Embed Size (px)
Citation preview
9/19/17
1
IntroductiontoEvidenceBasedMedicine
ChaisiriAngkurawaranonDepartmentofFamilyMedicine
Outline
1.Introduction:whatisEBM2.Thestepsinevidencebasedpractice3.Anexample4.Reflectionandfurtherinformation
Question:Whichisit?AorB
AThedoctor istheretogivethepatients alltheinformationthatthepatientneedsinorderthatthepatient canmakeadecision,andthedoctorshouldthenimplementthatdecisiononcethepatient hasmadeit
BThepatient istheretogivethedoctor alltheinformationthatthedoctorneedsinorderthatthedoctor canmakeadecision,andthepatientshouldthenimplementthatdecisiononcethedoctor hasmadeit
Wewillcomebackattheendofclass
WhyEBM
• A21st centuryclinicalwhocannotcriticallyreadastudyisasunpreparedasonewhocannottakeabloodpressureorexaminethecardiovascularsystem
Evidencebasedmedicineandthemedicalcurriculum.BMJ2008:337:704-705
EvidenceBasedMedicine EBM
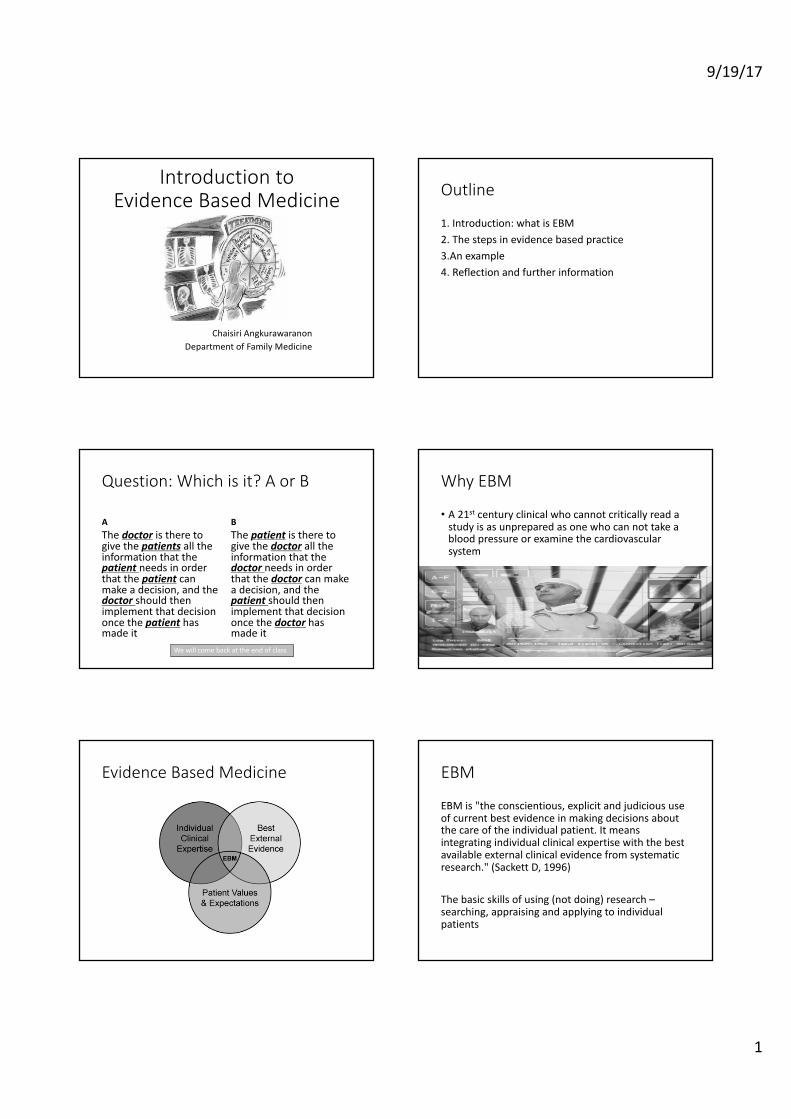
EBMis"theconscientious,explicitandjudicioususeofcurrentbestevidenceinmakingdecisionsaboutthecareoftheindividualpatient.Itmeansintegratingindividualclinicalexpertisewiththebestavailableexternalclinicalevidencefromsystematicresearch."(Sackett D,1996)
Thebasicskillsofusing(notdoing)research–searching,appraisingandapplyingtoindividualpatients
9/19/17
2
EBM
• EBMistheintegrationofclinicalexpertise,patientvalues,andthebestevidenceinto thedecisionmakingprocessforpatientcare.
• Clinicalexpertisereferstotheclinician'scumulatedexperience,educationandclinicalskills.
• The patientbringstotheencounterhisorherownpersonalanduniqueconcerns,expectations,andvalues.
• Thebestevidenceisusuallyfoundinclinicallyrelevantresearchthathasbeenconductedusingsoundmethodology.(Sackett D,2002)
Example1
• Apatientcometotheclinicwithfreshdogbite• Itlooksclean• Itisnecessarytogiveprophylacticantibiotics
Yes
No
Example1
• Ametaanalysisindicatedthattheaverageinfectionratefordogbiteswas14%andthatantibioticshalvedtherisk
• Wouldyougiveprophylacticantibiotic
CummingsP(1994)Antibioticstopreventinfectioninpatientswithdogbitewounds:Ameta-analysisofrandomizedcontroltrials.AnnalsofEmergencyMedicine23:533-40
Whatskillsareneededforacliniciantotoapplysuchevidence?
2.StepsinEBM
• 2.1Formulateananswerablequestion--ASK• 2.2Trackdownthebestevidenceofoutcomesavailable-- ACQUIRE
• 2.3criticallyappraisetheevidence(howgoodandwhatitmeans)– APPRAISE
• 2.4applytheevidence-- APPLY• Results+clinicalexpertise+patientvalues
• 2.5Assessoutcome- ASSESS
Exercise
• Insmallgroups:• Writedownsomeclinicalquestionsorproblemsthatyouthinkadoctormayface
• Don’tthinktoohard• Canuseyourownexperienceorfamilyexperience
http://www.mathgoodies.com/calculators/random_no_custom.html
CommonTypesofclinicalQuestion
Question Questiontype
WhatshouldIdoaboutthis conditionorproblem Intervention
Whatisthecause oftheproblem Aetiology andriskfactors
Doesthisperson havetheconditionorproblem? Diagnosis
Whowillgettheconditionorproblem Prognosticandprediction
Howcommonisthe problem Frequencyandrate
Whatarethetypes ofproblems Phenomenaorthoughts
9/19/17
3
Backgroundquestions
• Asked for general knowledge about a disorder• Has two essentials components:
• a question root ( who, what, where, how, why) with a verb
• a disorder
Backgroundquestions
• WhatarethesymptomsandsignsofsomeonepresentingwithMI?
• WhatarethediagnosistestsforMI?• WhatarethecausesofMI?• WhatarethetreatmentsforMI• Textbooks answer background questions, they
contain collected & synthesized wisdom for topics that do not change often.
Clinicalquestions(Foregroundquestions)◆Knowyourbackground◆Askedforspecific knowledgeaboutmanagingpatientswithadisorder
◆Ithas4components(PICO analysis):P - Patient/PopulationI- InterventionC- ComparisonO - Outcome
Step ins EBM
1.Formulate an answerable question - ASK
PICOPrinciple Description
Population Therelevent peopleinrelationtotheclinicalproblem
Intervention(orindicatororindextest)
Intervention, exposureortestthatyouwanttofindoutaboutinrelationtotheclinicalproblem
Comparator Thealternative, controlstrategy,exposureortestforcomparisonwiththeoneyouareinterestedint
Outcome Whatyouoryourpatientisconcernedabouthappening (ornothappening)
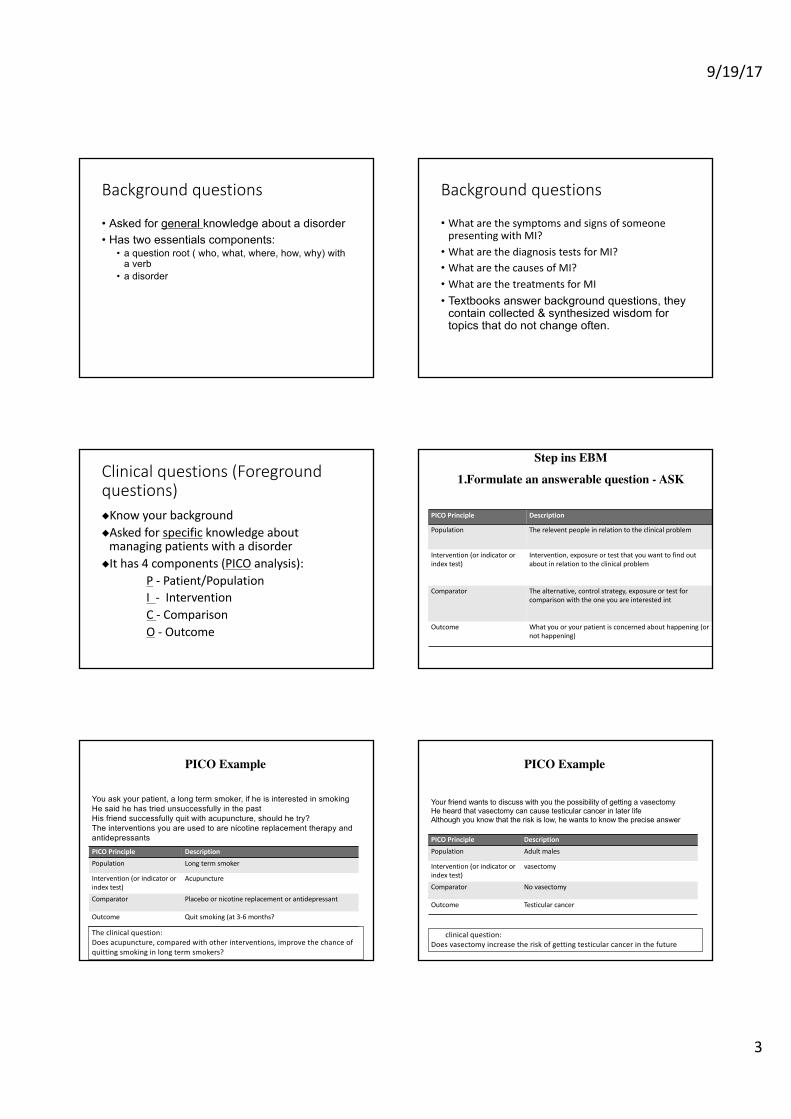
PICO Example
You ask your patient, a long term smoker, if he is interested in smokingHe said he has tried unsuccessfully in the pastHis friend successfully quit with acupuncture, should he try?The interventions you are used to are nicotine replacement therapy and antidepressantsPICOPrinciple DescriptionPopulation Longtermsmoker
Intervention(orindicatororindextest)
Acupuncture
Comparator Placebo ornicotinereplacementorantidepressant
Outcome Quitsmoking(at3-6months?
Theclinicalquestion:Doesacupuncture,comparedwithotherinterventions,improvethechanceofquittingsmokinginlongtermsmokers?
PICO Example
Your friend wants to discuss with you the possibility of getting a vasectomyHe heard that vasectomy can cause testicular cancer in later lifeAlthough you know that the risk is low, he wants to know the precise answer
PICOPrinciple DescriptionPopulation Adultmales
Intervention(orindicatororindextest)
vasectomy
Comparator Novasectomy
Outcome Testicularcancer
Theclinicalquestion:Doesvasectomyincreasetheriskofgettingtesticularcancerinthefuture?
9/19/17
4
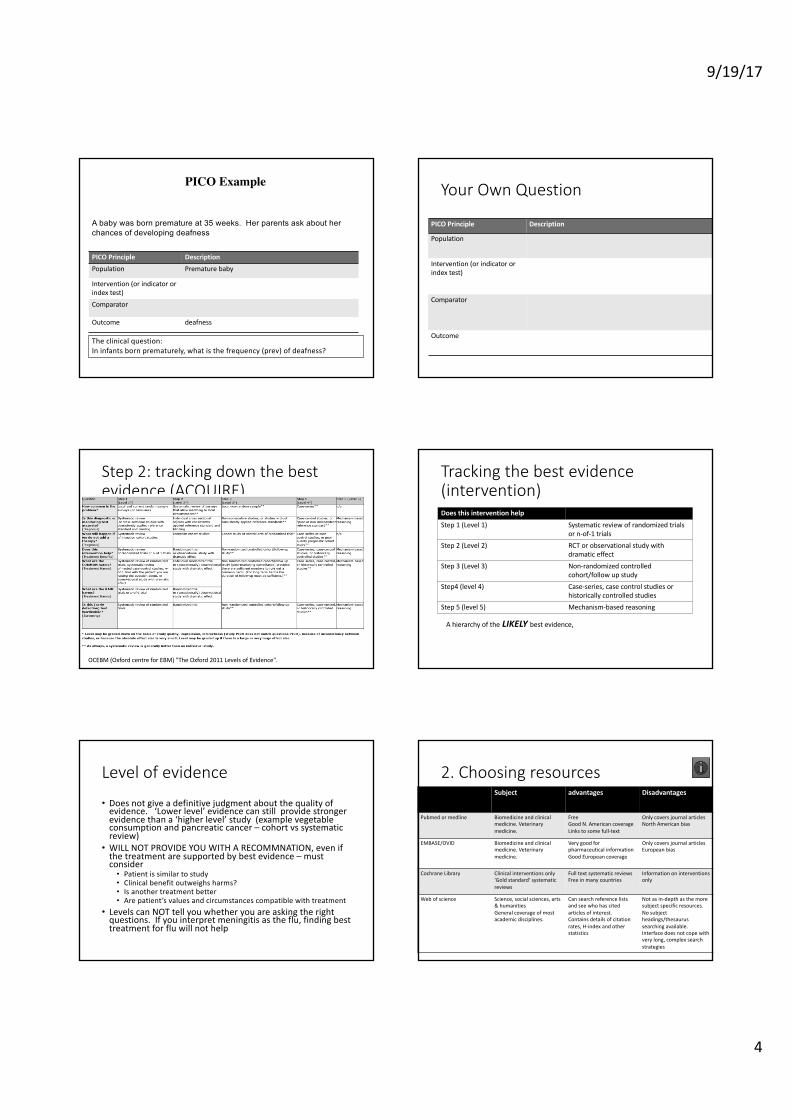
PICO Example
A baby was born premature at 35 weeks. Her parents ask about her chances of developing deafness
PICOPrinciple DescriptionPopulation Prematurebaby
Intervention(orindicatororindextest)Comparator
Outcome deafness
Theclinicalquestion:Ininfantsbornprematurely,whatisthefrequency(prev)ofdeafness?
YourOwnQuestion
PICOPrinciple Description
Population
Intervention(orindicatororindextest)
Comparator
Outcome
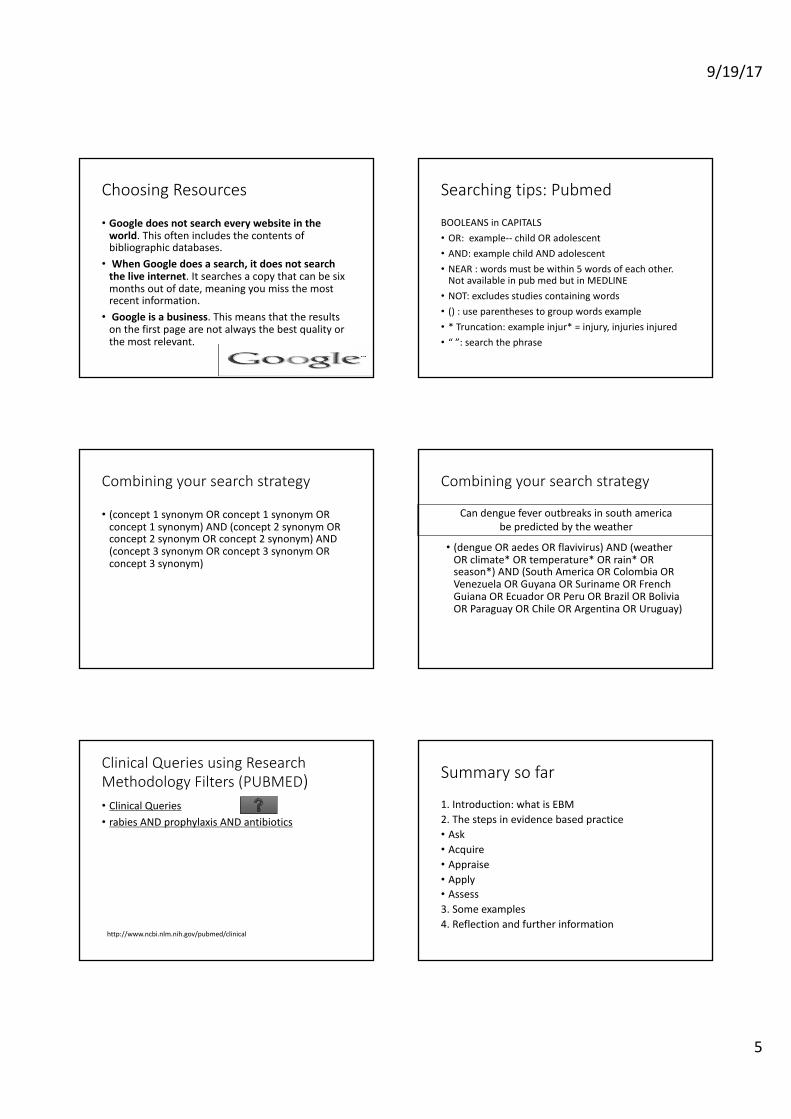
Step2:trackingdownthebestevidence(ACQUIRE)
OCEBM(Oxfordcentre forEBM)"TheOxford2011LevelsofEvidence".
Trackingthebestevidence(intervention)DoesthisinterventionhelpStep1(Level1) Systematicreviewofrandomized trials
orn-of-1trialsStep 2(Level2) RCT orobservationalstudywith
dramaticeffectStep 3(Level3) Non-randomizedcontrolled
cohort/follow upstudyStep4 (level4) Case-series, casecontrolstudiesor
historicallycontrolledstudiesStep5(level5) Mechanism-basedreasoning
Ahierarchyofthe LIKELYbestevidence,
Levelofevidence
• Doesnotgiveadefinitivejudgmentaboutthequalityofevidence.‘Lowerlevel’evidencecanstillprovidestrongerevidencethana‘higherlevel’study(examplevegetableconsumptionandpancreaticcancer– cohortvs systematicreview)
• WILLNOTPROVIDEYOUWITHARECOMMNATION,evenifthetreatmentaresupportedbybestevidence– mustconsider
• Patientissimilartostudy• Clinicalbenefitoutweighsharms?• Isanothertreatmentbetter• Arepatient’svaluesandcircumstancescompatiblewithtreatment
• LevelscanNOTtellyouwhetheryouareaskingtherightquestions.Ifyouinterpretmeningitisastheflu,findingbesttreatmentforfluwillnothelp
2.ChoosingresourcesSubject advantages Disadvantages
Pubmed ormedline Biomedicineandclinicalmedicine.Veterinarymedicine.
FreeGoodN.AmericancoverageLinkstosomefull-text
OnlycoversjournalarticlesNorthAmericanbias
EMBASE/OVID Biomedicineandclinicalmedicine.Veterinarymedicine.
VerygoodforpharmaceuticalinformationGoodEuropeancoverage
OnlycoversjournalarticlesEuropeanbias
CochraneLibrary Clinicalinterventionsonly‘Goldstandard’systematicreviews
FulltextsystematicreviewsFreeinmanycountries
Informationoninterventionsonly
Webofscience Science,socialsciences,arts&humanitiesGeneralcoverageofmostacademicdisciplines.
Cansearchreferencelistsandseewhohascitedarticlesofinterest.Containsdetailsofcitationrates,H-indexandotherstatistics
Notasin-depthasthemoresubjectspecificresources.Nosubjectheadings/thesaurussearchingavailable.Interfacedoesnotcopewithverylong,complexsearchstrategies
9/19/17
5
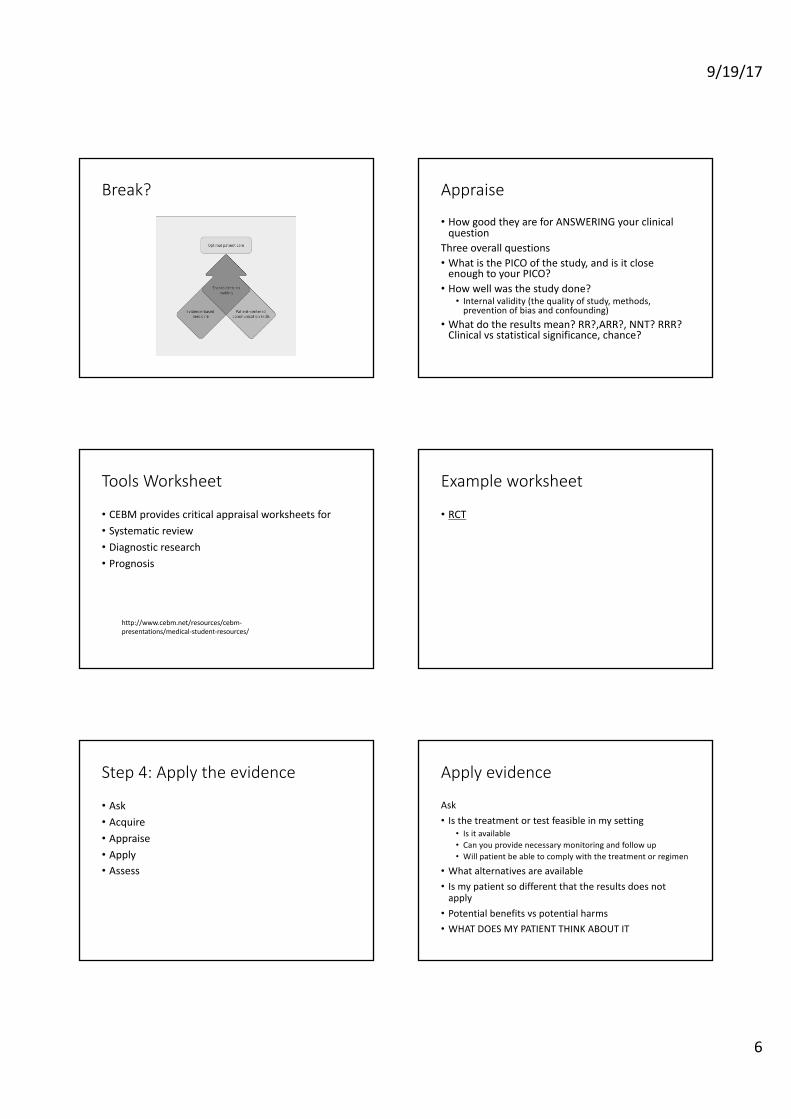
ChoosingResources
• Googledoesnotsearcheverywebsiteintheworld.Thisoftenincludesthecontentsofbibliographicdatabases.
• WhenGoogledoesasearch,itdoesnotsearchtheliveinternet.Itsearchesacopythatcanbesixmonthsoutofdate,meaningyoumissthemostrecentinformation.
• Googleisabusiness.Thismeansthattheresultsonthefirstpagearenotalwaysthebestqualityorthemostrelevant.
Searchingtips:Pubmed
BOOLEANSinCAPITALS• OR:example-- childORadolescent• AND:examplechildANDadolescent• NEAR:wordsmustbewithin5wordsofeachother.NotavailableinpubmedbutinMEDLINE
• NOT:excludesstudiescontainingwords• ():useparenthesestogroupwordsexample• *Truncation:exampleinjur*=injury,injuriesinjured• “”:searchthephrase
Combiningyoursearchstrategy
• (concept1synonymORconcept1synonymORconcept1synonym)AND(concept2synonymORconcept2synonymORconcept2synonym)AND(concept3synonymORconcept3synonymORconcept3synonym)
Combiningyoursearchstrategy
• (dengueORaedes ORflavivirus)AND(weatherORclimate*ORtemperature*ORrain*ORseason*)AND(SouthAmericaORColombiaORVenezuelaORGuyanaORSurinameORFrenchGuianaOREcuadorORPeruORBrazilORBoliviaORParaguayORChileORArgentinaORUruguay)
Candenguefeveroutbreaksinsouthamericabepredictedbytheweather
ClinicalQueriesusingResearchMethodologyFilters(PUBMED)• ClinicalQueries• rabiesANDprophylaxisANDantibiotics
http://www.ncbi.nlm.nih.gov/pubmed/clinical
Summarysofar
1.Introduction:whatisEBM2.Thestepsinevidencebasedpractice• Ask• Acquire• Appraise• Apply• Assess3.Someexamples4.Reflectionandfurtherinformation
9/19/17
6
Break? Appraise
• HowgoodtheyareforANSWERINGyourclinicalquestion
Threeoverallquestions• WhatisthePICOofthestudy,andisitcloseenoughtoyourPICO?
• Howwellwasthestudydone?• Internalvalidity(thequalityofstudy,methods,preventionofbiasandconfounding)
• Whatdotheresultsmean?RR?,ARR?,NNT?RRR?Clinicalvs statisticalsignificance,chance?
ToolsWorksheet
• CEBMprovidescriticalappraisalworksheetsfor• Systematicreview• Diagnosticresearch• Prognosis
http://www.cebm.net/resources/cebm-presentations/medical-student-resources/
Exampleworksheet
• RCT
Step4:Applytheevidence
• Ask• Acquire• Appraise• Apply• Assess
Applyevidence
Ask• Isthetreatmentortestfeasibleinmysetting
• Isitavailable• Canyouprovidenecessarymonitoringandfollowup• Willpatientbeabletocomplywiththetreatmentorregimen
• Whatalternativesareavailable• Ismypatientsodifferentthattheresultsdoesnotapply
• Potentialbenefitsvs potentialharms• WHATDOESMYPATIENTTHINKABOUTIT
9/19/17
7
IncorporatePatientvaluesSimplecommunicationprocess• Explainwhatwouldhappenwedidnothing• Explainwhattheoptionsare(feasibility,risk,benefit)
• Checkthepatient’sexpectationsandideas
StepsinEBM
5.Assess• Followupthepatientandassessmentofoutcomesafterimplicationoftreatment
Outline
1.Introduction:whatisEBM2.Thestepsinevidencebasedpractice(5A’s)3.Someexamples4.Reflectionandfurtherinformation
Example
• Mr.ShaspoorlymanageTypeIIdiabetesandaskiftakingcinnamonwouldimproveherfastingbloodglucose
• Task1:Asking-- DefinePICO• Task2:Acquire--definesimplesearchterms
Searching Thestudy
• LeachMJ,KumarS.Cinnamonfordiabetesmellitus.CochraneDatabase ofSystematicReviews2012,Issue9
• Thisarticlesystematicallyreviewedpapersinvestigatingwhethercinnamonaffecteddiabeticmanagement,usingfastingbloodglucoseasitsprimaryoutcome.
• Thepaper’srecentpublicationsuggeststhatthelatestevidencecollectedwillhavebeenincludedintheirreview.
• ThemeanagerangeofparticipantsintrialsreviewedincludedthatofMissS.
9/19/17
8
AppraisalTheauthors’search: 14searchengineswereusedtofindrelevantpapers,including:• – TheCochraneLibrary(issue12,2011).– MEDLINE(untilJanuary2012).– EMBASE(untilJanuary2012).
Selection:– 2reportersindependentlyscannedtheabstractofeverypaperretrievedbythe searchtoensureinclusioncriteriaweremet:• Randomised controlledtrials• Orallyadministeredmonopreparations ofcinnamon• Placebo/activemedication/notreatment.• TypeIorIIdiabetes– Potentiallimitation–onlypaperspublishedinEnglishwereselected.Pertinentreportspublishedinotherlanguagesmayhavebeenmissed.
Appraisal
RANDOMISATION• 10 prospective, parallel-group design, randomised control trials, involving a
total of 577 participants with either Type 1 or 2 diabetes were included. • 1 of the 10 studies didn’t use a placebo control.• 6 studies were double-blinded, 2 single-blinded and 2 undefined with respect
to blinding. – However, the precise blinding protocol was not clearly described in many trials
included in the review. ALLOCATION• Gender was approximately distributed evenly in most trials.• The mean age of participants ranged from 52-63 years.• Bias was assessed independently by two reviewers using a pre-defined criteria
(Higgins, 2008).• Risk of bias was
high or unclear in 8/10 trials, with the remaining 2 assessed as having a moderate risk.
Leach MJ, Kumar S., 2012.
Appraisal
MAINTENANCE – All studies used oral monopreparation of cinnamon in tablet or capsule
form.– 3 studies were excluded after careful evaluation of the full publication –
primarily due to failure to meet the diagnostic criteria for Type 1 or 2 diabetes.
– Where possible, any relevant missing information on the trial was sought from the original author(s) of the article – e.g. reasons for drop-outs were inconsistently reported.
MEASUREMENT – Heterogeneity was assessed by visual inspection of the forest plots and
by using a standard Chi2 test:• Cinnamon vs. Placebo; Outcome – fasting blood glucose level
(mmol/L) Chi2=0.97. – If one of the primary outcome parameters showed significant
differences between the intervention groups subgroup analysis was performed:• Cinnamon species• Cinnamon dosage• Treatment duration• Type of diabetes (I or II)
Results
The Results (interpretation of findings)• There were 8 studies reporting data on fasting blood glucose for 388 participants.
• These showed significant heterogeneity (Chi2=0.82).• Visual inspection of the funnel plot and subgroup analysis led the authors to
exclude 2 out of these 8 studies as outliers. • Analysis of the 6 remaining studies found no statistically significant
difference in fasting blood glucose between cinnamon and placebo groups (P=0.55 ; 95%CI -0.34 to 0.18).
• Adverse effects were recorded in 4 trials.– 3 events in intervention groups:
• Rash• Hives• Hypoglycaemic episode
– 4 events in control groups. • Nausea• Stomach ache• Other frequent illness
– Overall, there was no significant difference between adverse effects in the intervention and control group.
Implications
• Apply– whatwouldyousay
Outline
1.Introduction:whatisEBM2.Thestepsinevidencebasedpractice(5A’s)3.Anexample4.SelfReflectionandfinalthoughts
9/19/17
9
SelfReflection
Nextyearask• Areyouaskinganyquestionsatall?• Whatisyoursuccessrateinaskinganswerablequestions
• Howisyoursearchinggoing?--- stillGOOGLE?/Wikepedia/Pantip?
• Areyoucriticallyappraisingyoursearchresults• Areyouapplyingevidenceinclinicalpractice
EBM
• Helpyoumakeclinicaldecision• Sharedecisionwithpatients• Providebetterdiagnosticreasoning• Understandbenefitsversusharms• Allowyoutopracticemoresafely
FinalThoughts
• Widevariationsinimplementationofevidencebasedpractice
CrisisinEBM• Theevidencebased‘qualitymark’hasbeenmisappropriatedbyvestedinterests(drugandmedicaldeviceindustries)
• Toomuchevidence(toomanyguidelines)• Marginalgainsandashiftfromdiseasetorisk• Overemphasisonfollowingalgorithmicrules• Poorfitformultimorbidity
RealconceptofEBM
• Makestheethicalcareofthepatientitstoppriority• Demandsindividualizedevidenceinaformatthatcliniciansandpatientscanunderstand
• Characterizedbyexpertjudgmentratherthanmechanicalrulefollowing
• Sharesdecisionswithpatientsthroughmeaningfulconversation
• Buildsonstrongdoctor-patientrelationshipandthehumanaspectsofcare
• Appliestheseprinciplesatcommunitylevelforevidencebasedpublichealth
FinalQuestion:Whichisit?AorB
AThedoctor istheretogivethepatients alltheinformationthatthepatientneedsinorderthatthepatient canmakeadecision,andthedoctorshouldthenimplementthatdecisiononcethepatient hasmadeit
BThepatient istheretogivethedoctor alltheinformationthatthedoctorneedsinorderthatthedoctor canmakeadecision,andthepatientshouldthenimplementthatdecisiononcethedoctor hasmadeit
Questions