Embed Size (px)
Citation preview

Introduction to Multifamily Groups
Alex Kopelowicz, MDAlex Kopelowicz, MD
Thomas E. Backer, PhDThomas E. Backer, PhD
Human Interaction Research InstituteHuman Interaction Research Institute
New Haven, CT October 28, 2011New Haven, CT October 28, 2011

AgendaAgenda
9:00 - 9:15 am Welcome and introductions
9:15 - 10:00 am Definition of MFG and evidence for its effectiveness
10:00 – 10:30 am Steps for implementing MFG in New Haven
10:30 – 10:45 am Break
10:45 – 12:00 pm Overview of MFG components
12:00 – 1:00 pm Lunch
1:00 -1:30 pm Tailoring MFG for New Haven
1:30 – 2:00 pm Workplace Fundamentals to augment MFG
2:15 – 2:30 pm Challenges of implementing MFG
2:30 – 2:45 pm Evaluating process and outcomes of MFG
2:45 – 3:00 pm Next steps

Why Focus on the MFG Approach with Families?
Clients and relatives need information to help them Clients and relatives need information to help them better understand mental disorders or other better understand mental disorders or other problemsproblems
Clients want and need the support of their familiesClients want and need the support of their families Relatives often provide assistance, and want to be a Relatives often provide assistance, and want to be a
part of the clientpart of the client’’s recovery and successs recovery and success Clients want to develop skills and benefit from the Clients want to develop skills and benefit from the
help of their relativeshelp of their relatives Relatives need help reducing caregiver burdenRelatives need help reducing caregiver burden Families need help reducing stress at homeFamilies need help reducing stress at home

PORT Treatment PORT Treatment RecommendationsRecommendations
Patients who have on-going contact with their Patients who have on-going contact with their families should be offered a family families should be offered a family psychosocial intervention which spans at least psychosocial intervention which spans at least nine months and which provides a nine months and which provides a combination of education about the illness, combination of education about the illness, family support, crisis intervention, and family support, crisis intervention, and problem solving skills training. Such problem solving skills training. Such interventions should also be offered to non-interventions should also be offered to non-family caregivers.family caregivers.

Approaches toApproaches toWorking with FamiliesWorking with Families
PsychoeducationPsychoeducation
Communication skills trainingCommunication skills training
Problem solving techniquesProblem solving techniques
Social network development Social network development

Principles of Multifamily Groups
Engage Families on their Own Terms Psychoeducation is Ongoing and Interactive Keep Tension and Conflict in Family Meetings
to a Minimum Family Work is Oriented Toward the Future The Needs of the Whole Family are Addressed,
Not Just the Client Avoid Blaming the Family

7
Critical Ingredients of Critical Ingredients of an Effective MFGan Effective MFG
Longer-term (6-9 months or longer)Longer-term (6-9 months or longer) Delivered by trained facilitatorsDelivered by trained facilitators Broad view of who is Broad view of who is ““familyfamily”” Inclusion of individual in family sessionsInclusion of individual in family sessions Education of families Education of families Concern and empathy demonstrated for Concern and empathy demonstrated for
individual and relativesindividual and relatives Avoidance of blaming or pathologizing familyAvoidance of blaming or pathologizing family Fostering development of all family membersFostering development of all family members

Better Outcomes in Better Outcomes in Family PsychoeducationFamily Psychoeducation
Over 20 controlled clinical trials, comparing to Over 20 controlled clinical trials, comparing to standard outpatient treatment, have shown:standard outpatient treatment, have shown:– Much lower relapse rates and rehospitalizationMuch lower relapse rates and rehospitalization
Up to 75% reductions of rates; minimally 50%Up to 75% reductions of rates; minimally 50%– Increased employmentIncreased employment
At least twice the number of consumers employed, and At least twice the number of consumers employed, and up to four times greater--over 50% employed after two up to four times greater--over 50% employed after two years--when combined with supported employmentyears--when combined with supported employment
– Improved family relationships and well-beingImproved family relationships and well-being– Reduced friction and family burdenReduced friction and family burden– Reduced medical illness in family membersReduced medical illness in family members
Doctor visits for family members decreased by over Doctor visits for family members decreased by over 50% in one year50% in one year
Dixon et al 2003

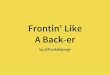
Efficacy of MFG – RCT Study Results
174 Mexican-American subjects
1 year of treatment 1 year of follow-up Overall log-rank
Χ2=13.3, df=2, p=.001.
Time To Hospitalization
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 1-4 5-8 9-12 13-18 19-24
Months After Baseline
% N
ot
Re
ho
sp
ita
liz
ed
A
S
C

Implementing MFG Implementing MFG in New Havenin New Haven
Step 1 - Initial analysis of site population and environmentStep 1 - Initial analysis of site population and environment Step 2 - Site orientation and learning (October 28)Step 2 - Site orientation and learning (October 28) Step 3 - Creation of adapted MFG for employmentStep 3 - Creation of adapted MFG for employment Step 4 - Site staff training (date TBA)Step 4 - Site staff training (date TBA) Step 5 - Family psychoeducation session (date TBA)Step 5 - Family psychoeducation session (date TBA) Step 6 - Implementation and operation of MFG (6-9 months)Step 6 - Implementation and operation of MFG (6-9 months)
(including two troubleshooting visits by Dr. Kopelowicz)(including two troubleshooting visits by Dr. Kopelowicz) Step 7 - Evaluation of MFG process and outcomesStep 7 - Evaluation of MFG process and outcomes Step 8 - Analysis of MFG and report to Casey FoundationStep 8 - Analysis of MFG and report to Casey Foundation

Stages of a Multifamily Group
JoiningFamily and Clientseparately3-6 weeks
Psycho-educa-tional workshopFamilies only1 day
Ongoing MFGFamilies & Clients
6-9 months

Joining with Families & ClientsJoining with Families & Clients
JOINING means to CONNECT, BUILD RAPPORT, CONVEY JOINING means to CONNECT, BUILD RAPPORT, CONVEY EMPATHY, ESTABLISH AN ALLIANCE, ENGAGEEMPATHY, ESTABLISH AN ALLIANCE, ENGAGE
It is the first stage of treatmentIt is the first stage of treatment Designed to create a bond between client/family members Designed to create a bond between client/family members
and facilitatorsand facilitators Facilitators as advocatesFacilitators as advocates

Joining Procedures Joining Procedures
THREE Joining MeetingsTHREE Joining Meetings
SEPARATELY with Relatives and ClientsSEPARATELY with Relatives and Clients
WEEKLY – 1 HOUR with Relatives, ½ HOURWEEKLY – 1 HOUR with Relatives, ½ HOUR
with Clientswith Clients Start sessions ASAP after crisis such as Start sessions ASAP after crisis such as
hospitalizationhospitalization Gain an understanding of familyGain an understanding of family’’s stresses, s stresses,
problems, reactions to clientproblems, reactions to client’’s problems, etc.s problems, etc.

Joining – IJoining – I
15 Minutes of SOCIAL TALK15 Minutes of SOCIAL TALK Review any recent CRISIS: Who and What Review any recent CRISIS: Who and What
Helped or DidnHelped or Didn’’tt IDENTIFY WARNING SIGNS – PRODROMAL IDENTIFY WARNING SIGNS – PRODROMAL
SIGNS – PRECIPITANTSSIGNS – PRECIPITANTS Distribute to Families & Keep for Future Distribute to Families & Keep for Future
ReferenceReference Describe the Plan for Ongoing MFG sessionsDescribe the Plan for Ongoing MFG sessions 5 Minutes SOCIALIZING5 Minutes SOCIALIZING

Joining – II Joining – II
15 Minutes of SOCIAL TALK15 Minutes of SOCIAL TALK FAMILYFAMILY’’S EXPERIENCE DURING EPISODES S EXPERIENCE DURING EPISODES
The Sharing of Painful Events: A Crucial The Sharing of Painful Events: A Crucial Aspect of Aspect of ““JoiningJoining””
The Client/FamilyThe Client/Family’’s Understanding of s Understanding of the the ClientClient’’s Problems s Problems
FamilyFamily’’s Social Network & Resources s Social Network & Resources (Material & Emotional)(Material & Emotional)
5 Minutes SOCIALIZING5 Minutes SOCIALIZING

Joining – IIIJoining – III
15 Minutes of SOCIAL TALK15 Minutes of SOCIAL TALK FAMILYFAMILY’’S SOCIAL NETWORK & RESOURCESS SOCIAL NETWORK & RESOURCES SHORT & LONG-TERM GOALS (e.g., Prevent SHORT & LONG-TERM GOALS (e.g., Prevent
Relapse)Relapse) Preparation for Workshop & MFGsPreparation for Workshop & MFGs

Family Psychoeducation WorkshopFamily Psychoeducation Workshop
(sample for families of adults with serious mental illnesses)(sample for families of adults with serious mental illnesses)
9:00-10:00am9:00-10:00am What is Mental Illness?What is Mental Illness?
-Causes - Symptoms-Causes - Symptoms
-Duration - Hope -Duration - Hope
10:00-10:15am10:00-10:15am BreakBreak
10:15-12:00pm10:15-12:00pm Treatment of Serious Mental IllnessTreatment of Serious Mental Illness
-Medication-Medication
-Hospitalization-Hospitalization
-Family Psychoeducation-Family Psychoeducation
-Social Skills Training-Social Skills Training
12:00-1:00pm12:00-1:00pm LunchLunch
1:00-4:00pm1:00-4:00pm The Family and Serious Mental IllnessThe Family and Serious Mental Illness
-Familial Reaction-Familial Reaction
-Family Problems-Family Problems
-Family Support-Family Support

Elements of MFG SessionsElements of MFG Sessions
Five to eight familiesFive to eight families Two facilitatorsTwo facilitators 1 ½-Hour sessions – biweekly 6-9 months1 ½-Hour sessions – biweekly 6-9 months Refreshments/snacks are providedRefreshments/snacks are provided Initial sessions avoid emphasis on clinical Initial sessions avoid emphasis on clinical
issuesissues Initial sessions emphasize establishing a Initial sessions emphasize establishing a
working alliance by building group identity working alliance by building group identity and developing a sense of mutual interest and developing a sense of mutual interest and concern. Drop outs are failuresand concern. Drop outs are failures

First MFG Session First MFG Session
““GETTING TO KNOW EACH OTHERGETTING TO KNOW EACH OTHER”” Go Around the RoomGo Around the Room
BackgroundBackground HobbiesHobbies OccupationOccupation InterestsInterests Facilitator Goes First (Discloses/Shares with Facilitator Goes First (Discloses/Shares with
Group)Group)
SETTING BASIC RULESSETTING BASIC RULES Regular ATTENDANCE (for Relatives)Regular ATTENDANCE (for Relatives) CONFIDENTIALITY (No Pressure to Disclose)CONFIDENTIALITY (No Pressure to Disclose) INTERACTION AMONG MEMBERSINTERACTION AMONG MEMBERS
PHYSICAL/EMOTIONAL CONTROLPHYSICAL/EMOTIONAL CONTROL

Second MFG Session Second MFG Session
Group processGroup process
Building a SENSE OF TRUST & COMMITMENTBuilding a SENSE OF TRUST & COMMITMENT Sense of COMMON EXPERIENCE (Listen to each other)Sense of COMMON EXPERIENCE (Listen to each other) Strengthening GROUP IDENTITY & SENSE OF RELIEFStrengthening GROUP IDENTITY & SENSE OF RELIEF The CLIENTThe CLIENT’’S INNER EXPERIENCESS INNER EXPERIENCES Facilitators emphasize the vital role of SHARING Facilitators emphasize the vital role of SHARING GRIEF,GRIEF, CONFUSION, GUILT, FEAR with those CONFUSION, GUILT, FEAR with those ““on the same on the same boatboat”” AND HOPEAND HOPE
Remind participants about Problem Solving Remind participants about Problem Solving (next session)(next session)

General Points on MFGGeneral Points on MFG
New MembersNew Members Late-Arriving MembersLate-Arriving Members Reminders about AttendingReminders about Attending Crises & EmergenciesCrises & Emergencies
COMMUNICATION & INTERACTIONSCOMMUNICATION & INTERACTIONS Facilitators DONFacilitators DON’’T speak for clients or T speak for clients or relativesrelatives Interaction among members is essentialInteraction among members is essential Clients are ENCOURAGED (not pressured) toClients are ENCOURAGED (not pressured) to participateparticipate
Respect otherRespect other’’s turn and avoid criticisms turn and avoid criticism

Problem Solving in MFGsProblem Solving in MFGs
The CORE of MFG SessionsThe CORE of MFG Sessions Designed to compensate for Information-Designed to compensate for Information-
Processing Deficits Processing Deficits FORMAT:FORMAT:
Checking inChecking in 15 Minutes15 MinutesGo-roundGo-round 20 Minutes20 MinutesSelecting a Problem to SolveSelecting a Problem to Solve 5 Minutes5 MinutesSolving the ProblemSolving the Problem 45 Minutes45 MinutesWrap-up SocializingWrap-up Socializing 5 Minutes5 Minutes
Facilitators should GET READY and HAVE A PLAN Facilitators should GET READY and HAVE A PLAN – IN ADVANCE– IN ADVANCE

Selecting a Problem Selecting a Problem to Solveto Solve
TOPICS:TOPICS:Safety in The HomeSafety in The HomeMedication ComplianceMedication ComplianceDrugs and AlcoholDrugs and AlcoholLife EventsLife EventsOutside Agency EventsOutside Agency EventsDisagreements among Family MembersDisagreements among Family MembersConflict with a Family GuidelineConflict with a Family Guideline
““REJECTEDREJECTED”” PROBLEMS: PROBLEMS:Make a Direct Suggestion and Review OutcomeMake a Direct Suggestion and Review OutcomeMeet Outside the Group (e.g., Crises)Meet Outside the Group (e.g., Crises)Refer to Past Solutions that ApplyRefer to Past Solutions that ApplyRefer to Solution/Family with Successful Refer to Solution/Family with Successful
OutcomeOutcome

The Problem-Solving MethodThe Problem-Solving Method
1.1. Define the Problem or GoalDefine the Problem or Goal
2.2. List Possible SolutionsList Possible Solutions
3.3. Evaluate Advantages and Disadvantages of Evaluate Advantages and Disadvantages of each Solutioneach Solution
4.4. Choose Choose ““the Bestthe Best”” Solution Solution
5.5. Implement Plan to Carry Out SolutionImplement Plan to Carry Out Solution
6.6. Review Implementation and OutcomeReview Implementation and Outcome

MFG is FlexibleMFG is Flexible
MFG programs have been created for adults MFG programs have been created for adults and adolescentsand adolescents
Clinical populations have included clients Clinical populations have included clients with schizophrenia, depression, ADHD and with schizophrenia, depression, ADHD and many other problemsmany other problems
This MFG will focus on employment problemsThis MFG will focus on employment problems

The key question is:
What are the factors that need to be considered prior to implementing the employment-focused MFG intervention with the target population in New Haven?

Target Population for Target Population for Employment-Focused MFGEmployment-Focused MFG
Adults who are hard to serve/hard to Adults who are hard to serve/hard to employ/hard to houseemploy/hard to house
Many have concurrent mental health, Many have concurrent mental health, addiction and trauma problemsaddiction and trauma problems
Employment options include supported Employment options include supported employment, subsidized employment, day employment, subsidized employment, day labor, part time (typically not benefitted jobs)labor, part time (typically not benefitted jobs)

Tailoring MFG to the Needs Tailoring MFG to the Needs of Clients in New Havenof Clients in New Haven
AttitudesAttitudes– ClientsClients’’ assumptions about employment and the assumptions about employment and the
benefits of services are targetedbenefits of services are targeted
Subjective NormsSubjective Norms– Emphasis on encouraging family members to Emphasis on encouraging family members to
actively support the clientactively support the client’’s employment effortss employment efforts
Perceived Behavioral ControlPerceived Behavioral Control– Utilization of problem solving techniques to Utilization of problem solving techniques to
overcome financial, insurance and transportation overcome financial, insurance and transportation obstacles to employmentobstacles to employment

Workplace Fundamental SkillsWorkplace Fundamental Skills
How work changes your lifeHow work changes your life Learn about your workplaceLearn about your workplace Identify your own stressorsIdentify your own stressors Manage symptoms and medsManage symptoms and meds Interactions to improve jobInteractions to improve job Appropriate socializationAppropriate socialization Supports and motivationSupports and motivation

Challenges of Challenges of Implementing MFG Implementing MFG
Is the MFG relevant for families of clients in Is the MFG relevant for families of clients in my agency?my agency?
Are potential MFG trainers (or family Are potential MFG trainers (or family facilitators) available at my agency?facilitators) available at my agency?
Are resources available to support Are resources available to support implementing the MFG at my agency?implementing the MFG at my agency?
Are there two or more staff who can commit Are there two or more staff who can commit to the two-day MFG training sessions?to the two-day MFG training sessions?

Evaluating MFG Evaluating MFG Process and OutcomesProcess and Outcomes
Staff Training Pre- and Post-SurveysStaff Training Pre- and Post-Surveys Family Member Pre-InterviewsFamily Member Pre-Interviews Family Member Post-InterviewsFamily Member Post-Interviews Client Pre-DataClient Pre-Data Client Post-DataClient Post-Data Facilitator and Administrative InterviewsFacilitator and Administrative Interviews
Evaluation forms are available onlineEvaluation forms are available online

Contact InformationContact Information
Dr. Alex Kopelowicz, Dr. Alex Kopelowicz, [email protected]
Dr. Tom Backer, Dr. Tom Backer, [email protected]
We look forward to working with you!We look forward to working with you!