cell 2009; 139: 267-284

Central Sensitization:Glia-Neuron Interaction
• Toll-Like Receptors (TLR2 and TLR4)– Innate immune receptors that respond to diverse pathogens
and pathogen- or damage-associated molecular patterns (PAMPs & DAMPs) as well as endogenous signals such as IL-1b, TNFα, IL-6 and nitric oxide
– Activation of TLRs results in immune-like processes, such as the release of pro-inflammatory (and neuroexcitatory) cytokines and phagocytosis• Exposure to DAMPs may increase glial expression of P2X receptors
increased neuronal excitability• Development of nociceptive hypersensitivity correlates temporally
with increased TLR4 expression after injury– Sensory neurons themselves may express TLRs and adaptor proteins
Milligan and Watkins Nat Rev Immunol. 2009; 10: 23-36
Grace PM, et al. Nat Rev Immunol. 2014; 14: 217-231

Central Sensitization:Glia-Neuron Interaction
• Glia may become “primed” following stress, aging, illness or injury such that subsequent injury leads to unregulated activation that maintains central sensitization and leads to chronic pain• Opioids like morphine (and its “inactive” metabolites)
activate TLR4 resulting in such priming and central sensitization, which actually opposes analgesia!– This non-opioid receptor activity is also implicated in opioid
reward, craving and withdrawal– As well as opioid-induced hyperalgesia

Summary
• Complex changes in both pain sensation, transmission and processing lead to chronic pain– Peripheral– Central• Spinal Cord• Supraspinal structures