Embed Size (px)
Citation preview

PAEDIATRIC SURGERY II
IntussusceptionJoana Lopes
Simon N Huddart
AbstractIntussusception is the invagination of a segment of bowel into the distal
adjacent bowel. Mostly it involves the distal ileum and proximal colon and
no lead point can be identified. It is the most common cause of bowel
obstruction in infants and young children. It typically presents in infants
between 2 months and 2 years of age with episodic severe colicky
abdominal pain, vomiting that progresses to being bilious, abdominal
distension, and bleeding per rectum which is classically described as ‘red-
currant jelly’ stool. If not diagnosed and treated promptly the pathology
will progress to bowel necrosis, sepsis and death.
Patients usually need resuscitation and stabilization before investigation
anddefinite treatment. The diagnostic test of choice is an ultrasound scan of
the abdomen. The first-line treatment is an air-reduction enema that will be
successful in 80% of cases. Surgery with manual reduction of the intussus-
ception and possible bowel resection is reserved for cases presenting with
peritonitis, cases where a pathological lead point is identified, where air-
enema failed or where this procedure is complicated by bowel perforation.
Keywords Bowel obstruction; intussusception; redcurrant jelly
Introduction
Intussusception is definedas the invagination of a proximal segment
of intestine (intussusceptum) into the lumen of the adjacent more
distal segment of intestine (intussuscipiens). The intussusceptum
becomes the inner segment of intestine and the intussuscipiens the
outer segment of intestine in the intussusception.
Intussusception leads to bowel obstruction and if untreated
necrosis of the incarcerated bowel. It is the most common cause
of bowel obstruction in infants and young children.
History
1674e Intussusception was first described by Paul Barbette from
Amsterdam. The condition was invariably fatal.
1830e The first successful surgery was performed by John Wil-
son, but the surgical mortality was more than 75%.
1876e Harald Hirschsprung, a Danish paediatrician from
Copenhagen best known for describing congenital megacolon
and pyloric stenosis, first described hydrostatic reduction. The
diagnosis was clinical as radiographs were not available until
1895.
Joana Lopes MRCS is a Specialist Registrar in Paediatric Surgery at
University Hospital of Wales, Cardiff, UK. Conflicts of interest: none
declared.
Simon N Huddart MA MBBS FRCS FRCS(Paed) is a Consultant Neonatal and
Paediatric Surgeon at University Hospital of Wales, Cardiff, UK. Conflicts
of interest: none declared.
SURGERY 31:12 626
1959e Treatment of intussusception with insufflation of air
was first described by Fiorito from Argentina.
Epidemiology
The incidence in the UK is 1.6e4 cases per 1000 live births with
a male-to-female ratio of 3:2. It typically presents in infants
between 2 months and 2 years of age and 50% of the cases
present between 3 months and 10 months of age and 65% of the
cases before 1 year of age.
There is a seasonal variation in incidence with peaks in Spring
and Winter corresponding to peaks in occurrence of rotavirus
and adenovirus infections.
Aetiology/pathophysiology
In 95% of cases the intussusception is ileo-colic, arising in the
distal ileum and passing through the ileo-caecal valve into the
proximal colon. In decreasing frequency of occurrence it can also
be ileo-ileal, caeco-colic, colo-colic and jejuno-jejunal.
In 10% of cases a lead point (for example a polyp or hae-
mangioma) in the intestinal wall, driven by peristalsis in the
adjacent intestine, drags its associated segment of intestine (the
intussusceptum) into the distal bowel (the intussuscipiens).
In primary or idiopathic intussusception (90% of cases) a lead
point cannot be identified. It is thought that these idiopathic
cases might result from enlarged Peyer’s patches acting as a lead
point. Viral illnesses (upper tract respiratory infections and
gastroenteritis) may be the cause for the hypertrophy of the
lymphoid tissue. Adenovirus and to a lesser extent rotavirus have
been implicated in 50% of cases. The typical presentation
happens at the age of weaning occurs raising the possibility that
immune stimulation by newly introduced feeds may be a cause.
Food allergies are also considered to be a possible cause of
primary intussusception.
The incidence of intussusception increased in the USA after the
introduction of a rotavirus vaccine in 1998. Studies showed that the
risk increased 20e30-fold within 2weeks following the first dose of
the vaccine and three- to sevenfold within 2 weeks after the second
dose. Therewas no increased risk after the 3rd dose or 3weeks after
any of the doses. As a result, the vaccinewaswithdrawn a year after
being licensed.Twonewvaccinesagainst rotaviruswere licensed in
the USA (in 2006 and 2008). These had pre-licensure trials that
specifically evaluated the risk of intussusception and did not find it
tobe increased. Post-marketing surveillance is still ongoing.A study
that includeddataonmore than800,000dosesofoneof thevaccines
in the USA has not shown an increase in intussusception cases.
Postoperative intussusception (1% of childhood intussuscep-
tion) is another form of primary intussusception but a separate
entity on its own. It can happen following abdominal or thoracic
surgery, generally for malignancy, after retroperitoneal dissec-
tion and after chemo- or radiotherapy. It is usually ileo-ileal.
It is unclear why the intussusception develops but the current
belief is that it results from the proximal small bowel recovering
its peristalsis before the distal bowel and therefore being pushed
into the latter. It may also be due to spasm or oedema of the
bowel wall after surgery so acting as a lead point. Or it could be
due to dysmotility.
In secondary intussusception there is a pathological lead
point. Pathological lead points are more common outside the
Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.

Associated conditions seen with intussusception
C PeutzeJeghers syndrome e hamartous polyps act as
a lead point
C HenocheSchonlein Purpura e submucosal haematomas
act as a lead point. Intussusception seen in approximately
3.5% of patients with HenocheSchonlein purpura
C Cystic fibrosis e inspissated bowel contents act as a lead
point. Intussusception seen in approximately 1% of cystic
fibrosis patients
C Coeliac disease
C Clostridium difficile colitis
Note e Intussusception has been described in premature infants
and has been postulated as a possible cause for small bowel
atresia in neonates.
Box 2
PAEDIATRIC SURGERY II
typical age range with more than 20% seen in patients over 2
years of age. They are also more commonly ileo-ileal intussus-
ceptions and can recur if not excised.
Possible pathological lead points are listed in Box 1 and
associated conditions are listed in Box 2.
The first consequence of intussusception is bowel obstruction,
the second is compromise of the intussuscepted bowel: the
intussuscipiens distends, the intussusceptum and its mesentery
are compressed, and there will initially be lymphatic and venous
outflow obstruction, bowel wall oedema, followed by arterial
obstruction and eventually bowel necrosis.
Spontaneous reduction of intussusception undoubtedly
occurs. However, the natural history of the condition is to
progress to sepsis and death, unless it is recognized and treated
successfully.
Presentation
Over 80% of patients have episodes of colicky abdominal pain
with screaming, drawing up the legs and pallor. The episodes
recur every 10e20 minutes. Around 80% of patients vomit. This
may be early due to the pain or late due to obstruction when it
becomes bilious. Around a third of patients pass blood per
rectum with what is classically described as ‘redcurrant jelly’
stool. These are dark red mucoid clots that result from
compression of the mucous glands within the intussusceptum
plus bowel ischaemia and sloughing of the mucosa e this is
therefore a later sign. Most patients do not pass much stool after
they have emptied their colon since they are obstructed; however
up to 20% of patients may have had diarrhoea as a prodromal
illness. Only one-third of patients have the triad of colicky
abdominal pain, vomiting and bloody stools.
These are generally previously fit and well children, well
nourished and in good health. If early in the disease process,
between attacks the child may appear deceivingly well or asleep.
As the disease progresses, the child will become progressively
lethargic in between episodes of pain, progressively more dis-
tended due to ongoing obstruction, severely dehydrated and
shocked. Fever is a late sign due to bowel necrosis and sepsis.
Pathological ‘lead points’
C Meckel’s diverticulum
C Duplication cyst
C Polyp
C Appendix
C Ectopic pancreas
C Submucosal haematoma
C Inspissated bowel content
C Haemangioma
C Lymphoma
C Lipoma
C Carcinoid tumour
C Melanoma
C Foreign bodies (including trans-gastric-jejunal feeding tubes)
Box 1
SURGERY 31:12 627
In an episode of pain, the child may be difficult to examine,
there may be audible peristaltic rushes and a mass may be
palpable or even visible if the child is thin anywhere in the
abdomen. The classic examination finding is that of a right upper
quadrant sausage-shaped mass (present in 60e80% of cases).
Dance’s sign is the appearance of a flat or empty right lower
quadrant due to the mobile caecum having vacated the right iliac
fossa.
Rarely, the intussusceptum can be felt on rectal examination
or can be seen prolapsing through the anus. This needs to be
differentiated from a rectal prolapse as reduction of intussus-
cepted bowel misdiagnosed as a rectal prolapse could be life
threatening. If a lubricated tongue blade inserted along the side
of the protruding mass can be advanced more than 2 cm into the
anus the diagnosis of intussusception should be considered.
Postoperative intussusception tends to have an atypical
presentation and it should be suspected in any children with
prolonged or recurrent postoperative ileus. Mostly it happens
from 10 days to within a month post-surgery. It is usually ileo-
ileal. As postoperative functional ileus and adhesional
obstruction are more frequent causes for bowel obstruction
after surgery, intussusception may not be diagnosed.
Investigations
Imaging
An abdominal ultrasound scan (USS) is the preferred modality of
imaging to diagnose intussusception and often it will be the only
imaging needed. Its sensitivity and specificity approaches 100%
with an experienced operator. It may also distinguish between
ileo-ileal intussusception and ileo-colic intussusception guiding
further treatment.
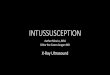
The cross-sectional view of an intussusception on USS is
characterized by the ‘target sign’ (Figure 1) e two concentric
rings of low echogenicity separated by a ring of high echogenicity
representing the walls of the intussusceptum and intussusci-
piens. Longitudinally it is characterized by the ‘pseudo-kidney
sign’ (Figure 2) e superimposed layers of low and high echo-
genicity representing the oedema of the bowel walls. Doppler can
be used to detect blood flow within the intussusception.
Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.

Figure 1 Ultrasound scan showing ‘target sign’.
PAEDIATRIC SURGERY II
A plain abdominal X-ray is no longer the investigation of
choice but may have been taken and should be studied. The
radiograph may show the features of bowel obstruction and may
give the impression of a mass (an area of paucity of bowel loops
or an opacity within a gas filled bowel loop). The target sign or
coiled spring sign is an area of concentric lucencies that repre-
sents a cross-sectional appearance of the invaginated mesentery
and bowel into the intussuscipiens. The meniscus sign is a cres-
cent-shaped lucency in the colon that represents the outlining the
distal end of the intussusceptum by gas. The right iliac fossa is
usually gas free. However, the abdominal X-ray may be normal.
A contrast enema is rarely required to make the diagnosis but
where the diagnosis is not clear, it may be diagnostic and
therapeutic.
A pathological lead point should be considered in those over
2 years of age and those with recurrent intussusceptions. An
ultrasound and a contrast study may help, but CT or MRI may be
necessary.
Laboratory
Routine baseline blood tests need to be obtained. Due to the
dehydration, blood electrolytes and renal function need to be
assessed and corrected if needed. The blood loss associated with
intussusception rarely requires transfusion.
Management
The management follows the advanced paediatric life support
(APLS) algorithms remembering that these children can present
in a very unwell state and need resuscitation before further
investigation or treatment.
Figure 2 Ultrasound scan showing ‘pseudo-kidney sign’.
SURGERY 31:12 628
Severe abdominal distension and pulmonary aspiration of
gastric content can lead to respiratory compromise. Bowel
obstruction, dehydration and ill-understood associated auto-
nomic changes in the vasculature can result in some children
having profound circulatory compromise and requiring signifi-
cant fluid resuscitation.
The patient requires an appropriately sized and functional
naso-gastric tube which is aspirated and then left on free
drainage for gastric decompression and secure intravenous
access. Sometimes supplemental oxygen and rarely endotracheal
intubation are required.
Fluid resuscitation may be needed to restore intravascular
volume with 0.9% normal saline or Hartmann’s given initially as
a 20 ml/kg bolus and then repeated up to two times if necessary
guided by monitoring with clinical reassessment to evaluate the
response to treatment. A blood transfusion might be needed if
high volumes of fluid are required and urinary catheterization
would then be appropriate. Hypothermia needs to be prevented
whilst patients are moved between different clinical areas (acci-
dent and emergency/radiology suit/theatre/ward). Intravenous
antibiotics (cefuroxime and metronidazole) should be started.
Only stabilized patients can thereafter undergo further
investigation and treatment.
Radiological reduction
An air-reduction enema under fluoroscopic guidance performed
in accordance with the guidelines of the British Society of
Paediatric Radiologists is the treatment of choice. Radiological
reduction used to be performed with barium under fluoroscopic
guidance for both diagnosis and treatment. Water-soluble
isotonic contrast has also been used as this does not carry the
risks of barium peritonitis if intestinal perforation occurs. Air-
enemas have been shown to be as equally effective and if
perforation ensues contamination is not as extensive. The
disadvantage of air-reduction is the poorer visualization of the
reduction and possible lead points and the risk of the develop-
ment of a tension pneumoperitoneum.
The procedure should only be undertaken once the child has
been resuscitated sufficiently.
The absolute contraindications to radiological reduction are
evidence of peritonitis or perforation and the identification of
a pathological lead point. Relative contraindications are the
presence of an ileo-ileal intussusception (as they are more diffi-
cult to reduce radiologically and have a higher incidence of
pathological lead points), a grossly distended abdomen and
children above the age of 3 years as they may be too uncooper-
ative for the procedure or maintain recollection of the events
which could be traumatic.
Consent should be obtained for the procedure with discussion
of the risks of failure, perforation, tension pneumoperitoneum,
cardiorespiratory collapse, need for emergency peritoneal
decompression and surgery, and of course recurrence.
The air-reduction enema takes place in the radiology suit with
adequate resuscitation equipment and expertise (APLS-trained
staff) available should the child deteriorate or arrest.
The procedure should be performed by an experienced radi-
ologist and an experienced member of the surgical team needs to
be present in order to manage the child if a tension pneumo-
peritoneum ensues.
Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.

Figure 3 Intraoperative picture of an intussusception that has been
delivered.
PAEDIATRIC SURGERY II
The child should be closely monitored throughout (heart
rate and pulse oximetry as minimum monitoring require-
ments). Antibiotics and opiate analgesia (usually as intrave-
nous morphine) are given before the start of the procedure
and naloxone should be available to be administered if
needed.
A catheter is inserted into the child’s rectum. The child is
immobilized, with the buttocks held together (in order to
achieve a tight seal around the catheter). The catheter is
attached to a pressure monitoring device, with a cut off at 120
mmHg.
Under fluoroscopic control air is insufflated into the colon to
achieve a pressure of 80e100 mmHg. This pressure is held for up
to 3 minutes in order to try and reduce oedema and then the
intussusception. Intermittent fluoroscopic screening allows one
to assess the progress of reduction of the intussusceptum. If the
first attempt fails the child should be allowed a rest before
a further attempt is made. With subsequent attempts the pressure
increases up to a maximum of 120 mmHg. Up to three attempts
are made. Successful reduction is demonstrated by the free flow
of air into the distal ileum. If doubt remains about the success of
the reduction (the IC valve may be too oedematous to allow air to
pass into the small bowel) then a repeat ultrasound scan may be
useful.
Success rates are between 75 and 80%. If symptoms have
been present for more than 48 hours the success rate is lower.
If reduction is successful the child is kept nil by mouth for
12hours beforefluids are allowed. If the child hadopiate analgesia,
monitoring needs to be continued for a periodof time as respiratory
depression may develop. Antibiotics can be stopped at 24 hours if
the child is well and discharge is usually possible within 48 hours.
If the procedure fails but the child is stable the procedure can
be repeated 2e4 hours later. If the child is not clinically well then
surgery is necessary.
Of note is the fact that recurrent intussusception can be
treated following the same principles as a first episode. The
success rate for air-enema is the same as for a first presentation,
even if it previously failed and surgery was needed.
The most significant complication of an air-reduction enema
is perforation of the bowel. If this occurs the high pressure gas
within the colon escapes and causes a tension pneumo-
peritoneum, which may compress the inferior vena cava and lead
to cardiovascular collapse. Immediate treatment is necessary
with insertion of a large-bore cannula into the abdomen to
release the pressure. Definitive management is by laparotomy.
The perforation can happen either under the form if a small
necrotic patch of bowel or a long linear tear along the anti-
mesenteric border of the bowel.
Surgery
Surgery is performed if there is a contraindication to radiological
reduction or, if this was unsuccessful, if radiological reduction
created a perforation or the parents have refused to give consent
to an air-reduction enema.
A transverse muscle-cutting incision is made on the right-
hand side of the abdomen, usually above the level of the umbi-
licus. The intussusception is delivered (Figure 3) (it is occa-
sionally necessary to mobilize the colon to achieve this).
Moderate serous ascites may be found due to the obstruction.
SURGERY 31:12 629
Once the edge of the intussusceptum is found this is gently
manipulated back upstream. Mild pressure can decrease the
oedema and help with the manoeuvre. Pulling the intussuscep-
tum should not be attempted, as it is likely to cause tearing or
perforation. If the intussusception is reduced the bowel must be
assessed for viability and to examine for a lead point. It is
important to realize that the first part of the intestine to invagi-
nate and the last part to reduce may be particularly thickened
and indented. This is commonly seen and is not a pathological
lead point and does not need resection.
Inability to reduce the intussusception, concerns over the
viability of the bowel or identification of a pathological lead
point require a resection (needed in approximately one-third to
one-half of cases) this might be a simple resection or a limited
right hemicolectomy with an end-to-end anastomosis or rarely
a diverting stoma depending on the condition of the bowel and
child.
An incidental appendicectomy may be performed especially if
a lower incision has been selected.
Postoperatively the child should have a naso-gastric tube in
place, receive adequate analgesia, fluids and antibiotics and be
monitored closely. Normally it is possible to start oral fluids 12e
24 hours after once any ileus has settled. Patients should only be
discharged when eating and stooling normally.
Laparoscopy started being used for diagnostic purposes only.
However its role in managing intussusception is evolving with
some surgeons are using it to attempt reduction only and if
unsuccessful they proceed to a laparoscopic-assisted procedure
(by exteriorization of the bowel through a periumbilical incision)
or converting to open, but some centres are using laparoscopy
even if bowel resection is needed.
The majority of surgeons will be using a three-port technique
(one infraumbilical port, two ports on the left-hand side of the
abdomen). An atraumatic bowel clamp is used to grasp the
intussusceptum and an intestinal grasping forceps is used to hold
the caecum. The caecum is then pushed away while pressure is
applied distal to the intussuscipiens.
The main difference from the open technique is that traction
on the proximal bowel is usually required.
Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.

PAEDIATRIC SURGERY II
Outcome
If diagnosed and treated promptly, the current prognosis of
intussusception is excellent, with patients having no long-term
complications.
There is a 1% risk of perforation with air-enema reduction,
more likely if the history is long (>48 hours). Post-perforation
the main risk is respiratory compromise due to tension pneu-
moperitoneum that needs to be decompressed immediately, any
peritoneal contamination tends to be minimal.
The recurrence rate is less than 5%. In 30% of cases it occurs
within 24 hours, in 70% of cases within 6 months. Recurrence is
less likely after surgical treatment.
Intussusception has a mortality (<1%) with deaths associated
with a delay in diagnosis, inadequate fluid resuscitation, inade-
quate antibiotic cover and failure to recognize recurrent or
residual intussusception following reduction.
SURGERY 31:12 630
Future
Slow hydrostatic reduction with saline enema under ultrasound
guidance has been reported in China with 95.5% of 5218
patients having successful reduction and a perforation rate of
0.17% with no mortality. This method has the advantage of not
requiring radiation and might be an alternative to current
practice. The likely increased reduction rate may be due to the
time over which reduction takes place. Oedema may be more
likely to resolve with gentle pressure applied over a longer time
than with the three short, sharp, high-pressure periods currently
employed. A
FURTHER READING
Grosfeld JL. Pediatric surgery. 6th edn. Philadelphia: Mosby Elsevier, 2006.
Crown Copyright � 2013 Published by Elsevier Ltd. All rights reserved.