Embed Size (px)
Citation preview
JOURNAL OF CLINICAL MICROBIOLOGY,0095-1137/01/$04.0010 DOI: 10.1128/JCM.39.2.804–807.2001
Feb. 2001, p. 804–807 Vol. 39, No. 2
Copyright © 2001, American Society for Microbiology. All Rights Reserved.
CASE REPORTS
Invasive Fungal Sinusitis and Meningitis Due to Arthrographiskalrae in a Patient with AIDS
PETER V. CHIN-HONG,1 DEANNA A. SUTTON,2 MARGUERITE ROEMER,3 MARK A. JACOBSON,1
AND JUDITH A. ABERG1,2*
Department of Medicine, University of California, San Francisco, and the Medical Service, San Francisco GeneralHospital,1 and Department of Laboratory Medicine, University of California, San Francisco General Hospital,3
San Francisco, California, and Fungus Testing Laboratory, Department of Pathology, The University ofTexas Health Science Center, San Antonio, Texas2
Received 20 June 2000/Returned for modification 13 September 2000/Accepted 4 November 2000
We report the first described case of Arthrographis kalrae pansinusitis and meningitis in a patient with AIDS.The patient was initially diagnosed with Arthrographis kalrae pansinusitis by endoscopic biopsy and culture.The patient was treated with itraconazole for approximately 5 months and then died secondary to Pneumocytiscarinii pneumonia. Postmortem examination revealed invasive fungal sinusitis that involved the sphenoid sinusand that extended through the cribiform plate into the inferior surfaces of the bilateral frontal lobes. There wasalso an associated fungal meningitis and vasculitis with fungal thrombosis and multiple recent infarcts thatinvolved the frontal lobes, right caudate nucleus, and putamen. Post mortem cultures were positive for A.kalrae.
CASE REPORT
The patient was a 33-year-old man with AIDS (CD41 T-cellcount, 7 cells/ml; human immunodeficiency virus [HIV] type 1[HIV-1] RNA viral load, 82,000 copies/ml) who was receivinghighly active antiretroviral therapy and who was initially ad-mitted to the hospital with a 4-day history of increasing bilat-eral retroorbital pain. The patient had just finished an 8-weekcourse of nafcillin for osteomyelitis. The patient’s past medicalhistory included cytomegalovirus retinitis with left-eye blind-ness, Pneumocystis carinii pneumonia, disseminated Mycobac-terium avium complex infection, recurrent oral candidiasis, andchronic renal insufficiency. The patient’s medications includedsaquinavir, nelfinavir, lamivudine, azithromycin, ethambutol,ganciclovir, filgrastim, epoetin alfa, nystatin, and fluconazole.A computed tomography scan showed severe maxillary, eth-moid, and sphenoid sinusitis. The patient was initially startedon piperacillin-tazobactam, and nafcillin was restarted. Even-tually, the patient was discharged and was given ciprofloxacinand clindamycin, with symptomatic improvement. Two weekslater the patient was readmitted to the hospital with alteredmental status secondary to acute on chronic renal failure thatimproved with dialysis. However, the patient had been com-plaining of persistent headaches and retroorbital pain; thus, amagnetic resonance image (MRI) of his brain including orbit-al-sinus cuts was obtained. This showed persistent extensivepansinus disease. There was also a hyperintensity at the supe-rior aspect of the left sphenoid sinus, which resulted in concern
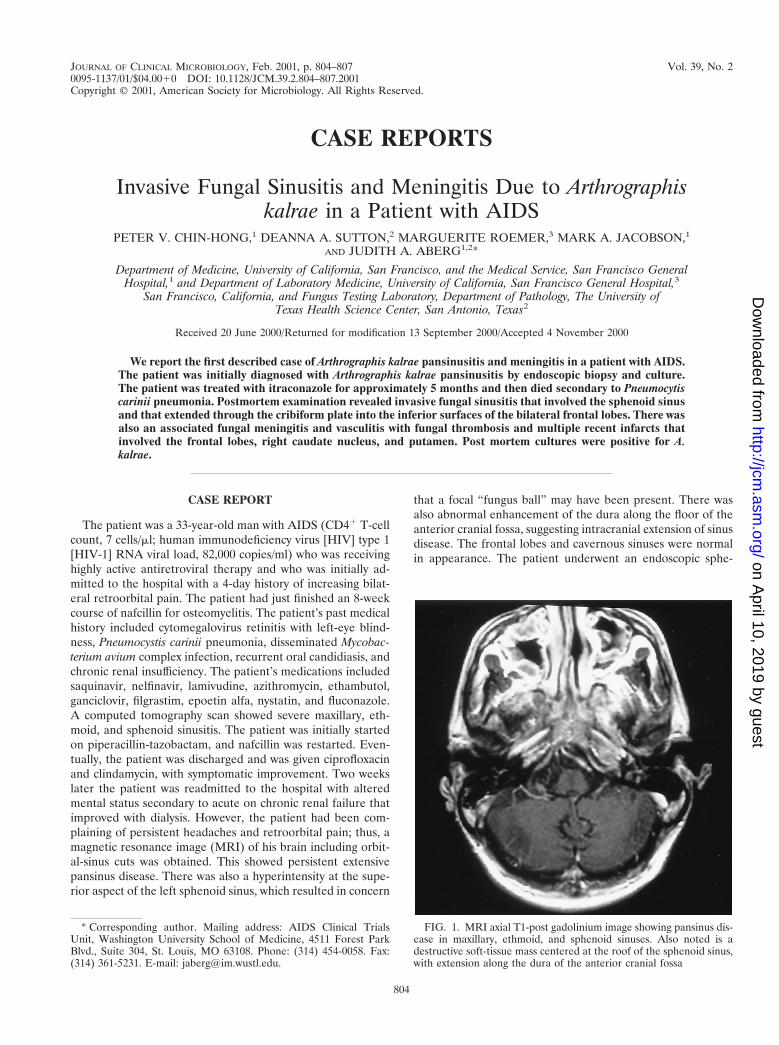
that a focal “fungus ball” may have been present. There wasalso abnormal enhancement of the dura along the floor of theanterior cranial fossa, suggesting intracranial extension of sinusdisease. The frontal lobes and cavernous sinuses were normalin appearance. The patient underwent an endoscopic sphe-
* Corresponding author. Mailing address: AIDS Clinical TrialsUnit, Washington University School of Medicine, 4511 Forest ParkBlvd., Suite 304, St. Louis, MO 63108. Phone: (314) 454-0058. Fax:(314) 361-5231. E-mail: [email protected].
FIG. 1. MRI axial T1-post gadolinium image showing pansinus dis-ease in maxillary, ethmoid, and sphenoid sinuses. Also noted is adestructive soft-tissue mass centered at the roof of the sphenoid sinus,with extension along the dura of the anterior cranial fossa
804
on April 10, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

noidotomy and biopsy that revealed hyphal forms. The patientwas then started on itraconazole. Cultures of the purulentmaterial from the left sphenoid revealed Arthrographis kalrae.Subsequent MRIs over the following 3 months essentiallyshowed no interval change (Fig. 1). As there was still no evi-dence of extension into the frontal lobe parenchyma, itracon-azole therapy was continued. Five months after the patient firstpresented with sinusitis, he was admitted for respiratory dis-tress, but unfortunately, he died as a result of enterococcalsepsis and P. carinii pneumonia. Notably, postmortem exami-nation also revealed invasive fungal sinusitis involving thesphenoid sinus and extending through the cribiform plate intothe inferior surfaces of the bilateral frontal lobes (Fig. 2).There was also an associated fungal meningitis and vasculitiswith fungal thrombosis and multiple recent infarcts involvingthe frontal lobes, the right caudate nucleus, and the putamen.Postmortem cultures were positive for A. kalrae.
Microbiology. Operatively obtained sphenoid fluid wasplated in the microbiology laboratory onto Sabouraud dextroseagar (Emmons), inhibitory mold agar, and brain heart infusionagar (Remel, Lenexa, Kan.). The media were incubated at30°C. After 48 h of incubation, cream-colored, glabrous colo-nies were observed. Microscopically, elongated oval buddingyeast cells were seen. The germ-tube test was negative. Sincethe initial morphology appeared yeast-like, the isolate wasinoculated onto an API 20C AUX identification strip (bioMerieux, Marcy l’Etoile, France). After 72 h of incubation onlyglucose was assimilated, generating an API 20C AUX profile
number of 2000000. According to the manufacturer’s database,this profile number is listed as “good likelihood but low selec-tivity” for Blastoschizomyces capitatus, Candida krusei, Torulop-sis glabrata, Candida lambica, and Hanseniaspora valbyensis.Since this profile is close to those for more than one taxonstored in the database, the manufacturer specifies that addi-tional criteria must be used to verify the identification. Addi-tional tests and the slowly emerging morphology of the isolatewere not consistent with any of the suggested organisms, and infact, A. kalrae is not included in the API 20C AUX database.
The fungus was weakly urease positive, was resistant to cy-cloheximide, did not assimilate nitrate, and grew at 37°C. After5 days of incubation, the cream-colored glabrous colonies be-came velvety due to formation of hyphae and developed a paleyellow reverse. Elongate oval blastoconidia, septate hyalinehyphae, and simple rectangular arthroconidia on conidio-phores and intercalary in the hyphae were observed (Fig. 3) inslide culture preparations stained with Myco-Perm Red (Sci-entific Device Lab, Inc., Glenview, Ill.). The slide cultures weregrown on cornmeal agar with Tween and potato dextrose agarwith thiamine (Remel). The isolate was then referred to theFungus Testing Laboratory, Department of Pathology, TheUniversity of Texas Health Science Center at San Antonio, foridentification and susceptibility testing. There the isolate wasaccessioned into the stock collection as UTHSC 97-2663 andwas subcultured onto potato flakes agar (PFA) slants, a PFAplate, and a PFA slide culture (prepared in-house) (11). Col-onies on PFA at 25°C were initially cream and moist with a
FIG. 2. Silver stain demonstrating hyphal invasion of the sphenoid bone (print courtesy of Amy Heerema, Department of Pathology, Universityof California, San Francisco).
VOL. 39, 2001 CASE REPORTS 805
on April 10, 2019 by guest
http://jcm.asm
.org/D
ownloaded from
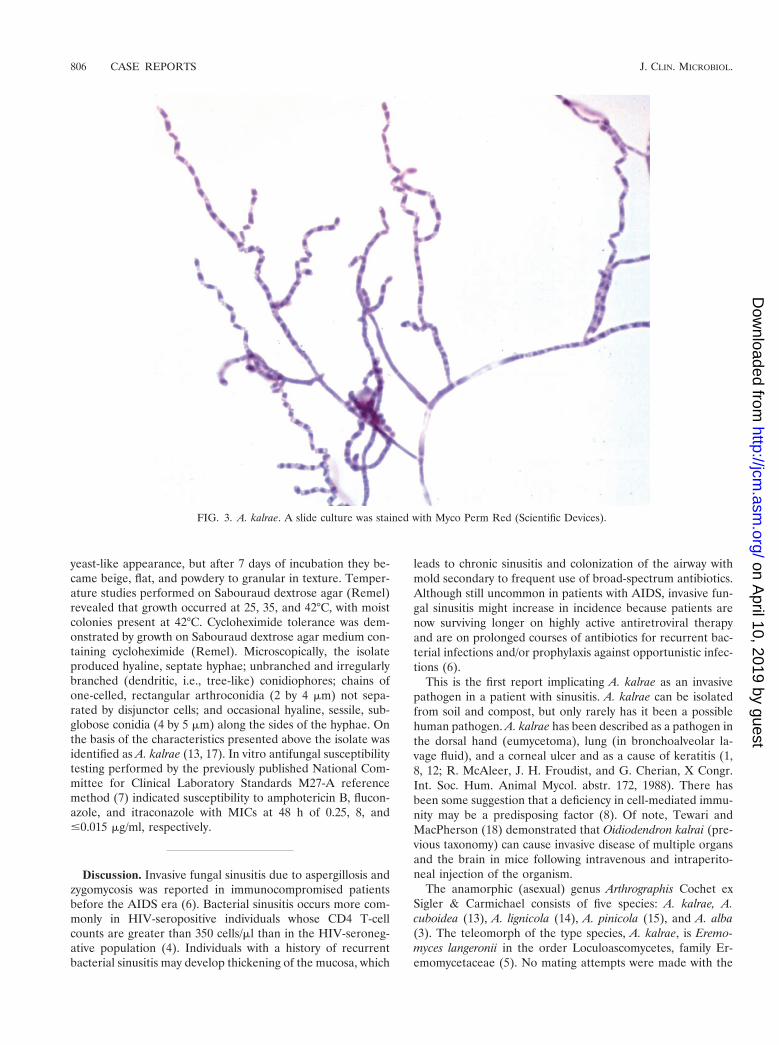
yeast-like appearance, but after 7 days of incubation they be-came beige, flat, and powdery to granular in texture. Temper-ature studies performed on Sabouraud dextrose agar (Remel)revealed that growth occurred at 25, 35, and 42°C, with moistcolonies present at 42°C. Cycloheximide tolerance was dem-onstrated by growth on Sabouraud dextrose agar medium con-taining cycloheximide (Remel). Microscopically, the isolateproduced hyaline, septate hyphae; unbranched and irregularlybranched (dendritic, i.e., tree-like) conidiophores; chains ofone-celled, rectangular arthroconidia (2 by 4 mm) not sepa-rated by disjunctor cells; and occasional hyaline, sessile, sub-globose conidia (4 by 5 mm) along the sides of the hyphae. Onthe basis of the characteristics presented above the isolate wasidentified as A. kalrae (13, 17). In vitro antifungal susceptibilitytesting performed by the previously published National Com-mittee for Clinical Laboratory Standards M27-A referencemethod (7) indicated susceptibility to amphotericin B, flucon-azole, and itraconazole with MICs at 48 h of 0.25, 8, and#0.015 mg/ml, respectively.
Discussion. Invasive fungal sinusitis due to aspergillosis andzygomycosis was reported in immunocompromised patientsbefore the AIDS era (6). Bacterial sinusitis occurs more com-monly in HIV-seropositive individuals whose CD4 T-cellcounts are greater than 350 cells/ml than in the HIV-seroneg-ative population (4). Individuals with a history of recurrentbacterial sinusitis may develop thickening of the mucosa, which
leads to chronic sinusitis and colonization of the airway withmold secondary to frequent use of broad-spectrum antibiotics.Although still uncommon in patients with AIDS, invasive fun-gal sinusitis might increase in incidence because patients arenow surviving longer on highly active antiretroviral therapyand are on prolonged courses of antibiotics for recurrent bac-terial infections and/or prophylaxis against opportunistic infec-tions (6).
This is the first report implicating A. kalrae as an invasivepathogen in a patient with sinusitis. A. kalrae can be isolatedfrom soil and compost, but only rarely has it been a possiblehuman pathogen. A. kalrae has been described as a pathogen inthe dorsal hand (eumycetoma), lung (in bronchoalveolar la-vage fluid), and a corneal ulcer and as a cause of keratitis (1,8, 12; R. McAleer, J. H. Froudist, and G. Cherian, X Congr.Int. Soc. Hum. Animal Mycol. abstr. 172, 1988). There hasbeen some suggestion that a deficiency in cell-mediated immu-nity may be a predisposing factor (8). Of note, Tewari andMacPherson (18) demonstrated that Oidiodendron kalrai (pre-vious taxonomy) can cause invasive disease of multiple organsand the brain in mice following intravenous and intraperito-neal injection of the organism.
The anamorphic (asexual) genus Arthrographis Cochet exSigler & Carmichael consists of five species: A. kalrae, A.cuboidea (13), A. lignicola (14), A. pinicola (15), and A. alba(3). The teleomorph of the type species, A. kalrae, is Eremo-myces langeronii in the order Loculoascomycetes, family Er-emomycetaceae (5). No mating attempts were made with the
FIG. 3. A. kalrae. A slide culture was stained with Myco Perm Red (Scientific Devices).
806 CASE REPORTS J. CLIN. MICROBIOL.
on April 10, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

case isolate. A. alba is distinguished from A. kalrae by beingwhite, failing to grow at 37°C, and lacking a Trichosporiellasynanamorph. A. cuboidea is distinguished by more rapidgrowth and cube-shaped arthroconidia. A. lignicola is distin-guished by broader yellow arthroconidia, while A. pinicolaforms conidiomata and fails to grow on media containing cy-cloheximide.
In patients with AIDS, sinusitis is more common and moreresistant to treatment than sinusitis in immunocompetent hosts(4, 6). The etiology is still predominantly bacterial, with Strep-tococcus pneumoniae, Haemophilus influenzae, and Moraxellacatarrhalis commonly invoked. Staphylococcus aureus andPseudomonas aeruginosa are other pathogens that have beenisolated. P. aeruginosa, an uncommon pathogen in immuno-competent patients, can account for as much as 17% of casesof acute sinusitis and 20% of cases of chronic sinusitis in theHIV-infected population (4). Bacterial sinusitis can occur atany CD4 count, but as CD4 counts decline, sinusitis becomesmore chronic. Fungal sinusitis is rarely reported and typicallyoccurs in patients with CD4 counts less than 150 cells/ml. Arecent report of sinusitis caused by Scedosporium apiospermumin an AIDS patient (2) reviewed 24 other cases of fungalsinusitis via a MedLine search: 19 were caused by Aspergillusspecies, with the others caused by Schizophyllum commune,Cryptococcus neoformans, Candida albicans, Rhizopus arrhizus,and Pseudallescheria boydii (asexual stage, Scedosporium apio-spermum). Alternaria alternata has also been reported to be acause of sinusitis (5). Management of fungal sinusitis in AIDSpatients remains controversial, with many advocating both sur-gical drainage and antifungal chemotherapy. Endoscopic sinussurgery is an outpatient procedure with minimal morbidity thathas allowed many more patients to become eligible for biopsyand to have improved sinus drainage (4, 16). The choice ofantifungal agent is unclear, with no randomized trials con-ducted given the low prevalence. In Aspergillus sinusitis, itra-conazole has been reported to be an effective alternative toamphotericin B, with various levels of success (6). Althoughthe role of antifungal susceptibility testing has not been wellvalidated and it is not known how well MICs translate intoclinical efficacy (9), it is generally accepted that factors otherthan the MIC alone may significantly affect the outcome.These factors include the pharmacokinetics of the drug, gen-eral host factors, sites of infection, and the virulence of thepathogen (10). Above all, despite the most aggressive andcombined therapy, fungal sinusitis can be a relentlessly pro-gressive disease. The case described here demonstrates that A.kalrae has the potential to cause invasive sinusitis in an immu-nocompromised host.
This research was supported by a grant from the National Institutesof Health, University of California San Francisco—Gladstone Instituteof Virology and Immunology Center for AIDS Research (P30MH59037).
REFERENCES
1. Degavre, B., J. M. Joujoux, M. Dandurand, and B. Guillot. 1997. First reportof mycetoma caused by Arthrographis kalrae: successful treatment with itra-conazole. J. Am. Acad. Dermatol. 37:318–320.
2. Eckburg, P. B., A. R. Zolopa, and J. G. Montoya. 1999. Invasive fungalsinusitis due to Scedosporium apiospermum in a patient with AIDS. Clin.Infect. Dis. 29:212–213.
3. Gene, J., J. M. Guillamon, K. Ulfig, and J. Guarro. 1996. Studies on kera-tinophilic fungi. X. Arthrographis alba sp. nov. Can. J. Microbiol. 42:1185–1189.
4. Lee, K. C., and T. A. Tami. 1999. Otolaryngologic manifestations of HIVdisease, p. 564–567. In P. T. Cohen, M. A. Sande, and P. A. Volberding (ed.),The AIDS knowledge base, 3rd ed. Lippincott, Williams & Wilkins. Phila-delphia, Pa.
5. Malloch, D., and L. Sigler. 1988. The Eremomycetaceae (Ascomycotina).Can. J. Bot. 66:1929–1932.
6. Meyer, R. D., C. R. Gaultier, J. T. Yamashita, R. Babapour, H. E. Pitchon,and P. R. Wolfe. 1994. Fungal sinusitis in patients with AIDS: report of 4cases and review of the literature. Medicine 73:69–78.
7. National Committee for Clinical Laboratory Standards. 1997. Referencemethod for broth dilution antifungal susceptibility testing of yeasts. Ap-proved standard M27-A. National Committee for Clinical Laboratory Stan-dards, Wayne, Pa.
8. Perlman, E. M., and L. Binns. 1997. Intense photophobia caused by Arthrog-raphis kalrae in a contact lens-wearing patient. Am. J. Opthalmol. 123:547–549.
9. Pfaller, M. A., J. H. Rex, and M. G. Rinaldi. 1997. Antifungal susceptibilitytesting: technical advances and potential clinical applications. Clin. Infect.Dis. 24:776–784.
10. Rex, J. H., M. A. Pfaller, J. N. Galgiani, M. S. Bartlett, A. Espinel-Ingroff,M. A. Ghannoum, M. Lancaster, F. C. Odds, M. G. Rinaldi, T. J. Walsh,A. L. Barry, and Subcommittee on Antifungal Susceptibility Testing of theNational Committee for Clinical Laboratory Standards. 1997. Developmentof interpretive breakpoints for antifungal susceptibility testing: conceptualframework and analysis of in vitro-in vivo correlation data for fluconazole,itraconazole, and Candida infections. Clin. Infect. Dis. 24:235–247.
11. Rinaldi, M. G. 1982. Use of potato flakes agar in clinical mycology. J. Clin.Microbiol. 15:1159–1160.
12. Sigler, L., and M. J. Kennedy. 1999. Aspergillus, Fusarium, and other oppor-tunistic moniliaceous fungi, p. 1212–1241. In P. R. Murray, E. J. Baron,M. A. Pfaller, F. C., Tenover, and R. H. Yolken (ed.), Manual of clinicalmicrobiology, 6th ed. ASM Press, Washington, D.C.
13. Sigler, L., and J. W. Carmichael. 1976. Taxonomy of Malbranchea and someother hyphomycetes with arthroconidia. Mycotaxon 4:349–488.
14. Sigler, L., and J. W. Carmichael. 1983. Redisposition of some fungi referredto Oidium microspermum and a review of Arthrographis. Mycotaxon 18:495–507.
15. Sigler, L., Y. Yamaoka, and Y. Hiratsuka. 1990. Taxonomy and chemistry ofa new fungus from bark beetle infected Pinus contorta var. latifolia. Part 1.Arthrographis pinicola sp. nov. Can. J. Microbiol. 36:77–82.
16. Sooy, C. D. 1987. Impact of AIDS on otolaryngology head and neck surgery,p. 1–27. In E. N. Meyers (ed.), Advances in otolaryngology. Head and necksurgery, vol. 1. YearBook, Chicago, Ill.
17. Sutton, D. A., A. W. Fothergill, and M. G. Rinaldi. 1998. Guide to clinicallysignificant fungi. The Williams & Wilkins Co., Baltimore, Md.
18. Tewari, R. P., and C. R. MacPherson. 1968. Pathogenicity and neurologicaleffects of Oidiodendron kalrai for mice. J. Bacteriol. 95:1130–1139.
VOL. 39, 2001 CASE REPORTS 807
on April 10, 2019 by guest
http://jcm.asm
.org/D
ownloaded from





























