-
Investigations Stratification Front Line Clinical
ApplicationsNew Frontiers and Emerging Treatment Paradigms for
Optimizing Management of Obesity
Focus on Multimodal Interventions for Weight Loss and Novel
Pharmacological Strategies Targeting the Central Nervous
SystemMARC-ANDRE CORNIER, MD - Program ChairmanAssociate Professor
of MedicineDivision of Endocrinology, Metabolism and
DiabetesAnschutz Health and Wellness CenterUniversity of Colorado
School of MedicineDenver, CO
-
Distinguished FacultyMARC-ANDRE CORNIER, MD - Program
ChairmanAssociate Professor of MedicineDivision of Endocrinology,
Metabolism and DiabetesAnschutz Health and Wellness
CenterUniversity of Colorado School of MedicineDenver, CO
REKHA KUMAR, MD, MSDiabetes, Endocrinology and MetabolismWeill
Cornell Medical CollegeAssistant Professor of MedicineNew York
Presbyterian HospitalNew York, NY
ROBERT J. MALCOLM, MDProfessor, Department of Psychiatry and
Behavioral SciencesAssociate Dean for Continuing Medical Education,
College of MedicineMedical University of South CarolinaCharleston,
SC
-
Investigations Stratification Front Line Clinical
ApplicationsCurrent Challenges and Barriers to Optimizing
Management of Obesity
A Year 2014 Status Report for the Primary Care Physician and
Clinical Subspecialist
MARC-ANDRE CORNIER, MD - Program ChairmanAssociate Professor of
MedicineDivision of Endocrinology, Metabolism and DiabetesAnschutz
Health and Wellness CenterUniversity of Colorado School of
MedicineDenver, CO
-
Obesity by the NumbersOverweight U.S. adults:67%U.S. adults with
obesity:33%U.S. children with obesity:17%
Annual U.S. health care expenditures for obesity:> $ 200
billion
U.S. consumer expenditures for weight loss products:> $ 50
billionDaily deaths from obesity complications> 1,000
-
Disproportionate Increase in Severe ObesitySturm R, Pub Health,
2007Today, more than 1.7 million US adults with BMI>50
-
Complications of Obesity65+
-
Long-term Control of Obesity 20131% =750,000U.S. adults
Chart1
0.025
0.01
0.0005
0.96
Intervention
2.5%
Sheet1
LifestyleSurgeryMedicationsUnmet Needs
Intervention2.5%1%0.1%96%
-
Obesity is CounterintuitiveHides in plain sightMost obesity NOT
recognized by physicians or the publicNOT mainly in AmericaNOT
simply a problem of eating too muchNOT a single disorder very
heterogeneousPossibly 100 or more clinically meaningful
subtypesThis recognition is essential to solving the problem
-
Cause of Obesity Historical viewLifestyle
choiceCharacterological flaw (willpower, psychology) Current
perspectiveComplex physiologyEpidemic from changes in modern
environmentGenetic Predisposition (physiology) in the wrong
environmentWidely recognized as a disease Huge burden of associated
illness a cause of more than 60 medical disorders (including 12
types of cancer)Devastating effect on efficacy and quality of
life
-
Weight and Energy BalanceBy the laws of physics
-
Average adults consume 2000-2500 kcal/dayAverage adults
therefore consume 2-3 times as much food as requiredExcess intake
is available for physiological emergenciesMaintaining weight within
20 lbs. between ages 21 and 65 requires matching of intake and
expenditure within 0.2%Corresponds to accuracy of 4-5 kcal/dayLess
than one-half potato chipMaintenance of normal fat stores (and body
weight) requires precise disposal of 60-70% of ingested calories
dailyThe Normal Physiology of Energy Balance
-
Obesity: A Failure of Weight
RegulationGeneticsEnvironmentAltered food supplyReduced physical
activityStressDrugsOthers?
-
Barriers, Challenges and Opportunitiesto Obesity Management Our
biologyFavors fat storageCan this be
manipulated?EnvironmentMacroenvironment more difficult to
changeMicroenvironment can be changed by the individual?Health Care
SystemLack of buy in from providers, patients and
insurersOthers?
-
Epidemiology and Clinical Approaches to Obesity Management
What Do Trials, Algorithms, and Clinical Experience Teach Us
About Sequencing Treatment Approaches for Obesity? Investigations
Stratification Front Line Clinical ApplicationsREKHA KUMAR, MD,
MSDiabetes, Endocrinology and MetabolismWeill Cornell Medical
CollegeAssistant Professor of MedicineNew York Presbyterian
HospitalNew York, NY
-
Obesity DiagnosisObesity is defined an excess of body fatBody
fat is difficult to measure cheaplyFor people with average
lifestyles, Body Mass Index (BMI) has been the measure of
obesityBMI = Wt in Kg divided by height in M squaredBMI has been
divided into categories18-25 is normal, 25-30 is overweight, 30-35
is class I, 35-40 is class II, >40 is class III
-
Relationship Between Mortality and BMIData from Lew EA:
Mortality and weight: insured lives and the American Cancer Society
studies. Ann Intern Med 103:1024-1029, 1985.Very
LowLowModerateHighVery High20 25 30 35
402.52.01.51.00MenWomenMortality RatioBody Mass Index, kg/m2
-
Mortality: Diastolic Blood Pressure
-
Mortality: Body Mass Index
Chart1
1
1.2
1.6
2.5
Relative Risk
BMI (kg/m2)
Sheet1
20253035
Relative Risk11.21.62.5
-
BMI Classes are Poor at Estimating RiskThe BMI classes assume
that mortality and morbidity is proportional to BMIThis is not
necessarily true. There are very obese people who are otherwise
healthy.In other chronic diseases like cancer there is a staging
system to estimate riskAn obesity staging system may be a better
approach to estimating medical risk of obesity
-
EOSS Predicts Mortality in NHANES IIIPadwal R, Sharma AM et al.
CMAJ 2011
-
Edmonton Obesity Staging System (EOSS)Sharma AM & Kushner
RF, Int J Obes 2009MedicalMentalFunctionalabsentabsentabsent
-
Edmonton Obesity Staging SystemStage 0: No obesity related risk
factorsStage 1: Subclinical risk factors borderline HTN or DM,
minor aches or psychopathologyStage 2: Established obesity-related
disease HTN, DM, PCO, moderate limitations ADLStage 3: Established
organ damage MI, CHF, DM comp, significant limitations of ADLStage
4: Severe disabilities end stage and limitations like wheelchair
useSharma AM and Kushner RF. Int J Obes. 2009;33:289-95
-
EOSS Predicts Mortality at Every BMI Level NHANES IIIPadwal R,
Sharma AM et al. CMAJ 2011Overweight
-
EOSS Distribution Across BMI CategoriesNHANES III
(1988-1994)OverweightClass IIIPadwal R, Sharma AM et al. CMAJ
201150 million23 million10 million6 million
Chart1
15
28
47
10
Overweight
Sheet1
Overweight
EOSS Stage 015
EOSS Stage 128
EOSS Stage 247
EOSS Stage 310
To resize chart data range, drag lower right corner of
range.
Chart1
5
17
64
14
Class II
Sheet1
Class II
EOSS Stage 05
EOSS Stage 117
EOSS Stage 264
EOSS Stage 314
To resize chart data range, drag lower right corner of
range.
Chart1
8
19
59
14
Class I
Sheet1
Class I
EOSS Stage 08
EOSS Stage 119
EOSS Stage 259
EOSS Stage 314
To resize chart data range, drag lower right corner of
range.
Chart1
5
14
67
14
Class III
Sheet1
Class III
EOSS Stage 05
EOSS Stage 114
EOSS Stage 267
EOSS Stage 314
To resize chart data range, drag lower right corner of
range.
-
Obesity is Leveling in PrevalenceThe prevalence of obesity in
1961 was 10% in men and 15% in women defined as BMI >30Obesity
prevalence started to rise in 1980The prevalence of obesity is now
leveling off at 35.5% of the population.The prevalence of diabetes
follows the prevalence of obesity by approximately 10 yearsDiabetes
prevalence started to rise in 1990
-
NHANES Prevalence of Obesity1961-2012
Chart1
10.515
1216
12.216.5
2225
27.533.5
3133.4
32.235.5
35.535.8
Men
Women
Year
Percent of Population
BMI >30
Sheet1
6172789100040812
Men10.51212.22227.53132.235.5
Women151616.52533.533.435.535.8
To resize chart data range, drag lower right corner of
range.
m
w
-
Work Related Physical Activity is FallingChurch TS et al. Plos
One.2011;6(5):e19657
-
Fall in Energy Expenditure at WorkChurch TS et al. Plos
One.2011;6(5):e19657
1960 1970 1980 1990 2000 2010YearMean Occupation Related
METsOccupation Related Daily Energy Expenditure (calories)1960 1970
1980 1990 2000 2010Year
-
Weight Gain Predicted by Activity et al. Plos
One.2011;6(5):e19657
-
What is Causing the EpidemicPeople are less active and are
eating moreThere are many causes. We cannot just scapegoat fast
foodObesity virus Adenovirus D-36 is one causeEndocrine disruptors
have been suggestedRegardless of the cause, eating less and being
more active will help you will hear more in this seminar on ways to
accomplish that.
- Another Cause of ObesityAdenovirus of D group 36 (AD-36) causes
obesity in non-human primates but one cannot intentionally infect
humansAD-36 antibodies: 30% of obese and 11% leanIn identical twins
discordant for antibodies, the positive twin had 2.1% more fat and
had a BMI 1.4 units higher (p
-
Is Obesity Prevalence Important?Obesity is stigmatized
especially in women and causes psychological distress. Obesity is
associated with diabetesObesity is associated with hypertension and
heart diseaseObesity is associated with cancerObesity is associated
with osteoarthritis and much disability.
-
The Prevalence of Diabetes in the USCDC website
Chart1
5.8
5.8
5.8
5.9
6.1
6.4
6.6
6.6
6.5
6.4
6.7
7
7.6
7.8
8.3
8.3
8.5
10.3
10.5
11.1
12
12.9
13.6
14.2
15.2
16.3
17
17.8
19
20.2
20.9
Millions
Years
Millions in US with Diabetes
Sheet1
80818283848586878889909192939495969798990001020304050607080910
Millions5.85.85.85.96.16.46.66.66.56.46.777.67.88.38.38.510.310.511.11212.913.614.215.216.31717.81920.220.9
To resize chart data range, drag lower right corner of
range.
-
DiabetesThe prevalence of diabetes has tripled since the 1980s
and is increasingIt is estimated that 8.2% of the US population had
Type 2 diabetes in 2010 and it is predicted that 10.8% will have
Type 2 diabetes by 20200.2% of the population have type 1 diabetes
and 3.1% have undiagnosed diabetes28.4% of the US has
pre-diabetes
-
Diabetes is ExpensiveIt is estimated the diabetes costs the US
health care system $194 billion in 2010 and will cost an estimated
$500 billion in 2020.The US will spend approximately $3.4 trillion
in the next decade on diabetes-related careThe expense of diabetes
and those associated obesity-related diseases like cancer,
cardiovascular disease and others are and will stress our health
care delivery system
-
Obesity Increases Risk of Diabetes
Chart1
0
2
4
10
20
30
38
50
95
Risk DM
BMI
Fold Risk of DM
Sheet1
35
Risk DM024102030385095
To resize chart data range, drag lower right corner of
range.
-
Obesity Increases Disability
Chart1
0
18
25
35
40
55
Osteoarthritis
Quintile of Relative Weight
Percent With Osteoarthritis
Women Metropolitan Relative Weights
Sheet1
012345
Osteoarthritis01825354055
To resize chart data range, drag lower right corner of
range.
-
Mortality Risk with Staging SystemKuk JL et al. Appl Physiol
Nutr Metab. 2011;36:570-576HR for All CauseHR for All
CVDRefRef****
Chart1
1
1.1
1.4
1.6
Series 1
Sheet1
Series 1
NW1
Stage 0/11.1
Stage 21.4
Stage 31.6
To resize chart data range, drag lower right corner of
range.
Chart1
1
0.8
2
2.1
Series 1
Sheet1
Series 1
NW1
Stage 0/10.8
Stage 22
Stage 32.1
To resize chart data range, drag lower right corner of
range.
-
Association Between EOSS and Mortality Risk in Aerobics Center
Longitudinal Study (n = 29 533)Kuk JL, et al. Appl. Physiol. Nutr.
Metab. 2011;36: 570
-
Obesity Related Disease Improves with Weight LossSjostrom L et
al. N Engl J Med. 2007;357(8):741-52
Chart1
812.5
12.3
2.34.4
Weight Loss
Control
Percent
SOS Surgical Obesity Study
Sheet1
Weight LossControl
Mortality (p
-
SummaryObesity can be diagnosed by class and stagePeople in the
US are less active and eating more, but multiple causes for obesity
existComplications of obesity include diabetes, heart disease,
cancer and increased mortalityObesity is expensive and straining
our health care delivery systemIt is of utmost importance to screen
for obesity and intervene in its management
-
Regulating Energy Balance: The Pivotal Role of the Central
Nervous System in Appetite Regulation
Focus on 5HT2c Receptors and Other CNS Signaling Systems
Controlling Neuroregulation of Energy BalanceInvestigations
Stratification Front Line Clinical ApplicationsROBERT J. MALCOLM,
MDProfessor, Department of Psychiatry and Behavioral
SciencesAssociate Dean for Continuing Medical Education, College of
MedicineMedical University of South CarolinaCharleston, SC
-
Weight Regulating Mechanisms and Effect of Anti-obesity Drugs
Its Complicated!Valentino MA, Lin JE, Waldman SA. Clin Pharm &
Therapeutics (2010) 87 6, 652662.
doi:10.1038/clpt.2010.57Endogenous Signaling of Appetite-regulating
Hormones, Neuropeptides, and Neurotransmitters, and The Drugs That
Target These PathwaysSlide:Dr. Caroline Apovian
-
High EnergyENERGYENERGYSedentary LifestyleDense Foods(sugar or
fat)INTAKEEXPENDITUREGenetic &Biological
Susceptibilities(Underlying basis)
-
ControlledSystemControllerFeedback ModelAfferent
SignalsEfferent
ControlsFat
-
ControlledSystemControllerAfferent
SignalsEfferent
ControlsFatAnatomyMonoaminesPeptidesCytokinesFeedback Model
-
Picture of Frohlichs Case of Hypothlamic Obesity
-
Location of Hypothalamic Centers That Affect
FeedingLaThalamusMamillo-thalamicTrackDorsal HyopthalmusDorsomedial
HypoLateral HypoSurap-optic nucleusVentromedial HypoLateral
Hypothalamic Lesions Ventromedial Hypothalamic Lesions
-
ControlledSystemControllerAfferent
SignalsEfferent
ControlsFatAnatomyMonoaminesPeptidesCytokinesFeedback Model
-
Monoamines, Peptides, Amino Acids & Drugs Affecting Food
Intake Anandamide (cannabinoid agonist)Serotonin (5HT-1a auto)
Serotonin Pump InhibitorsAnti-histamines Serotonin (5
HT-2c)Gamma-amino butyric acid (GABA)Histamine Noradrenergic Agents
Cannabinoid Antagonists
-
Serotonin Biology - ISerotonin is most concentrated in the
hypothalamus, basal ganglia and brainstem7 groups of 14 serotonin
receptors are known5HT-1 - Intronless, G-protein coupled receptor
that inhibits adenylyl cyclase5HT-2Contains introns, that are
coupled to G-protein receptors that activate phospholipase C5-HT2C
is only in the brain 5HT-3 - Ligand-gated ion channel
-
Activation of 5-HT1A auto-receptor increases feedingActivation
of 5-HT1B and 5-HT2C by any 5-HT agonist will reduce food
intake5-HT receptors in PVN specifically decrease fat
intakeKnock-out of 5-HT2C receptor produces obesity and
convulsions. Serotonin reuptake inhibitors and releasers can
precipitate weight loss or weight gain
Serotonin Biology - II
-
02468101214CarbohydrateFatProtein2-Hr Food Intake
(kcal)SalineSerotoninSmith B et al AJP 1999Macronutrient
ChoiceSerotonin (and Other Agonists) in PVN Reduce Food Intake
-
5-HT2CRs Expressed by Pro-opiomelanocortin Neurons Regulate
Insulin Sensitivity in Liver Mice lacking 5-HT 2C receptors have
hepatic insulin resistanceWhich is normalized by re-expression of
5-HT(2C) receptors only in pro-opiomelanocortin (POMC) neurons
Evidence that 5-HT2C Rs expressed by POMC neurons are
physiologically important in regulating hepatic glucose production
and insulin sensitivityMoreover, this 5-HT2C R-melanocortin circuit
is sufficient to mediate the anti-diabetic effects of 5-HT2CR
agonists.Xu Y, et al Nat Neurosci. 2010 Dec;13(12):1457-9. Epub
2010 Oct 31
-
Serotonin 2c Receptor and Diabetes
-
Anorectic serotonin (5-HT) drugs activate pro-opiomelanocortin
(POMC) neurons in the arcuate nucleus of the hypothalamus. A
serotonin 2C receptor is expressed on POMC neurons and contributes
to this effect. Hypophagia induced by serotonin (5-HT) is
attenuated by either pharmacological or genetic blockade of
downstream melanocortin 3 and 4 receptors. Serotonin Interacts with
Melanocortin Pathways Regulating Energy Homeostasis
Heisler LK, Dowley MA Kishi T. Ann N Y Acad Sci. 2003
Jun;994:169-74.
-
Serotonin and Melancortin ReceptorsWe conclude that serotonin
(5-HT) drugs require functional 5-HT2C receptors in the POMC that
modulate melanocortin pathways to exert their effects on food
intake.
In animals without serotonin receptors, replacement specifically
in the POMC neurons restores suppression of insulin by CNS
serotonin Heisler LK, Dowley MA Kishi T. Ann N Y Acad Sci. 2003
Jun;1994:169-74.
-
INDEX Study CompletersMean Weight Loss (% Initial
Weight)Guy-Grand et al INDEX study Lancet 1988
-
Phentermine: A Noradrenergic Drug Reduces Body WeightMunro JF et
al BMJ 1968;1:352-4
-
ControlledSystemControllerAfferent
SignalsEfferent
ControlsFatAnatomyMonoaminesPeptidesCytokinesFeedback Model
-
Agouti-related peptideDynorphinGhrelinMelanin-concentrating
hormoneNeuropeptide YOrexin A (Hypocretin)RF-2 peptides (arginine
phenylalanine amide-2)Galanin-like-peptide
-MSHCorticotrophin-releasing
hormoneCholecystokininCocaine-amphetamine regulated
transcriptGlucagon-like peptide-1LeptinAmylinBombesin/GRPObestatin
(part of ghrelin)Nesfatin-1 (NEFA-NUCB2)Peptides That Affect Food
Intake
-
Peptides That Affect Food IntakeAgouti-related
peptideDynorphinGhrelinMelanin-concentrating hormoneNeuropeptide
YOrexin A (Hypocretin)RF-2 peptides (arginine phenylalanine
amide-2)Galanin-like-peptide -MSHCorticotrophin-releasing
hormoneCholecystokininCocaine-amphetamine regulated
transcriptGlucagon-like peptide-1LeptinAmylinBombesin/GRPObestatin
(part of ghrelin)Nesfatin-1 (NEFA-NUCB2)
-
Leptin the Ultimate Messenger of Fat StoresWeight Loss
POMC Serotonin 5-HT2c
Hypothalamus Leptin
-
Model of the Arcuate NucleusModel showing the afferentsignals
from the periphery that modulate the activityof hypothalamic
neurons ina reciprocal way to increaseor decrease food
intakeBadman, Science 2005
-
ControlledSystemControllerAfferent
SignalsEfferent
ControlsFatAnatomyMonoaminesPeptidesCytokinesFeedback Model
-
.Consumption of a High Fat Diet rapidly induces neuronal injury
in a brain area critical for energy homeostasis.
Thaler, J et al, J Clin Invest. 2012 Jan 3;122(1):153-62.
Obesity Is Associated with Inflammatory Hypothalamic Injury
-
Hypothalamic Inflammatory Markers Increase on High Fat
Diet0.51.01.52.02.0Il1-b Il-6 Tnf- Socs3 Nfkb IkBkb IkBk
Inflammatory MarkersmRNA (fold increase)Thaler JP et al J Clin
Invest 2012;122:153-162
-
.Consumption of a HFD rapidly induces neuronal injury in a brain
area critical for energy homeostasis.
In human beings there is MRI evidence for gliosis in the
hypothalamus of obese humans.
Collectively, this work identifies a potential link between
obesity and hypothalamic injury in humans as well as animal
models.
Thaler, J et al, J Clin Invest. 2012 Jan 3;122(1):153-62.
Obesity Is Associated with Inflammatory Hypothalamic Injury
-
Leptin Resistance and CytokinesTaking all of these phenomena
into account, we think that it is possible that overconsumption of
nutrients could be a reason for development of leptin
resistanceThis line of thinking favors the fact that increased
adiposity and consequent hyperleptinemia decreases the leptin
action and creates the leptin resistance
Ergin A, Cell Metabolism 2008;12:2004
-
Does This Explain How Something Environmental Turns Into
Something Physical?High fat diets and inflammationEvidence of
apoptosis and glial ensheathment of ARC neurons in animals rendered
obese by chronic HFD feeding. Moreover, these responses were
detected specifically in ARC POMC cells 25% reduction in the number
of hypothalamic POMC neurons Mice chronically fed a HFD. POMC cells
play an essential role to protect against obesityLoss of these
cells is sufficient in and of itself to cause excess weight gain in
mice Fattening Foods Cause Dropout of POMC Neurons and Glial
Ensheathment of ARC Neurons. Does That Explain Why Its So Hard To
Lose Weight?
-
Hypothetical Feed-forward, Positive Feedback Mechanism Drives
Weight UpWang J, Diabetes, 2001; DiMarzo V pers commOzcan L et al
Cell Metabolism; 2009 2012 Louis J. Aronne, MD
-
Food IntakeGut and LiverPancreasAutonomic Nervous SystemEnergy
ExpenditureAdipose Tissue 2007 LJ Aronne MD. Adapted from Campfield
LA et al. Science. 1998;280:1383-1387; Porte D et al. Diabetologia.
1998;41:863-881.Adrenal CortexEnergy Balance and Adipose StoresMeal
SizeAdrenal SteroidsLeptinAmylinInsulinExternal Factors Food
Availability, PalatabilityAdiponectinGhrelinGLP-1CCKVagusAfferent
Signals
EfferentNPYAGRPgalaninOrexin-ADynorphinCannabinoidsStimulate-MSHCRH/UCNGLP-ICARTNE5-HTInhibitCentral
SignalsWhat is Causing the Epidemic of Obesity and Why Is It So
Hard to Lose Weight?
-
Weight Regulating Mechanisms and Effect of Anti-obesity Drugs
Its Complicated!Valentino MA, Lin JE, Waldman SA. Clin Pharm &
Therapeutics (2010) 87 6, 652662.
doi:10.1038/clpt.2010.57Endogenous Signaling of Appetite-regulating
Hormones, Neuropeptides, and Neurotransmitters, and The Drugs That
Target These PathwaysSlide:Dr. Caroline Apovian
-
Treatment Gap in the Management of ObesityPhysicians Need
Effective Pharmacotherapies That Will Reduce Weight Significantly
and Reduce Weight-related Comorbidities0%
5%10%15%20%25%30%35%Current PharmacotherapyLap BandGastric
BypassTreatmentGapToo risky for many people
-
New Frontiers and Treatment Paradigms for Pharmacologic
Management of Obesity
Focus on Safety and Efficacy of Agents Affecting CNS Signaling
Systems and Appetite RegulationInvestigations Stratification Front
Line Clinical ApplicationsMARC-ANDRE CORNIER, MD - Program
ChairmanAssociate Professor of MedicineDivision of Endocrinology,
Metabolism and DiabetesAnschutz Health and Wellness
CenterUniversity of Colorado School of MedicineDenver, CO
-
Overall Treatment StrategyTypical Algorithm(Progress through
algorithm as clinically required)
-
Guide to Selecting Obesity Treatment
BMI
Treatment
40
Diet
Exercise
+
+
+
+
+
Pharmacology
w/ co- morbidities
+
+
+
Surgery
w/ co-morbidities
+
-
Where Have We Been? Where Are We Going?Obesity: A
physiologically controlled chronic disease. Medications work when
taken.Safety and benefit issues with obesityThe evolution of
chronic disease medicationsDrugs recently approved Drugs in late
developmentObesity drugs in the future
-
Fenfluramine 1-Year Rx & 1-Year Follow-up
-
Chronic Disease Drug DevelopmentDiuretics salt in urineCNS drugs
side effects eg. reserpine and depressionCombinations to lower side
effects and increase efficacyPeripherally acting drugs eg.
angiotensin receptor blockersOrlistat calories in stoolCNS drugs
side effects eg. amphetamine and addictionCombinations to lower
side effects and increase efficacy eg
topiramate-phenterminePeripherally acting drugs (in
development)
-
Obesity Pharmacotherapy A Bad Safety Record1893: Thyroid hormone
-> hyperthyroidism1933: Dinitrophenol ->
cataracts/neuropathy1937: Amphetamine -> addiction1967: Rainbow
pills (digitalis & diuretics) -> CV sx 1997: Fenfluramine
-> valvulopathy2000: Phenylpropanolamine -> stroke2004:
Herbal caffeine & ephedra -> CV sx2010: Sibutramine -> MI
and stroke
-
Weight Loss Drugs Approved by
FDAPhentermine/TopiramateQsymiaLorcaserinBelviqOrlistat Xenical,
Alli PhentermineAdipex, Fastin, Ionamin Diethylpropion Tenuate,
Tenuate, DospanPhendimetrazine Bontril, Plegine, Prelu-2,
X-TrozineMethamphetamine DesoxynBenzphetamine Didrex Mazindol
Sanorex, Mazanor
Generic Name Trade Name
-
Efficacy of Currently Available Weight Loss Medications
DrugPhentermineOrlistatLorcaserinPhentermine/TopiramateAverage
Weight Loss 3.6% > placebo2.75% > placebo3.3% > placebo9%
> placebo
-
PhentermineMechanism: Appetite suppressantInhibits NE and
dopamine releaseDose: 15-37.5 mg daily (AM)FDA approved for
short-term (3 months) useSide effects: Increased BP and HR,
insomnia, agitation, dry mouth, headache, tremorEfficacy: More
weight loss than placebo (~3-5%)
-
OrlistatMechanism: Inhibits lipases and blocks fat absorption by
~30% (reduction in absorbed fat)Dose: 60-120 mg TID (with meals)FDA
approved for long-term useSide effects: mild to moderate GI events,
potential for malabsorption of fat soluble vitamins, liver
toxicity?, nephrolithiasisEfficacy:More weight loss than placebo
(~4%)More lose at least 5% (35-69% vs 16-30% with placebo)More lose
at least 10% (16-25% vs 4-12% with placebo)Prevention of diabetes
incidenceImprovements in glycemic control in T2D
-
Lorcaserin Brand name: BelviqApproved in 2012 (10 mg BID) for
long-term weight managementMechanism:Selective 5-HT2C receptor
agonistincreases satiety appetite suppressantBays HE. Expert Rev
Cardiovasc Ther. 2009;7:1429-1445; Belviq [prescribing
information]. Woodcliff Lake, NJ: Eisai; Inc. 2012.
-
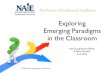
BLOOM Study Body Weight Over Years 1 and 25.81 0.16%2.16
0.14%BLOOM = Behavioral Modification and Lorcaserin for Obesity.
Smith SR, et al. N Engl J Med. 2010;363:245-256.
-
5.81 0.16%2.16 0.14%BLOOM = Behavioral Modification and
Lorcaserin for Obesity. Smith SR, et al. N Engl J Med.
2010;363:245-256.BLOOM Study Body Weight Over Years 1 and 2
-
47.5%20.3%22.6%7.7%BLOOM = Behavioral Modification and
Lorcaserin for Obesity. Smith SR, et al. N Engl J Med.
2010;363:245-256.BLOOM Study Body Weight Over Years 1 and 2
- Fasting Plasma GlucoseBLOOM-DMChange in Glycemic
ParametersHbA1C, -0.5%*P
-
Summary of EchocardiographicSafety MonitoringMore than 20,000
echocardiographsMore than 7,500 patientsLorcaserin did not increase
the risk of valvulopathy above the pre-specified margin relative to
placeboLorcaserin did not meaningfully affect regurgitant scores at
any heart valveFDA defined valvulopathy relative risk: 1.16 (95%
confidence interval (0.81, 1.67, NS)
-
Lorcaserin Most common AEs: Headache, nausea, dizziness,
fatigue, dry mouth, constipationNotesDiscontinue if 5% weight loss
is not achieved by week 12Discontinue for evaluation if signs or
symptoms of valvular heart diseaseDEA Schedule CIVPregnancy
category X Interesting effect on glycemia greater benefit than
expected for degree of weight lossBays HE. Expert Rev Cardiovasc
Ther. 2009;7:1429-1445; Belviq [prescribing information]. Woodcliff
Lake, NJ: Eisai; Inc. 2012.
-
Phentermine and FenfluraminePhen - FenWeintraub M et al. Clin
Pharmacol Ther. 51(5):586-94, 1992.
Chart1
00
-2-1
-4-3
-5-4
-7-5
-10-6.5
-11-7
-13-7
-15-7
-16-6.5
-16-6
-16-4
Phen 15/Fen 60 mg/d
Placebo
Weeks
Kg
N=121 p
-
Phentermine/Topiramate ERBrand name: QsymiaApproved in 2012 for
long-term weight managementMechanism:Phentermine: inhibits NE and
dopamine releaseTopiramate: mechanism on weight loss is not
knownIncreases satiety appetite suppressantDosing:Start at
3.75/23mg daily x 2 weeks thento 7.5/46mgAfter 12 weeks canto
11.25/69mg and 15/92mg
-
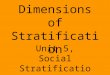
Gadde KM et al. Lancet.
2011;377(9774):1314-52Phentermine/Topiramate Phase III Trial
Chart1
000
-2-5-6
-3-8-10
-3.5-9-11.5
-3.5-10-12.5
-3-11-13
-2.5-11-13
-2-10.5-13
Placebo
Mid-Dose
High-Dose
Weeks
Percent Weight Loss
N = 2,487
Sheet1
PlaceboMid-DoseHigh-Dose
0000
8-2-5-6
16-3-8-10
24-3.5-9-11.5
32-3.5-10-12.5
40-3-11-13
48-2.5-11-13
56-2-10.5-13
-
Phentermine/Topiramate Phase III TrialGadde KM et al. Lancet.
2011;377(9774):1314-52
-
Phentermine/Topiramate Phase III TrialGarvey, et al. Am J Clin
Nutr 2012;95:297-308.
-
Phentermine/Topiramate ERMost common AEs: paresthesias,
dizziness, dysgeusia, insomnia, constipation and dry mouth.Other
AEs: BP and HR, headache, suicidal thoughts, myopia/secondary angle
closure glaucoma, cognitive impairment, metabolic
acidosis,creatinineNotesDiscontinue if 5% weight loss is not
achieved by week 12DEA Schedule Class IVPregnancy category X
Safety: fetal cleft palate - pregnancy test q mo.
-
Obesity Drugs and CVD Risk FactorsBays HE. Specialty Corner:
Investigational Anti-obesity Agents to Treat Adiposopathy and "Sick
Fat. pages 22-23. 2011
Anti-Obesity AgentBPLDL-CTGHDL-CPhentermine/ Topirmate
ERLorcaserinNo significant change
-
Whats in the Pipeline?New Frontiers and Treatment Paradigms for
Pharmacologic Management of Obesity
-
Naltrexone/BupropionNot yet FDA approvedCVD safety study in
progressDose: 3 week escalation to 16/180mg SR
bidMechanism:Naltrexone: opioid receptor antagonistBuproprion:
NE/dopamine reuptake inhibitorAppetite suppressant, reduces
cravings?Adverse events : Nausea, headache, constipation,
dizziness, vomiting, insomnia, dry mouth & hot flushes
- Bupropion 360 & Naltrexone 32
mgITT-LOCFObservedPlacebo-subtracted weight lossWeek 56NB16:
-3.7%NB32: -4.8%Placebo-subtracted weight lossCompletersNB16:
-4.9%NB32: -6.2%P
-
Liraglutide 3 mg/d in Obese SubjectsAstrup A et al. Lancet
374(9701):1606-16, 2009
Chart1
000
-1.2-1.4-1.6
-3-3.5-5.5
-4-5-7.5
-4-5.4-8
-3.8-5.4-8.5
Placebo
Orlistat 360mg/d
Liraglutide 3mg/d
Weeks
Kg Weight Lost
N=300, P
-
Zonisamide 360 + Bupropion 360 mgWeight Loss at 1 Year of
TreatmentPlacebo
(a)(N=72)Z120/B280(N=27)Z120/B360(N=36)Z240/B280(N=36)Z240/B360(N=26)Z360/B280(N=32)Z360/B360(N=39)(a)
Placebo weight loss through 24 weeks as noted previously
-
BeloranibMethionine Aminopeptidase 2 (MetAP2) Inhibitor METAP2
is an enzyme which plays a key role in the production and use of
fatty acidsReduced food intake?Reduced lipogenesis?Increased
lipolysis?
-
Belornib - Body Weight in MiceBody weights during the course of
1 mg/kg/day fumagillin (ZGN-201) treatment
- Belornib Weight Loss in HumansImpact of 2-18 ug/kg/dose ZGN-433
treatment on body weight in obese womenValues are medians SEM
(n=6-8) for the per protocol population.*** p
-
SummaryObesity is a chronic physiologically controlled disease
that requires chronic treatmentWe have two new CNS acting drugs for
obesity lorcaserin and phentermine/topiramateThere are 3 drugs in
late stage development: naltrexone/bupropion, liraglutide,
andzonisamide/bupropionPeripherally acting drugs are being
developed but may be limited by side effects.There is significant
variability in the weight loss response, so important to consider
predictors of response as we move forward
-
Real World Challenges in Obesity ManagementCase Study-Based
Learning Workshops and Clinical Simulations in Obesity
Management
Investigations Stratification Front Line Clinical
ApplicationsMARC-ANDRE CORNIER, MD - Program ChairmanAssociate
Professor of MedicineDivision of Endocrinology, Metabolism and
DiabetesAnschutz Health and Wellness CenterUniversity of Colorado
School of MedicineDenver, CO
-
ER, a 46-year-old woman, initially presents with high blood
pressure, which has been well controlled with a diuretic agent.
Since her last visit 6 months ago, she has been experiencing
some heartburn, self-treated with over-the-counter H2-blockers, and
more aching in her weight-bearing joints.
On exam, her height is 66 inches and body weight is 190 pounds,
up 5 pounds from her last visit. Blood pressure is 134/90, up
several points from her last visit as well. The rest of the exam is
unchanged.
Her previous lab tests were within normal limits. Current test
results indicate a fasting glucose of 118 mg/dL, total
triglycerides of 255 mg/dL, and high-density lipoprotein (HDL
cholesterol) of 42 mg/dL. All other tests are normal.Case Study
1
-
Case Study 1With a height of 66 inches and weight of 190 pounds,
ERs BMI is 31. This places her in Class I (mild) obesity.
Her waist circumference is 36 inches. This, in addition to her
triglycerides of 225 mg/dL, fasting glucose of 118 mg/dL, HDL
cholesterol of 42 mg/dL, and blood pressure of 134/90, shows that
she has the metabolic syndrome. This places her at increased risk
of cardiovascular disease.
In reviewing ERs history, you identify five obesity-related
conditions:HypertensionGastroesophageal reflux disease
(GERD)Impaired glucose tolerance (possible
diabetes)Hypertriglyceridemia and low HDL-C levelsArthralgia
-
Case Study 1 - Question 1You decide to order additional tests to
evaluate ERs hypertension and diabetes.
Based on the NHLBI algorithm, treatment for ERs obesity is
indicated.
At this point you would:
Recommend diet and lifestyle changesInitiate orlistatInitiate
lorcaserinInitiate phentermineInitiate phentermine HCl/topiramate
CR
-
Case Study 1 - Question 2In this case, diet and lifestyle
changes were recommended, with an assessment after 90 days.
The patient returned with an additional 2 lb. weight gain and
reported difficulty in maintaining diet.
At this point you would:Modify diet and lifestyle
recommendations and reassess in 90 daysInitiate orlistatInitiate
lorcaserinInitiate phentermineInitiate phentermine HCl/topiramate
CR
-
Case Study 1 - Question 390 days later, she is tolerating the
weight management drug well, has experienced a 5% weight loss, and
improvement in metabolic parameters. She reports increased energy
and improved self-esteem.
At this point you would:
Cease pharmacotherapy and recommend diet and lifestyle
changesCease pharmacotherapy, recommend diet and lifestyle changes,
and revisit in 90 daysMaintain current pharmacotherapySwitch to
alternative pharmacotherapy
-
Case Study 1 - Question 490 days later, she is not tolerating
the weight management drug well, has experienced a 5% weight loss,
and improvement in metabolic parameters. She reports increased
energy and improved self-esteem.
At this point you would:
Cease pharmacotherapy and recommend diet and lifestyle
changesCease pharmacotherapy, recommend diet and lifestyle changes,
and revisit in 90 daysMaintain current pharmacotherapySwitch to
alternative pharmacotherapy
-
42-year-old man with BMI 37Weight 242 lbs., up 5 lbs. from 6
months earlierGout well-controlled on allopurinolHyperlipidemia (on
low-dose simvastatin); bilateral knee arthritisExaminationCentral
obesity with waist circumference 44 in.BP 132/82Laboratory
studiesFasting glucose 90Fasting triglycerides 260Cholesterol 220;
LDL cholesterol 146; HDL cholesterol 38Other tests normalCase Study
2
-
Weight and lifestyle historyMildly heavy as a childGrew out of
it during adolescence; participated in competitive sports in high
school and college Weight stable at ~185 lbs. (BMI 28.3) until 12
years agoSlowly progressive 55 lb. weight gain over last 10
yearsWorks as salesman with hectic lifestyle; irregular meals;
frequent fast foods and snackingNo previous serious weight loss
attempts; feels healthyHas exercised at gym 4x/week over the past
year with only 4 lb. weight lossCase Study 2
-
Case Study 2 - Question 1You increase the dose of
simvastatin.What would you do to treat the obesity?Recommend a
healthier and more regular dietEncourage a more vigorous exercise
programRefer him to a psychologist for behavior
modificationInitiate orlistat therapyInitiate lorcaserin therapy42
MBMI 37Central distributionPre-DMDyslipidemiaGERD GoutOAChildhood
onsetSteady adult gainIrregular eaterFast food dietRegular
exerciserHectic lifestyle
-
Clinical progressHe listens to your dietary advice and stops
snackingHis hectic lifestyle continues, but he eats more meals at
home and is able to change from fast food to family style
restaurants when travelingContinues to exercise regularlyLost 4
lbs. (to 238 lbs.) in the first month but none since, despite
maintaining his new lifestyleAt follow-up 3 months later, his
weight is 239 lbs., BP 128/84 and LDL and total cholesterol in the
normal rangeCase Study 2
-
What would you do now?Continue to encourage a healthy dietRefer
to dietitian for nutritional managementRefer to a stress management
programInitiate phentermine therapyInitiate lorcaserin therapyCase
Study 2 Question 2
-
Clinical progressHe sees a dietitian who recommends a specific
dietary regimen, which he follows reasonably wellOver the ensuing 3
months, he loses 12 lbs.At his annual visit 9 months after that,
however, he has regained 10 of the 12 lbs. and weighs 237 lbs. (BMI
36.2)His cholesterol levels and BP remain normalHis fasting glucose
is 114, and his triglyceride level is 222, and his HbA1c is
6.6%Case Study 2
-
What would you do now?Continue to encourage a healthy dietRefer
back to the dietitian for additional counselingRefer to a stress
management programInitiate phentermine therapyInitiate lorcaserin
therapyCase Study 2 Question 3
-
Clinical progressYou begin phentermine at 15 mg/day, monitoring
BP and pulse carefullyHe reports dry mouth that resolves after
about 3 weeks; he otherwise tolerates the medication well, without
tachycardia, hypertension or subjective adverse effectsAt 30 days,
he has lost 5 lbs. (2.1% of pretreatment weight)At 3 months, he
weighs 223 lbs. (BMI 34.1), having lost 14 lbs. (5.9%) on
phentermineHe continues the recommended dietary changesTwo months
later (on phentermine for 5 months), he has lost 1 additional lb.
and weighs 222 lbs. (BMI 33.9)Total weight loss 20 lbs. since first
visit; total weight loss on phentermine 15 lbs. (6.3%)Case Study
2
-
Case Study 2 - Question 4What would you do now?Continue the
phentermine at 15 mg/day and re-emphasize the recommended diet and
lifestyle changesStop the phentermine and follow his clinical
progressStop the phentermine and start orlistat at 120 mg
tidIncrease the phentermine to 30 mg/dayRecommend consultation for
bariatric surgery
-
Clinical progressHe tolerates the increased dose of phentermine
well with only transient dry mouthAt 30 days, he has lost 2
additional lbs. (0.8% of pretreatment weight)At 3 months, he weighs
221 lbs. (BMI 33.8), having lost 16 lbs. (5.9%) on phentermine
overallCase Study 2
-
Case Study 2 - Question 5What would you do now?Continue the
phentermine at 30 mg/day and refer back to the dietitianStop the
phentermine and follow his clinical progressStop the phentermine
and start orlistat at 120 mg tidAdd topiramate by substituting the
low-dose combination of phentermine (3.75 mg/day) and topiramate
(23 mg/day) for the phentermine aloneRecommend consultation for
bariatric surgery
-
Clinical progressHe tolerates the low-dose
phentermine-topiramate combination (phen-top) well, without adverse
effectsAfter 14 days, you increase the phen-top dose to 7.5 mg
phentermine + 46 mg topiramate dailyIn the first 30 days of
phen-top therapy, he loses 3 lbs. to a weight of 218 lbs. (BMI
33.3)Over the next 3 months, he loses an additional 8 lbs. to a
weight of 210 lbs. (BMI 32.1)Case Study 2
-
Weight loss summaryInitial weight 242 (BMI 37)Diet modification
5 lb. weight loss over 1 year (2.1%)Phentermine 16 lb. weight loss
over 8 months (6.8%)Phentermine-topiramate combination 11 lb.
additional weight loss over 4 months (4.9%)Total medication-induced
weight loss 27 lbs. (11.4%)Current weight 210 lbs. (BMI 32.1), down
32 lbs. (13.2%) overall since initial visit 2 years earlierCase
Study 2
-
Case Study 2 - Question 6What would you do now?Continue the
phen-top at current dosingStop the phen-top, re-enforce lifestyle
adjustments and follow his clinical progressIncrease the phen-top
dosing to 15 mg phentermine + 92 mg topiramate daily (high dose)Add
lorcaserin at 10 mg bidRecommend consultation for bariatric
surgery
-
51-year-old woman with BMI 43.3Weight 252 lbs., height
54Well-controlled hypertension, hypothyroidism, Barretts esophagus,
osteoarthritis (s/p knee replacement), colonic polyps, and
depressionType 2 diabetes on pioglitazone, glimepiride and insulin
(long- and short-acting to total of 65 units/day) no eye,
neurological or vascular complicationsSleep apnea well-controlled
on CPAPOther medications include losartan, hydrochlorthiazide,
omeprazole, levothyroxine, omeprazole, aspirin and sertralineCase
Study 3
-
ExaminationCentral obesity with waist circumference 41
in.Benign, protuberant abdomen; no signs of chronic liver diseaseNo
signs of peripheral neuropathyBenign abdomenLaboratory
studiesFasting glucose 111HbA1c 7.1%AST 43, ALT 51, alkaline
phosphatase 120BUN 32; creatinine 1.2TSH 5.64Other tests normalCase
Study 3
-
Weight and lifestyle historyNormal weight as a child; overweight
in college and graduate school (weight 150-175; BMI
26-30)Progressive weight gain in adult life; insatiable appetite
with frequent cravings and large portionsNumerous unsupervised,
supervised and structured diets with variable weight loss (up to 30
lbs.); none maintainedAverage weight stable over the past few
years; currently at highest lifetime weightMarried with grown
children; works as financial plannerCooks regularly and well, and
entertains oftenExercises three times a week with a physical
trainerCase Study 3
-
Case Study 3 - Question 1You increase the dose of L-thyroxine.
How would you initiate obesity treatment?Recommend a
meal-replacement programSubstitute citalopram for sertralineRefer
her to a psychologist for cognitive-behavior therapy for the
depressionSubstitute metformin for glimepirideInitiate treatment
with a combination of phentermine and topiramate51 FBMI 43.3Central
distributionT2DM (55OSAHypothyroidismGERD / BarrettsOAColonic
polypsDepressionAdult onsetHealthy dietOften hungryLarge
portionsRegular exerciser
-
Clinical progressYou discontinue the sulfonylurea and start
metformin at 500 mg bid, monitoring her glucose carefully and
adjusting short-acting insulin as requiredIn the next 30 days, she
loses 5 lbs. to a weight of 247 lbs. (BMI 42.4)You increase the
metformin to 750 mg bidAt 3 months, she has lost a total of 14 lbs.
(5.6%) to 238 lbs.She reports a noticeably diminished appetite and
cravingsInsulin requirement falls from 65 to 52 units/day3 months
later, her weight is stable at 235 lbs. (BMI 40.3), down 17 lbs.
(6.7%)Case Study 3
-
Case Study 3 - Question 2What would you do now to treat the
obesity?Refer to a commercial weight loss programSubstitute
bupropion for sertralineInitiate therapy with a combination of
phentermine and topiramateInitiate therapy with lorcaserinRefer for
bariatric surgery
-
Clinical progressLow-dose phen-top (phentermine 3.75 mg +
topiramate 23 mg daily) initiated and well-toleratedAfter 14 days,
you increase the phen-top dose to phentermine 7.5 mg + topiramate
46 mg daily with no adverse consequencesIn the first 30 days of
therapy, she loses 4 lbs. (1.7%) to 231 lbs. (BMI 39.6)At 3 months,
she has lost a total of 6 lbs. (2.6%) to 229 lbs.Case Study 3
-
Case Study 3 - Question 3What would you do now?Continue the
phen-top at current dosing and add orlistat at 120 mg tidStop the
phen-top and start phentermine at 15 mg dailyStop the phen-top and
start lorcaserin at 10 mg bidStop the phen-top and start orlistat
at 120 mg tidStop the phen-top and substitute liraglutide s.c. for
the pioglitazone
-
Clinical progressShe tolerates the new medication wellAfter 30
days, she reports feeling increased hunger and her weight has
increased 3 lbs. to 232 lbs. After 60 days, her weight remains at
232 lbs. (BMI 39.8)Her diabetes remains well-controlled with a
fasting glucose of 114 and HbA1c of 6.9%Case Study 3
-
Case Study 3 - Question 4What would you do now?Stop all weight
loss medications and refer to a dietitian to reinforce healthy
eating habitsStop all weight loss medications and refer to a
psychologist for behavioral therapyContinue the current regimen and
restart a combination of phentermine and topiramateStop all weight
loss medications and institute an 8-week physician-supervised very
low calorie diet (VLCD)Stop all weight loss medications and refer
for bariatric surgery
-
Clinical progressShe undergoes uneventful laparoscopic Roux-en-Y
gastric bypass with post-operative weight loss ~50 lbs.Her diabetes
remains well controlled (HbA1c 6.6%) without need for insulin,
pioglitazone or liraglutide, and on a reduced dose of metformin
(500 mg bid)Other comorbidities improved or resolved except for
continued joint pain and reflux symptomsOne year after surgery, her
weight is down 51 lbs. to 181 lbs. (BMI 31.1), which has been
stable for more than 3 monthsShe feels much better overall but is a
bit disappointed in the weight loss outcome (which is less than the
average 65% excess weight loss from this operation)Case Study 3
-
Case Study 3 - Question 5What would you do now?Indicate that
there is no further therapy beyond surgery and reinforce the need
to follow a healthy lifestyleRefer her to a psychologist to help
address her expectationsEncourage her to extend post-operative
weight loss with a low-calorie (calorie restricted) dietInstitute
pharmacological therapy with lorcaserinRefer her back to the
surgeon for consideration of revising the surgical procedure
-
Clinical progressLorcaserin at 10 mg/day is started and
well-toleratedOver the next 6 months, she loses an additional 15
lbs. to a weight of 164 lbs. (BMI 27.3)Her comorbidities remain
improved, and her diabetes is in remission off all medications
(HbA1c 6.3%)Case Study 3
-
Weight loss summaryInitial weight 252 (BMI 43.3)Substitution for
weight-promoting drugs 23 lb. weight loss over 1 year
(2.1%)Phentermine-topiramate combination 16 lb. weight loss over 3
months (2.6%)Other pharmacological agents 3 lb. weight gain over 2
months (1.3%)Total medical weight loss 20 lbs. (7.9%)Gastric bypass
51 lbs. (22.0%) weight loss over 1 year (58.8% excess weight
loss)Lorcaserin after surgery 15 lbs. over 6 months Current weight
159 lbs. (BMI 27.3), down 93 lbs. (36.9%) since initial visit 3
years earlierCase Study 3
-
46-year-old woman with BMI 30.7Weight 190 lbs., up 5 lbs. from 6
months earlierHypertension, heartburn, weight-bearing joint pain
ExaminationCentral obesity with waist circumference 36 in.BP
134/90Laboratory studiesGlucose 118; HbA1c 6.4%Triglycerides 255
mg/dL, LDL cholesterol 140HDL cholesterol 42 mg/dLOther tests
normalCase Study 4
-
Weight and lifestyle historyNormal weight as child Progressive
weight gain after college exacerbated after having children in late
20sPreviously on intermittent diets with up to 20 lb. weight loss,
but invariable weight regainEats mostly home-prepared foodLittle or
no snacking, but eats meals irregularlySingle mother of 2
teenagers, with steady boyfriendWorks as nursing assistant on
evening and night shiftWalks extensively at work; no structured
exerciseCase Study 4
-
Case Study 4 - Question 1What treatment would you initially
recommend for this patient?1.Broad-based diet and lifestyle
counseling2.Implementation of moderate structured exercise
regimen3.Cooking classes4.Change jobs5.Initiate pharmacotherapy for
obesity46 FBMI 30.7Central distributionPre-DMHTNDyslipidemiaGERD
Joint painObesity onset 20sFailed dietsHome-cookerIrregular
eaterWalks a lotNight shift workerStressful life
-
Clinical progressModest, regular, aerobic exercise program
initiated and maintainedAt follow-up 2 months later, her weight was
down 6 lbs. to 184 lbs. (BMI 29.7)Case Study 4
-
You recommend that she continue the exercise program.What else
would you recommend now?Laud her success and encourage continuing a
healthy lifestyleRefer to exercise trainer to help with
exerciseEncourage a more regular eating patternSuggest that she
change to day shiftInitiate pharmacotherapy for obesityCase Study 4
Question 2
-
Clinical progressContinued regular exercise programStopped
grazing and began eating on regular scheduleChange in eating
schedule resulted in stabilization of sleep patterns as wellAt
follow-up three months later, her weight was down 8 more lbs. (14
lbs. weight loss total ), to 176 lbs. (BMI 28.4)She describes
increased energy and improved self-esteemCase Study 4
-
What would you recommend now?Encourage a healthy diet and
reassess HbA1cRefer to dietitian for nutritional managementInitiate
pharmacotherapy for obesityRecommend bariatric surgical evaluation
for type 2 diabetesRefer to plastic surgeon for liposuctionCase
Study 4 Question 3
-
Summary and Vision Statement
Near Term Challenges and Potential Strategies for Optimizing
Obesity Management in the Primary Care SettingInvestigations
Stratification Front Line Clinical Applications
-
SummaryObesity is a chronic physiologically controlled disease
that requires chronic treatmentMust be approached like other
chronic diseasesYes, there are still many barriers and challenges
to overcome with the management of obesity But there are also many
opportunitiesAwareness and education are critical!Lifestyle
modification is at the core of all our therapeutic optionsWe have
good pharmacotherapies and new agents on the horizon yet these are
underusedWe must use all of the tools at our disposition
-
SummaryReasons Why You Should Treat Overweight-ObesityExcess
adiposity adversely impacts healthObesity is a medical condition
with a physiologic and behavioral component like many other chronic
medical conditions we routinely treat on an ongoing basis in
primary care Our patients are asking for helpIf you dont, then who
will?
-
Questions and AnswersInvestigations Stratification Front Line
Clinical Applications
-
*******Etiology of Obesity
Obesity occurs when the bodys energy intake is out of balance
with its expenditure over an extended period.
The balance can be upset either by increased intake (eg, through
a high-fat, high-calorie diet) or decreased expenditure (eg,
through a sedentary lifestyle). A genetic predisposition to obesity
accelerates the process.
Treating obesity involves shifting the balance so that
expenditure exceeds intake.
**QNEXA_Core_06-16-10_v03_NO_HIDDEN.ppt*QNEXA*Between diet and
exercise and the current pharmacotherapy on one hand, and bariatric
surgery on the otherWe need more treatments to fill the treatment
gap, treat people in whom surgery is not indicatedIn hypertension
we have 100 medications in 9 categories,
**This table lists the medications approved by the United States
Food and Drug Administration (FDA) for the treatment of obesity;
only sibutramine (Meridia) and orlistat (Xenical) have been
approved for long-term use. All the approved medications act as
anorexiants, with the exception of orlistat, which blocks the
absorption of dietary fat. Anorexiants increase satiation (level of
fullness, which regulates the amount of food consumed during a
meal) or satiety (level of fullness after a meal, which determines
frequency of eating), or both. Although approved by the FDA for
short-term use, methamphetamine and benzphetamine are addictive and
should be avoided. Three anorexiant medications have been removed
from the marketplace because of increased risks of either valvular
heart disease (fenfluramine and dexfenfluramine) [1] or hemorrhagic
stroke (phenylpropanolamine) [2] associated with their use.
References1. Khan MA et al. The prevalence of cardiac valvular
insufficiency assessed by transthoracic echocardiography in obese
patients treated with appetite-suppressant drugs. N Engl J Med.
1998;339:713-718.2. Kernan WN et al. Phenylpropanolamine and the
risk of hemorrhagic stroke. N Engl J Med. 2000;343:1826-1832.
******Taken together, data from more than 20,000 echoes in
nearly 7500 patients show that lorcaserin did not increase the risk
of valvulopathy above a pre-specified level, and did not
meaningfully affect individual valve regurgitant scores.
[PAUSE]Lets move now to the evaluation of possible CNS
effects.**Confidential Draft - For Discussion Purposes
Only***CP1074317 Hayes, SAU8-15-2002 ****