Embed Size (px)
Citation preview

26ournal of Neurology, Neurosurgery, and Psychiatry 1996;60:256-274
NEUROLOGICAL INVESTIGATIONS
Investigation of muscle disease
F L Mastaglia, N G Laing
Various pathological processes, some geneti-cally determined and others acquired, may
Australian affect the function of the skeletal muscles andNeuromuscular may manifest in different ways. Some, such asResearch Institute, the congenital myopathies, produce weaknessUniversityDepartments of and hypotonia at birth whereas others do notMedicine and cause functional abnormalities until child-
Department of hood, adolescence, or adult life. With theNeurology and Clinical application of modem molecular biologicalNeurophysiology, techniques major advances have taken place inQueen Elizabeth IIMedical Centre, Perth, the identificaton of the genetic mutationsWestern Australia responsible for many of the hereditary muscleF L Mastaglia diseases and new mutations in nuclear orN G Laing mitochondrial DNA are being reported on aCorrespondence to regular basis. 2 These discoveries have had a
Department of Medicine, major impact on the diagnostic approach toCentre, GBlock, Nedlands, patients with these disorders and have led toWestern Australia 6009. the definition of new categories of myopathy
Table 1 Drug induced muscle disorders
Disorder Inducing drug
Myalgia Suxamethonium, danazol, clofibrate, salbutamol, lithium, captopril,colchicine, procainamide, metolazone, cytotoxics, zidovudine,isoetherine, zimeldine, labetalol, pindolol, cimetidine, penicillamine,gold, enalapril, rifampicin, i.-tryptophan, nifedipine
Myotonia Diazacholesterol, ,¢blockers,* «-agonists (fenoterol, ritodrine),*clofibrate,t diuretics (frusemide, ethacrynic acid, mersalyl,acetazolamide)t
Necrotising Alcohol, gemfibrozil, lovastatin, simvastatin, clofibrate, E-aminocaproicmyopathy acid, cyclosporin, zidovudine, cocaine, emetine
Mitochondrialmyopathy Zidovudine
Inflammatorymyopathy D-penicillamine, i.-tryptophan, others rarely
Autophagic myopathy Chloroquine, vincristine, colchicine, amiodarone, perhexilineType 2 atrophy CorticosteroidsLocalised myopathy Intramuscular antibiotics, narcotics
*May exacerbate myotonia.tMay cause myotonia in animals.
Table 2 Disorders in which muscle pain may be a prominent feature
Inflammatory HereditaryViral myositis Disorders of glycogen metabolismPyomyositis Carnitine palmityl transferase deficiencyParasitic myositis Myoadenylate deaminase deficiencyPolymyositis/dermatomyositis Mitochondrial myopathyGranulomatous myositis DystrophinopathyInterstitial myositis Sodium channel myotoniaLocalised nodular myositis Malignant hyperthermiaVasculitisEosinophilic fasciitis Others
FibromyalgiaToxic Polymyalgia rheumaticaAcute alcoholic myopathy Postviral myalgia/fatigueAcute/subacute drug induced myopathies Muscle overuse syndromesMyopathies due to envenomation Myopathy with tubular aggregates
EndocrineHypothyroidismOsteomalaciaHyperparathyroidism
such as the dystrophinopathies, encompassingthe Duchenne and Becker forms of musculardystrophy, the sarcoglycanopathies, whichinclude many cases of limb-girdle musculardystrophy, and the channelopathies comprisingthe periodic paralyses and myotonic syn-dromes.
This review focuses on the modernapproach to the clinical and laboratory investi-gation of patients with muscle diseases withparticular emphasis on the application of mole-cular techniques in diagnosis.
Clinical evaluationThe investigation of a patient with muscle dis-ease should always commence with a detailedhistory which, in the case of known hereditarydisorders, may provide an immediate indica-tion of the nature of the patient's condition.Moreover, a history of heavy alcohol con-sumption or administration of drugs withknown myotoxic actions (table 1) may point toa toxic and therefore potentially reversibleaetiology for the patient's symptoms.3 A his-tory of a thyroidectomy or parathyroidectomy,or symptoms of hypothyroidism or hyperthy-roidism, should alert the physician to the possi-bility of an endocrine cause whereas a historyof chronic diarrhoea, purgative misuse, orexcessive consumption of liquorice or otherpreparations containing glycyrrhizinic acidsuch as snuff, chewing tobacco, and certaintraditional Chinese medicines, should suggestthe possibility of hypokalaemic myopathy. Ahistory of malignancy, of a systemic connec-tive tissue disease, other autoimmune disease,or immunodeficiency state may indicate a pre-disposition to an inflammatory myopathy.When muscle pain is a feature, hypothyroid,
osteomalacic or other metabolic myopathy,parasitic infestation (for example, trichinosis),or a toxic myopathy or neuromyopathy shouldbe considered, (table 2), although in manypatients no specific aetiology will be foundeven with complete investigation. Myalgia,muscle weakness, or fatigue developing afteran acute viral infection also raises the possibil-ity of an inflammatory myopathy but in manysuch patients when fatigue and reduced exer-cise tolerance are the major symptoms, a diag-nosis of postviral chronic fatigue syndromewill usually be reached.
256
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
In certain instances it may be possible toreach a definitive diagnosis on the basis of thepattern of muscle involvement found on clinicalexamination or the finding of other distinctivefeatures such as myotonia, fatiguability, musclecontractures, or other systemic features.Although the distribution of muscle involve-ment in most of the acquired myopathies is rel-atively non-selective, in the genetic myopathiescertain patterns of muscle weakness are distinc-tive and may be diagnostically helpful although itis being increasingly recognised that the pheno-typic manifestations of specific genetic defectsmay be very variable (for example, the dys-trophinopathies). Involvement of the extraocu-lar and eyelid muscles is seen characteristicallyin oculopharyngeal muscular dystrophy, usuallyassociated with dysphagia and often with limbmuscle involvement. They are also involved inthe syndrome of chronic progressive externalophthalmoplegia, which is usually due to amitochondrial myopathy and may occur in iso-lation, or with a limb myopathy, or other sys-temic features such as pigmentary retinopathy,heart block, cerebellar ataxia, and sensorineuralhearing loss as in the Kearns-Sayre syndrome.Involvement of the facial muscles is usually aprominent feature in facioscapulohumeral mus-cular dystrophy but may also occur in myasthe-nia gravis, when it is usually associated withinvolvement of the extraocular muscles, andoften of the bulbar and limb muscles; fatigua-bility is a prominent feature. In myotonic dys-trophy there is often also involvement of thefacial muscles and, characteristically, there isatrophy and weakness of the sternomastoidsand of the distal limb muscles in the later stagesof the disease. Other systemic features whichpoint to the diagnosis include cataracts and, inmen, frontal baldness and testicular atrophy.Severe weakness of the neck extensor musclesleading to the "dropped head syndrome"6 mayoccasionally be the presenting feature inpatients with inflammatory myopathy and mayalso occur in motor neuron disease and long-standing myasthenia gravis. Weakness confinedto or most severe in the distal limb muscles alsooccurs in the distal myopathies and scapuloper-oneal syndrome.The limb-girdle syndrome, in which there is
involvement of the girdle and proximal limbmuscles, is relatively non-specific and may beseen in several genetic and acquiredmyopathies. Although in most cases ofpolymyositis and dermatomyositis there is apredominantly proximal pattern of muscleinvolvement, in inclusion body myositis the dis-tribution of muscle weakness is characteristi-cally selective, at least in the earlier stages of thecondition, with involvement especially of thequadriceps femoris muscles in the lower limbsand the forearm flexors, particularly the flexordigitorum profundus, in the upper limbs.7When present, the characteristic skin rash ofdermatomyositis over the face and the extensoraspects of the metacarpophalangeal and inter-phalangeal joints is diagnostic of that condition.
Muscle hypertrophy, when confined to thecalves, is seen most typically in Duchenne andBecker dystrophy, but occasionally also in
other types of muscular dystrophy or spinalmuscular atrophy, whereas more generalisedhypertrophy is common in myotonia con-genita. A hypertrophic myopathy may occa-sionally occur in patients with amyloidosis,sarcoidosis, or cysticercosis. Muscle contrac-tures occur, especially in Emery-Dreifuss mus-cular dystrophy, and are also a feature of thefibrosing myositis associated with scleromyx-oedema.8 It is always worth looking for muscletenderness, which, when confined to certainmuscles such as those of the calves, may indi-cate a focal inflammatory or vasculitic process,whereas the characteristic pattern of myofas-cial tenderness in patients with fibromyalgia isvirtually diagnostic of that condition.
Depressed deep tendon reflexes or sensoryabnormalities in a patient with a myopathysuggest the presence of an associated periph-eral neuropathy. This combination can occurin patients with drug induced neuromyopathy,connective tissue disease, inclusion bodymyositis, a paraneoplastic syndrome, or mito-chondrial myopathy.
Biochemical studiesCREATINE KINASEThe serum concentration of creatine kinase isthe most reliable biochemical indicator ofmuscle disease. The highest concentrationsoccur in patients with acute rhabdomyolysis,inflammatory or drug-induced myopathies,and Duchenne muscular dystrophy in theearly stages when the patient is still ambulant.High concentrations may also occur in somemetabolic myopathies such as hypokalaemic orhypothyroid myopathy. Moderately raisedconcentrations may also be found in patientswith chronic neuropathic conditions such asspinal muscular atrophy or motor neuron dis-ease, although it is rare for the creatine kinaseto exceed 10 times the normal maximum con-centration in these conditions.9 Raised crea-tine kinase concentrations may also be foundin some people, without clinical evidence ofneuromuscular disease'0 and may be useful indetecting those with a genetic risk of malig-nant hyperthermia, presymptomatic musculardystrophy, carriers of Duchenne and Beckermuscular dystrophy, and early inflammatorymyopathy (table 3). Serum creatine kinaseconcentrations are normal in most congenitalmyopathies, myotonic syndromes, and cor-ticosteroid and thyrotoxic myopathy.
Slight increases in serum creatine kinase (upto about three times the normal maximumconcentration) are not necessarily due to mus-cle disease and may occur transiently as aresult of strenuous exercise, minor muscletrauma including intramuscular injections,and insertion of EMG needle electrodes, orviral illnesses.9 In a situation where the crea-tine kinase concentration is unexpectedlyraised it is usual to repeat the test after aninterval of a week during which the patient isadvised not to engage in strenuous physicalexercise, and to consider embarking on furtherinvestigations only if the concentrationremains high or is rising.
257
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

258Mastaglia, Laing
Table 3 Causes of sustained increased serum creatinekinase concentrations in subjects without clinical signs ofmuscle diseasePhysical exerciseMuscle trauma
PressureFallsInjections
Acute psychosis/deliriumDyskinesiaeDrugs
AlcoholOthers*
HypothyroidismHypokalaemiaPresymptomatic
Malignant hyperthermiaMuscular dystrophiesInflammatory myopathiesMcArdle's disease
Carrier stateDuchenne, Becker dystrophy
Herditary hyperCKaemia
*See table 1.
Serum concentrations of other enzymessuch as aspartate and alanine aminotrans-ferase, aldolase, and lactate dehydrogenase areof less value than the creatine kinase concen-tration but may provide a clue to the presenceof muscle disease if they are found to be raisedas part of an initial biochemical screen in apatient with no other indication of liver dis-ease.
MYOGLOBINMyoglobinaemia and myoglobinuria may bedue to various causes1' and result in urinarypigmentation and a positive benzidine dipstick test on the urine as does haemoglobinuriaand haematuria. Confirmation of myoglobin-uria requires a specific myoglobin radioim-munoassay. Serum myoglobin concentrationsare raised in patients with inflammatory'2 andother necrotising myopathies but are not ofany additional value to the creatine kinaseconcentration in diagnosis or in monitoringthe response to treatment.
LACTATE CONCENTRATIONSVenous lactate concentrations may be raisedat rest and after low levels of exercise inpatients with mitochondrial myopathy anddefects of the respiratory enzyme chain.Conversely, lactate production is absent ordiminished in metabolic myopathies due todefects in glycogenolysis (for example,myophosphorylase or phosphorylase b kinasedeficiency) or of the glycolytic pathway (forexample, phosphofructokinase, phosphoglyc-erate mutase, phosphoglycerate kinase, or lac-tate dehydrogenase deficiency) and is the basisfor the forearm exercise test. This was previ-ously performed under ischaemic conditionsbut, because of the occurrence of severe rhab-domyolysis in some patients with glycogenmetabolic defects, this is no longer recom-mended.9 Venous blood samples for estima-tion of lactate and ammonia are taken at restand at 1, 2, 4, 6, and 10 minute intervals aftera one minute period of repetitive maximumisometric contractions of the forearm flexormuscles. Whereas there is normally a twofoldto threefold rise in the lactate concentrationwithin the first two minutes after exercise, thisresponse is absent or diminished in patients
with myophosphorylase deficiency or a gly-colytic defect. The rise in venous ammoniaconcentrations that normally occurs after exer-cise is absent or reduced in patients withmyoadenylate deaminase deficiency in whichammonia production during exercise isimpaired. 13
NUCLEAR MAGNETIC RESONANCESPECTROSCOPYWith NMR spectroscopy it is possible to mon-itor changes in muscle metabolite concentra-tions during exercise non-invasively (forexample, inorganic phosphate, phosphocrea-tine, ATP, lactate concentrations, and intra-cellular pH).'4 ' This may be useful in theevaluation of patients with disorders of gly-colytic or mitochondrial metabolism. Thetechnique is also useful in the evaluation ofpatients with fatigue and reduced exercise tol-erance to determine whether there is evidenceof an underlying defect of muscle energymetabolism.
OTHER STUDIESOther biochemical studies which may be rele-vant in the investigation of some patients withmuscle symptoms include serum potassium,calcium, phosphate, thyroxine, and cortisolconcentrations, as well as urea and creatinineconcentrations and urinary creatine and 3-methyl histidine excretion as indices of skeletalmuscle mass and breakdown.'6
Pharmacological testingAlthough in some families with malignanthyperthermia mutations have been found inthe ryanodine receptor gene and at risk sub-jects can therefore be detected using moleculargenetic techniques, in many other families aswell as in those without a known family historywho are suspected of being at risk, it is stillnecessary to perform in vitro muscle contrac-ture testing. This involves the exposure ofmuscle tissue obtained at biopsy to caffeineand halothane which, in at risk subjects,induce an exaggerated contractile response.Abnormal responses to caffeine and calciumions have also been described using theskinned muscle fibre technique.'7 Contracturetesting should also be performed in those withunexplained episodes of muscle stiffness orrhabdomyolysis during or after anaesthesia,with infections, or after exercise or heat expo-sure, and in patients with central core or multi-core disease who are also at risk.
Electrodiagnostic studiesELECTROMYOGRAPHYConventional EMG is an important investiga-tive procedure in patients with suspected mus-cle disease. Firstly, it will often provideconfirmation of a primary myopathic basis forthe patient's condition and allow differentia-tion from a neurogenic disorder. Charac-teristically, the duration of motor unit actionpotentials (MUAPs) is diminished as isMUAP amplitude although this is often less
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
pronounced and more variable, and there is anincreased number of polyphasic motor unitpotentials. With voluntary contraction there isearly recruitment of increased numbers ofshort duration MUAPs and an unduly fullinterference pattern which is often reduced inamplitude. Reduced motor unit recruitmentand electrical excitability of the muscle arefound during attacks of weakness in patientswith periodic paralysis. Spontaneous fibrilla-tion potentials, positive sharp waves, and com-plex repetitive discharges may be found insome myopathic disorders and are particularlyprominent in active inflammatory myopathiesand certain metabolic and toxic myopathies(for example, hypothyroid and chloroquinemyopathy), in some cases of Duchenne mus-cular dystrophy and distal myopathy, and inmyotonic disorders in which they are associ-ated with a pronounced increase in insertionalactivity and the diagnostic waxing and waning("dive bomber") myotonic discharges result-ing from electrical instability of the muscle cellmembrane.'8 The occurrence of spontaneouspotentials in non-myotonic myopathies hasbeen attributed to functional denervation ofmuscle fibres which have been disconnectedfrom their motor innervation as a result of seg-mental necrosis. Regenerating muscle fibreswhich have yet to be innervated may also be asource of spontaneous potentials.The distribution of EMG changes within
individual muscles and in representative proxi-mal and distal limb and axial muscles providesan indication of the extent of the myopathicprocess and pattern of muscle involvement.This may be useful in selecting a muscle forbiopsy, and may also indicate whether the dis-ease process is one which is affecting the mus-cles in a patchy manner (often the case in theinflammatory myopathies) or more diffusely(as in the muscular dystrophies or metabolicmyopathies). The coexistence in the samemuscle of typical myopathic MUAPs andlonger duration polyphasic potentials is apotentially confusing combination sometimesencountered in patients with very longstandingdenervating conditions such as spinal muscu-lar atrophy,'8 and in inclusion body myositis inwhich there may also be prominent fibrillationpotentials as well as increased fibre densityand jitter.'9
Although in many patients with well estab-lished myopathies the EMG changes are floridand unmistakable, in some patients withmilder forms of myopathy the motor unitchanges are less conspicuous. It is in the evalu-ation of such patients that quantitative tech-niques employing automated measurement ofMUAP variables and motor unit recruitmentfor given levels of effort are useful.'8
NEUROMUSCULAR TRANSMISSION STUDIESRepetitive nerve stimulation studies should beperformed if muscle fatigue is prominent or ifthere are other features suggestive of myasthe-nia gravis or of the Lambert-Eaton myasthenicsyndrome or other neuromuscular junctiondisorder.
Single fibre electromyography (SFEMG),
which can be performed either with voluntarymuscle activation or with nerve stimulation,characteristically shows increased jitter andintermittent blocking indicating failure of trans-mission at single motor endplates, and is moresensitive than repetitive nerve stimulation studiesin the diagnosis of neuromuscular transmissiondisorders.
In myasthenia gravis SFEMG shows anabnormality in up to 95% of patients with limbinvolvement and a normal SFEMG study in apatient with clearcut limb weakness and fatigueis strongly against the diagnosis of myasthe-nia.'8 However, similar abnormalities may befound in several myopathies and other neuro-muscular disorders and it is therefore essentialthat the findings are interpreted in the contextof the particular clinical situation.
NERVE CONDUCTION STUDIESMotor and sensory nerve conduction studies aswell as F wave and H reflex studies may beappropriate to exclude the possibility that thepatient's symptoms are due to a peripheral neu-ropathy. Moreover, a peripheral neuropathymay coexist in some patients with myotonicdystrophy, mitochondrial myopathy, druginduced myopathy, inclusion body myositis, orinflammatory myopathy associated with con-nective tissue diseases or malignancy.
Muscle imagingThe techniques of CT and MRI can provideinformation on the cross sectional area of limbor axial muscles and may therefore be useful indetecting muscle atrophy or hypertrophy anddefining selective patterns of muscle involve-ment in certain conditions such as the musculardystrophies and inclusion body myositis.20 21These techniques may also show differences inmuscle properties between conditions such asthe muscular dystrophies in which there isextensive fatty infiltration of muscle, and theinflammatory myopathies, but the changes arenot sufficiently specific to be of diagnosticvalue.22 The techniques are, however, of use indetecting and defining the extent of suppurativelesions of muscle (pyomyositis). Radioisotopictechniques with muscle scanning after adminis-tration of technitium pyrophosphate can also beused to detect such lesions as well as areas ofactive inflammatory myopathy in patients withpolymyositis or dermatomyositis, and areas ofmuscle infarction or pressure necrosis (crushsyndrome). Isotopic scanning may also be usedto show the extent of subcutaneous calcinosis inpatients with dermatomyositis and to monitorchanges with treatment.
Muscle biopsyA biopsy is still required to provide a definitivediagnosis in the case of many muscle diseases.This is especially so in the case of the inflam-matory myopathies, in sporadic cases ofmuscu-lar dystrophy, suspected metabolic myopathies,and in patients in whom there is still uncer-tainty as to whether the condition is primarilyneuropathic or myopathic after clinical and
259
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
EMG evaluation. In neuropathic disorders abiopsy from an affected muscle will show thecharacteristic changes of denervation includingangulated fibres, grouped fibre atrophy, and, ifthe condition is protracted, fibre type grouping,but will not necessarily differentiate betweenanterior horn cell and peripheral nerve disor-ders. In the more chronic neurogenic disor-ders-such as the spinal muscular atrophies-histological changes resembling those found inchronic myopathic disorders may also be pre-sent (secondary myopathic change).The effectiveness of muscle biopsy in estab-
lishing the diagnosis of myopathy is deter-mined by the correct choice of muscle, thecorrect biopsy technique, and the applicationof the appropriate staining and other proce-dures to the biopsy.23 In selecting a suitablebiopsy site the ideal muscle is one which isonly moderately affected (for example, withMRC grade 4 muscle power), and which hasnot been the site of previous intramuscularinjections or needle EMG studies. Muscleswhich are too severely weakened or atrophicshould be avoided as the histological changesin such muscles are often non-specific and dif-ficult to interpret. Selection of a needle oropen biopsy is determined by personal choice,experience, and availability. Whereas needlebiopsy requires only a minor incision and theprocedure can be repeated at multiple sitesand on more than one occasion, the size of thetissue sample obtained is limited and histologi-cal interpretation may be difficult, particularlyin diseases in which the muscle involvement ispatchy. In many instances therefore, and espe-cially in the case of suspected inflammatorymyopathy or vasculitis, an open biopsy ispreferable, having the advantage of providing alarger tissue sample and thereby reducingsampling error.To maximise the information derived from
the muscle biopsy a battery of histological andhistochemical stains should be applied rou-tinely to cryostat sections of frozen tissue. Inaddition, in some cases it will be necessary toapply other selected histochemical orimmunohistochemical techniques using mon-oclonal antibodies for the diagnosis of specificenzyme deficiencies, storage disorders, orother hereditary defects such as the dys-trophinopathies and sarcoglycanopathies.Electron microscopic examination of muscletissue is also necessary especially in cases ofsuspected mitochondrial myopathy, inclusionbody myositis, and in some congenitalmyopathies. Tissue should therefore be takenroutinely for this purpose at the time of thebiopsy and fixed in glutaraldehyde.23 In meta-bolic and other inherited myopathies it is alsoprudent to obtain an additional tissue samplefor quantitative biochemical analyses or molec-ular studies should these be required.
In the hereditary myopathies, immunohisto-chemistry of muscle biopsies should be usedwhenever possible to identify the patient orfamily muscle disease. For example, the auto-somal recessive Duchenne-like muscular dys-trophies and the limb-girdle dystrophies canbe very difficult to distinguish from Duchenne
and Becker dystrophy clinically, whereas anti-bodies can make the distinction very easily.Up until recently these cases were among theresidual of patients all muscle clinics have whoare difficult to categorise. For example,Bonnemann et al 24 in their recent characterisa-tion of mutations in ,8-sarcoglycan screened 62patients with possible ,B-sarcoglycan involve-ment out of a bank of 2500 muscle biopsies toidentify their one ,B-sarcoglycan patient. In ourown clinic, screening nine families undiag-nosed for years, with antibodies to adhalin,showed that three of the families were a-sarco-glycan (adhalin) negative (RD Johnson andBA Kakulas, unpublished observations) andthus are at risk from a sarcoglycanopathy.Immunohistochemistry or immunoblottingcan also predict the severity of disease forexample, in both the dystrophinopathies25 27and the sarcoglycanopathies2' 28 On the otherhand, molecular analysis cannot always pre-dict severity of disease, as people with appar-ently the same mutation can have differentseverities of disease29 perhaps due to alternatesplicing around the mutation.3"
Molecular diagnosisMolecular biology, particularly positionalcloning, has led to the recent major increase inunderstanding of the causes of inherited dis-eases, through identifying the genes mutatedin these diseases and thus the faulty proteins.32In the muscle clinic, similar molecular tech-niques can be used for four major purposes:* Identifying the precise disease affecting anindividual patient and family.* Accurate, simple prenatal diagnosis* Identifying asymptomatic members of fam-ilies who are at risk from having more severelyaffected offspring* Presymptomatic diagnosis.All of these lead to more accurate and appro-priate genetic counselling.
IDENTIFYING THE PRECISE DISEASE AFFECTINGAN INDIVIDUAL PATIENT AND FAMILYMolecular diagnosis is especially useful forconditions which are difficult to distinguishclinically or by other laboratory techniques.The sarcoglycanopathies,33 in which mutationsin adhalin, 8B-sarcoglycan, and y-sarcoglycanall look similar by immunohistochemistry, are agood example of diseases only distinguishableby molecular analysis.34
ACCURATE, SIMPLE PRENATAL DIAGNOSISIdentifying the precise mutation or mutationscausing the disease in a family also providesthe only really practical route to prenatal diag-nosis where that is appropriate. The only cur-rent alternative for inherited muscle diseaseswould be fetal muscle biopsy. 33
IDENTIFYING ASYMPTOMATIC MEMBERS OFFAMILIES WHO ARE AT RISK FROM HAVINGMORE SEVERELY AFFECTED OFFSPRINGMolecular diagnosis allows the identificationof minimally affected or asymptomatic per-sons. This is important for identifying carriers
260
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
of X linked diseases such as Duchenne andBecker muscular dystrophy, Emery-Dreifussdystrophy, and X linked centronuclear myopa-thy who are at risk of having affected male off-spring. It is also important for tracing at risksubjects-for example, in myotonic dystrophypedigrees-through cascade screening.
PRESYMPTOMATIC DIAGNOSISPresymptomatic diagnosis using moleculartechniques has been applied, for example, todiagnose the cause of the raised creatinekinase and to screen other family membersafter neonatal or infant screening forDuchenne muscular dystrophy.3637 Presymp-tomatic diagnosis is also possible by moleculartechniques in any of the later onset diseases,such as hypokalaemic periodic paralysis.38The polymerase chain reaction (PCR),39
which amplifies specific regions of DNA, hasplayed a major part in the molecular revolu-tion and is being manipulated for ever more
purposes-such as reverse transcriptase PCR(RT-PCR) which allows PCR to amplify spe-cific cDNA messages40 or the creation ofrestriction enzyme sites to discriminatebetween normal and mutant alleles.4'
DEGREES OF EASE OF MOLECULAR DIAGNOSISThere are perhaps three degrees of difficultyfor molecular diagnosis: easy, difficult, andaverage. Easy diseases to diagnose are those inwhich most cases are caused by a single muta-tion, or a few mutations, or mutations whichare simple to detect. Difficult diseases to diag-nose are: (a) those in which most cases are
caused by many different missense mutationswhich alter only a single amino acid and thusdo not truncate the protein; (b) diseases inwhich linkage to a particular locus has beenidentified but the disease gene has not beenidentified; or (c) diseases with significantgenetic heterogeneity-that is, where the sameclinical phenotype may be caused by muta-tions in a number of different genes. Averagediseases to diagnose are those caused in mostcases by nonsense mutations which produce a
premature stop codon and therefore truncatedproteins.
Easy diseases to diagnose by molecular analysisDiseases which currently fall into this categoryare:
(1) Myotonic dystrophy, in which the tripletrepeat expansion can be detected and sized bya PCR reaction, and/or Southern blottingusing EcoRI, BglI, or BamHI digestion.42(2) Duchenne and Becker muscular dystro-phy (for most patients) as most disease caus-
ing mutations are large deletions of thedystrophin gene. These deletions can bedetected by multiplex PCR analysis of DNAfrom affected boys to identify the deletedexons.25 43-45
(3) Spinal muscular atrophy (autosomalrecessive), in which the common deletion canbe detected by two single strand conformationpolymorphism (SSCP) analyses, one for exon7 of the survival motor neuron gene and onefor exon 8.46 47
(4) Hypokalaemic periodic paralysis, in whichmutations to two residues in the dihydropyri-dine receptor calcium channel (CACNL1A3)account for all cases so far described.48(5) Mitochondrial myopathies, in which thecommon point mutations can be tested forusing PCR followed by enzyme digestion41 49 orSSCP analysis.50
Difficult diseases to diagnose by molecular analysis
Diseases in which most cases are caused by manydifferent missense mutations-Finding the muta-tions causing disease in such conditions is themost difficult task for molecular analysis. Thisis because the entire gene sequence has to bescreened, and the difficulty is thereforeincreased if the gene message is large, which isthe case for many of the structural proteins ofmuscle. The difficulty of identifying missensemutations was reinforced again in a recentsummary of current methods of screeninggenes for unknown mutations,5' which statesthat, "Detection of mutations, particularly atthe 100% level is time consuming and expen-sive" and "The 'one best method' still remainselusive". Indeed, the plethora of techniquescurrently on the market for identifyingunknown mutations in genes indicates thatnone is ideal. A previous review52 summarisedthe techniques then current such as the simplesingle strand conformation analysis (SSCA),denaturing gradient gel electrophoresis(DGGE), heteroduplex analysis (HA),RNAase A cleavage, chemical mismatch cleav-age (CMC), and direct sequencing. Tech-niques which should perhaps be added to thelist include restriction endonuclease finger-printing (REF),53 dideoxyfingerprinting,54 andenzymatic mismatch cleavage (EMC).5556The heroic way to look for mutations is to
search genomic DNA. This will often involvesynthesising PCR primers for regions flankingeach of the exons of the gene followed by, forexample, SSCP analysis of each exon. Thiswould necessitate synthesising 80 primers for agene like the cardiac ,B-myosin heavy chaingene (MYH7) involved in familial hyper-trophic cardiomyopathy-as MYH7 has 40exons-and then performing 40 separateSSCPs. The short cut alternative is to examinethe cDNA for mutations.52 This reduces thenumber of base pairs that have to be screenedcompared with examining the genomicsequence of the gene. Analysis of cDNA willalso instantly disclose any deletions or duplica-tions of the message and splice site mutationswhich also significantly alter the size of thetranscript, leading to rapid identification ofone type of single base mutation.5758 To exam-ine the cDNA however, a source of RNA isrequired from the patient in whom the candi-date gene is expressed. This should be rela-tively simple, as nearly all patients with amuscle disease should have had a musclebiopsy, and RNA can easily be extracted fromfrozen muscle tissue and cDNA synthesisedfor examination. Analysis ofcDNA made fromillegitimate transcription messages59 shouldalways be considered as a possible means of
261
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing262
obtaining cDNA for muscle disease genes.However, in some cases it may be more appro-priate to analyse cDNA from muscle, (forexample, the mitochondrial myopathies), asthe mutations in skeletal muscle may be differ-ent and more relevant than those in circulatinglvmphocvtes.60-J -.
meinsagnoialtccauamserseechsevechsmipalfurmcexjserthetusshl
preDimlclegernethdisdiEpewIobge
Pem,mre
erglire
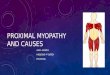
Figure 1 Proteintruncation for the deletionprone part of thedystrophin gene carried outon mRNA from musclebiopsies. Lanes 1 and 2 arefrom control musclebiopsies. Lanes 3, 4, 5,and 6 show variouslytruncated proteins in fourpatients with Duchennemuscular dystrophy.
cular dystrophies may also be included in thiscategory. Some of the different types can nowbe identified as sarcoglycanopathies or dystro-phinopathies by immunohistochemistry, but itis still a large task to precisely identify the geneinvolved by molecular diagnosis.
Suggesting that a missense mutation in any Average diseases to diagnose by molecular analysisssage is responsible for disease-especially Average diseases are those in which most muta-
a giant message like the dystrophin mes- tions causing disease are nonsense mutations,61_i2r
;e is fraught with difficulties.62 The criteria as these can be detected using the protein trun-rmally used to decide that an identified cation test (PTT).75 76 This test uses an in vitroeration in a DNA sequence is a disease translation system to synthesise protein fromising mutation include a major change of an cDNA. If there is a mutation in the proteinino acid, change of an amino acid con- coding region leading to a premature stopved in many species, the change not being codon, the protein synthesised in vitro will be:n in a large number of controls, and the shorter than normal and can be identified byange being in a candidate gene. However, electrophoresis. The PTT was first appliedm when all these criteria are fulfilled, the widely to the identification of nonsense, prema-ange may still not be disease causing.62 A ture stop codon producing, mutations in familialssense mutation found only in a single adenomatous polyposis coli75 and Duchennetient, or a small family, probably requires a muscular dystrophy,76 (fig 1), but it has also.ictional assay (not necessarily a transgenic been applied to neurofibromatosis.7778 The)use) or at least characterisation in an PTTl should perhaps be used for all recessivepression system to be certain that the mis- disorders, especially severe ones, as these are
nse mutation causes the disease.63 Unless often caused by nonsense mutations. For exam-,re is this degree of certainty about the sta- ple, the PTT would have detected many of thes of the identified alteration in DNA, it mutations so far described in the sarcogly-ould not be used for prenatal diagnosis. canopathies, especially the severe cases,24283379Diseases in which there is only linkage but the in which prenatal diagnosis would be most
?cise disease gene has not been identified- appropriate and there would be most likelihoodistal myopathy,64 65 dominant limb-girdle of pressure to rapidly find the family mutation.ascular dystrophy,6667 X linked centronu- Obviously some diseases fit into both thear (myotubular) myopathy,68 oculopharyn- easy and difficult categories or both the easyal muscular dystrophy,69 and recessive and average categories. Duchenne muscularmaline myopathy7' are all diseases in which dystrophy is both easy for most mutations andere is at present linkage but no identified average for the minority. Mitochondrialsease gene. When there is only linkage for a myopathies are easy for most cases and diffi-sease, the use of linkage for diagnosis should cult for the others. The common mtDNArhaps be restricted to individual families in point mutations can be tested relatively easily,hich the significant LOD score of 3 has been but all the other possible mutations are diffi-tained, especially if there is evidence of cult to screen for and to separate from poly-netic heterogeneity for the disease. morphisms not causing disease.80 This is alsoDiseases with significant genetic heterogeneity- true for other diseases. However, testing only!rhaps the best example of this at present is for the common known mutations becomes a
alignant hyperthermia, in which although self fulfilling prophecy and unless the rest of
any families show linkage to the ryanodine the transcript is screened for mutations, manyceptor gene on chromosome 1971 many oth- mutations causing disease may be missed.s apparently do not72 73 and virtually only sin- As emphasised by Forrest et all' it is essentiale families have shown linkage to other that comprehensive databases of gene muta-
gions ofthe genome.74 The limb-girdle mus- tions and perhaps, even more importantly,databases of normal polymorphisms should becreated and widely disseminated, so that indi-
~3 1 vidual diagnostic laboratories can cross checkwhether a base change identified in a patient isa known mutation causing disease, a known
_ftd'I'Momoma; polymorphism, or entirely new.
Muscular dystrophiesThe classification of the muscular dystrophieshas undergone considerable change with therecognition of the disease genes and molecularbasis for some of these conditions-in particu-lar, the X linked and the limb-girdle dystro-phies (table 4).' The availability of genetic or
molecular markers for many of these condi-tions has meant that the diagnosis can now beestablished with greater precision and that dis-eases manifesting with similar phenotypes can
MWimmmmww
:........ :....--.-.--.-
4I'
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
Table 4 Muscular dystrophies
Dystrophy type Locus Gene
X linked:Dystrophinopathies Xp21-2 Dystrophin
DuchenneBeckerQuadriceps myopathyMyalgia and crampsHyperCKaemia
Emery-Dreifuss Xq28 EmerinCentronuclear myopathy Xq28 ?
Autosomal dominant:FacioscapulohumeralFSHD 4q35 ?FSHD2 ? ?
Limb-girdle*LGMD1A 5q22-q34 ?LGMD1B ? ?
Distal*MPD1 14q ?
Oculopharyngeal*OPMD 14ql 1-2-q13 ?
Autosomal recessiveLimb-girdleLGMD2A 15qI5-1-q21-1 CalpainLGMD2B 2q13-pI6 ?LGMD2C (SCARMD) 13ql2 rsarcoglycanLGMD2D 17ql2-q21-33 Adhalin (a-
sarcoglycan)LGMD2E 4q12 ,B-sarcoglycan
CongenitalLAMA2 6q2 MerosinFukuyama 9q31-q33 ?
Distal (Myoshi)* 2p ?Oculopharyngeal*
*Autosomal dominant or recessive.
be readily distinguished. For example, in somepatients with Becker dystrophy who have a
dystrophin mutation the clinical phenotypemay closely resemble that of limb-girdle mus-
cular dystrophy, which is now known to haveat least seven different genetic varieties (table4). Other examples include the differentiationof merosin deficiency from a dystrophinopathyin infants with congenital muscular dystrophyand the differentiation of adhalin deficiencyfrom dystrophinopathy in the severe childhoodautosomal recessive form of muscular dystro-phy (now classified as LGMD2C). The molec-ular definition of these conditions has also hadimportant implications for the identification ofheterozygote carriers and for prenatal diagno-sis, especially in the X linked dystrophies. Ithas also led to the recognition that there is a
wide range of phenotypic expression and clini-cal severity, particularly in the dystro-phinopathies and sarcoglycanopathies.798'
DIAGNOSTIC APPROACHThe diagnostic approach to the patient with a
suspected muscular dystrophy initially involvesa detailed clinical assessment of the affectedpatient and family history which, when posi-tive, may point to an X linked disorder or toone of the distinctive forms of dominantlyinherited myopathy such as facioscapulo-humeral dystrophy or distal myopathy.Electromyography is helpful in confirming themyopathic nature of the condition and exclud-ing myotonic or chronic neurogenic con-
ditions. A raised serum creatine kinaseconcentration, although not specific, may alsobe a diagnostic pointer particularly if the con-
centration is very high as is usually the case inthe early stages of Duchenne or Becker muscu-lar dystrophy when concentrations of up to300 times normal may occur. However, in theother dystrophies less pronounced increases or
normal concentrations may be found. The highserum creatine kinase in affected boys withDuchenne dystrophy at birth has been thebasis for the development of neonatal screen-ing programmes for newborn males in somecountries.82 The detection of isolated cases byneonatal screening makes it possible to preventthe birth of secondary cases in families and ithas been estimated that it is possible to prevent15 to 20% of new cases of Duchenne dystro-phy with this type of screening.
In most instances definitive diagnosis of amuscular dystrophy and recognition of the par-ticular type still requires a muscle biopsy forroutine histology and immunohistochemicalstaining for dystrophin and for the other pro-teins of the dystrophin-glycoprotein complexsuch as the sarcoglycans. The immunohisto-chemical demonstration of complete or partialdystrophin deficiency is the gold standard forestablishing the diagnosis of Duchenne andBecker muscular dystrophy. Complete or virtu-ally complete absence of dystrophin is charac-teristic of Duchenne dystrophy whereas inBecker dystrophy there is usually patchypreservation of the protein on the sarcolemmaof muscle fibres. Dystrophin immunohisto-chemistry may therefore be of prognostic aswell as diagnostic value in differentiatingDuchenne and Becker dystrophy in youngboys. The importance of using a panel of anti-bodies to different regions of the dystrophinmolecule from the N to the C terminus hasbeen emphasised.83
Immunoblotting for dystrophin in muscletissue is a more sensitive technique, which mayshow more subtle changes in the molecular sizeor amount of dystrophin. Hoffman et al 26showed that patients with Duchenne musculardystrophy had less than 3% of the normalquantity of dystrophin, intermediate patientshad up to 60% of normal concentrations,whereas patients with Becker dystrophy mostoften had abnormal sized dystrophin ratherthan abnormal quantities.
MOLECULAR DIAGNOSISDystrophinopathiesThe main applications of molecular diagnosisare accurate diagnosis if other methods havefailed or are inappropriate, accurate diagnosisof asymptomatic subjects (in the case of theseX linked diseases this largely means carriers),and prenatal diagnosis.The dystrophin gene was the first major dis-
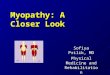
ease gene to be identified by positional cloning.The dystrophin message and the distributionof deletion mutations which cause about 70%of cases of Duchenne and Becker musculardystrophy were first described in 1987.84However, pulsed field gel electrophoresis hadalready indicated that most mutations causingDuchenne dystrophy were large deletions.85The identification of the dystrophin geneimmediately allowed much more accurate dif-ferential diagnosis of Duchenne and Beckermuscular dystrophy using the available cDNAprobes.86-88 Molecular diagnosis of boysaffected with dystrophinopathies is now carriedout by multiplex PCR of genomic DNA (fig 2),
263
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
which gives a diagnosis in hours rather than theprevious days or weeks.23 Prenatal diagno-sis is also achieved with multiplex PCR when afamily deletion has been identified, and bylinkage using microsatellites89 for the dys-trophin gene in the large minority of families inwhich deletions have not been identified.Splice site mutations in the gene can be identi-fied by RT-PCR.5758
Identification of carriers of dystro-phinopathies has been achieved with dosageSouthern blotting,90 92 presence of junctionfragments,85 and non-inheritance of alleles.93However, as with all aspects of molecular diag-nosis, carrier detection has moved to PCR;PCR dosage has been used with great accuracyto identify carriers9495 as has RT-PCR fromillegitimate transcription of the dystrophinmessage in circulating lymphocytes.40The increasing diversity of dystrophinopathy
phenotypes has been reviewed by Beggs et al96and includes quadriceps myopathy,97 crampsand myalgia,98 99 hyperCKaemia,'00 and Xlinked cardiomyopathy. '10 102
Limb-girdle muscular dystrophiesThe first recessive limb-girdle muscular dystro-phy gene to be localised (LGMD2A) was onchromosome 15103104 through linkage in fami-lies from the island of Reunion. Mutations inthe calcium activated protease gene calpainwere subsequently identified both in the fami-lies from Reunion and in the Amish familieswhich showed linkage to the chromosome 15region. 305 (Two different autosomal recessivelimb-girdle muscular dystrophies segregate inthe Amish community-the other isLGMD2E.34) The identification of calpain as
the mutant gene in LGMD2A was the firstimplication of a non-structural protein in a
muscular dystrophy.105 No abnormalities in thedystrophin associated glycoproteins were
detected in patients with LGMD2A.1'0 107
There are four other localised or identifiedrecessive limb-girdle muscular dystrophygenes: LGMD2C, LGMD2D, and LGMD2Eare the sarcoglycanopathies whereasLGMD2B, localised to the short arm of 2p,108is an as yet unidentified gene.
There are at least two genes for autosomaldominant limb-girdle muscular dystrophy, one(LGMD1A) localised on chromosome 5.6667The other (LGMD1B) is not yet localised.'9
SarcoglycanopathiesAdhalinopathy (a-sarcoglycanopathy) was thefirst sarcoglycanopathy to be identified, ini-tially by deficiency in immunohistochemicalstaining"0 and later by mutations in theadhalin gene.28111112 Adhalinopathy is alsoknown as recessive limb-girdle muscular dys-trophy type D (LGMD2D). Mutations in theother two sarcoglycans have now been demon-strated. Mutations in the /B-sarcoglycan geneon chromosome 4 are associated withLGMD2E, the second limb-girdle musculardystrophy found among the Amish34 and alsoother communities.24 Mutations in the ysarco-
glycan gene on chromosome 13 are associatedwith severe congenital autosomal recessivemuscular dystrophy (SCARMD, LGMD2C).33In each of these diseases there is a reduction ofimmunohistochemical staining for all threesarcoglycans. Thus reduction of immunostain-ing for any of the sarcoglycans in the absenceof reduction in dystrophin staining indicatesmutation in one of, at present, three genes. AsLim et al 34 state in the discussion of theirpaper, only molecular investigation of all thecandidate genes can provide a definitive diag-nosis.
Congenital muscular dystrophyCongenital muscular dystrophies are charac-
Figure 2 Duchennemuscular dystrophymultiplex PCR. Lane 1:size standard; lanes 2, 4, 6,8: patients with Duchennemuscular dystrophy; lanes3, 5, 7, 9: control: lanes 2and 3 (from top down)promotor, exons 3, 8, 50,53: lanes 4 and 5: exons13, 16, 74; lanes 6 and 7:exons 48, 43, 47, 60; lanes8 and 9: exons 19, 42, 4.Patient is deleted for at leastexons 48 and 50 (arrows).
264
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
terised by severe dystrophic changes of musclefrom birth."3 Tome et al'07 were the first toshow merosin (IAMA2) deficiency in cases ofcongenital muscular dystrophy of the occidentaltype. However, not all of the clinically indistin-guishable cases showed merosin deficiency,and this heterogeneity is yet to be explained on
a molecular basis. It is estimated that 40% ofoccidental congenital muscular dystrophycases show LAMA2 deficiency."13 Sub-sequently mutations of the LAMA2 gene were
identified in patients with congenital musculardystrophy. 114The LAMA2 gene maps to the long arm of
chromosome 6, the Japanese form of congeni-tal muscular dystrophy, Fukuyama musculardystrophy to the long arm of chromosome 9,115and thus a different as yet unidentified genemust be involved. Fukuyama muscular dystro-phy and Walker-Wallberg syndrome may begenetically identical."6
Facioscapulohumeral muscular dystrophyA gene for facioscapulohumeral muscular dys-trophy (4q35) was first mapped in 1990 tochromosome 4 near the telomere." 7 Sub-sequently, altered sized fragments involving a
repeated sequence with homeodomain homol-ogy were identified in familial and sporadiccases of facioscapulohumeral muscular dystro-phy."18 119 The precise gene or genes affected bythe chromosomal rearrangements have not,however, been identified and thus the mecha-nism of pathogenesis remains a mystery. Inaddition, recombination with the altered sizedfragments has been documented'20 and not allfacioscapulohumeral muscular dystrophy fami-lies show linkage to 4q35. 121 Facioscapulo-humeral muscular dystrophy is thus still a
problematic disease for molecular diagnosis.
Oculopharyngeal muscular dystrophyA gene for oculopharyngeal muscular dystro-phy among French Canadians has been linkedto the proximal long arm of chromosome 14close to the genes for cardiac a-myosin and ,Bmyosin69 and in the same region as a gene fordominant distal myopathy.65
Emery-Dreifuss muscular dystrophyThe Emery-Dreifuss muscular dystrophy gene
has been identified and its protein productnamed emerin.'22 Emerin seems to be a trans-membrane protein but its function is uncer-
tain.
Distal myopathyTwo genes for distal muscular dystrophy havebeen localised. One (MPD1) with a phenotypesimilar to that originally described by Gowers65and the other for the recessive Miyoshi myopa-
thy.64 It is interesting that the MPD 1 gene
maps to a similar region of chromosome 14 as agene for oculopharyngeal muscular dystrophy69and that the Miyoshi myopathy gene is in asimilar region of chromosome 2 to a gene forautosomal recessive limb-girdle muscular dys-trophy (LGMD2B) 108 raising the possibilitythat the two conditions may be caused bymutations in the same gene.'23
Myotonic syndromesTable 5 gives a classification of these condi-tions, based on the underlying moleculardefects. Differentiation of the various types isusually possible on the basis of clinical featuressuch as the age of onset, pattern of inheri-tance, provocative factors for the myotonia,and the presence or absence of dystrophicmuscle weakness or other systemic features.
MYOTONIC DYSTROPHYThis is the most common of the genetic formsof myotonia and is transmitted as an autoso-mal dominant trait with considerable variabilityin the degree of phenotypic expression and ageof onset of symptoms. The congenital form, inwhich there is generalised hypotonia andweakness, often with facial diplegia and a dis-tinctive tent shaped mouth, may occur in theoffspring of either affected males or femalesbut the more severe cases are usually the off-spring of female heterozygotes who may them-selves be only very mildly affected.'24 125Mental retardation and delay in motor andspeech development are common in earlyonset cases. Myotonia is not present inaffected infants but is usually readily demon-strable in the tongue, hand, and forearm mus-
cles in patients presenting during adolescenceor early adult life, and tends to become pro-gressively less severe with the passage of time.Progressive weakness and atrophy of the fore-arm, calf, and sternomastoid muscles occur as
the condition progresses and in some casesweakness of the facial, bulbar, and respiratorymuscles also develops and may be associatedwith irregular breathing patterns, sleepapnoea, and respiratory failure.'26 Ventilatoryfunction studies as well as monitoring ofbreathing and arterial blood gases during sleepshould be performed if these problems are sus-
pected.Other distinctive features in the adult include
frontal baldness and testicular atrophy in menand distinctive subcapsular cataracts, which are
best seen with slit lamp examination.'25 Cardiacinvolvement also occurs and electrocardio-graphic abnormalities which include atrioven-tricular and intraventricular conduction defectsand atrial or ventricular arrhythmias, are com-
mon and may cause Stokes-Adams attacks or
even sudden death.'25 127 The incidence ofmitral valve prolapse is also increased in some
families.'28 Investigation of cardiac function,including ECG and echocardiography, shouldtherefore be performed routinely and, whenindicated, ECG monitoring and radionuclide
Table 5 Classification of hereditary myotonias
Myotonia Gene
Chloride channel myotonias:Autosomal dominant (Thomsen) CLCN1Autosomal recessive (Becker) CLCN1
Sodium channel myotonias:Paramyotonia congenita SCN4AMyotonia fluctuans SCN4AMyotonia permanens SCN4A
Dystrophic myotonias:Myotonic dystrophy Myotonin protein kinaseProximal myotonic myopathy ?
265
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
angiocardiography may also be indicated.Other systemic manifestations which mayrequire investigation in their own right includediabetes mellitus, disorders of the thyroid orimmune function, and gastrointestinal and gen-itourinary abnormalities.'25
Myotonic dystrophy is one of the easy mus-cle diseases to diagnose by molecular tech-niques, as virtually all cases have variations ofthe same mutation: the expansion of the CTGtriplet repeat in the myotonin protein kinasegene on chromosome 19.129-131 The large tripletrepeat expansions causing severe disease canbe identified by Southern blotting after diges-tion of genomic DNA with EcoRI, and smallerexpansions can be identified by digestion withBglI or BamHl.41 The PCR can identify nor-mal subjects by the presence of two alleleswithin the normal size range and the verysmall expansions in minimally affected orasymptomatic subjects (fig 3).131 132 Often, thisidentifies where the disease came from in afamily with someone other than the person thefamily has always suspected. Thus by cascadescreening it is possible to detect and warnthose family members at risk from possiblecardiac complications and sudden death.A dominantly inherited myotonic myopathy
with proximal muscle weakness and cataractswithout the characteristic trinucleotide repeatexpansion has recently been described'33 134and has been shown not to be allelic with thegenes for myotonic dystrophy or for the chlo-ride or sodium channelopathies.'33
CHLORIDE CHANNEL MYOTONIA
Wa. _It is now known that both the autosomal dom-inant (Thomsen) and recessive (Becker) formsof myotonia congenita are caused by muta-tions in the muscle chloride channel (CLCN1)
1 2 3 4 5 gene on chromosome 7.48 Symptoms may bepresent from birth in the dominant form but
Figure 3 Analysis of the often do not develop until early childhood ormyotonic dystrophy triplet adolescence. The myotonia is widespread,repeat expansion by PCR. usually painless, and more severe in the reces-
Lane 1: grandmothershowing two normal sized sive form beig accentuated by rest, cold, and
alleles; lane 2: emotion and improving with repeated muscleasymtomatic grandfather contraction. It is commonly associated withshowing one normal sized diffuse muscular hypertrophy, particularly inallele and a smallexpansion; lane 3: uncle of affected males. Muscle weakness may developproband (son) oflanes 1 after exercise, particularly in cases of the reces-and 2 showing non- sive form of the condition, and is associatedinheritance ofgrandfather's allele with a reduction in the amplitude of the
(expansion too bigfor evoked CMAP and twitch tension.'35 In addi-PCR); lane 4: mother of tion, some degree of fixed weakness and atro-
proband (daughter) oflanes 1 and 2 showing phy with EMG evidence of myopathy
non-inheritance of develops, particularly in the forearm and ster-grandfather's allele nomastoid muscles, in about two thirds of(expansion too bigfor . . . . .PCR); lane 5: proband patients with the recessive condition."6
(daughter of lane 4) To date, a total of 19 separate mutations inshowing non-inheritance of the CLCN1 gene have been identified, sixmother's allele, expansion being associated with dominant disease and 13
with the recessive disease.48 Most (four out offive) of the truncating mutations cause reces-
sive disease. The mutations are spreadthroughout the coding region of the gene andmany have been found in single families, indi-cating that other mutations are highly likely tobe found in other families. Myotonia con-
genita is therefore one of the difficult diseases
to diagnose, with molecular techniques requir-ing screening of the entire coding region of thegene.
SODIUM CHANNEL MYOTONIAThese varieties of myotonia have all beenlocalised to the same locus and have beenassociated with different mutations in the asubunit of the sodium muscle channel gene(SCN4A) on chromosome 17.48 137 In paramy-otonia congenita myotonia is characteristicallyinduced by cold exposure, particularly in thefacial and hand muscles, and may be associ-ated with attacks of weakness (cold paresis)which improve with warming. In most casesthe myotonia is increased by repeated musclecontraction (paradoxical myotonia) ratherthan improving as in most other myotonic dis-orders. In potassium sensitive paramyotonia(paralysis periodica paramyotonica) paradoxi-cal myotonia and episodes of weakness areprecipitated by potassium administration.Such cases account for the overlap betweenparamyotonia and hyperkalaemic periodicparalysis in some families.A third variety of sodium channel myotonia
has been designated myotonia fluctuans. Inthis condition, which is dominantly inherited,myotonia is of variable severity at differenttimes, may be associated with painful musclespasms, with a tendency to increase in severityafter exercise, ingestion of potassium, andadministration of depolarizing agents, and isresponsive to treatment with acetazolamide'37or, in some families, mexilitine.'38 A fourthvariety of sodium channel myotonia with con-tinuous severe myotonia, muscle stiffness, andhypertrophy has also been described and des-
48ignated myotonia permanens.The mutations in these conditions are
spread through a large part of the codingregion of the SCN4A gene making moleculardiagnosis difficult, although two mutations,Thri 31 3Met and Glyl 306Val, predominatein paramyotonia congenita and should be ini-tially screened for.
Periodic paralysisSome conditions may cause episodic weaknessor paralysis of the limb muscles (table 6). It isdifficult to evaluate the importance of a com-plaint of episodic weakness unless the patientis watched during an attack. Most patientswho complain of episodes of weakness are infact referring to fatigue. In those patients whodo have episodes of documented weakness it isfirst necessary to exclude disorders of neuro-muscular transmission such as myastheniagravis, demyelinating disorders of the periph-eral or central nervous system, transientischaemic episodes, or attacks of hystericalweakness. If these conditions can be excluded,the possibility of one of the primary periodicparalyses arises, particularly if there are otheraffected family members (table 6).
Differentiation between the main varietiesof primary periodic paralysis is usually possibleon the basis of the duration of the attacks ofweakness, provocative factors, and serum
*
266
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
Table 6 Classification ofperiodic paralyses
Hereditary:Hypokalaemic (DHP receptor; 1 q3 1-32)Potassium sensitive (SCN4A; 17q23-25)
HyperkalaemicParamyotonia congenitaParalysis periodica paramyotonicaAndersen's syndrome
Acquired:HypokalaemicHyperkalaemicThyrotoxic
potassium concentrations during attacks. Inhypokalaemic periodic paralysis the attacks are
often precipitated by carbohydrate ingestionand tend to be less frequent and of longerduration (up to 24 hours) than in the potas-sium sensitive periodic paralyses (for example,hyperkalaemic periodic paralysis) in which theattacks are often precipitated by fasting or byresting after exercise.'3 Although the serum
potassium concentration during an attack ofweakness may help to distinguish thehypokalaemic from the hyperkalaemic form,potassium concentrations are often normal inthe second and may occasionally also be nor-
mal in the hypokalaemic form.9 The serum
creatme kinase concentration is often raised in
severe attacks of both forms and may be some-
what raised even between attacks. Myotonia,when present clinically or evident on EMG, ismore suggestive of hyperkalaemic periodicparalysis or paramyotonia but may occasion-ally occur in the eyelid muscles inhypokalaemic periodic paralysis.9When carried out during an attack of weak-
ness EMG shows a progressive reduction inmotor unit recruitment and in the amplitudeof the compound muscle action potentialevoked by motor nerve stimulation, whereasrepetitive nerve stimulation shows a transientpotentiation of the compound muscle actionpotential.'39 A myopathic EMG pattern maybe found even during the attack free intervalparticularly in patients who develop fixed mus-cle weakness, as often occurs in those whohave had the condition for several years.Changes in the evoked compound muscleaction potential also occur with exercise andare the basis for the hand exercise testdescribed by McManis et al.'40 Serial measure-
ments of compound muscle action potentialamplitudes show a greater than normalincrease during exercise and decrease in thepost-exercise period in patients with periodicparalysis. The test was found to be abnormalin 70% of cases of periodic paralysis but didnot distinguish between the different forms.
Another form of exercise testing, which isuseful in detecting some cases of hypo-kalaemic periodic paralysis, including asymp-tomatic cases, is that described by Kantolaand Tarssanen,'4' which involves a 30 minuteperiod of bicycle ergometry. Affected personsdo not show the normal rise in plasma potas-sium concentrations after the exercise period.
Muscle biopsy shows a characteristic vacuo-lar change in muscle fibres, and sometimesnecrotic muscle fibres, particularly during an
attack of weakness, but sometimes even duringattack free intervals, in both major forms of
periodic paralysis. Vacuolar change may befound even in some family members withoutdefinite attacks of weakness.'4' Although thebiopsy changes are distinctive, a biopsy is sel-dom necessary as the results of provocativetests and molecular genetic analysis are usuallydiagnostic.As the plasma potassium concentrations
during an attack of weakness are sometimesmisleading, provocative tests remain impor-tant in evaluating people with a negative familyhistory or those from families in which themutation is not known. In hypokalaemic peri-odic paralysis, attacks of weakness may beinduced by giving an oral glucose load (1-5gm/kg over three minutes; maximum 100 g).9Muscle strength in selected groups, serumelectrolytes, and ECG should be monitoredevery 30 minutes for three to five hours. Ifweakness does not develop, an intravenousglucose load (3 g/kg in water) is given over aperiod of one hour. If weakness does notdevelop after 30 minutes, intravenous insulin(0 1 U/kg) is given and repeated at 60 minutesif weakness fails to develop. Regular measure-ments of muscle strength and of plasma elec-trolyte and glucose concentrations, and ECGshould be performed throughout the test andthe period of induced weakness.9 13
In the potassium sensitive forms of periodicparalysis attacks of weakness may be inducedby oral potassium loading.913 A widely usedprotocol involves giving 0 05 g/kg of potas-sium chloride in a glucose free solution over aperiod of three minutes. Muscle strength,serum electrolytes, and ECG are monitoredevery 15 minutes in the first two hours andevery 30 minutes in the next two hours andweakness usually develops after 90 to 180minutes. If the initial test is negative, higherpotassium loads of 0 1 to 0 15 g/kg may beused. The test is contraindicated in patientswith insulin dependent diabetes mellitus orrenal insufficiency. Cold testing, involvingimmersion of the arm in water at 10°C for 30minutes, may be useful in confirming the diag-nosis of paramyotonia in patients with a his-tory of episodes of cold induced weakness ormyotonia.9The molecular basis for both the
hypokalaemic and hyperkalaemic forms ofperiodic paralysis have now been defined.Hypokalaemic periodic paralysis has beenshown to be caused by three mutations in thedihydropyridine receptor calcium channelgene (CACNLIA3) on chromosome 1 q3 1-32affecting two amino acid residues.3848 142 143 Themutations can be detected by PCR followedby enzyme digestion as they either create ordestroy restriction enzyme sites'42 or bySSCP.38 Mutations in the gene encoding the asubunit of the skeletal muscle sodium channel(SCN4A) causing hyperkalaemic periodicparalysis were first described in 1991.144145 Arecent review by Lehmann-Horn and Riidel48catalogues the five mutations of SCN4A nowknown to be associated with hyperkalaemicperiodic paralysis. Two of the mutations,Thr7O4Met and Met1 592Val, predominateand can be screened for first. There is perhaps
267
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
a degree of genetic heterogeneity in hyper-kalaemic periodic paralysis as one family witha convincing clinical diagnosis of the diseasedid not map to the SCN4A gene.62 Mutationsin the same gene have also been found in somefamilies with paramyotonia congenita48 andin some cases of hyperkalaemic periodicparalysis associated with cardiac arrhythmias(Andersen's syndrome) 146 147
Congenital myopathiesThe congenital myopathies are a heteroge-neous group of disorders which may result inhypotonia in infancy or may present later inchildhood with weakness and delayed motormilestones (table 7). Some, such as centralcore disease, are benign and relatively non-progressive whereas others such as X linkedcentronuclear myopathy are usually fatal ininfancy. Skeletal abnormalities such as talipes,scoliosis, and hip dislocation as well as dys-morphic features are not uncommon. Ptosisand ophthalmoplegia are often a feature incentronuclear myopathy and may also occur inminicore disease. Respiratory insufficiencymay occur, particularly in nemaline myopathy,centronuclear myopathy, and cytoplasmicbody myopathy. The congenital myopathiesshould be considered in the differential diag-nosis of the floppy infant and need to be dis-tinguished from other neuromuscular andCNS disorders which may produce infantilehypotonia.
In all of these conditions a definitive diag-nosis relies on a muscle biopsy with fullhistochemical and electron microscopic exam-ination of muscle tissue. These will identifyspecific morphological changes such as centralcores, nemaline rods, central nucleation, andabnormalities of myofibre differentiation andfibre type proportions or distinctive inclusionbodies (for example, cytoplasmic bodies, fin-ger print bodies, spheroid bodies, hyaline bod-ies, reducing bodies, zebra bodies, and tubularaggregates). This will also exclude other con-ditions such as congenital muscular dystrophy,metabolic myopathies, and neurogenic disor-ders such as spinal muscular atrophy and con-genital peripheral neuropathies.9 148The genetic basis for some of the congenital
myopathies such as central core disease,nemaline myopathy, and the neonatal form ofcentronuclear myopathy have now beendefined. To date, one gene for autosomaldominant nemaline myopathy has been linked
Table 7 Congenital myopathies
Central core disease*Nemaline myopathyCentronuclear myopathyMinicore disease*Congenital fibre type disproportionMyopathies with cytoplasmic inclusions
Fingerprint body myopathyReducing body myopathyCytoplasmic body myopathyHyaline body myopathyMyopathy with tubular aggregatesZebra body myopathySarcotubular myopathy
*Predisposition to malignant hyperthermia.
to chromosome 1149 and a mutation in the a-tropomyosin gene TPM3 has been shown tosegregate with the disease.'50 A gene for reces-sive nemaline myopathy has been localised tochromosome 2.70 Neither of the loci map tothe known locations for the a-actinin genes.'51This and the mutation in tropomyosin mayindicate that nemaline myopathy is a diseaseof the thin filament rather than of the Z disc.'23Central core disease was first linked to thesame region of chromosome 19 as malignanthyperthermia'52 153 and then mutations associ-ated with central core disease were identifiedin the RYRi gene.'54-'56 Thus both malignanthyperthermia and central core disease arecaused by mutations in the RYRI gene andwhether central cores manifest or not maydepend on the degree of calcium loading ofthe individual muscle fibres.'55
Mitochondrial myopathiesSince the discovery of the first mitochondrialDNA mutations in 1988"157 58 it has becomeapparent that the clinical spectrum of mito-chondrial diseases is extremely diverse, rang-ing from relatively mild and slowly progressivemyopathies confined to the extraocular mus-cles (chronic progressive external ophthalmo-plegia) to severe fatal infantile myopathies (forexample, cytochrome c oxidase deficiency)and multisystem encephalomyopathies (suchas the Kearns-Sayre, MEIAS, and MERFFsyndromes9 159--162) (table 8). In addition, defi-ciencies of mitochondrial enzymes encoded bynuclear DNA have been identified (for exam-ple, succinate dehydrogenase deficiency).
CLINICAL PHENOTYPES AND GENOTYPESTable 9 shows that mitochondrial defects maybe associated not only with myopathic disor-ders but with a wide variety of other neurolog-ical and non-neurological manifestations.
Although some classic syndromes have beendefined (table 8), there is a certain amount ofoverlap between these and new phenotypiccombinations are still being identified.Moreover, there is considerable variability inthe age of onset, rate of progression, andextent of phenotypic expression in differenttissues even within the major syndromes. This
Table 8 Mitochondrial myopathies andencephalomyopathies
Progressive external ophthalmoplegiaSporadicFamilial
Kearns-Sayre syndromeOphthalmoplegiaPigmentary retinopathyCardiac conduction defectsCerebellar ataxiaSensorineural deafness
Limb-girdle myopathyInfantile myopathy
Benign reversibleSevere fatal
MERFF syndromeMyoclonusEpilepsyMyopathy
MELAS syndromeMyopathyLactic acidosisStroke-like episodes
268
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
Table 9 Clinical manifestations of mitochondrial disease
Neurological Non-neurological
External ophthalmoplegia Short statureLimb myopathy Cardiac conductionFatiguability and poor exercise defects
tolerance CardiomyopathyCerebellar ataxia Pigmentary retinopathyEpilepsy CataractsMyoclonus Lactic acidosisSensorineural deafiess Diabetes mellitusPeripheral neuropathy HypoparathyroidismDementia Renal tubular defectsStroke Episodic nausea andVascular headache vomitingDystonia PancytopeniaBasal ganglion calcification Intestinal pseudo-
obstructionMultiple lipomas
heterogeneity is characteristic of this group ofdisorders'63 and is attributable to the randomdistribution of mitochondria containing themutated DNA within different tissues and tothe admixture of normal and abnormal popula-tions of mitochondria within the cells of thesetissues (heteroplasmy) as a result of which dif-ferent tissues in the same patient and differentmembers of the same family may be involvedto different degrees.The classic syndromes have been associated
with different types of genomic defect. Forexample, patients with the pure form ofchronic progressive external ophthalmoplegia(CPEO) usually have single majordeletions'59 160 but point mutations have beenfound in some patients.2 Similarly, thosepatients with the Kearns-Sayre syndrome havesingle large mtDNA deletions which occur
sporadically.'57 164 In patients with familialCPEO two distinct syndromes have been iden-tified. In the first, which is maternally inher-ited, deletions are not found, whereas in thesecond, which is dominantly inherited, largescale multiple mtDNA deletions are usuallypresent and are thought to be secondary to amutation in a nuclear gene encoding a factorwhich controls mtDNA replication.'65 Such agene has recently been linked to chromosome1Oq23 3-24-3 in a Finnish family with autoso-mal dominant CPEO.50 Cases presentingpurely with a proximal myopathy may also bedominantly inherited'66 but are uncommonand the genotypic basis for these cases has notbeen defined. In the encephalomyopathy syn-dromes different point mutations have beenfound in tRNA-lys (nucleotides 8344 or 8356)in the MERRF syndrome'67 and tRNA-leu(nucleotides 3243, 3251, 3252, 3271 or 3291)in the MELAS syndrome.2160
DIAGNOSTIC APPROACHIn patients with CPEO, Kearns-Sayre syn-
drome, or one of the other classic syndromes,the clinical features are often sufficiently dis-tinctive to strongly suggest the diagnosis of amitochondrial disorder, and in familial cases, a
maternal pattern of transmission would alsoraise the possibility of such a diagnosis. Araised fasting venous lactate concentration isan additional diagnostic pointer. Lactate con-centrations are usually normal in cases ofCPEO, but venous and CSF concentrations
are often raised in the MELAS syndrome andmay also be raised in Kearns-Sayre syndromeand in patients with a proximal myopathy orencephalomyopathy.I59 A muscle biopsy is themost important diagnostic investigation, thecharacteristic findings being of ragged redfibres with the modified Gomori trichromestain, with abnormally prominent subsar-colemmal mitochondrial aggregates with theoxidative enzyme stains (NADH dehydroge-nase, succinate dehydrogenase) and abnormalmitochondrial morphology with mitochondrialinclusions on electron microscopy. In addi-tion, histochemical staining for cytochromeoxidase activity shows a characteristic mosaicpattern of fibres lacking enzyme activity inmost cases. Immunohistochemical techniquesmay be applied to determine whether nuclearor mtDNA encoded subunits of cytochromeoxidase are absent. In situ hybridisation withprobes to different parts of the mtDNA mole-cule may also be used to study the distributionof mutant mitochondria in muscle fibres.The identified common mutations in the
mitochondrial genome associated withMERRF or MELAS can be tested using PCRfollowed by enzyme digestion41 49 or SSCPanalysis. 168 The major deletions of the mtDNAassociated with Kearns-Sayre syndrome orCPEO may be identified either using Southernblotting80 or PCR'69 including long rangePCR, which can amplify the entire 16 569base pairs of the mtDNA in one reaction.'70The severity of the disease relates to the per-centage of mutant mitochondria,60 which canbe estimated either after Southern blotting, orenzyme digestion after PCR, or from SSCP.167Whether all the base changes shown to be
associated with mitochondrial related diseaseactually cause disease may be debatable; somemay merely be linked to other disease causingmutations.'7' On the other hand, the polymor-phisms of mtDNA may contribute to dis-ease. 172 The mitochondrial genome is thusproblematic for molecular diagnosis, the rele-vance of some mutations to disease beingunclear.
Acute rhabdomyolysis and myoglobinuriaVarious hereditary and acquired disorders maylead to episodes of severe widespread musclefibre destruction and myoglobinuria."Clinically, there is widespread muscle weak-ness which may be profound and in severecases there is often severe muscle pain, tender-ness, and depression of the deep tendonreflexes. When myoglobinuria is severe it maylead to the development of acute renal failure.In patients with malignant hyperthermia mus-cle rigidity, hyperpyrexia, and rhabdomyolysisusually develop during anaesthesia when sus-ceptible subjects are exposed to halothane andsome other inhalational anaesthetic agents,but episodes of rhabdomyolysis may also beprecipitated by stress, strenuous physicalactivity, or systemic infective illnesses.
Patients presenting in this way for the firsttime should undergo a detailed clinical assess-ment for a drug induced, toxic, or infective
269
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
cause and hypokalaemia, hypothyroidism, andother metabolic disorders should be excluded.Patients in whom no obvious cause can beidentified-especially those in whom there is ahistory of previous episodes-should have amuscle biopsy and appropriate biochemicalinvestigations for an underlying genetic disor-der such as malignant hyperpyrexia or a disor-der of glycolysis or fatty acid metabolism." 173
Susceptibility to malignant hyperthermia inhumans was first linked to the region contain-ing the ryanodine receptor calcium releasechannel on chromosome 1971 174 after themutation for swine malignant hyperthermiawas linked to the glucose phosphate isomerasegene which maps in humans to chromosome19. A few mutations have now been identifiedin the relatively large (15 kb) RYRI gene mes-sage'75 in a minority of families with malignanthyperthermia.74 The aim ofmolecular diagnosisin this condition must be to reduce thereliance on the extremely invasive current goldstandard of the muscle contracture test, withwhich the molecular diagnosis is not always inagreement.7274 However, until a clearer andmore comprehensive list of mutations in theRYR1 gene causing malignant hyperthermia isavailable, including resolution of the apparentgenetic heterogeneity, and the discrepanciesbetween molecular diagnosis and the contrac-ture test are resolved, molecular diagnosis forsusceptibility to malignant hyperthermia willremain problematical.
Painful muscle conditionsMuscle pain may be a feature of somemyopathies and other conditions (table 2).The pain may be focal or diffuse and mayoccur at rest, during, or after exercise. Whenmyalgia develops after an infective illness, analcoholic binge, exposure to a myotoxic drug,or after an episode of envenomation, the causeis usually apparent. A wide variety of drugsmay cause myalgia and muscle cramps withoutsignificant muscular weakness and the symp-toms usually resolve promptly after withdrawalof the offending agent (table 1). The finding ofsignificant muscular weakness, tenderness,and increase in serum creatine kinase suggests anecrotising myopathy and a muscle biopsy isusually warranted to confirm the diagnosis. Abiopsy is also indicated when an inflammatorymyopathy is suspected and should include theoverlying fascia, if there is a possibility of fasci-itis. Muscle pain and stiffness are commonsymptoms in hypothyroidism and in patientswith metabolic bone disease. The diagnosis insuch patients can usually be confirmed byappropriate biochemical and other studieswithout resorting to muscle biopsy.
Muscle pain and cramping which developduring exercise suggest a disorder of muscleenergy metabolism, such as deficiency ofmyophosphorylase, phosphofructokinase, orother glycolytic enzyme defect, or of carnitinepalmityl transferase, especially if there is a his-tory of discolouration of the urine after exer-cise, suggesting myoglobinuria. Such patientswarrant further investigation including the
forearm exercise test (see above) and assays ofcarnitine and carnitine palmityl transferaseactivity as well as a muscle biopsy for histo-chemical and biochemical studies to confirmthe diagnosis of these metabolic disorders.With molecular studies mutations causing dis-ease have been identified in some of these con-ditions but such studies are not usuallynecessary for the diagnosis. A muscle biopsy isalso necessary for the diagnosis of mitochon-drial myopathy, malignant hyperthermia, dys-trophin deficiency, and tubular aggregates,which may sometimes present with unex-plained myalgia, cramps, or exercise intoler-ance.The vast majority of patients with com-
plaints of muscle pain, stiffness, or crampingdo not have any significant muscular weaknessor other evidence of muscle disease. It isimportant in such patients to look for evidenceof muscular and myofascial tenderness. Thefinding of point tenderness in the typical sitesis diagnostic of the condition of fibromyalgiaand invasive investigations such as EMG andmuscle biopsy can usually be avoided.Similarly, a pattern of proximal or axial musclepain and stiffness with malaise in elderlypatients with preserved muscle strength and araised erythrocyte sedimentation rate is diag-nostic of polymyalgia rheumatica and warrantsa therapeutic trial ofprednisone without musclebiopsy, although the possibility of an underly-ing connective tissue or metabolic disorder ormalignancy should always be considered andinvestigated appropriately. In a third group ofpatients, with the postviral myalgia/fatiguesyndrome, there are no diagnostic clinical orlaboratory abnormalities. Muscle biopsy andEMG may, however, be indicated in suchpatients to exclude an inflammatory or meta-bolic myopathy, particularly when symptomsare disabling and if the serum creatine kinaseconcentration is raised.
Inflammatory myopathiesThe diagnosis of an inflammatory myopathymay be readily made on clinical grounds inpatients with the characteristic skin changes ofdermatomyositis or with the typical pattern ofmuscle weakness seen in inclusion bodymyositis and may also be suspected in patientswith a connective tissue disorder such as sys-temic lupus erythematosus, progressive sys-temic sclerosis, mixed connective tissuedisease, Sj6gren's syndrome, or other autoim-mune disease who develop a proximal myopa-thy and would be supported by the finding ofraised serum creatine kinase and an abnormalEMG (see above). However, it is importantthat the diagnosis should be firmly establishedon histological grounds and a muscle biopsyshould always be performed before commenc-ing treatment. An open biopsy, usually fromthe deltoid or vastus lateralis muscle, is prefer-able for the diagnosis of inflammatory myopa-thy. In addition to routine histologicalpreparations, mononuclear cell populations,immune complex deposition, MHC, andintercellular adhesion molecule expression can
1270
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
be assessed with immunohistochemical tech-niques.176 177
Other investigations are directed towardsidentifying any underlying immune or infec-tive disorder or malignancy. These shouldinclude an autoantibody screen for antinuclearfactor, rheumatoid factor, anti-RNP, and,when appropriate, other autoantibodies suchas PM-Scl and Ku, which are frequently asso-ciated with the polymyositis/sclerodermaoverlap syndrome, and antibodies to theaminoacyl-tRNA synthetases such as Jo-1which are found in patients with myositis andassociated interstitial lung disease and otheroverlap features.178 As patients with HIV andHTLV-1 infection may develop an inflamma-tory myopathy similar to polymyositis,'79 sero-logical testing for HIV and HTLV-1 infectionas well as studies of lymphocyte subsets arealso indicated, especially in areas where infec-tion with these agents is prevalent. The possi-bility of an underlying malignancy should beconsidered, particularly in adults presentingwith dermatomyositis but it is rare in patientswith juvenile dermatomyositis, connective tis-sue disease, or inclusion body myositis.'80 Thesearch for a malignancy should include adetailed clinical evaluation, including pelvicand rectal examination, routine haematologi-cal and biochemical studies, chest radiogra-phy, and mammography in females. Inaddition, in patients with dysphagia a bariumswallow or upper gastrointestinal endoscopyshould be performed to exclude carcinoma ofthe oesophagus or gastro-oesophageal junctionbefore attributing the dysphagia to the myositis.
Cardiac involvement, resulting in arrhyth-mias, heart block, or congestive cardiac failuremay sometimes occur even in patients withisolated polymyositis or dermatomyositis. 180
Electrocardiography, and when appropriateother investigations of cardiac function,should therefore be performed during theactive phase of the disease. In addition, assess-ment of respiratory function should be per-formed, especially in patients with severemuscle disease or suspected interstitial lungdisease.'80 181
Quantitative assessment of muscle strengthin representative upper and lower limb musclegroups using a myometer or isokineticdynamometer is important in assessing thepatient's response to treatment and makes itpossible to recognise an upward or downwardtrend in muscle performance even before thereis a change in the patient's functional state orMRC grading.'8' Serial measurements of theserum creatine kinase concentration are also ofvalue in assessing the response to treatmentand a rising creatine kinase concentration,even within the normal range, may be the firstindication of reactivation of the myositis in apatient who has previously been in remis-sion. 181 Measurements of serum concentra-tions of myoglobin and of soluble interleukin 2receptor concentrations in blood have beenreported to be sensitive indicators of diseaseactivity'2 182 but are not widely used.
We are grateful to Mrs S Moncrieff for secretarial assistance, to
Ms L Kelloway for fig1 and to Mr M Davis, Ms J Dench, andMs N Harber for figs 2 and 3..
1 Neuromuscular disorders: gene location. NeuromusculDisord 1995;6:I-III.
2 Mitochondrial encephalomyopathies: gene mutation.Neuromuscul Disord 1995;6:V-VI.
3 Argov Z, Mastaglia FL. Drug-induced neuromuscular dis-orders in man. In: WaltonJN, Karpati G, Hilton-JonesD, eds. Disorders of voluntary muscle. 6th ed. Edinburgh:ChurchillLivingstone, 1994:898-1029.
4 Lane RJM, Mastaglia FL. Drug-induced myopathies inman. Lancet 1978;ii:562-5.
5 Mastaglia FL. Toxic myopathies. In: Rowland LP,DiMauro S, eds. Handbook of clinical neurology.Amsterdam: Elsevier, 1992:595-622.
6 Suarez GA, Kelly JJ. The dropped head syndrome.Neurology 1992;42: 1625-7.
7 Garlepp MJ, Mastaglia FL. Inclusion body myositis. JNeurol Neurosurg Psychiatry 1996;60:251-5.
8 Harvey JM, Mastaglia FL, Zilko PJ, Ojeda VJ, Cheah PS.Scleromyxedema and inflammatory myopathy: a clinico-pathological study of three patients. Aust NZ J Med1986;16:329-35.
9 Griggs RC, MendellJR, Miller RG. Evaluation and treat-ment of myopathies. Contemporary neurology series.Philadelphia: FA Davis, 1995.
10 Sunohara N, Takagi A, Nonaka I, Sugita H, Satoyoshi E.Idiopathic hyperCKemia. Neurology 1984;34:544-7.
11 Tien I, DiMauro S, Rowland LP. Myoglobinuria. In:Rowland LP, DiMauroS, eds. Handbook of clinical neu-rology. Amsterdam: Elsevier, 1992:553-93.
12 Kagen U. Myoglobinaemia in inflammatory myopathies.J7AMA 1977;237:1448-52.
13 Moxley RT. Metabolic and endocrine myopathies. In:Walton JN, Karpati G, Hilton-Jones D, eds. Disorders ofvoluntary muscle. 6th ed. Edinburgh: ChurchillLivingstone, 1994:647-716.
14 Argov Z, Bank WJ. Phosphorus magnetic resonance spec-troscopy (3'PMRS) in neuromuscular disorders. AnnNeurol 1991;30:90-7.
15 Moussavi RS, Carson PJ, Boska MD, Weiner MW, MillerRG. Nonmetabolic fatigue in exercising human muscle.Neurology 1989;39: 1222-6.
16 McKeran RO, Hallidan D, Purkiss P, Royston P. 3-methylhistidine excretion as an index of myofibrillarprotein catabolism in neuromuscular disease. J NeurolNeurosurg Psychiatry 1979;42:536-4 1.
17 Ohkoshi N, Yoshizawa T, Mizusawa H, et al. Malignanthyperthermia in a patient with Becker muscular dystro-phy: dystrophin analysis and caffeine contracture study.Neuromusc Disord 1995;5:53-8.
18 Fawcett PRW, Barwick DD. The clinical neurophysiologyof neuromuscular disease. In: Walton JN, Karpati G,Hilton-Jones D, eds. Disorders of voluntary muscle. 6thed. Edinburgh: Churchill Livingstone, 1994:1033-104.
19 Eisen A, Berry K, Gibson G. Inclusion body myositis:myopathy or neuropathy? Neurology 1983;33: 1109-14.
20 Grindrod S, Tofts P, Edwards R. Investigation of humanskeletal muscle structure and composition by X-raycomputerised tomography. Eur J Clin Invest 1983;13:465-8.
21 Kiers L. Diabetic muscle infarction: magnetic resonanceimaging (MRI) avoids the need for biopsy. Muscle Nerve1995;18:129-30.
22 De Visser M, Verbeeten B. Computed tomography of theskeletal musculature in Becker-type muscular dystrophyand benign infantile spinal muscular atrophy. MuscleNerve 1985;8:435-44.
23 Pamphlett R. Muscle biopsy. In: Mastaglia FL, WaltonJN, eds. Skeletal muscle pathology. 2nd ed. Edinburgh:Churchill Livingstone, 1992:95-121.
24 Bonnemann CG, Modi R, Noguchi S, et al. -sarcoglycan(A3b) mutations cause autosomal recessive musculardystrophy with loss of sarcoglycan complex. NatureGenet 1995;11:266-73.
25 Beggs AH, Kunkel LM. Improved diagnosis ofDuchenne/Becker muscular dystrophy. 7 Clin Invest1990;85:613-9.
26 Hoffman EP, Fischbeck KH, Brown RH, et al.Characterization of dystropin in muscle-biopsy speci-mens from patients with Duchenne's or Becker'smuscular dystrophy. N Englj7Med 1988;318: 1363-8.
27 Hoffman EP, Kunkel LM, Angelini C, Clarke A, JohnsonM, Harris JB. Improved diagnosis of Becker musculardystrophy by dystrophin testing. Neurology 1989;39:1011-7.
28 Piccolo F, Roberds SL, Jeanpierre M, et al. Primaryadhalinopathy: a common cause of autosomal recessivemuscular dystrophy of variable severity. Nature Genet1995;10:243-5.
29 Malhotra SB, Hart KA, Klamut HJ, et al. Frame-shiftdeletions in-patients with Duchenne -and Becker muscu-lar dystrophy. Science 1988;242:755-9.
30 Chelly J, Gilgenkrantz H, Lambert M, et al. Effect of dys-trophin gene deletions on mRNA levels and processingin Duchenne and Becker muscular dystrophies. Cell1990;63: 1239-48.
31 Morisaki H, Morisaki T, Newby LK, Holmes EW.Alternative splicing: a mechanism for phenotypic rescueof a common inherited defect. J Clin Invest 1993;91:2275-80.
32 Collins FS. Positional cloning moves from perditional totraditional. Nature Genet 1995;9:347-50.
33 Noguchi S, McNally EM, Othmane KB, et al. Mutations in
271
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
the dystrophin-associated protein '-sarcoglycan in chro-mosome 13 muscular dystrophy. Science 1995;270:819-22.
34 Lim LE, Duclos F, Broux 0, et al. ,-sarcoglycan: charac-terization and role in limb-girdle muscular dystrophylinked to 4q12. Nature Genet 1995;11:257-65.
35 Evans MI, Greb A, Kunkel LM, et al. In utero fetal musclebiopsy for the diagnosis of Duchenne muscular dystro-phy. AmJ Obstet Gynecol 199 1;165:728-32.
36 Bradley DM, Parsons EP, Clarke AJ. Experience withscreening newborns for Duchenne muscular dystrophyin Wales. BMJ 1993;306:357-60.
37 Greenberg CR, Jacobs HK, Halliday W, Wrogmann K.Three year's experience with neonatal screening forDuchenne/Becker muscular dystrophy: gene analysis,gene expression and phenotype prediction. Am Y MedGenet 1991;39:68-75.
38 Ptacek LJ, Tawil R, Griggs RC, et al. Dihydropyridinereceptor mutations cause hypokalaemic periodic paraly-sis. Cell 1994;77:863-8.
39 Mullis KB, Faloona FA. Specific synthesis of DNA invitro via a polymerase-catalysed chain reaction. MethEnzymol 1987;155:335-50.
40 Roberts RG, Bentley DR, Barby TFM, et al. Direct diag-nosis of carriers of Duchenne and Becker muscular dys-trophy by amplification of lymphocyte RNA. Lancet1990; 336:1523-6.
41 Zeviani M, Amati P, Bresolin N, et al. Rapid detection ofthe A-G mutation of mtDNA in Italian families withmyoclonus epilepsy and ragged red fibers. Am Y HunGenet 199 1;48:203-1 1.
42 Shelbourne P, Winquist R, Kunert E, et al. UnstableDNA may be responsible for the incomplete penetranceof the myotonic dystrophy phenotype. Human MolecularGenetics 1992;1:467-73.
43 Abbs S, Yau SC, Clark S, Mathew CG, Bobrow M. Aconvenient multiplex PCR system for the detection ofdystrophin gene deletions: a comparative analysis withcDNA hybridisation shows mistypings by both methods.JfMed Genet 199 1;28:304-1 1.
44 Chamberlain JS, Gibbs RA, Ranier JE, Nguyen PN,Caskey CT. Deletion screening of the Duchenne mus-cular dystrophy locus via multiplex DNA amplification.Nucleic Acids Res 1988;16:1 1141-56.
45 Chamberlain JS, Gibbs RA, Ranier JE, Caskey CT.Multiplex PCR for the diagnosis of Duchenne musculardystrophy. In Innis M, Gelfland D, Sninsky J, White T,eds. PCR protocols: a guide to methods and applications.San Diego: Academic Press, 1990:272-81.
46 Lefebvre S, Burglen L, Reboullet S, et al. Identificationand characterization of a spinal muscular atrophy-deter-mining gene. Cell 1995;80:155-65.
47 Rodrigues NR, Owen N, Talbot K, Ignatius J, Dubowitz V,Davies KE. Deletions in the survival motor neuron geneon 5q 13 in autosomal recessive spinal muscular atrophy.Human Molecular Genetics 1995;4:631-4.
48 Lehmann-Horn F, Rudel R. Hereditary nondystrophicmyotonias and periodic paralyses. Curr Opin NeurolNeurosurg 1995;8:402-10.
49 Wallace DC: Mitochondrial DNA mutations and neuro-muscular disease. TIGS 1989;5:9-13.
50 Suomalainen A, Kaukonen J, Amati P, et al. An autosomallocus predisposing to deletions of mitochondrial DNA.Nature Genet 1995;5:146-51.
51 Forrest S, Cotton R, Landegren U, Southern E. How tofind all those mutations. Nature Genet 1995;10:375-6.
52 Grompe M. The rapid detection of unknown mutations innucleic acids. Nature Genet 1993;5:111-7.
53 Liu Q, Sommer SS. Restriction endonuclease fingerprint-ing (REF): a sensitive method for screening for muta-tions in long, contiguous segments of DNA.Biotechniques 1995;18:470-7.
54 Sarkar G, Yoon H-S, Sommer SS. Dideoxy fingerprinting(ddf): a rapid and efficient screen for the presence ofmutations. Genomics 1992,13:441-3.
55 Mashal RD, Koontz J, Sklar J. Detection of mutations bycleavage of DNA heteroduplexes with bacteriophageresolvases. Nature Getnet 1995;9:177-83.
56 Youil R, Kemper BW, Cotton RGH. Screening for muta-tions by enzyme mismatch cleavage with T4 endonucle-ase VII. Proc Natl Acad Sci USA 1995;92:87-91.
57 Wilton SD, Johnsen RD, Pedretti JR, Laing NG. Two dis-tinct mutations in a single dystrophin gene: identifica-tion of an altered splice-site as the primary Beckermuscular dystrophy mutation. Am .7 Med Genet1993;46:563-9.
58 Wilton SD, Chandler DC, Kakulas BA, Laing NG:Identification of a point mutation and germinalmosaicism in a Duchenne muscular dystrophy family.Human Mutation 1994;3:133-40.
59 Chelly J, Gilgenkrantz H, Hugnot JP, et al. Illegitimatetranscription: application to the analysis of truncatedtranscripts of the dystrophin gene in nonmuscle culturedcells from Duchenne and Becker patients. .7 Clin Invest1991;88:1161-6.
60 Wallace DC: Mitochondrial diseases: genotype versusphenotype. TIGS 1993;9:128-33.
61 Prior TW, Papp AC, Snyder PJ, et al. A missense muta-tion in the dystrophin gene in a Duchenne musculardystrophy patient. Nature Genet 1993;4:357-60.
62 Wang J, Zhou J, Todorovic SM, et al. Molecular geneticand genetic correlations in sodium channelopathies: lackof founder effect and evidence for a second gene. Am 7Hum Genet 1993;52:1074-84.
63 Ohno K, Hutchinson DO, Milone M, et al. Congenitalmyasthenic syndrome caused by prolonged acetyl-choline receptor channel openings due to a mutation inthe M2 domain of the E subunit. Proc NatlAcad Sci USA1995;92:758-62.
64 Bejaoui K, Hirabayashi K, Hentati F, et al. Linkage ofMiyoshi myopathy (distal autosomal recessive musculardystrophy) locus to chromosome 2p12-14. Neurology1995;45:768-72.
65 Laing NG, Laing BA, Meredith C, et al. Autosomal dom-inant distal myopathy: linkage to chromosome 14. An.7Hum Genet 1995;56:422-7.
66 Speer MC, Yamaoka LH, Gilchrist JH, et al.Confirmation of genetic heterogeneity in limb-girdlemuscular dystrophy: linkage of an autosomal dominantform to chromosome 5q. Am _7 Hum Genet 1992;50:1211-7.
67 Yamaoka LH, Westbrook CA, Speer MC, et al. Develop-ment of a microsatellite genetic map spanning 5q31-33and subsequent placement of the LGMD1A locusbetween D5S 178 and IL9. Neuromuscul Disord 1994;4:471-5.
68 Janssen EAM, Hensels GW, van Oost BA, et al. The genefor X-linked myotubular myopathy is located in an 8Mb region at the border of Xq27 3 and Xq28.Neuromuscul Disord 1994;4:455-6 1.
69 Brais B, Xie Y-G, Sanson M, et al. The oculopharyngealmuscular dystrophy locus maps to the region of the car-diac a and ,B myosin heavy chain genes on chromosome14ql 1 2-q1 3. Human Molecular Geneticsl 995;4:429-34.
70 Wallgren-Pettersson C, Avela K, Marchand S, et al. Agene for autosomal recessive nemaline myopathyassigned to chromosome 2q by linkage analysis.Neuromuscul Disord 1995;5:441-3.
71 McCarthy TV, Healy JMS, Heffron JJA, et al.Localization of malignant hyperthermia susceptibilitylocus to human chromosome 19ql2-13 2. Nature 1990;343:562-4.
72 Deufel T, Golla A, Iles D, et al. Evidence for genetic het-erogeneity of malignant hyperthermia susceptibility. Am7 Hum Genet 1992;50:1151-61.
73 Levitt RC, Nouri N, Jedlicka AE, et al. Evidence forgenetic heterogeneity in malignant hyperthermia suscep-tibility. Genomics 1991,11:543-7.
74 MacLennan DH. Discordance between phenotype andgenotype in malignant hyperthermia. Curr Opin NeurolNeurosurg 1995;8:397-401.
75 Powell SM, Petersen GM, Krush AJ, et al. Moleculardiagnosis of familial adenomatous polyposis. N Engl .7Med 1993;329:1982-7.
76 Roest PAM, Roberts RG, Sugino S, van Ommen G-JB,den Dunnen JT. Protein truncation test (PTT) for rapiddetection of translation-terminating mutations. HumanMolecular Genetics 1993;2: 1719-21.
77 Heim RA, Silverman LM, Kam-Morgan LNW, LuceMC. Screening for truncated NFI proteins. NatureGenet 1994;8:318-9.
78 Heim RA, Kam-Morgan LNW, Binnie CG, et al.Distribution of 13 truncating mutations in the neurofi-bromatosis 1 gene. Human Molecular Genetics 1995;4:975-81.
79 Campbell KP. Adhalin gene mutations and autosomalrecessive limb-girdle muscular dystrophy. Ann Neurol1995;38:353-4.
80 Byrne E. Mitochondrial DNA abnormalities in humandisease. Med 7Aust 1991;154:646-7.
81 Kakulas BA. The spectrum of dystrophinopathies. In:Lane RJM, ed. Handbook of muscle disease. New York:Marcell Dekker 1996 (in press).
82 Van Ommen GJB, Scheuerbrandt G. Neonatal screeningfor muscular dystrophy. Consensus recommendation ofthe 14th workshop sponsored by the European Neuro-muscular Center (ENMC). Neuromuscul Disord 1993;3:231-9.
83 Muntoni F, Mateddu A, Cianchetti C, et al. Dystrophinanalysis using a panel of anti-dystrophin antibodies inDuchenne and Becker muscular dystrophy. _7 NeurolNeurosurg Psychiatry 1993;56:26-3 1.
84 Koenig M, Hoffman EP, Bertelson CJ, Monaco AP,Feener C, Kunkel LM. Complete cloning of theDuchenne muscular dystrophy (DMD) cDNA andpreliminary genomic organization of the DMD genein normal and affected individuals. Cell 1987;50:509-17.
85 den Dunnen J, Bakker E, Klein-Breteler E, Pearson P, vanOmmen G. Direct detection of more than 50% of theDuchenne muscular dystrophy mutations by field inver-sion gels. Nature 1987;329:640-2.
86 Laing NG, Mears ME, Thomas HE, et al. Differentiationof Becker muscular dystrophy from limb-girdle muscu-lar dystrophy and Kugelberg-Welander disease using acDNA probe. Med 7Aust 1990;152:270-1.
87 Lunt PW, Cumming WJK, Kingston H, et al. DNAprobes in differential diagnosis of Becker muscular dys-trophy and spinal muscular atrophy. Lancet 1 989;i:46-7.
88 Norman A, Thomas N, Coakley J, Harper P. Distinction ofBecker from limb-girdle muscular dystrophy by meansof dystrophin cDNA probes. Lancet 1989;i:466-8.
89 Weber JL, May PE. Abundant class of human DNA poly-morphisms which can be typed by the polymerase chainreaction. Am _J Hum Genet 1989;44:388-96.
90 Hejtmancik J, Harris S, Tsao C, Ward P, Caskey C.Carrier diagnosis of Duchenne muscular dystrophy
272
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Investigation of muscle disease
using restriction fragment length polymorphisms.Neurology 1986;36: 1553-62.
91 Laing NG, Siddique T, Bartlett RJ, et al. Duchenne mus-cular dystrophy: detection of deletion carriers by spec-trophotometric densitometry. Clin Genet 1989;35:393-8.
92 Mao Y, Cremer M. Detection of Duchenne muscular dys-trophy carriers by dosage analysis using the DMDcDNA clone 8. Hum Genet 1989;81:193-5.
93 Bartlett RJ, Pericak-Vance MA, Lanman JT, et al.Prenatal detection of an inherited Duchenne musculardystrophy deletion allele. Neurology 1987;37:355-6.
94 Abbs S, Bobrow M. Analysis of quantitative PCR for thediagnosis of deletion and duplication carriers in the dys-trophin gene. JfMed Genet 1992;29:191-6.
95 Ioannou P, Christopoulos G, Panayides K, KleanthousM, Middleton L. Detection of Duchenne and Beckermuscular dystrophy carriers by quantitative multiplexpolymerase chain reaction analysis. Neurology 1992;42:1783-90.
96 Beggs AH, Hoffman EP, Snyder JR, et al. Exploring themolecular basis for variability among patients withBecker muscular dystrophy: dystrophin gene and pro-tein studies. Am JfHum Genet 1991;49:54-7.
97 Sunohara N, Arahata K, Hoffman EP, et al. Quadricepsmyopathy: forme fruste of Becker muscular dystrophy.Ann Neurol 1990;28:634-9.
98 Gospe SM, Lazaro RP, Lava NS, Grootscholten BS,Scott MO, Fischbeck KH. Familial X-linked myalgiaand cramps: a non-progressive myopathy associatedwith a deletion in the dystrophin gene. Neurology1989;39: 1277-80.
99 Malapert D, Recan D, Leturcq F, Degos JD, GherardiRK. Sporadic lower limb hypertrophy and exerciseinduced myalgia in a woman with dystrophin gene dele-tion. J Neurol Neurosurg Psychiatry 1995;59:552-4.
100 Servidei S, Manfredi G, Mirabella M, et al. FamilialhyperCKemia can be a variant of Becker muscular dys-trophy. Neurology 1993;43:A293.
101 Piccolo G, Azan G, Tonin P, et al. Dilated cardiomyopathyrequiring cardiac transplantation as initial manifestationof Xp21 Becker type muscular dystrophy. NeuromusculDisord 1994;4: 143-6.
102 Yoshida K, Ikeda S-I, Nakamura A, et al. Molecularanalysis of the Duchenne muscular dystrophy gene inpatients with Becker muscular dystrophy presentingwith dilated cardiomyopathy. Muscle Nerve1993;16:1161-6.
103 Beckmann JS, Richard I, Hillaire D, et al. A gene for limb-girdle muscular dystrophy maps to chromosome 15 bylinkage. CR Acad Sci (Paris) 1991;312:141-8.
104 Fougerousse F, Broux 0, Richard I, et al. Mapping of achromosome 15 region involved in limb girdle musculardystrophy. Human Molecular Genetics 1994;3:285-93.
105 Richard I, Broux 0, Allamand V, et al. Mutations in theproteolytic enzyme calpain 3 cause limb-girdle musculardystrophy type 2A. Cell 1995;81:27-40.
106 Matsumura K, Nonaka I, Campbell KP. Abnormalexpression of dystrophin-associated proteins inFukuyama-type congenital muscular dystrophy. Lancet1993;341:521-2.
107 Tome FMS, Evangelista T, Leclerc A, et al. Congenitalmuscular dystrophy with merosin deficiency. C R AcadSci (Paris) 1994;317:351-7.
108 Bashir R, Strachan T, Keers S, et al. A gene for autosomalrecessive limb-girdle muscular dystrophy, maps to chro-mosome 2p. Human Molecular Genetics 1994;3:455-7.
109 Speer MC, Yamaoka LH, Gilchrist JM, et al. Evidence forgenetic heterogeneity in the dominant form of limb-girdlemuscular dystrophy. Am YHum Genet 1993;53:A1082.
110 Matsumura K, Tome FMS, Collin H, et al. Deficiency ofthe 50K dystrophin-associated glycoprotein in severechildhood autosomal recessive muscular dystrophy.Nature 1992;359:320-2.
111 Ljunggren A, Duggan D, McNally E, et al. Primaryadhalin deficiency as a cause of muscular dystrophy inpatients with normal dystrophin. Ann Neurol 1995;38:367-72.
112 Roberds SL, Leturq F, Allamand V, et al. Missense muta-tions in the adhalin gene linked to autosomal recessivemuscular dystrophy. Cell 1994;78:625-33.
113 Arahata K, Ishii H, Hayashi YK. Congenital musculardystrophies. Curr Opin Neurol Neurosurg 1995;8:385-90.
114 Helbling-Leclerc A, Zhang X, Topaloglu H, et al.Mutations in the laminin a2-chain gene (LAMA2) causemerosin-deficient congenital muscular dystrophy.Nature Genet 1995;11:216-8.
115 Toda T, Segawa M, Nomura Y, et al. Localization of agene for Fukuyama type congenital muscular dystrophyto chromosome 9q31-33. Nature Genet 1993;5:283-6.
116 Toda T, Yoshioka M, Nakahori Y, et al. Genetic identity ofFukuyama-type congenital muscular dystrophy andWalker-Warburg syndrome. Ann Neurol 1995;37:99-101.
117 Wijmenga C, Frants RR, Brouwer OF, Moerer P, WeberJL, Padberg GW. Localisation of facioscapulohumeralmuscular dystrophy gene on chromosome 4. Lancet1 990;336:65 1-3.
118 Wijmenga C, Brouwer OF, Padberg GW, Frants RR.Transmission of de novo mutation associated withfacioscapulohumeral muscular dystrophy. Lancet 1992;340:985-6.
119 Wijmenga C, Hewitt JE, Sandkuijl LA, et al.Chromosome 4q DNA rearrangements associated with
facioscapulohumeral muscular dystrophy. Nature Genet1992;2:26-30.
120 Weiffenbach B, Dubois J, Storvick D, et al. Mapping thefacioscapulohumeral muscular dystrophy gene is com-plicated by chromosome 4q35 recombination events.Nature Genet 1993;4:165-9.
121 Gilbert JR, Stajich JM, Wall S, et al. Evidence for hetero-geneity in facioscapulohumeral muscular dystrophy(FSHD). Am J Hum Genet 1993;53:401-8.
122 Bione S, Maestrini E, Rivella S, et al. Identification of anovel X-linked gene responsible for Emery-Dreifussmuscular dystrophy. Nature Genet 1994;8:323-7.
123 Laing NG. Inherited disorders of contractile proteins inskeletal and cardiac muscle. Curr Opin Neurol Neurosurg1995;8:391-6.
124 Hageman ATM, Gabreels, Liem KD, Renkawek K, BoonJM. Congenital myotonic dystrophy; a report on thir-teen cases and a review of the literature. Jf Neurol Sci1993;115:95-101.
125 Harper PS. Myotonic dystrophy. Major problems in neurol-ogy. Vol 9. Philadelphia: WB Saunders, 1979.
126 Serisier DE, Mastaglia FL, Gibson GJ. Respiratory mus-cle function and ventilatory control I in patients withmotor neurone disease, II in patients with myotonic dys-trophy. QJ7Med 1982;202:205-26.
127 Viitasalo MT, Kala R, Karli P, Eisalo A. Ambulatoryelectro-cardiographic recording in mild or moderatemyotonic dystrophy and myotonia congenita(Thomsen's disease). JfNeurol Sci 1983;62: 181-90.
128 Winters SJ, Schreiner B, Griggs RC, Rowley P, NandaNC. Familial mitral valve prolapse and myotonic dystro-phy. Ann Intern Med 1976;85:19-22.
129 Buxton J, Shelbourne P, Davies J, et al. Detection of anunstable fragment of DNA specific to individuals withmyotonic dystrophy. Nature 1992;355:547-8.
130 Fu Y-H, Pizzuti A, Fenwick Jr RG, et al. An unstabletriplet repeat in a gene related to myotonic musculardystrophy. Science 1992;255:1256-8.
131 Mahadevan M, Tsilfidis C, Sabourin L, et al. Myotonicdystrophy mutation: an unstable CTG repeat in the 3'untranslated region of the gene. Science 1992;255:1253-5.
132 Reardon W, Harley HG, Brook JD, et al. Minimal expres-sion of myotonic dystrophy: a clinical and molecularanalysis. J Med Genet 1992;29:770-3.
133 Ricker K, Koch MC, Lehmann-Hom F, et al. Proximalmyotonic myopathy. Neurology 1994;44:1448-52.
134 Thornton CA, Griggs RC, Moxley RT. Myotonic dystro-phy with no trinucleotide repeat expansion. Ann Neurol1994;35:269-72.
135 Sun SF, Streib EW. Autosomal recessive generalisedmyotonia. Muscle Nerve 1983;6: 143-7.
136 Becker PE. Syndromes associated with myotonia: clinical-genetic classification. In: Rowland LP, ed. Pathogenesisof human muscular dystrophies. Amsterdam: ExcerptaMedica 1977:699-705.
137 Hudson AJ, Ebers GC, Bulman DE. Brain 1995;118:547-63.
138 Ricker K, Moxley RT, Heine R, Lehmann-Hom F.Myotonia fluctuans. A third type of muscle sodiumchannel disease. Arch Neurol 1994;51:1095-102.
139 Campa JA, Sanders DB. Familial hypokalaemic periodicparalysis. Arch Neurol 1974;31:110-5.
140 McManis PG, Lambert EH, Daube JR. The exercise test inperiodic paralysis. Muscle Nerve 1986;9:704-10.
141 Kantola IM, Tarssanen LT. Diagnosis of familialhypokalemic periodic paralysis: role of the potassiumexercise test. Neurology 1992;42:2158-61.
142 Elbaz A, Vale-Santos J, Jurkat-Rott K, et al. Hypo-kalaemic periodic paralysis and the dihydropyridinereceptor (CACNL1A3): genotype/phenotype correla-tions for two predominant mutations and evidence forthe absence of a founder effect in 16 Caucasian families.AmJHum Genet 1995;56:374-80.
143 Jurkat-Rott K, Lehmann-Hom F, Elbaz A, et al. A cal-cium channel mutation causing hypokalaemic periodicparalysis. Human Molecular Genetics 1994;3: 1415-9.
144 Ptacek U, Trimmer JS, Agnew WS, Roberts JW, PetajanJH, Leppert M. Paramyotonia congenita andhyperkalaemic periodic paralysis map to the samesodium channel gene locus. Am JfHum Genet 1991;49:851-4.
145 Rojas CV, Wang J, Schwarts LS, Hoffman EP, PowellBR, Brown RHJ. A MET to VAL mutation in the skele-tal muscle Na+ channel a- subunit in hyperkalaemicperiodic paralysis. Nature 1991;354:387-9.
146 Baquero JL, Ayala RA, Wang J, et al. Hyperkalemic peri-odic paralysis with cardiac dysrhythmia: a novel sodiumchannel mutation? Ann Neurol 1995;37:408-1 1.
147 Tawil R, Ptacek U, Pavlakis SG, et al. Andersen's syn-drome: potassium-sensitive periodic paralysis, ventricu-lar ectopy, and dysmorphic features. Ann Neurol1994;35:326-30.
148 Fardeau M. Congenital myopathies. In: Mastaglia FL,Walton JN, eds. Skeletal muscle pathology. 2nd ed.Edinburgh: Churchill-Livingstone, 1992:237-81.
149 Laing NG, Majda BT, Akkari PA, et al. Assignment of agene (NEMI) for autosomal dominant nemalinemyopathy to chromosome 1. Am J Hum Genet 1992;50:576-83.
150 Laing NG, Wilton SD, Akkari PA, et al. A mutation in thea-tropomyosin gene TPM3 associated with autosomaldominant nemaline myopathy. Nature Genet 1995;9:75-9.
273
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from

Mastaglia, Laing
151 Beggs AH, Byers TJ, Knoll JHM, Boyce FM, Bruns GAP,Kunkel L. Cloning and characterization of two humanskeletal muscle alpha-actinin genes on chromosome oneand eleven. J Biol Chem 1992;267:9281-8.
152 Haan EA, Freemantle CJ, McCure JA, Friend KL,Mulley JC. Assignment of the gene for central core dis-ease to chromosome 19. Hum Genet 1990;86:187-90.
153 Kausch K, Lehmann-Horn F, Janka M, Wieringa B,Grimm T, Muller CR. Evidence for linkage of the centralcore disease locus to the proximal long arm of humanchromosome 19. Genomics 1991;10:765-9.
154 Quane KA, Healy JMS, Keating KE, et al. Mutations inthe ryanodine receptor gene in central core disease andmalignant hyperthermia. Nature Genet 1983;5:51-5.
155 Quane KA, Keating KE, Healy JMS, et al. Mutationscreening of the RYR1 gene in malignant hyperthermia:detection of a novel tyr-ser mutation in a pedigree withassociated central cores. Genomics 1994;23:236-9.
156 Zhang Y, Chen HS, Khanna VK, et al. A mutation in thehuman ryanodine receptor gene associated with centralcore disease. Nature Genet 1993;5:46-50.
157 Holt IJ, Harding AE, Morgan-Hughes JA. Deletions ofmuscle mitochondrial DNA in patients with mitochon-drial myopathies. Nature 1988;331 :717-9.
158 Wallace DC, Singh G, Lott MT, et al. MitochondrialDNA mutations associated with Leber's hereditary opticneuropathy. Science 1988;242:1427-30.
159 Jackson MJ, Schaefer JA, Johnson MA, Morris AAM,Tumbull DM, Bindoff LA. Presentation and clinicalinvestigation of mitochondrial respiratory chain disease.Brain 1995;118:339-57.
160 Johns DR. Mitochondrial DNA and disease. New Engl JMed 1995;333:638-44.
161 Morgan-Hughes JA. Mitochondrial diseases. In:Mastaglia FL, Walton JN, eds. Skeletal muscle pathology.2nd ed. Edinburgh: Churchill-Livingstone, 1992:367-424.
162 DiMauro S, Moraes CT. Mitochondrial encephalomy-opathies. Arch Neurol 1993;50:1197-208.
163 Mechler F, Johnson MA, Mastaglia FL, et al.Mitochondrial myopathies. A clinico-pathological studyof cases with and without extra-ocular muscle involve-ment. Aust NZJrMed 1986;16:185-92.
164 Zeviani M, Moraes CT, DiMauro S, et al. Deletions ofmitochondrial DNA in Keams-Sayre syndrome.Neurology 1988;38: 1339-46.
165 Zeviani M, Servidei S, Gellera C, Bertini E, DiMauro S,DiDonato S. An autosomal dominant disorder with mul-tiple deletions of mitochondrial DNA starting at the D-loop region. Nature 1989;339:309-1 1.
166 Mechler F, Fawcett PRW, Mastaglia FL, Hudgson P.Mitochondrial myopathy: a study of clinically affectedand asymptomatic members of a six-generation family. 7Neurol Sci 198 1;50:191-200.
167 Ozawa M, Goto Y-I, Sakuta R, Tanno Y. Tsuji S, Nonaka I.The 8,344 mutation in mitochondrial DNA: a compari-
son between the proportion of mutant DNA and clinico-pathological findings. Neuromusc Disord 1995;5:483-8.
168 Suomalainen A, Ciafaloni E, Koga Y, Peltonen L,Dimauro S, Schon EA. Use of single strand conforma-tion polymorphism analysis to detect point mutations inhuman mitochondrial DNA. J Neurol Sci 1992;111:222-6.
169 Kawai H, Akaike M, Yokoi K, et al. Mitochondrialencephalomyopathy with autosomal dominant inheri-tance: a clinical and genetic entity of mitochondrial dis-eases. Muscle Nerve 1995;18:753-60.
170 Cheng S, Higuchi R, Stoneking M. Complete mitochondr-ial genome amplification. Nature Genet 1994;7:350-1.
171 Howell N, Kubacka I, Halvorson S, Howell B,McCullough DA, Mackey D. Phylogenetic analysis ofthe mitochondrial genomes from Leber hereditary opticneuropathy pedigrees. Genetics 1995;140:285-302.
172 Lertrit P, Kapsa RMI, Jean-Francois MJB, et al.Mitochondrial DNA polymorphism in disease: a possi-ble contributor to respiratory dysfunction. HumanMolecular Genetics 1994;3: 1973-81.
173 DiMauro S, Tonin P, Servidei S. Metabolic myopathies.In: Rowland LP, DiMauro S, eds. Handbook of clinicalneurology. Amsterdam: Elsevier, 1992:479-526.
174 MacLennan DH, Duff C, Zorzato F, et al. Ryanodinereceptor gene is a candidate for predisposition to malig-nant hyperthermia. Nature 1990;343:559-61.
175 Zorzato F, Fujii J, Otsu K, et al. Molecular cloning ofcDNA encoding human and rabbit forms of the Ca2'release channel (ryanodine receptor) of skeletal muscle. 7Biol Chem 1990;265:2244-56.
176 Arahata K, Engel AG. Monoclonal antibody analysis ofmononuclear cells in myopathies. I. Quantitation ofsubsets according to diagnosis and sites of accumulationand demonstration and counts of muscle fibers invadedby T cells. Ann Neurol 1984;16:193-208.
177 Karpati G, Carpenter S. Pathology of the inflammatorymyopathies. In: Mastaglia FL, ed. Inflammatorymyopathies. Bailliere's Clinical Neurology 1993,213:527-56.
178 Bernstein RM. Autoantibodies in myositis. In: MastagliaFL, ed. Inflammatory myopathies. Bailliere's ClinicalNeurology 1993;213:599-615.
179 Dalakas MC, Pezeshpour GH. Neuromuscular diseasesassociated with human immunodeficiency virus infec-tion. Ann Neurol 1988;23(suppl):S38-S48.
180 Mastaglia FL, Ojeda VJ. Inflammatory myopathies: Part I.Ann Neurol 1985;17:215-27.
181 Mastaglia FL, Laing BA, Zilko P. Treatment of inflamma-tory myopathies. In: Mastaglia FL, ed. Inflammatorymyopathies. Bailliere's Clinical Neurology 1993;2/3:717-40.
182 Woolf RE, Baethge BA. Interleukin-1a, interleukin-2, andsoluble interleukin-2 receptors in polymyositis. ArthRheum 1990;33:1007-14.
274
on Septem
ber 23, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.3.256 on 1 March 1996. D
ownloaded from