Embed Size (px)
Citation preview

TITLE PAGE
Full Title: BIVALIRUDIN, GLYCOPROTEIN INHIBITOR AND
HEPARIN USE AND ASSOCIATION WITH OUTCOMES
OF PRIMARY PERCUTANEOUS CORONARY
INTERVENTION IN THE UNITED KINGDOM
Short title : Primary PCI – outcomes by anti-thrombotic choice
Authors names, degrees and affiliations :
1) Alex Sirker, MA (Cantab), MB BChir, PhD; University College London Hospitals,
UK
2) Mamas Mamas MA (Oxon), BM BCh, DPhil; Keele University and University of
Manchester, UK
3) Derek Robinson MA (Cantab), MSc, DPhil; University of Sussex, UK
4) Simon Anderson MSc, MB BCh, PhD; University of Manchester, UK
5) Tim Kinnaird MB BCh, MD; University Hospital of Wales, UK
6) Rod Stables MA (Cantab), BM BCh, DM: Liverpool Heart and Chest Hospital, UK
7) Mark A de Belder MA (Cantab), MD; The James Cook University Hospital,
Middlesborough, UK
8) Peter Ludman MA (Cantab), MD; Queen Elizabeth Hospital, Birmingham, UK
9) David Hildick-Smith MA (Cantab), MD; Brighton and Sussex University
Hospitals, UK
Address for correspondence and reprints
Dr. David Hildick-Smith, Department of Cardiology, Royal Sussex County Hospital, Eastern Road, Brighton, UK. BN2 5BEEmail: [email protected] Telephone: +44 (0)1273 664494 ; Fax: +44 (0)1273 684554
Total word count : 4869
1

ABSTRACT
Aims
The HORIZONS trial reported a survival advantage for bivalirudin over heparin-with-
glycoprotein inhibitors (GPI) in primary PCI for ST elevation myocardial infarction.
This drove an international shift in clinical practice. Subsequent studies have
produced divergent findings on mortality benefits with bivalirudin. We investigated
this issue in a larger population than studied in any of these trials, using the United
Kingdom national PCI registry.
Methods and Results
61,136 primary PCI procedures were performed between January 2008 and January
2012. Demographic and procedural data were obtained from the registry. Mortality
information was obtained through the UK Office of National Statistics. Multivariable
logistic regression and propensity analysis modelling were utilized to study the
association of different antithrombotic strategies with outcomes. Unadjusted data
demonstrated near-identical survival curves for bivalirudin and heparin-plus-GPI
groups. Significantly higher early and late mortality was found in patients treated with
heparin alone (p<0.0001) but this group had a markedly higher baseline risk. After
propensity matching, the bivalirudin versus heparin-plus-GPI groups still
demonstrated very similar adjusted mortality (odds ratio 1.00 at 30 days, and 0.96 at 1
year). Patients treated with heparin alone continued to show higher mortality after
adjustment, although effect size was considerably diminished (odds ratio versus other
groups 1.17-1.24 at 30 days).
2

Conclusions
Analysis of recent UK data showed no significant difference in short or medium term
mortality between STEMI patients treated with bivalirudin versus heparin-plus-GPI at
primary PCI.
KEYWORDS
heparin, bivalirudin, glycoprotein inhibitor, primary PCI, STEMI, antithrombotic
Abbreviations in manuscript:
CABG – coronary artery bypass grafting
DAPT – dual antiplatelet therapy
GPI – glycoprotein 2b3a inhibitor
PCI – percutaneous coronary intervention
PPCI – primary PCI
RCT – randomized controlled trial
STEMI – ST elevation myocardial infarction
MACCE – major adverse cardiac and cerebrovascular events
NACE – net adverse clinical events
OR – odds ratio
CI – confidence interval
3

BIVALIRUDIN, GLYCOPROTEIN INHIBITORS AND
HEPARIN USE AND ASSOCIATION WITH OUTCOMES OF
PRIMARY PERCUTANEOUS CORONARY INTERVENTION
IN THE UNITED KINGDOM
Introduction
Primary PCI (PPCI) has become the treatment of choice for ST elevation myocardial
infarction (STEMI). However the optimal antithrombotic regimen remains
controversial. Evidence for benefit of GPIs came from trials such as ADMIRAL,
CADILLAC and ISAR 2. (1) A meta-analysis of over 27,000 patients treated with
abciximab in PPCI RCTs showed significant short- and long- term mortality benefits.
(2) Studies on other GPI agents suggested similar benefits.(3-5) However, subsequent
studies challenged their ongoing relevance. For example, BRAVE-3 suggested that
benefits of abciximab in STEMI were negated when higher loading doses of
clopidogrel were used.(6) The place of GPIs was further challenged by the
HORIZONS trial.(7) Early and late mortality benefits were found with bivalirudin,
compared to a heparin-plus-routine GPI combination, with a 30-day absolute
mortality difference of 1% (relative risk 0.66). The mechanisms by which bivalirudin
achieved these mortality benefits remain unclear and several issues are noteworthy.
(a) The earlier incidence of stent thrombosis with bivalirudin (with later catch-up in
the other treatment arm) was postulated to be relevant (since in-hospital complications
might be more rapidly and hence successfully addressed) – however a recent
HORIZONS substudy indicated this theory was not the explanation.(8) (b) The other
4

main candidate mechanism is via the demonstrably lower rate of bleeding in patients
receiving bivalirudin. However the means by which early bleeding problems led to
survival curves that were still diverging beyond 1 year is uncertain.(9) (c) Even more
intriguingly, a recently published analysis from HORIZONS indicates that the
mortality benefits of bivalirudin over heparin-plus-GPI were evident even when
patients with major bleeds were excluded.(10) This led to speculation about
additional, poorly defined pleiotropic actions of bivalirudin. This mortality advantage
appeared to be restricted to patients with the highest blood leucocyte counts, for
unknown reasons (11). Subsequent studies that compared bivalirudin with other
antithrombotic strategies (including EuroMax, BRIGHT, HEAT-PPCI and most
recently MATRIX Antithrombin), have produced inconsistent mortality findings
(covered in greater detail in the Discussion). This has led to considerable uncertainty
in terms of potential survival benefits with bivalirudin use compared to other
therapies in PPCI.
The diversity of clinical practice in the UK permits the study of 3 broad
antithrombotic combinations in primary PCI - bivalirudin, heparin-with-GPI, and
heparin-alone. We sought to investigate patterns of use and their association with
outcomes, using the United Kingdom National Registries for PCI procedures and
mortality.
5

Methods
UK National PCI Database
Data on PCI in the UK are compiled under the auspices of the National Institute of
Cardiovascular Outcomes Research (NICOR) and the British Cardiovascular
Intervention Society (BCIS). The dataset is composed of 113 variables, including
patient demographics and procedural details. Mortality tracking is undertaken
annually using the patients’ unique National Health Service numbers to link the
BCIS-NICOR database to that held by the UK Office of National Statistics (ONS), on
which all UK deaths are recorded. This tracking is not available for patients in
Scotland or Northern Ireland. Details on data capture, handling and validation in the
registry have been published previously (18).
Study population
Study subjects were those patients who underwent a PPCI procedure for STEMI in
the UK between 1st January 2008 and 1st January 2012. This time period was chosen
since it reflects an era of “contemporary STEMI management” in which, for example,
high dose oral antiplatelet loading was routinely used pre-procedure and radial access
was utilized in a significant proportion of cases.
Outcome measures
6

The primary outcome measure for this study was 30-day mortality. Secondary
endpoints were 1-year mortality, time to death (survival curve analysis), and in-
hospital major bleeding. Major bleeds comprised gastrointestinal bleeds, intracerebral
bleeds, retroperitoneal bleeds, blood or platelet transfusion, or an arterial access site
complication requiring surgery. Major bleeding events were obtained from recorded
entries on the BCIS-NICOR database - recording is dependent on appropriate
completion of the relevant field on the database (concerning PCI complications) by
clinical staff, either at the time of the PPCI procedure (for early bleeds) or
subsequently (for delayed bleeds). This field is not cross-populated from another
database (in contrast to mortality data).
Study definitions
Patients were coded into 3 treatment groups based on physician-allocated therapy at
time of STEMI. These groups were i) bivalirudin, ii) heparin-alone (i.e. without
accompanying GPI or bivalirudin), iii) heparin-plus-GPI. Patients who received
bivalirudin plus heparin were coded within the bivalirudin group. Patients who
received both bivalirudin and a GPI were also coded within the bivalirudin group
(since they were considered likely to represent an initial bivalirudin strategy with bail-
out GPI).
Statistical methods
7

a) Descriptive statistics
For basic analysis of patient demographics, procedural characteristics and unadjusted
outcomes, continuous variables were evaluated as means ± SD. Means, standard
deviations and percentages quoted refer to numbers within the cohort where data were
available. Chi-square tests were used to assess the significance of differences in
proportions between groups for categorical variables. Student t-testing was used for
continuous variables. Log-rank testing was used for survival curve analysis. All
statistical tests were two-tailed and p<0.05 was taken as significant.
b) Imputation
To reduce inherent bias from complete case-only analysis, missing values were
addressed by a standard technique of multiple imputation, performed using the MI
and MIANALYZE procedures of the statistical software SAS (version 9.2).
c) Multivariable logistic regression modelling
Since the primary endpoint was binary, a standard logistic regression model was
employed. The model was constructed by fitting it first to treatment allocation alone
and then by adding each of the variables of interest to the model individually.
Variables of interest were selected to encompass known or potential predictors of 30
day mortality, and included: age, gender, weight, diabetes, hypertension, smoking,
cerebrovascular disease (TIA or stroke), peripheral vascular disease, renal impairment
(defined as serum creatinine>200 micromoles/litre or on dialysis), warfarin use,
cardiogenic shock, previous MI, previous PCI, previous CABG, Q wave on ECG, and
procedural details (including year of procedure, route of access, use of a novel potent
oral antiplatelet agent (i.e. prasugrel or ticagrelor), left main stem culprit lesion, use of
8

thrombectomy, and IABP use. Type of stent (DES versus BMS) was also included
since it typically appears as an independent predictor of mortality in registry studies
of PCI, almost certainly reflecting selection bias on the part of operators. Hence stent
type may be considered a surrogate marker for other unrecorded or unquantified
comorbidities (including frailty) and its use as regressor within the model should help
to mitigate the influence of unmeasured confounders. Variables found to be
significant (p<0.05) on univariate analysis were put forward into a multivariable
logistic regression.
d) Propensity analysis
As an alternative method for addressing the potential confounding factors due to non-
randomized treatment allocation, propensity matching was employed in a separate
analysis. Propensity scores were derived for each patient, based on the estimated
probabilities of that patient being assigned to each of the treatment groups, given the
values of various predictor variables for treatment allocation. The propensity score
was then obtained using a multinomial regression model. The predictors for treatment
allocation were chosen as those measurable variables that were likely to influence
which of the 3 treatments under consideration was chosen by the operator. Hence
factors associated with increased bleeding risk (and therefore appearing on standard
bleeding risk scores (19)) were included, with the full list of variables used as shown
in for the multivariate analysis, (section c) above).
In order to undertake propensity matching involving more than 2 treatment groups,
the method described previously by Spreeuwenberg et al was employed. (20). This
used logistic regression with 30-day mortality as the response, with regressors
9

consisting of the propensity scores p1, p2 and their product p1p2, as well as the three
treatments. Standard checks for overlap of propensity scores between the treatment
arms, and subsequently for the balance of covariates, were performed.
Multivariable logistic regression modelling and propensity analysis modelling were
performed at 30 day and 1 year post PPCI time points, involving those patients on
whom there was available mortality data at the respective time points.
Results
Patient numbers, baseline demographics and procedural details
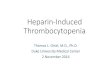
The summary of patient numbers is shown in Figure 1. The lower proportion of
tracked mortality data for the heparin-plus-GPI group reflected high use of this
strategy in Scotland, where database linkage was not possible. Baseline clinical
demographics are displayed in Table 1. It was noted that the heparin-only treatment
group contained patients with a significantly greater incidence of risk factors for
adverse outcome compared to other 2 treatment arms – specifically, greater age; more
frequent diabetes, hypertension, smoking history, peripheral vascular disease,
cerebrovascular disease and significant renal impairment; poorer NYHA class at
baseline; more prior IHD and prior CABG, and greater concurrent use of warfarin.
Procedural details are given in Table 2. Patients presenting with shock were found in
highest proportion in the heparin-plus-GPI group. In contrast, use of radial access, a
10

thrombectomy device, drug-eluting stents and novel oral antiplatelet drugs (prasugrel
or ticagrelor) was found in the highest frequency in the bivalirudin group.
Unadjusted mortality
Unadjusted mortality data for the 3 groups during hospital admission, at 30 days and
at 1 year, are shown in Table 3. Short- and medium- term mortality were significantly
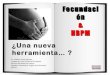
higher in the heparin-only treatment groups. This is also shown in Figure 2, where log
rank testing demonstrated poorer unadjusted survival for heparin-only patients
(p<0.0001 for heparin-only versus other groups; for bivalirudin versus heparin-plus-
GPI, p=0.63).
Major bleeding
Database-recorded rates of in-hospital major bleeding were 38/4158 (0.91%) for
bivalirudin, 273/35129 (0.78%) for heparin-plus-GPI, and 110/21849 (0.5%) for
heparin alone. Of the 38 patients on bivalirudin who had a major bleed, 3 patients had
received a GPI and 35 patients received heparin. Of the 4120 bivalirudin patients who
did not have a major bleed, 600 were on a GPI and 3520 were on heparin. GPI use
was not significantly different between those in the bivalirudin group who did and did
not have a major bleed (p=0.25, chi-square test).
Multivariable logistic regression model for 30-day mortality and 1 year mortality
30-day mortality data were available for 54,514 patients (breakdown by treatment
shown in Figure 1). Following univariate logistic regression and backward stepwise
11

elimination, the following variables remained significant and were thus included in
the multivariable regression model: age, gender, diabetes, hypertension, smoker/ex-
smoker, cerebrovascular disease, peripheral vascular disease, renal impairment, year
of procedure, previous PCI, Q waves, access site, shock, left main lesion, stent type
(DES or BMS), IABP use, use of prasugrel or ticagrelor, and treatment allocation
groups (bivalirudin, heparin plus GPI, and heparin-only, with one of these acting as
the reference level).
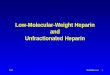
The association of treatment allocation with 30-day mortality is indicated by the
Forest plot in Figure 3a. The bivalirudin and heparin-plus-GPI groups showed very
similar results, whilst heparin-only patients showed significantly higher mortality.
The odds ratios and 95% CI boundaries were as follows (comparisons shown in the
form x:y, with y acting as the reference) bivalirudin : heparin/GPI - OR 1.01 (95% CI
0.84-1.21), p=0.92; heparin-only : heparin/GPI - OR 1.24 (95% CI 1.13-1.35),
p<0.0001 and heparin-only : bivalirudin – OR 1.23 (95% CI 1.02-1.47), p=0.026.
Results 1-year post-PPCI are shown graphically in Figure 4a. The parsimonious
model contained similar variables to that derived for 30-day mortality, with the
addition of weight and previous MI, and the exclusion of smoking, hypertension and
gender. Patterns remained essentially unchanged from those seen at 30 days. The odds
ratios and 95% CI boundaries at 1 year were bivalirudin : heparin/GPI – OR 0.96
(95% CI 0.83-1.11), p=0.59; heparin-only : heparin/GPI – OR 1.28 (95% CI 1.19-
1.37), p<0.0001; and heparin-only : bivalirudin – OR 1.33 (95% CI 1.15-1.54),
p<0.0001.
12

Propensity analysis modelling for 30-day mortality and 1 year mortality
Propensity analysis based comparison of treatment groups is shown in Figure 3b and
4b. Consistent with the findings from multivariable analysis, there was no significant
evidence for a difference between bivalirudin and GPI in terms of 30 day mortality.
The odds ratios were bivalirudin : GPI – OR 1.00 (95% CI 0.84-1.18), p=0.98;
heparin : GPI – OR 1.17 (95% CI 1.08-1.27), p<0.0001; and heparin : bivalirudin –
OR 1.18 (95% CI 1.00-1.38), p=0.05. When comparison is made to Figure 3a, it is
seen that these 2 distinct modelling methods produced strikingly similar findings.
Patterns seen at 30 days post PPCI remain evident at 1 year. The odds ratios and 95%
CI boundaries at 1 year were bivalirudin : heparin/GPI - OR 0.96 (95% CI 0.84-1.10),
p=0.57; heparin-only : heparin/GPI - OR 1.24 (95% CI 1.16-1.32), p<0.0001; and
heparin-only : bivalirudin - OR 1.29 (95% CI 1.13-1.47), p=0.0002.
13

Discussion
Rationale for present study
Our study employed the UK national registry of PCI to analyse patterns of practice
and address areas of continuing controversy in STEMI management. HORIZONS had
a profound impact on the management of STEMI patients, in part due to its findings
of reduced mortality with bivalirudin. This led to changes in European and American
guidelines (21, 22). The HORIZONS findings on mortality were supported by an
analysis of STEMI patients in the US PREMIER registry but follow-up in this latter
work only covered index hospital admissions and hence early post-discharge events
would have been missed.(12) In contrast, the EuroMax trial studied 30-day outcomes,
finding a significant reduction in the composite of death plus major bleeding (driven
by the latter), favouring bivalirudin over a strategy in which heparin was used in
combination with a GPI in the majority (69%) of cases.(13) A patient-level pooled
analysis of HORIZONS and EuroMax did not demonstrate any significant reduction
in all-cause mortality with bivalirudin use (with bail-out GPI) versus heparin +/- GPIs
(14). Consistent findings followed from the multicentre Chinese BRIGHT study, with
non-significant changes in mortality despite significant reductions in major bleeding
with bivalirudin versus heparin-plus-GPI (15). No study yet has been adequately
14

powered to definitively address mortality effects and this question remains
unresolved.
Another contentious issue is the role for a ‘heparin-only’ strategy (i.e. without
planned concomitant GPI or bivalirudin) in primary PCI. The HEAT PPCI trial
recently addressed this in an all-comers RCT (using GPIs only for bail out, in both
arms) and found heparin yielded similar bleeding rates but significantly fewer
ischaemic events (stent thrombosis or reinfarction) compared to bivalirudin at 30 days
(16). The impact of these findings on mortality remains unclear, although a non-
significant absolute mortality difference of 0.8% (favouring the heparin group) was
noted. In contrast, BRIGHT reported a borderline significant reduction in NACE with
bivalirudin (driven by reduced bleeding) but no difference in mortality between
heparin-only and bivalirudin treatment groups in BRIGHT. Most recently, data has
been presented from the European MATRIX study (17) CHANGE REF in over 7000
patients with acute coronary syndromes (including STEMI). There was no evidence of
significant reduction in a composite MACE primary endpoint with bivalirudin versus
heparin, +/- GPI (used in 4.6% and 26% of cases respectively). It did however find
significant reductions in bleeding and in all-cause mortality. MATRIX is the first
RCT since HORIZONS to suggest an all-cause mortality benefit with bivalirudin use.
However, as with HORIZONS, an important caveat is that the apparent advantage
with bivalirudin over heparin, in terms of bleeding, is likely driven (at least in part) by
the differential GPI use between comparator arms. However, whether this explains the
mortality signal favouring bivalirudin in these two studies remains unclear. We
therefore analysed the UK national database of primary PCI to explore this specific
issue further.
15

Patient demographics and treatment allocation
Review of patient demographics and treatment allocation in our study population
showed that many patients receive heparin alone. These patients tended to be older,
and have more comorbidities. This may reflect the view that giving heparin alone
would be considered a safer option than use of heparin-plus-GPI in patients felt to be
at higher risk of bleeding (particularly relevant to operators who do not use
bivalirudin). The greater incidence of unfavourable patient characteristics in the
heparin-only group is likely to be (at least) partly responsible for the poorer
unadjusted outcomes of this group - these adverse traits are only partially quantifiable
and incompletely captured in the BCIS dataset (in common with other registries),
hence important differences (such as patient frailty) might not be reconciled even
when advanced statistical methods were employed in adjusted analyses.
Heparin-plus-GPI tended to be used in patients at relatively lower risk of bleeding
(lower age, less renal dysfunction, fewer females etc.). Some differences were also
seen in baseline demographics and procedural characteristics between the bivalirudin
and heparin-plus-GPI cohorts. It is noteworthy that the use of either prasugrel or
ticagrelor was most common in the bivalirudin group, and then more common in the
heparin only group compared to those treated with both heparin and a GPI. It is
conceivable that operators felt the benefits of a GPI were fewer when these new
antiplatelet drugs (rather than clopidogrel) were used. Operators who elected to use
bivalirudin were also more likely to incorporate other recent developments in PCI,
such as radial access and thrombectomy devices. Hence it is certainly plausible that
operators choosing bivalirudin might be ‘early adopters’ of other PPCI innovations.
16

However, an alternative and equally plausible explanation relates to the higher
proportion of bivalirudin use during the latter part of the time period under
consideration, when these other PCI developments were also being incorporated more
frequently into clinical practice. Of course, both explanations may be valid, since they
are not mutually exclusive. Importantly however, the influence of all these potentially
confounding factors (i.e. other aspects of PPCI treatment and the year of treatment
itself) should be mitigated through their inclusion as covariates in both our logistic
regression and propensity-based analyses.
Association of anti-thrombotic choice and outcomes
There was a close similarity between the unadjusted survival curves for the
bivalirudin and heparin-plus-GPI groups. 30-day mortality was 5.1% and 4.6%
respectively from our data – if there had been an underlying absolute difference of 1%
in mortality between these two received-treatment groupings, we calculate that our
sample size gave 78-81% power to detect this as a significant difference between
groups (at p<0.05). Of course, the unmatched nature of these non-randomly assigned
groups makes it impossible to directly infer the impact of antithrombotic therapy from
this non-significant difference. In order to gain insight into the potential underlying
effects on mortality of these alternative received-treatments, two different forms of
statistical modelling were employed. The findings of the two different models
strongly concurred. Neither model provided evidence for a mortality difference at 30
days between bivalirudin and heparin-plus-GPI inhibitor groups. This signal is thus
consistent with that from the strategy comparisons performed in the RCTs EuroMax,
BRIGHT and also ISAR REACT 4 (which examined a high-risk NSTEMI setting)
17

(13, 15, 24). One of the most potent messages from HORIZONS was an improved
survival with bivalirudin in STEMI, which helped to drive practice change
internationally (towards greater use of this drug). However this does not appear
consistent with the overall published experience to date and our findings are
consistent with a pooled analysis of recent randomized studies indicating no survival
difference with these contrasting antithrombotic options (25).
Even after statistical adjustment, the heparin-only group in our work fared less well.
As discussed above, it is certainly possible that adjustments (based, by necessity, only
on captured and quantified variables) may not compensate for all differences between
groups – hence an incompletely reconciled higher baseline risk in the heparin-only
group might explain the higher mortality seen. However, the results do raise an
alternative possibility, namely that a decision to use heparin on its own (possibly due
to fear of bleeding problems) might increase the risk for an adverse cardiovascular
outcome. This result would of course be contrary to the message emerging from
HEAT PPCI and hence it is worth considering why this might be so (26). In this
regard, it might be highly relevant that over 90% of patients in HEAT PPCI received a
potent novel oral antiplatelet agent (prasugrel or ticagrelor) compared with a far lower
proportion (13.8%) in our heparin-only group. It is thus plausible that the lack of
concomitant use of either a novel oral antiplatelet agent or an intravenous GPI in the
vast majority of these patients leaves them with insufficient platelet inhibition during
this early window i.e. during, and in the hours immediately after, PPCI. This might, in
turn, translate into increased adverse events with a consequent impact on survival.
Limitations
18

Being derived from a real-world PCI registry, this paper incorporates “all-comers”
undergoing primary PCI for STEMI, avoiding selection and screening bias against
high-risk patients (as is frequently encountered in RCTs). The registry represents
daily practice and contributes to the overall knowledge base, alongside data from
carefully controlled trials. However, a number of caveats and limitations must be
borne in mind to allow appropriate reader interpretation of our presented findings.
1) Common to all registry-based work, it is recognized that no statistical modelling
can fully compensate for unidentified or unmeasured confounding factors that may be
imbalanced between non-randomly allocated treatment groups. We recognize that the
presence of such confounders may therefore also have potentially influenced
comparisons in our work.
2) A second noteworthy issue is that comparisons were made between groups based
on received antithrombotic treatments. This is intrinsically different to a comparison
of treatment protocols – for example, the database does not allow differentiation
between GPI use being planned versus bail-out. Hence the heparin-plus-GPI group in
our work will include patients managed with both of these strategies (planned use and
bail-out use) and hence is somewhat heterogeneous. A further source of heterogeneity
arises from between-centre and between-operator differences in protocols for the use
of alternative antithrombotics – for example, in centres where bivalirudin is available,
it may be the default choice for some operators, whilst being used more selectively
(only in higher bleeding risk cases) by others. In contrast, at centres where bivalirudin
is not available, heparin-only is likely to be the selected strategy for high bleeding risk
cases. Nevertheless, we strongly feel that our analysis by received-treatment provides
useful new information, but it should not be misinterpreted as a comparison of upfront
treatment strategies.
19

3) As the BCIS registry is not monitored at the point of data entry, mis- or under-
recording of the antithrombotic used is, of course, possible. However, we believe that
any such under-recording would be entirely unintentional and very unlikely to
introduce any important systematic bias in favour of any particular antithrombotic
treatment.
4) The low recorded major bleeding rates reflect a combination of i) the BCIS
definition of major bleeding (see Methods), which differs from contemporary trial
definitions, making direct comparisons difficult, and ii) the possibility of under-
recording of bleeding problems by operators, since this requires retrospective logging
of events. This bleeding event registration contrasts with the robustness of our
mortality data taken from the UK Government’s Office of National Statistics.
5) Neither dosing of antithrombotic used nor ACT values achieved are recorded in the
BCIS-NICOR registry. Usual UK practice is consistent with European and US
guidelines with usual initial unfractionated heparin dose in the range 70-100 units
heparin/kg body weight without GPI and 50-70 units heparin/kg body weight when
used with GPI (reference to ESC/EACTS guidelines on myocardial revascularisation).
Conclusions
In summary, our analysis of the UK National PCI database from 2008-2012 shows no
significant difference in short or medium term mortality between groups treated with
bivalirudin versus heparin-plus-GPI in primary PCI. Our statistical modelling
suggests that previously described mortality benefits of bivalirudin over heparin-plus-
GPI are not evident in contemporary practice. Further RCTs of different regimens in
the current era are warranted, but our data suggest that the differences in mortality
20

outcomes associated with different regimens might be small. Thus, very large studies
might be needed to conclusively settle these issues.
Funding Sources None
Disclosures/Conflicts of Interest None
21

References
1. Kandzari DE, Hasselblad V, Tcheng JE, Stone GW, Califf RM, Kastrati A, et al. Improved clinical outcomes with abciximab therapy in acute myocardial infarction: a systematic overview of randomized clinical trials. Am Heart J 2004;147(3):457-62.2. De Luca G, Suryapranata H, Stone GW, Antoniucci D, Tcheng JE, Neumann FJ, et al. Abciximab as adjunctive therapy to reperfusion in acute ST-segment elevation myocardial infarction: a meta-analysis of randomized trials. Jama 2005;293(14):1759-65.3. De Luca G, Ucci G, Cassetti E, Marino P. Benefits from small molecule administration as compared with abciximab among patients with ST-segment elevation myocardial infarction treated with primary angioplasty: a meta-analysis. J Am Coll Cardiol 2009;53(18):1668-73.4. Zeymer U, Margenet A, Haude M, Bode C, Lablanche JM, Heuer H, et al. Randomized comparison of eptifibatide versus abciximab in primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction: results of the EVA-AMI Trial. J Am Coll Cardiol 2010;56(6):463-9.5. Akerblom A, James SK, Koutouzis M, Lagerqvist B, Stenestrand U, Svennblad B, et al. Eptifibatide is noninferior to abciximab in primary percutaneous coronary intervention: results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol 2010;56(6):470-5.6. Mehilli J, Kastrati A, Schulz S, Frungel S, Nekolla SG, Moshage W, et al. Abciximab in patients with acute ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention after clopidogrel loading: a randomized double-blind trial. Circulation 2009;119(14):1933-40.7. Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med 2008;358(21):2218-30.8. Dangas GD, Claessen BE, Mehran R, Brener S, Brodie BR, Dudek D, et al. Clinical outcomes following stent thrombosis occurring in-hospital versus out-of-hospital: results from the HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) trial. J Am Coll Cardiol 2012;59(20):1752-9.9. Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, et al. Heparin plus a glycoprotein IIb/IIIa inhibitor versus bivalirudin monotherapy and paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction (HORIZONS-AMI): final 3-year results from a multicentre, randomised controlled trial. Lancet 2011;377(9784):2193-204.10. Stone GW, Clayton T, Deliargyris EN, Prats J, Mehran R, Pocock SJ. Reduction in Cardiac Mortality With Bivalirudin in Patients With and Without Major Bleeding: The HORIZONS-AMI Trial (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction). J Am Coll Cardiol 2014;63(1):15-20.11. Palmerini T, Brener SJ, Mehran R, Dangas G, Genereux P, Riva DD, et al. Leukocyte count is a modulating factor for the mortality benefit of bivalirudin in ST-segment-elevation acute myocardial infarction: the HORIZONS-AMI trial. Circ Cardiovasc Interv 2013;6(5):518-26.
22

12. Pinto DS, Ogbonnaya A, Sherman SA, Tung P, Normand SL. Bivalirudin therapy is associated with improved clinical and economic outcomes in ST-elevation myocardial infarction patients undergoing percutaneous coronary intervention: results from an observational database. Circ Cardiovasc Qual Outcomes 2012;5(1):52-61.13. Steg PG, van 't Hof A, Hamm CW, Clemmensen P, Lapostolle F, Coste P, et al. Bivalirudin started during emergency transport for primary PCI. N Engl J Med 2013;369(23):2207-17.14. Stone GW, Mehran R, Goldstein P, Witzenbichler B, Van't Hof A, Guagliumi G, et al. Bivalirudin versus heparin with or without glycoprotein IIb/IIIa inhibitors in patients with STEMI undergoing primary percutaneous coronary intervention: pooled patient-level analysis from the HORIZONS-AMI and EUROMAX trials. J Am Coll Cardiol 2015;65(1):27-38.15. Han Y, Guo J, Zheng Y, Zang H, Su X, Wang Y, et al. Bivalirudin vs heparin with or without tirofiban during primary percutaneous coronary intervention in acute myocardial infarction: the BRIGHT randomized clinical trial. Jama 2015;313(13):1336-46.16. Shahzad A. How Effective are Antithrombotic Therapies in PPCI (HEAT PPCI). In: American College of Cardiology/i2 Annual Scientific Session.; 2014; Washington DC; 2014.17. Valgimigli M, Calabro P, Cortese B, Frigoli E, Garducci S, Rubartelli P, et al. Scientific foundation and possible implications for practice of the Minimizing Adverse Haemorrhagic Events by Transradial Access Site andSystemic Implementation of AngioX (MATRIX) trial. J Cardiovasc Transl Res 2014;7(1):101-11.18. Ludman PF. British Cardiovascular Intervention Society Registry for audit and quality assessment of percutaneous coronary interventions in the United Kingdom. Heart 2011;97(16):1293-7.19. Flores-Rios X, Couto-Mallon D, Rodriguez-Garrido J, Garcia-Guimaraes M, Gargallo-Fernandez P, Pinon-Esteban P, et al. Comparison of the performance of the CRUSADE, ACUITY-HORIZONS, and ACTION bleeding risk scores in STEMI undergoing primary PCI: insights from a cohort of 1391 patients. Eur Heart J Acute Cardiovasc Care 2013;2(1):19-26.20. Spreeuwenberg MD, Bartak A, Croon MA, Hagenaars JA, Busschbach JJ, Andrea H, et al. The multiple propensity score as control for bias in the comparison of more than two treatment arms: an introduction from a case study in mental health. Med Care 2010;48(2):166-74.21. O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Jr., Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;61(4):e78-140.22. Steg PG, James SK, Atar D, Badano LP, Blomstrom-Lundqvist C, Borger MA, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012;33(20):2569-619.23. Stone GW, McLaurin BT, Cox DA, Bertrand ME, Lincoff AM, Moses JW, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med 2006;355(21):2203-16.24. Kastrati A, Neumann FJ, Schulz S, Massberg S, Byrne RA, Ferenc M, et al. Abciximab and heparin versus bivalirudin for non-ST-elevation myocardial infarction. N Engl J Med 2011;365(21):1980-9.
23

25. Ferrante G, Valgimigli M, Pagnotta P, Presbitero P. Bivalirudin versus heparin in patients with acute myocardial infarction: A meta-analysis of randomized trials. Catheter Cardiovasc Interv 2015.26. Shahzad A, Kemp I, Mars C, Wilson K, Roome C, Cooper R, et al. Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial. Lancet 2014;384(9957):1849-58.
24

FIGURE LEGENDS
Figure 1 : Summary of antithrombotic treatment allocation and procedural
numbers per group
Figure 2 : Kaplan-Meier curves for survival (i.e. freedom from death), censored
at 1 year post primary PCI - Probability of survival is shown on the vertical axis.
Table below graph indicates numbers at risk in each group at 100, 200 and 300 days.
Figure 3 : Forest plot indicating effect of treatment allocation on 30-day mortality
from a) multivariable logistic regression model and b) propensity matching
model - Comparisons are shown as x : y (y being the reference), such that a position
left of OR 1 indicates greater survival with x and a position right of OR 1 greater
survival with y.
Figure 4 : Forest plot indicating effect of treatment allocation on 1-year mortality
from a) multivariable logistic regression model and b) propensity matching
model - Comparisons are shown as x : y (y being the reference), such that a position
left of OR 1 indicates greater survival with x and a position right of OR 1 greater
survival with y.
25