Embed Size (px)
Citation preview


Investing in SightStrategic Interventions to
Prevent Vision Loss in Australia
Contents
Executive summary 5Background 9
1. Costing the interventions 131.1 General methodology and parameters 131.2 Prevalence and population data 141.3 Health costs and health cost inflation 161.4 Indirect costs and loss of well-being 171.5 Treatment effectiveness and compliance 182. Awareness, detection and early intervention 212.1 Promote regular vision testing 212.1.1 Two-year eye exams for the elderly 232.1.2 Two-year eye exams for Aboriginal and Torres Strait Islander people 252.1.3 Two-year eye exams for those with a family history of glaucoma 262.1.4 Two-year eye exams for people with diabetes 272.1.5 Five-year eye exams for ‘normal risk’ Australians aged 40 or over 282.2 Promote the cessation of smoking 292.3 Promote the use of sunglasses/protective eye-wear 322.4 Promote low vision rehabilitation services 342.5 Promote the prevention of eye injuries 372.6 Increase community awareness of vision care 393. Models of treatment and care 413.1 Reduce cataract surgery waiting lists 413.2 Improve access to subsidised spectacle programs 423.3 Sustainable funding for retinal photography 453.4 Sustainable funding for cost-effective AMD therapies 473.5 Improve access for the disadvantaged 484. Other interventions 514.1 Support eye research and development and its prioritisation 514.2 Professional workforce implications 544.2.1 Impacts of the interventions on prevalence of vision impairment 554.2.2 Calculations of workforce requirements 57
List of abbreviations 59References 61Appendix A – Summary of workshop agenda and participants 64Summary of workshop agenda and participants 66Workshop outcomes 67Appendix B – International research agenda 71Eye Research Australia and Access Economics 79
1Investing in Sight

2 Investing in Sight
Tables
Table I Eye care intervention package, costs, benefits and cost-effectiveness 6Table II Eye care interventions, costs, benefits and cost effectiveness analysis,
first year and lifetime 8Table III Initial list of interventions from Clear Insight report 10Table 1-1 Prevalence rates for vision impairment (<6/12), by age and condition 15Table 1-2 Proportion of mild, moderate and severe vision impairment, by condition 15Table 1-3 Life expectancies used in modelling (Years) 15Table 1-4 Estimated health costs per case, PV, 2005-06 to 2007-08 16Table 1-5 Estimated indirect costs per case, by type, PV, 2005-06 to 2007-08 17Table 1-6 Disability weights, future discounted, by condition 17Table 1-7 Financial conversion parameters: VSL, VLY and discount rate 17Table 1-8 Treatment effectiveness and compliance, by condition 18Table 2-1 Population (%) having eye checks, 2 and 5 years, by age group 22Table 2-2 Summary of eye exam legislation by State/Territory 23Table 2-3 Eye exams, elderly, health treatment costs by disease 24Table 2-4 Eye exams, elderly, cost effectiveness analysis, first 3 years
and lifetime 24Table 2-5 Eye exams, Aboriginal and Torres Strait Islanders,
cost effectiveness analysis, first 3 years and lifetime 25Table 2-6 Eye exams, glaucoma family history, cost effectiveness analysis,
first 3 years and lifetime 26Table 2-7 Eye exams, diabetes, cost effectiveness analysis, first 3 years
and lifetime 27Table 2-8 Five-yearly eye exams, ‘normal’ risk, cost effectiveness analysis,
first 3 years and lifetime 28Table 2-9 Summary of cost effectiveness analysis of 5-yearly eye examinations,
$m, $/QALY 28Table 2-10 Modelled results of total benefits of Quit smoking program 30Table 2-11 Benefits (PV) from Quit smoking program, AMD and cataract 31Table 2-12 Quit smoking, cost effectiveness analysis summary,
first 3 years and lifetime 31Table 2-13 SunSmart, cost effectiveness analysis summary,
first 3 years and lifetime 32Table 2-14 Cost effectiveness analysis calculations for SunSmart
intervention, to 2100 33Table 2-15 Low vision services, cost effectiveness analysis summary,
first 3 years and lifetime 36Table 2-16 Vision loss at time of trauma, and ongoing 38Table 2-17 Ocular trauma, cost effectiveness analysis summary,
first 3 years and lifetime 38Table 2-18 General awareness campaign, cost effectiveness
analysis summary, first 3 years and lifetime 39Table 2-19 Summary of net benefits, Group 1 and General awareness 40

3Investing in Sight
Figures
Table 3-1 Cataract surgery, cost effectiveness analysis summary,first 3 years and lifetime 41
Table 3-2 Subsidised spectacles, cost effectiveness analysis summary,first 3 years and lifetime 44
Table 3-3 Retinal photography, cost effectiveness analysis summary,first 3 years and lifetime 46
Table 3-4 Indigenous eye care, cost effectiveness analysis summary,first 3 years and lifetime 50
Table 4-1 Comparison of research and development expenditureby disease, 2000-01 ($’000) 51
Table 4-2 Research and development, new expenditure required to bring eye research expenditure to the national average 52
Table 4-3 Research and development, cost effectiveness analysis summary,first 3 years and lifetime 52
Table 4-4 Reduced cases of vision impairment from the modelledinterventions, 2006-2024 56
Table 4-5 Workforce implications for interventions, ophthalmologistsand optometrists, 2005-06 58
Table A-1 Workshop participants 66
Figures
Figure 1-1 Vision impairment by cause in over-40s, Australia, 2004 (<6/12 visionand/or visual field of <20o or homonymous hemianopia) 14
Figure 1-2 Blindness by cause in over-40s, Australia, 2004 (<6/60 vision and/or avisual field of <10o) 14
Figure 1-3 Composition of total costs, vision disorders, 2004 from Clear Insight 16Figure 4-1 Comparison of vision impairment prevalence projections,
with and without policy interventions, 2004-2024 55Figure A-1 Workshop agenda 65

4 Investing in Sight

5Investing in Sight
This analysis reveals that, if eye care interventions costing around $190m in2005-06 were implemented (10% of the direct health costs of vision impair-ment), net financial savings of over $650m could be realised. Moreover, 11%of the burden of vision impairment could be averted in the first year, equiva-lent to additional well-being of over 4,500 DALYs (worth over $700m), subjectto relieving workforce supply constraints.
Clear Insight- The Economic Impact and Cost of Vision Loss in Australia (AccessEconomics, 2004), identified the extent and cost of vision impairment includingblindness in Australia – $9.85bn in 2004, affecting nearly half a million Australians.
This companion report has developed, in consultation with key stakeholders, a costedplatform of strategic policy interventions to eradicate preventable blindness andvision impairment through early detection, prevention, rehabilitation, education andresearch.
• The total cost of the package in 2005-06 is $188.8m ($186.4m if certain eyeexaminations are limited to people aged over 50 rather than those aged over 40).
• The net financial benefits in the first year would be negative, but would becomepositive in 2006-07 – saving $1-2m in that year. Over the lifetime of the popula-tions impacted by the interventions, these financial savings would total over$650m in present value terms.
- Financial savings are derived from direct health benefits and indirect financialbenefits such as reduced need for care and low vision devices, and enhancedcapacity to work.
- While the upfront expenditure is lower if screening is limited to those over 50years, the net benefits and cost-effectiveness are poorer, since the eye exami-nations are cost-saving for high risk Australians aged 40-49.
• Quality of life gains are considerable – over 4,500 DALYs in the first year (worthover $700m accumulating to $7.7bn over the lifetime of the populations), savingsome 11% of the loss of well-being from vision impairment and blindnessnationally (Table 1-1).
- The term ‘loss of well-being’ is used throughout this report instead of the well-defined concept in health economics, ‘burden of disease’ as measured bydisability adjusted life years (DALYs). It measures the suffering and prematuredeath from a disease or injury and does not imply that people experiencingdisease or injury are a burden on society.
Executive summary
The cost of visionimpairment andblindness inAustralia was$9.85bn in 2004.
Eye care interventionscosting around$190m in 2005-06 wouldgive lifetimedirect netfinancial savingsof over $650m.

6 Investing in Sight
Savings arederived fromdirect health
benefits and fromindirect financialbenefits such as
reduced need forcare and low
vision devices,and enhanced
capacity to work.
Quality of lifegains are
considerable –nearly 5,000
DALYs.
Executive summary
Table I: Eye care intervention package, costs, benefits and cost-effectiveness
Cost
Total Net DALYs DALYs effectiveness
Costs $m Benefit $m Saved as $m* Expressed $/QALY
Scenario 1: With eye examinations for those aged 40 years and older
2005-06 188.8 -25.7 4,600 748 5,591
2006-07 116.9 2.3 3,069 499 cost-saving
2007-08 113.6 1.2 2,969 483 cost-saving
Lifetime 1,620.3 661.8 47,576 7,734 cost-saving
Scenario 2: With eye examinations for those aged 50 years and older
2005-06 186.4 -26.8 4,511 733 5,934
2006-07 114.6 1.3 2,985 485 cost-saving
2007-08 111.3 0.3 2,890 470 cost-saving
Lifetime 1,572.5 652.4 47,083 7,654 cost-saving
* Converted using the value of a life year = $162,561. Note: “Cost-saving” indicatesthat net benefits are positive so DALYs do not have to be ‘purchased’. All amountsexpressed as present values (2005-06).
The intervention package was agreed through a process of consultation amongststakeholders from within the eye care community, through a broad-basedconsultative workshop in Melbourne in January 2005 and through inputs into this report.The package includes four groups of actions (Table II).
• A major campaign targeting awareness, detection and prevention (total cost,including health system impacts of $90.0m in 2005-06) through:
- regular vision testing, particularly for high risk groups such as the elderly,people with diabetes, Aboriginal and Torres Strait Islander people and peoplewith a family history of glaucoma;
- reducing risk factors for cataract and age-related macular degeneration –smoking and exposure to UV light, through linking with Quit and SunSmart;
- preventing eye injuries; and- enhancing access to low vision services.
• Enhancing models of treatment and care (total cost, including health systemimpacts of $79.0m in 2005-06) for people with vision impairment through:
- reducing cataract surgery queues by outsourcing to the private sector orincreasing public sector resources;
- improving access to subsidised spectacle programs across Australia;- providing funding for retinal photography (for example through an MBS
item number); and- improve access to eye health services for Australian and Torres Strait
Islanders through fly-in services by eye care professionals.

7Investing in Sight
• Supporting eye research and development (total cost of $19.7m in 2005-06)and developing a process to prioritise and increase funding; and
• Addressing workforce and training constraints in the short and longer term- the interventions would require a workforce equivalent of 113 FTE
ophthalmologists and 137 FTE optometrists in 2005-06;- this potential supply constraint may need to be creatively addressed through a
combination approach of increasing training conduits, importing skills, andsharing workloads better between eye care professionals and other healthworkers – e.g., training more nurses in retinal photography, using moreoptometrists and Aboriginal Health Workers for eye examinations.
This report underscores that addressing preventable and treatable visionimpairment in Australia is not just cost effective, but cost-saving over thelonger term.• Indeed, highly cost-effective options such as increasing access to the subsidised
spectacle program could cross-subsidise other initiatives, such as the fly-in servicefor indigenous eye care, that are paramount on the basis of equity, but are bothcostly and less cost-effective.
At $190m in 2005-06, it represents an investment of just 0.23% of total healthexpenditure and 9.9% of health spending on vision disorders ($1.9bn) – aninsightful investment for the current half million and those future Australianswho would otherwise live with vision impairment and blindness.
Executive summary
Addressingpreventable andtreatable visionimpairment inAustralia is notjust cost-effective,but cost-savingover the longerterm.
A committmentof $190m, just0.23% of totalhealthexpenditure, or9.9% of healthspending onvision disorders,would be aremarkablyinsightfulinvestment.

8 Investing in Sight
Executive summary
Table II: Eye care interventions, costs, benefits and cost effectiveness analysis, first year and
lifetime
Intervention Total Net $/QALY Total Net $/QALY
Cost ($m) Benefit ($m) cost ($m)benefit ($m)
Group 1: Awareness, Detection and Prevention - Total costs 2005-06 - $188.8m
1.1.1 Exams 2005-06 59.9 -7.3 5,068
Elderly Lifetime 473.4 -102.7 9,641
40-74 50-74
1.1.2 2005-06 2.0 1.1 cost-saving 0.9 0.7 cost-saving
Indigenous Lifetime 28.7 9.5 cost-saving 10.8 5.2 cost-saving
1.1.3 2005-06 0.5 0.2 cost-saving 0.3 0.2 cost-saving
Glaucoma Lifetime 10.4 1.3 cost-saving 5.5 1.5 cost-saving
1.1.4 2005-06 11.3 4.4 cost-saving 9.8 5.0 cost-saving
Diabetes Lifetime 221.0 12.9 cost-saving 167.6 27.9 cost-saving
1.1.5 2005-06 2.1 0.7 cost-saving 1.0 0.3 cost-saving
5-yr exams Lifetime 41.3 4.4 cost-saving 16.2 2.4 cost-saving
1.2 2005-06 3.7 -3.6 2,860,384
Smoking Lifetime 3.7 39.1 cost-saving
1.3 2005-06 0.9 -0.9 infinite
SunSmart Lifetime 0.9 96.6 cost-saving
1.4 2005-06 9.1 14.4 cost-saving
Low vision Lifetime 61.8 120.9 cost-saving
1.5 2005-06 0.9 -0.8 5,172,295
Eye trauma Lifetime 0.9 -0.1 46,342
1.6 General 2005-06 2.0 -1.9 16,667 2.0 -2.7 18,690
Awareness Lifetime 6.1 -1.8 1,297 6.1 2.1 3,871
Group 2: Models of Treatment and Care - Total Costs 2005-06 - $79.0m
2.1 Cataract 2005-06 63.0 -23.4 16,280
Queues Lifetime 63.0 -23.4 16,280
2.2 Subsidised 2005-06 3.7 28.1 Cost-saving
spectacles Lifetime 71.3 500.8 Cost-saving
2.3 DR photo- 2005-06 -3.1 3.1 Cost-saving
graphy item no. Lifetime -75.3 75.3 Cost-saving
2.4 2005-06 na na na
AMD Lifetime na na na
2.5 2005-06 15.4 -15.4 undefined
Indigenous Lifetime 257.6 -257.6 undefined
Group 3: Research and Development - Total costs 2005-06 - $19.7m
3.1 Research and 2005-06 19.7 -19.7 infinite
development Lifetime 463.9 257.4 Cost-saving
Group 4: Professional Education and Workforce - No additional costs
4.1 2005-06 na na na
Workforce Lifetime na na na
Note: All amounts expressed as present values (2005-06).

9Investing in Sight
Access Economics Pty Limited was commissioned by Eye Research Australia to identifyand cost a package of strategic policy interventions that would cost-effectively enhanceprevention and treatment of vision impairment, including blindness, in Australia. Theinterventions were to be based on areas identified in our earlier report Clear Insight: TheEconomic Impact and Cost of Vision Loss in Australia (Access Economics, 2004). Assuch, this report forms a companion report to that earlier document.
AimThe aim of the project was to formulate, in consultation with key stakeholders, a costedplatform of strategic policy interventions that would provide a comprehensiveassessment of additional spending required, and where it might best be directed, toeradicate preventable blindness/vision impairment and its impact through earlydetection, prevention, rehabilitation, education and research.
Methodology(1) Identifying the interventionsAn initial list of interventions was drawn from Clear Insight, covering a spectrum ofdiseases of the eye and adnexa including cataract, diabetic retinopathy, glaucoma, age-related macular degeneration, refractive error and other visual disturbances (Table 1-3).From this rather lengthy list, priorities were established in consultation with EyeResearch Australia and stakeholders, through a workshop in Melbourne, Australia on 21January 2005 facilitated by Access Economics. The aim of the workshop was todevelop a consolidated list of interventions, including specification of target populationsin each case and detail of the nature of the desired intervention. Historical cost-effectiveness analysis from the Australian and international literature edified theselection of priorities from the list, as did other considerations such as equity (e.g.provision in rural areas) and ethnicity or racial group (e.g. provision of interventions toAboriginal and Torres Strait Islander communities based on need). The workshopparticipants and outcomes are summarised in Appendix A.
(2) Costing the interventionsModelling the interventions involved consideration of the delivery mechanism for each,the estimated impact effectiveness in reaching the target population, as well as detailedanalysis of immediate and secondary costs and benefits. For example, screeningservices that identify otherwise untreated cases result not only in the cost of thescreening but also the additional cost of the recommended treatment(s) over varyingtime frames and with varying degrees of effectiveness in reducing vision loss, thussaving some indirect costs and loss of well-being due to vision impairment. These werestrongly linked to those identified in Clear Insight – direct, indirect and the ‘intangible’aspects of improved well-being. Net impacts were summarised for 2005-06, 2006-07,2007-08 and over the ‘lifetime’ of the impacts. Pathways are explained in detail inChapters 1 through 4.
Background
A list ofinterventions wasestablished inconsultation withEye ResearchAustralia and eyecare communitystakeholders.
Modellinginvolvedconsideration ofthe deliverymechanism, itsestimated impacteffectiveness ofimmediate andsecondary costsand benefits.

10 Investing in Sight
Background
Table III: Initial list of interventions from Clear Insight report
Cataract
• promote protective behaviour: stop smoking and reduce ocular UV exposure;
• detect those with unoperated cataract with simple aged-care vision tests;
• improve efficiency and capacity of cataract surgery services; and
• have Australians test their vision on a regular basis (every 5 years).
Diabetic retinopathy
• promote awareness amongst those with diabetes of the need for regular eye examinations;
• involve all members of the diabetes management team in promoting eye examinations every
two years;
• update training for eye care professionals so that patient management follows
clinical practice guidelines;
• and develop, evaluate and report sustainable local and regional models of screening.
Glaucoma
• promote community awareness about the family links for glaucoma;
• have regular eye examinations for those with a family history of glaucoma and those over the
age of 50;
• and seek better ways of treating glaucoma and promoting clinical practice guidelines.
Macular degeneration
• encourage cessation of smoking;
• support access to optimal rehabilitation for all those with vision loss;
• research to confirm the genetic basis of AMD; and
• research to develop and evaluate new treatment strategies.
Refractive error
• have Australians test their vision on a regular basis (every 5 years);
• have elderly Australians vision-tested as part of aged care assessments;
• establish appropriate referral pathways for those detected with poor vision; and
• improve access to subsidised spectacle programs.
General
• increase community awareness of the importance of eye health and vision care through:
- programs to encourage routine vision testing at least every five years and every two
years for high risk groups,
- promotion of regular use of sunglasses and protective eye wear to reduce eye injury,
UV exposure and radiation e.g. linked to SunSmart,
- promotion of non-smoking to prevent age-related macular degeneration and cataracts
e.g. linked to Quit,
- protection from eye injuries in rural areas and at home,
• coordinate and fund prevention, education, early intervention and rehabilitation to reduce the
impact of vision loss,
• screening for high risk groups, including those with diabetes, a family history of eye disease
and Aboriginal and Torres Strait Islander people,

Table III continued
General (continued)
• vision testing for older Australians as a part of extended aged care assessment by GPs and
by Aged Care Assessment Teams,
• improved access to services for specific disadvantaged groups, such as those from cultural
and linguistically diverse backgrounds,
• education of the public of the importance of prevention, early intervention, rehabilitation and
education programs,
• improved access and coverage to low cost spectacle services across Australia by
altering eligibility and reducing waiting lists,
• increased awareness of services, roles and responsibilities among service providers, and
• increased awareness and effective referral pathways to eye health and rehabilitation services.
In some cases as expected, data inadequacies prevented the definitive modelling ofcertain aspects of intervention impacts. In these cases ‘best estimates’ are providedtogether with indicative scenario analysis. If interventions are implemented in Australia,evaluation will be important to compare actual results with those modelled.
(3) The way forwardThe Executive Summary draws together the threads from the analysis, providingconclusions and recommendations for a platform of proposals and the possible phasingof their introduction. Key themes of the report are the importance of early intervention,treatment and priority-driven research in preventing future loss of well-being from visionimpairment and promoting wellness.
The draft report was circulated to a reference group from within the Australian eye carecommunity for inputs prior to finalisation. The final report thus represents a stronglyendorsed position from within the Australian eye care community, of recommendedstrategic interventions that could assist in continuing to promote world best practice ineye care and improve the quality of life for the half million Australians who currently livewith vision impairment and its impacts.
11Investing in Sight
Background
This reportprovides astronglyendorsedposition fromwithin theAustralian eyecare communityof recommendedstrategicinterventions.

12 Investing in Sight

13Investing in Sight
1. Costing the Interventions1.1 General methodology and parameters
In consultation with key stakeholders, the order of interventions was consolidated wherethere was overlap. These modifications are explained in the rest of the chapters as theyarise and the final consolidated list of interventions is presented below.
Group 1: Awareness, detection and prevention• 1.1 Promote regular vision testing (through multiple pathways)
-1.1.1 Elderly, 75+ years (2 year)- 1.1.2 Aboriginal and Torres Strait Islander people 40/50-74 years (2 year)-1.1.3 Family history of glaucoma 40/50-74 years (2 year)-1.1.4 Diabetes 10-74 years (2 year)-1.1.5 General population, 40/50-74 years, (5 year)
• 1.2 Promote the cessation of smoking (with QUIT)• 1.3 Promote the use of sunglasses/protective eye-wear (with SunSmart)• 1.4 Promote education and encourage access to low vision rehabilitation services• 1.5 Promote the prevention of eye injuries• 1.6 Increase community awareness of the importance of vision care
Group 2: Models of treatment and care• 2.1 Reduce cataract surgery waiting lists (through greater capacity/efficiency)• 2.2 Improve access to subsidised spectacle programs across Australia• 2.3 Sustainable funding for retinal photography (MBS item number)• 2.4 Sustainable funding for cost-effective therapies for AMD• 2.5 Improve access to eye health services for specific disadvantaged groups
Group 3: Research and development• 3.1 Support eye research and development and develop a process to prioritise and
increase funding
Group 4: Professional education and workforce• 4.1 Provide for the workforce and training implications of other initiatives
A number of issues common to many or most interventions are described in the rest ofSection 1.1.
Key themes arethe importanceof earlyintervention,treatment andpriority drivenresearch inpreventing futureloss of well-beingfrom visionimpairment.

14 Investing in Sight
1.2 Prevalence and population data
Prevalence rates for vision impairment relating to eye disorders were calculated in ClearInsight (Access Economics, 2004) based on epidemiological data from the MelbourneVisual Impairment Project and the Blue Mountains Eye Study. Definitions of presentingvision impairment and blindness are:
• Blindness: worse than 6/60 vision and/or a visual field of <10o in the better eye;• Vision impairment: worse than 6/12 vision and/or visual field <20o or homonymous
hemianopia in the better eye.
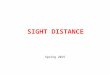
There were over 480,000 Australians aged over 40 with vision impairment in 2004, 5.4%of the population, with prevalence increasing with age. Over 50,000 of theseAustralians (0.57% of the population) are legally blind. The ‘big five’ causes of visionimpairment in Australia are: refractive error (RE); cataract; age-related maculardegeneration (AMD); glaucoma and diabetic retinopathy (DR). Together these accountfor 91% of vision impairment and nearly 88% of blindness, with AMD accounting foralmost half the cases of blindness. Some 80% of vision impairment is avoidable ortreatable. Other eye conditions, such as neuro-ophthalmic conditions, retinitispigmentosa or conjunctivitis have varying degrees of prevalence, visual impacts, andhealth system and other cost impacts (Figure 1-1, Figure 1-2). In 2005, the number ofAustralians with vision impairment is estimated to exceed half a million (503,914).
Figure 1-1: Vision impairment by cause in over-40s, Australia, 2004 (< 6/12 vision and/or visual
field <20o or homonymous hemianopia)
AMD 48,319
Glaucoma 13,741
Cataract 68,657
Diabetic Retinopathy7,758Other Retinal 15,891
Refractive Error 296,742
Total 480,257
Neuro-ophthalmic 8,662 Other 20,490
62%
10%3%
14%
4%
2%
2%3%
14%
12%
10%48%
4%8%
3%1.5%
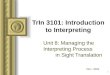
Neuro-ophthalmic 1,404 Retinitis Pigmentosa 769
Refractive Error 1,882Other 4,370
Glaucoma 6,901
Cataract 6,111
Diabetes andOther Retinal 4,908
Total 50,548
AMD24,204
Figure 1-2: Blindness by cause in Over-40s, Australia, 2004 (< 6/60 vision and/or a visual field
of <10o)
Of the 480,000Australians aged
over 40 withvision impairment
in 2004, 50,000of these arelegally blind.

15Investing in Sight
Prevalence and population data
For this report, the age-specific prevalence rates by disease have been applied to ABSmid-case (Series B) population projections (ABS, 2003), adjusted to reflect revisions inDecember 2004 to actual population numbers, in order to estimate future prevalence ofthe various conditions in terms of number of people. The proportion of those withvision impairment that is mild, moderate and severe was also calculated, as shown inTable 1-2, by disease, based on MVIP data, with ‘other’ calculated as the prevalence-weighted average of the ‘big five’.
A key demographic parameter for the lifetime modelling in particular, was lifeexpectancy, which varied by age, gender and ethnicity, as per Table 1-3.
Table 1-1: Prevalence rates for vision impairment (<6/12), by age and condition
Cataract DR Glaucoma AMD RE Other Total
40-49 0.0% 0.0% 0.0% 0.0% 0.5% 0.2% 0.6%
50-59 0.0% 0.0% 0.0% 0.0% 1.8% 0.3% 2.3%
60-69 0.1% 0.2% 0.1% 0.0% 3.9% 0.3% 4.7%
70-79 1.4% 0.1% 0.3% 0.8% 7.8% 0.8% 11.1%
80-89 6.6% 0.5% 1.4% 4.6% 13.0% 1.9% 28.7%
90+ 15.2% 0.6% 1.2% 13.0% 7.9% 2.4% 40.3%
Source: Combined data from the Melbourne Visual Impairment Project and Blue Mountains Eye Study.
Table 1-2: Proportion of mild, moderate and severe vision impairment, by condition
Cataract DR Glaucoma AMD RE Other Total
Mild (6/12 to 6/18) 60.2% 30.6% 5.1% 23.4% 83.4% 37.1% 65.8%
Moderate (<6/18 to 6/60) 26.7% 47.8% 40.8% 38.4% 14.6% 41.1% 23.5%
Severe (>6/60) 13.0% 21.6% 54.2% 38.3% 2.0% 21.9% 10.6%
Source: Melbourne Visual Impairment Project, specially provided byEye Research Australia.
Table 1-3: Life expectancies used in modelling (Years)
Life Expectancy Males Females Persons
10-74 (general) 41.2 45.4 43.3
40-74 (general) 26.6 30.6 28.6
50-74 (general) 21.2 25.0 23.1
Aboriginal and Torres Strait Islander, 40-74 17.2 20.2 18.7
Aboriginal and Torres Strait Islander, 50-74 12.6 14.9 13.8
75+ 7.8 9.0 8.5
Source: ABS (2004)
Five conditionscause threequarters of thevision lossin Australia.

16 Investing in Sight
1.3 Health costs and health cost inflation
Direct healthcosts in 2004 for
all disorders ofthe eye and
adnexa were over$1.8 billion.
Direct health costs in 2004 for all disorders of the eye and adnexa were over $1.8 billion(Clear Insight Access Economics, 2004) – see Figure 1-3.
For this project, average costs per case (Table 1-4) were estimated by:• dividing the health system expenditure estimated for 2004 by the prevalence for
that year to calculate cost per case in 2004;- for AMD, an additional $30m was included to allow for the photodynamic
therapy (PDT) funded in the 2002/03 Federal Budget that was conservativelyexcluded in Access Economics (2004);
• setting the categories for DR and ‘other’ to the average overall, since there wereanomalies in these data due to the following factors;- the prevalence data reflect vision impairment, whereas the cost data are disease
specific (so highly prevalent conditions like conjunctivitis skewed the costresults, even thought this rarely causes vision loss); and
- unstable prevalence data for DR, which led to unacceptable standard error andthus unusable;
• projecting to 2005-06 based on health cost inflation of 2.9% per annum for 1.5years from CY2004 to FY2005-06; 2.9% was also used to project after 2005-06;- 2.9% is the average health cost inflation over the period to 1992-93 to 2002-03
(AIHW, 2004); and- Expressing this as a present value (PV) so comparison can be made with future
benefits streams, by discounting by the bond rate (5.8%pa).
Table 1-4: Estimated health costs per case, PV, 2005-06 to 2007-08
Cataract DR Glaucoma AMD* RE Other
2005-06 4,965 3,965 2,193 1,067 919 3,965
2006-07 4,825 3,853 2,131 1,037 893 3,853
2007-08 4,689 3,745 2,071 1,007 868 3,745
*AMD includes an allowance for the estimated cost of Visudyne therapy
Figure 1-3: Composition of total costs, vision disorders, 2004 from Clear Insight
Total $9.85bn Hospital $692m
Loss ofWell-being $4,818m
Aids, other indirect $371m
Other health costs $726m
Out-of-hospital medical $406m
Transfer DWLs $208m
Carers $845m
4%7%
4%
9%49%
7%
Lost income $1,781m
18%
2%
DirectCosts$1,824m
IndirectCosts$3,224m
}
}

17Investing in Sight
1.4 Indirect costs and loss of well-being
Vision impairmentdecreases thequality andlength of life, andincreasesmorbidity andmortality.
The burden ofdisease wasestimated asover 40,000disabilityadjusted lifeyears.
Visual impairment decreases the quality and length of life. It is associated with othermorbidity and mortality through falls, hip fractures, other accidents and depression.Employment rates are lower for people with vision impairment and there is alsoincreased need for care, aids and devices, social isolation and other impacts. Indirectcosts were estimated as $3.2 billion in 2004 (Access Economics, 2004).For this project, average costs per case were estimated by dividing the cost components from Access Economics (2004) by prevalence and multiplying by averageconsumer price inflation (1.9% per annum) to project to 2005-06 and beyond,discounting by the bond rate to express as a present value (Table 1-5).
The loss of well-being was estimated as over 40,000 disability adjusted life years(DALYs) in 2004 (Access Economics, 2004), including associated mortality.For this project, DALYs per case are estimated as disability weights by condition fromMathers et al (1999), who attribute disability weights to vision impairment of:
• 0.02 for mild vision loss;• 0.17 for moderate vision loss; and• 0.43 for severe vision loss.
Using these weights together with the proportions of vision impairment that are mild,moderate and severe from Table 1-2 above, generates disability weights for eachcondition as shown in Table 1-6, for 2005-06. These need to be discounted in thefuture by the discount rate for healthy life (3.3%). Conversions to financial measures arebased on the value of a life year (VLY) of $162,561, calculated from the value of astatistical life (VSL) and the discount rate as per Table 1-7. This methodology isexplained in detail in Access Economics (2004).
Table 1-5: Estimated indirect costs per case, by type, PV, 2005-06 to 2007-08
Total Indirect Production Premature Carer Other indirect
Costs Losses Mortality Costs Costs
2005-06 $6,874 $3,815 $11 $1,809 $1,239
2006-07 $6,616 $3,674 $11 $1,743 $1,193
2007-08 $6,377 $3,539 $11 $1,678 $1,149
Table 1-6: Disability weights, future discounted, by condition
Cataract DR Glaucoma AMD RE Other
2005-06 0.11 0.18 0.30 0.23 0.05 0.17
2006-07 0.11 0.18 0.30 0.23 0.05 0.17
2007-08 0.11 0.17 0.29 0.22 0.05 0.16
Table 1-7: Financial conversion parameters: VSL, VLY and discount rate
Value of a Statistical Life $3.7m
Discount Rate 3.3%
Value of a Life Year $162,561

18 Investing in Sight
1.5 Treatment effectiveness and compliance
Cataract hasbecome the mostcommon elective
operation.
Up to 98% ofsevere vision loss
from diabetescould be
prevented.
Estimating treatment effectiveness and compliance was undertaken by using applicableinternational and Australian literature together with expert opinion.
• Effectiveness is the percentage of vision loss that can be avoided through timelyclinical intervention, given current prevalence of vision impairment.
• Compliance is the percentage of people who are likely to adhere to recommendedtimely clinical intervention.
Results are summarised in Table 1-8, and the basis for each parameter is explainedafter it.
Cataract, Refractive Error and ‘Other’: For refractive error the MVIP study provideddata on the change since baseline of presenting vision acuity in the five years tofollow-up. In 95% of cases VA was still better than 6/12 at the follow-up, so theirlenses lasted the full five years or had been successfully changed in that time. The dataalso showed that compliance (those with refractive error wearing their lenses as aproportion of the total) was 99%. The other treatment effectiveness and complianceparameters were based on expert opinion from Eye Research Australiaophthalmologists in turn based on evidence from the American Academy ofOphthalmology, favouring conservative estimates. Extrapolations were used where datawere missing (AAO October 2003, www.aao.org).
Diabetic Retinopathy: Turner et al (1998) estimated the treatment effectiveness ofcontrolling blood pressure to prevent diabetic complications and found that for DR itwas effective in preventing 98% of severe DR, 50% of moderate DR and 25% of mildDR; these percentages were multiplied by the proportion of mild, moderate and severevision impairment for the lifetime parameter (43.3%). Since life expectancy at averageage of onset was 9.5 years, the proportions of vision loss at 1, 2, 3 and 5 years werecalculated as a straight line extrapolation from the lifetime estimate. Compliance of80% was based on expert opinion from Eye Research Australia ophthalmologists in turnbased on evidence from the American Academy of Ophthalmology (AAO October 2003,www.aao.org).
Table 1-8: Treatment effectiveness and compliance, by condition
Treatment effectiveness Cataract DR Glaucoma AMD RE Other
1 year 99% 95.9% 99.7% 3.8% 99.1% 50%
2 years 98% 91.8% 98.5% 3.6% 98.2% 50%
3 years 97% 87.8% 97.6% 1.6% 97.3% 50%
5 years 95% 79.6% 95.2% 2.1% 95.4% 50%
Lifetime 95% 53.0% 82.9% 2.1% 88.7% 50%
Compliance 90% 80% 67% 95% 99% 80%

19Investing in Sight
Treatment effectiveness and compliance
Half of those withglaucoma do notknow theyhave it.
Smoking is thebiggestmodifiable riskfactor for AMD.
Glaucoma: Kass et al (2002) assessed the effectiveness of (topical ocular hypertensive)medication interventions for primary open angle glaucoma through a randomised trial.Their Kaplan-Meier plot of cumulative probability of developing glaucoma at 1, 2, 3, 5and 7 years (lifetime) was used to calculate the parameters for effectiveness ofmedication. These compared well with the results of Heijl et al (2002) of reductions inintra-ocular pressure (but with no vision impairment measure), who concluded that“treatment effects were present in both older and younger patients, high and normaltension glaucoma, and eyes with less and greater visual field loss.” Similar patternswere evident in relation to surgical effectiveness in later stage glaucoma patients (vanVeldhuisen et al, 2000). Compliance parameters are based on expert opinion from EyeResearch Australia ophthalmologists in turn based on evidence from the AmericanAcademy of Ophthalmology (AAO October 2003, www.aao.org) together with Taylor etal (2002) and Stewart et al (2004).
Age-related macular degeneration: Treatment effectiveness is based on the premisethat only one third of neovascular AMD (which of itself comprises around 60% of casesof late AMD1) is treatable. Of these, laser photocoagulation (LPC) is cost effective andcan be used in approximately 15% of cases (Hopley et al, 2004). The MacularPhotocoagulation Study (MPS), a large randomised controlled multicentre study, foundthat treatment enabled a significant (we modelled 80% at 1 year and 70% at 2 years)reduction in the risk of severe visual loss in the first two years (>2/12) but fell to 20% atfive years (assumed the same as lifetime effectiveness, since life expectancy at averageage of onset is less than five years). Photodynamic therapy (PDT) for unsuccessful LPCin neovascular AMD generates a 10% vision impairment improvement for early AMDand 7.6% for late AMD (Hopley et al). Compliance of 95% is based on expert opinionfrom Eye Research Australia ophthalmologists in turn based on evidence from theAmerican Academy of Ophthalmology (AAO October 2003, www.aao.org).
1 Geographic AMD is not treatable and comprises 40% of cases.

20 Investing in Sight

21Investing in Sight
2. Awareness, detection and early intervention2.1 Promote regular vision testing
Those over 40who have had anormal examneed to be testedat least onceevery 5 years.
All Australiansshould have aneye exam if theynotice a changein vision.
In modelling, Workshop Interventions 1.4, 1.5 and 2.1 were combined together, due tosubstantial overlaps in relation to:
• type of intervention (vision testing);• populations (e.g. an elderly person may be an Aboriginal and Torres Strait Islander,
have diabetes and/or have a family history of glaucoma); and• delivery mechanisms (e.g. ACAT assessments, driver’s license tests).
The general consensus from the Workshop on this issue was the aim of providingregular eye exams, with an emphasis on Australians aged over 40 years (examinationsfor over-40’s and over-50’s were modelled). The exception to this was regular screeningfor people with diagnosed diabetes from puberty (modelled as from age 10). Regardingfrequency of exams, the focus group recommended two-year eye exams for those inhigh risk groups – the elderly, defined as 75 and over, and potentially combined withtaking a driver’s license renewal test or with and ACAT assessment (Nottle et al, 2000);Aboriginal and Torres Strait Islander people; people with diabetes mellitus; and peoplewith a family history of glaucoma. For other Australians aged over 40/50 years, whomwe shall refer to as the ‘normal risk’ group, five-year exams were recommended.Moreover, all Australians should have an eye exam if they notice a change in vision.These recommendations are in line with the clinical literature (Taylor et al, 2004).
For modelling purposes, to calculate the costs and benefits of exams in 2005-06 it isnecessary to calculate the following for each group.1. The number of people in the target population in that year, by age and gender (Nag).
2. The number of people reached by the intervention, Rag = Nag x r where r = reach ofthe intervention (expressed as a percentage).
3. The total cost of the eye exams, CE = Rag x ACE where ACE = average cost of eyeexams. The basis for ACE was a weighted averaged of two MBS item numbersdeemed by specialists as the appropriate ones to use:
• 10900, the cost of an initial eye consultation with an optometrist, which paid$60.25 in November 2004; inflating this by 2.9% (average health cost inflation) toend-2005 gave $62.00 and taking into account gap payments (assuming these add15.6% to fees based on the GP ‘gap’ average) and the average bulk-billing rate(96.8%, December 2004), the price used was $62.31;
• 104, the cost of an initial consultation with a specialist, which paid $72.60 inNovember 2004 inflated to $74.71 and adjusted to take account of non-Federalpayments with a bulk-billing rate of 26.8% gives $83.24.
• The weights were the share of optometrists (68.7%) and ophthalmologists (31.3%)respectively in seeing patients, based on Keeffe et al (2002), with the weightedaverage price being $68.86.

22 Investing in Sight
Promote regular vision testing
4. The number of people identified from the eye exams as having vision impairmentrequiring new health system treatment, who would not otherwise have been identifiedand treated, by age, gender and disease VIagd = Ragd x i where i = incidence,approximated from Taylor et al (2004) as per Table 2-1, with the distribution betweendisease as per prevalence pagd, where p = the probability for someone of thatage/gender of having a particular eye disease, based on overall prevalence.
5. The cost of additional treatment, modelled as incurred in the health care system overthe remaining lifespan for the cases of new vision impairment identified through the‘additional’ exams in the base year, multiplied by the proportion who comply withtreatment and by the average (discounted) health cost per person per annum, whichvaries by disease. The health costs in each of the first three years are also separatelyidentified (in present value terms).
6. The benefits, for those for whom the treatment is effective, assessed in terms ofquality of life (QoL), productivity and other ‘indirect’ gains from enhanced vision (lessneed for carers, aids and modifications). QoL is measured by the disability adjustedlife years (DALYs) averted, converted to a financial measure using a conservative VSL(value of a statistical life). Other indirect financial cost savings per person with visionimpairment are based on those calculated in Clear Insight. Benefits are alsomeasured over the remaining lifespan as well as identifying benefits in each of thefirst three years.
Some key data for the regularity in the population of eye examinations are derived fromMVIP and summarised in Table 2-1. For people with diabetes, the frequency of eyeexaminations is based on different data (see Section 2.1.4).
Table 2-1: Population (%) having eye checks, 2 and 5 years, by age group
Age group Test in Not Target Test in Not Target %
last 2yrs tested pa population last 5yrs tested pa population incidence
40-74 42.5% 28.7% 2,276,852 74.4% 5.1% 406,313 2.1%
50-74 45.7% 27.2% 1,337,985 81.0% 3.8% 187,019 2.4%
75+ 54.5% 22.8% 288,440 83.0% 3.4% 43,080 10.6%
Source: Keeffe et al (2002) and supplementary data request from Eye ResearchAustralia.

23Investing in Sight
Those over 75should have aneye examevery 2 years.
Some consideration was given to the definition of ‘the elderly’ for this exercise. Theconclusion was that those aged 75 years and over, in order to link with the majority ofcurrent State/Territory legislation in relation to compulsory eye exams for older peopleto renew their driving licenses. This legislation is briefly summarised in Table 2-2.
From Table 2-1, we see that 54.5% of Australians aged 75 and over had an eye test inthe last two years, so 22.8% of over-75 year olds would need to be screened each yearfor two-year tests equating to 288,440 people in the target population. The ‘reach’ ofthe intervention is assumed to be 75%, since it is deemed feasible that three quarters ofelderly people each year could all be reached through a combination of driving testlinks, ACAT assessments and the awareness/education activities costed in the generalawareness-raising intervention (1.4). Mathematically, .75N = R = 216,330, andmultiplying R by ACE ($68.86) gives screening cost of the eye exams of $14.9m in2005-06. In the following year, the other half of those unscreened would need to bescreened, in PV terms $14.5m and so on. The present value in 2005-06 dollars for thelifetime additional screening costs is $111.2m.
2.1.1 Two-year eye exam for the elderly
Table 2-2: Summary of eye exam legislation by State/Territory
State/Territory Summary of current regulation and % of those who drive
of older age groups
Australian Capital Territory Eye chart test for obtaining and renewing a licence (max of 5
years between renewals).
New South Wales Eye chart test for obtaining and renewing a licence (max of 5
years between renewals; annual medical exam mandatory for
drivers aged 80 years and over. Proportion driving increases
from 66% of those aged 16-19 to 90% of those aged 30-39
and then falls to 69% of those aged 70-79 and to 30.6% of
those aged 80 and over).
Northern Territory Eye chart test for obtaining and renewing a licence
(max of 5 years).
Queensland No eye testing required; drivers aged 75 years and over are
required to carry a current medical certificate (which covers
eye tests). Proportion driving increases from 65% of those
aged 21-24 to 96% of those aged 25-29 and then falls to 68%
of those aged 60-69 and to 34.6% of those aged 75 and over.
South Australia No eye chart tests; annual medical exam required for drivers
aged 70 years and over.
Tasmania Eye exam required for obtaining a licence; annual medical
certificate required for drivers aged 75 years and over.
Victoria Eye exam for obtaining a licence; no further requirements for
eye tests or conditions on older drivers.
Western Australia Eye chart test to obtain a licence; medical certificate required
for drivers aged 75 years and over.

24 Investing in Sight
Two yearly eyeexams for elderly
Australians arehighly
cost-effective.
Two-year eye exam for the elderly
Of those who are elderly and newly examined, the number with vision loss who were notalready being treated is estimated as 10.6% so 23,014 people are likely to be found tohave vision impairment, distributed by disease (based on prevalence by age). Multiplyingthese by compliance rates and average health treatment costs and discounting gives thePV each year and over the lifetime as shown in Table 2-3.
In terms of benefits, since the target group is elderly, productivity benefits are excluded.The gross indirect benefits for 2005-06 are $52.5m, so subtracting the cost ofexaminations ($14.9m) and health treatment ($45.0m), overall there is a net cost of $7.3m(rounded) in 2005-06 (Table 2-4). However, since 1,449 DALYs are averted, the costeffectiveness analysis shows $5,068 in 2005-06, worsening to $9,641 over the lifetime ofthe population examined (since the benefits from the effectiveness of interventionsdwindle over the lifetime but costs of treating vision impairment continue till average lifeexpectancy). Nonetheless, at each stage two-year eye exams for elderly Australiansare in the highly cost-effective range.
Table 2-3: Eye exams, elderly, health treatment costs by disease
Cataract DR Glaucoma AMD RE Other Total
People identified
with vision impairment 5,408 294 932 3,950 11,007 1,422 23,014
PV health cost
2005-06 ($m) 24.17 0.93 1.36 4.00 10.02 4.51 45.0
PV health cost
2006-07 ($m) 23.49 0.91 1.32 3.89 9.73 4.38 43.7
PV health cost
2007-08 ($m) 22.83 0.88 1.29 3.78 9.46 4.26 42.5
PV ($m) of lifetime
health treatment cost 194.5 7.5 11.0 32.2 80.6 36.3 362.2
Table 2-4: Eye exams, elderly, cost effectiveness analysis, first 3 years and lifetime
Total Costs, $m Net Benefit, $m Cost-effectiveness,
$/QALY
2005-06 59.9 -7.3 5,068
2006-07 58.2 -8.1 5,808
2007-08 56.6 -9.0 6,738
Lifetime 473.4 -102.7 9,641

25Investing in Sight
Up to $1.1 millioncould be spentpromoting eyechecks toAboriginal andTorres StraitIslander peopleand have netfinancial benefitsoverall.
ABS Cat No 3238.0 was used to estimate the population of Aboriginal and Torres StraitIslander people in 2005 aged between 40 and 74 years, and between 50 and 74 years.Those over 75 will be captured in Intervention 1.1.1 above, so are not double-countedhere. The ABS predicts a high and low series population so an average of these twoseries was used for this intervention.
It was not possible to identify the propensity of Aboriginal and Torres Strait Islanderpeople to have a two yearly eye exam so it was assumed that they may be 25% lesslikely to be examined than non-Aboriginal and Torres Strait Islander people of the sameage, and 25% more likely to have vision loss over the period (e.g. greater rates ofdiabetes, losing spectacles, etc). Similar methodology is applied as for the elderly,noting different life expectancies and this time including productivity benefits (since thisis a working age population).2 Also, the ‘impact’ parameter is only 50% for Aboriginaland Torres Strait Islander people, rather than 75% for other Australians, reflecting lesserexposure to commercial media and access to health system pathways. On current ABSdata, there are an estimated 18,860 people impacted aged 40-74 and 8,670 impactedaged 50-74, of whom an estimated 504 (40-74) and 263 (50-74) would requiretreatment.
Aboriginal and Torres Strait Islander eye checks are found to be not justcost-effective but cost-saving (see Table 2-5). Relative to screens for the elderly, thehigher cost-effectiveness largely reflects the greater proportion of refractive error beingpicked up in examinations and effectively corrected. Delivery costs are not includedsince they are covered in intervention 3.5. Indicative budgets for reaching Aboriginaland Torres Strait Islander people for eye checks could be drawn from the ‘net benefit’column – e.g. in 2005-06 up to $1.1 million could be spent promoting eye checks toAboriginal and Torres Strait Islander people and the intervention would still have netfinancial benefits overall.
2.1.2 Two-year eye exams for Aboriginal andTorres Strait Islander people
Table 2-5: Eye exams, Aboriginal and Torres Strait Islanders, cost effectiveness analysis,
first 3 years and lifetime
Total Costs, $m Net Benefit, $m Cost-effectiveness, $/QALY
40-74
2005-06 2.0 1.1 cost-saving
2006-07 1.9 1.0 cost-saving
2007-08 1.9 0.9 cost-saving
Lifetime 28.7 9.5 cost-saving
50-74
2005-06 0.9 0.7 cost-saving
2006-07 0.9 0.6 cost-saving
2007-08 0.9 0.6 cost-saving
Lifetime 10.8 5.2 cost-saving
2 The methodology imputes the same prevalence rates and treatment costs as in the general
Australian population, in the absence of better data.

26 Investing in Sight
A family historyincreases the
risk of glaucoma4 times.
The probability of having a family history of glaucoma (Pr(GF)) is equal to the probabilityof having either parent with glaucoma minus the probability of having both parents withglaucoma. The probability of having either parent with glaucoma for people aged 40-75is estimated as the prevalence of glaucoma in the population of over-40s, derived fromClear Insight age prevalence rates applied to 2005 population estimates.3 Theprobability of having glaucoma (Pr(G)) is equal to this total population proportion(0.158%).
Thus:Pr(GF) = 2 ∗ Pr(G) - Pr(G)2 = 0.316%
The number of people who have a family history of glaucoma can therefore beestimated as Pr(GF) ∗ Popn 40-74 in 2005 = 25,047 of whom 28.7% are not having two-yearly eye exams (Table 2-1). For those aged 50-74, the respective figures are 15,575in the target population of whom 27.2% need screening, in a year, who are not alreadybeing screened. The impact parameter used is 75%, and this time the 2.1% (40-74)and 2.4% (50-74) who require treatment are adjusted upwards for glaucoma only, whichis estimated as four times the risk of people without a family history of glaucoma(Access Economics, 2004). All up, 120 people aged 40-74 or 80 people aged 50-74would require treatment. Costs and net benefits are shown in Table 2-6, again withcost-saving results throughout for people with a family history of glaucoma.
2.1.3 Two-year eye exams for those with afamily history of glaucoma
Table 2-6: Eye exams, glaucoma family history, cost effectiveness analysis, first 3 years
and lifetime
Total Costs, $m Net Benefit, $m Cost-effectiveness, $/QALY
40-74
2005-06 0.5 0.2 cost-saving
2006-07 0.5 0.2 cost-saving
2007-08 0.5 0.2 cost-saving
Lifetime 10.4 1.3 cost-saving
50-74
2005-06 0.3 0.2 cost-saving
2006-07 0.3 0.1 cost-saving
2007-08 0.3 0.1 cost-saving
Lifetime 5.5 1.5 cost-saving
3 This may slightly overestimate numbers since some people with a family history of glaucoma,
whose parent(s) with glaucoma are still alive, may already be over 75 or over, but this is extremely
rare.
2.1.4 Two-year eye exams for people with Diabetes
The number of people with known diabetes was estimated by applying prevalenceshares for self-reported diabetes by age from the Australian National Health Survey

27Investing in Sight
Half of thosewith diabetesdo not havethe necessaryeye examevery 2 years.
2.1.4 Two-year eye exams for peoplewith diabetes
(ABS, 2002). This gave a total of 608,667 aged 10 or over with known diabetes ofwhom 497,442 are aged 10-74. McKay et al (2000) estimates that 50.4% of those withdiabetes have had a dilated eye exam in the last two years. Thus the estimated rate ofthose with diabetes who have missed their two-yearly eye check is 24.8% per annum(half of 49.6%). This rate was applied to estimate the number in the target populationas 123,366 aged 10-74. With impact of 75% the number of screens is substantial at92,524, with 1,468 requiring treatment. The increased risk for retinopathy among thediabetic population is calculated from the ratio of the probabilities of having eachcondition – once diabetes is known, the elevated risk for retinopathy is 14.2 times thatin the general population.
Using similar methodology as for the other population screens, Table 2-7 presents thecost-effective results for diabetic screening. The results are very sensitive to theparameters – in particular, if the parameter for those who need a screen is increasedfrom 24.8% to 28.7% and the age-specific visual loss is increased from 1.3% to 2.1%(the parameters used those with a family history of glaucoma), then more than 2,000extra DALYs would be gained over a lifetime, including hundreds in the first year.
Table 2-7: Eye exams, diabetes, cost effectiveness analysis, first 3 years and lifetime
Total Costs, $m Net Benefit, $m Cost-effectiveness, $/QALY
10-74
2005-06 8.9 -0.2 1,715
2006-07 8.6 -0.4 3,743
2007-08 8.4 -0.6 5,836
Lifetime 212.7 -57.8 27,274
2.1.5 5-Year Eye Exam for ‘Normal Risk’ Australians aged 40 or Over
This intervention aims to target the ‘general’ population who are not in a high riskcategory. The target population for five-year eye exams (i.e., the number in the normalrisk group) is the population aged 40-74 or 50-74, less those people in the high riskgroups in each4, who do not have regular five-year screens (5.1% and 3.8% per annumrespectively). Total target populations are thus 376,732 and 169,976. However, theimpact parameter is much lower for this intervention, as pathways for care are less welldefined and, as such, we have used the average impact (5.76%) of a variety of healtheducation and information interventions from a literature search. The number ofadditional Australians requiring eye screens in 2005-06 is thus estimated as 21,709 and9,795 in each of the two age-groups, of whom 464 and 209 respectively are estimatedto require treatment each year.
4 The overlap between those people under 74 who are Aboriginal and Torres Strait Islander, have a
family history of glaucoma and are known diabetics is likely to be very small so is not included in
the modelling.

28 Investing in Sight
2.1.5 Five-year eye exam for ‘normal risk’Australians aged 40 or over
Table 2-8: Five-yearly eye exams, ‘normal’ risk, cost effectiveness analysis, first 3 years and
lifetime
Total Costs, $m Net Benefit, $m Cost-effectiveness, $/QALY
40-74
2005-06 2.1 0.7 cost-saving
2006-07 2.1 0.6 cost-saving
2007-08 2.0 0.6 cost-saving
Lifetime 41.3 4.4 cost-saving
50-74
2005-06 1.0 0.3 cost-saving
2006-07 0.9 0.3 cost-saving
2007-08 0.9 0.3 cost-saving
Lifetime 16.2 2.4 cost-saving
Table 2-9: Summary of cost effectiveness analysis of 5-yearly eye examinations, $m, $/QALY
1.1.1 Elderly (75+) 1.1.4 Diabetes (10-74)
Total Net Total Net
Cost Benefit $/QALY Cost Benefit $/QALY
2005-06 59.9 -7.3 5,068 8.9 -0.2 1,715
2006-07 58.2 -8.1 5,808 8.6 -0.4 3,743
2007-08 56.6 -9.0 6,738 8.4 -0.6 5,836
Lifetime 473.4 -102.7 9,641 212.7 -57.8 27,274
40-74 50-74
Aboriginal and Torres Strait Islander
1.1.2 2005-06 2.0 1.1 cost-saving 0.9 0.7 cost-saving
2006-07 1.9 1.0 cost-saving 0.9 0.6 cost-saving
2007-08 1.9 0.9 cost-saving 0.9 0.6 cost-saving
Lifetime 28.7 9.5 cost-saving 10.8 5.2 cost-saving
Glaucoma 2005-06 0.5 0.2 cost-saving 0.3 0.2 cost-saving
1.1.3 2006-07 0.5 0.2 cost-saving 0.3 0.1 cost-saving
2007-08 0.5 0.2 cost-saving 0.3 0.1 cost-saving
Lifetime 10.4 1.3 cost-saving 5.5 1.5 cost-saving
5-yr exams 2005-06 2.1 0.7 cost-saving 1.0 0.3 cost-saving
1.1.5 2006-07 2.1 0.6 cost-saving 0.9 0.3 cost-saving
2007-08 2.0 0.6 cost-saving 0.9 0.3 cost-saving
Lifetime 41.3 4.4 cost-saving 16.2 2.4 cost-saving
Table 2-9 summarises the cost effectiveness analysis from the eye examinations – thelargest costs are incurred in two-year screens for the elderly and people with diabetes,followed by five-year exams for ‘normal risk’ Australians.
Results of the cost benefit and cost effectiveness analyses are tabulated in Table 2-8.Five-year eye screens in either the general 40-74 or 50-74 populations are alsofound to be cost-saving.
Five-yeareye screens
for ‘normal risk’Australians aged
40 or over arecost saving.

29Investing in Sight
AMD andCataract arelinked tosmoking.
2.2 Promote the cessation of smoking
This intervention was modelled on the successful National Tobacco Campaign (NTC).During a six month campaign in 1997, the NTC campaign promoted the Quit programthrough TV ads, print media, a campaign website, and a national Quit line. The NTCcampaign was extensive, with Federal contributions of $7.1 million and furthercontributions from the State governments of $1.85 million. A conservative estimate ofthe costs of running a similar campaign would put the cost at around $3.7 million (DHA,2000, p 221).
The NTC targeted Australian smokers aged 18 to 40 years. Access Economics has alsoused this target population for costing this intervention, amounting to some 2.1 millionAustralians. The Department of Health and Ageing released a research report into theeffectiveness of the NTC in April 2004. The report presented results from aquestionnaire of randomly selected individuals. It found that, following a key eye-related advertising campaign, the level of awareness about smoking leading to loss ofsight was 5% of the survey group, up from less than 1% prior to the awarenesscampaign (DHA, 2004, p9). Thus 5% is used as the modelled effectiveness of thisintervention in awareness raising, a total of 103,914 people who attempt to quitsmoking as a result of the campaign.
There are various outcomes of attempts to quit smoking . Of those who attempt toquit, 20-25% remain abstinent after 6 months, 10% after 12 months (Miller and Wood,2001, p1), and 3-5% of smokers quit for a year or longer (p14). Of people who eversmoked 50% eventually successfully quit (p1); relapse is higher for adolescents than foradults (p34), and while in the past 90% of quitters did so on their own, in the US 20-35% now use medication or some other form of assistance (p14). Moreover, unlike theeye examination interventions, where people with existing vision impairment areidentified and treated, successful attempts to quit smoking reduce population risk ofeye disease, so the future prevalence pattern is adjusted and the calculated healthsystem expenditure (averted) becomes a benefit rather than a cost.
Increased relative risk (odds ratios) for age-related macular degeneration from smokingin the literature reviewed ranges from 1.75 for early age-related maculopathy (Smith etal, 1996), to 3.2 for neovascular AMD and 3.92 for late AMD, (Smith et al, 1996), and ashigh as 5.82 for current smokers and geographic atrophy in the Blue Mountains EyeStudy (BMES) (Smith et al, 2001). For cataract the odds ratios are lower, and anAustralian estimate of 1.89 for nuclear cataract (McCarty et al, 2000), representingaround 17% of the population attributable risk for nuclear cataract. Mitchell et al (1999)estimate that smoking is responsible for around 20% of all cases of blindness inAustralians over 50.
Impacts of quitting smoking occur at various stages in the life cycle, so benefits may bedelayed. Lifetime cost effectiveness analysis would be much more positive than in theearly years, since the cost is limited to that up-front of running the campaign. Finally,there are many other positive benefits of quitting smoking – reduced risk of major

30 Investing in Sight
The next step is to separate out the benefits derived from averting cases of AMD andcataract. The same effectiveness parameter of 16% is used as above – i.e., 16% ofpeople impacted successfully quit smoking in 2005/06 relative to a control situation ofno intervention and hence no extra quitters in that year.
Promote the cessation of smoking
sources of mortality and morbidity such as cardiovascular disease, cancer and chronicobstructive pulmonary disease. Ideally these should all be captured in the analysis.Access Economics has previously developed a model to capture the impacts of quittingsmoking, taking into account these many impacts and their various lags. The modelprovides a structured tool which enhances the ability to assess the impacts of healthinterventions in terms of their flow-through effects in averting health risks, disease andinjuries, and their associated costs as borne by workers, employers, governments and other sectors of the Australian community.
This model has been used to run a simulation of this intervention, to estimate the totalbenefits for reduction in smoking for this target population, assuming 16% effectivenessbased on findings from the literature. The total benefits were found to be $113,000 inthe first year (financial savings from all health and other impacts), plus 1.3 DALYsaverted. Over a lifetime, the financial benefits were $42.8m, plus 8,463 DALYsaverted.
Table 2-10 provides detailed results, including who shares in the benefits and a financialconversion of the DALYs.
Table 2-10: Modelled results of total benefits of Quit smoking program
Health Productivity Other Sub Suffering DALYs Total
Lifetime (net of -total & Premature
benefits ($m) transfers) Mortality
Individual 3.5 4.5 4.0 12.1 1,375.7 8,463 1,387.8
Employer - 7.7 - 7.7 - - 7.7
State Government 4.3 - - 4.3 - - 4.3
Federal Government 8.8 0.3 - 9.1 - - 9.1
Community 2.4 3.5 3.7 9.6 - - 9.6
Total 19.1 16.0 7.7 42.8 1,375.7 8,463 1,418.5
Health Productivity Other Sub Suffering DALYs Total
Lifetime (net of -total & Premature
benefits ($m) transfers) Mortality
Individual 6,225 17,855 9,881 33,961 203,848 1.3 237,809
Employer - 30,336 - 30,336 - - 30,336
State Government 6,132 - - 6,132 - - 6,132
Federal Government15,158 1,160 - 16,318 - - 16,318
Community 3,611 13,651 9,138 26,399 - - 26,399
Total 31,125 63,002 19,019 113,146 203,848 1.3 316,993
The National TobaccoCampaign – a Federal, Stateand Territory Health Initiative

31Investing in Sight
4.5% of the totalfinancial benefitsand just under1% of the qualityof life gains fromquitting smokingare gained fromavoiding visionimpairment.
Promote the cessation of smoking
With costs of $3.7m for this intervention, the cost-benefit analysis for effects on visionimpairment alone would be negative over the lifetime – ($1.8m). However, if wecompare the costs to the $42.8m of total benefits, clearly there is a substantial gain –$39.1m over the lifetime. In the first year, though, even with all the benefits, the$4m campaign costs would substantially outweigh the benefits with the cost perQALY being around $2.8m (Table 2-12).
Table 2-11: Benefits (PV) from Quit smoking program, AMD and cataract
2010 2020 2030 2040 2050 Benefits
Reduced cases of cataract 0 1 13 59 73
PV cataract cost/decade/case ($) 61,773 31,599 23,087 16,897
DALYs averted per case 0.7 0.5 0.4 0.3
PV cataract cost/decade total ($) 14,897 35,741 289,609 996,356 1,336,603
DALYs averted total 0.2 0.6 5.4 19.8 25.9
Reduced cases of AMD - - 1 29 185 216
PV AMD cost/decade/ case ($) 41,399 39,371 14,768 10,440 7,394
DALYs averted per case 1.9 1.5 1.1 0.9 0.7
PV AMD cost/ decade total ($) 9,495 16,703 130,968 436,038 593,204
DALYs averted total 0.4 1.3 11.1 40.8 53.6
Total $ saved - 24,392 52,444 420,577 1,432,393 1,929,807
Total DALYs saved - 0.52 1.90 16.50 60.59 79.52
Table 2-12: Quit smoking, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost $m Net Benefit $m $/QALY
2005-06 3.7 -3.6 2,860,384
2006-07 - 0.1 cost-saving
2007-08 - 0.1 cost-saving
Lifetime 3.7 39.1 cost-saving
• This generates benefits by 2050 of $1.9m, of which $1.3m are from 73 fewercases of cataract and $0.6m are from 216 fewer cases of age-relatedmacular degeneration.
• In total nearly 80 DALYs (in present value terms) are gained from the intervention.• This suggests that 4.5% of the total financial benefits and just under 1% of the
quality of life gains from quitting smoking are gained from avoidingvision impairment.

32 Investing in Sight
UV exposure is amajor risk factor
for cataract.
2.3 Promote the use ofsunglasses/protective eye-wear
The costs of the SunSmart program were used as a proxy for a similar campaign underthis intervention that would specifically target prevention of eye exposure to UV lightthrough wearing of sunglasses and other sun protection. The SunSmart program costsamounted to $869,000, which included the cost of the total resources used for theprogram (SunSmart, 2002, p4).
Ocular exposure has been found to account for 10% of population attributable risk forcortical cataract in the community (McCarty et al, 2000, p3720), and around 6% of allcataract. McCarty et al (2000) found that the odds ratio for high UV-B exposure (>0.02Melbourne sun-years) in developing cortical cataract was 1.55.
The target population for this intervention is the whole of the Australian population, witha 5% impact parameter for the campaign, as per the findings in relation to the NTC ofsaturation awareness programs relating to behavioural change. Lifetime impacts aremodelled as for the smoking intervention and, for consistency and given the lack ofalternative data, the same effectiveness parameter of 16% is conservatively adopted,although it is likely that it is much easier for impacted people to achieve sun-protectionthan it is to give up an addictive substance like tobacco.
Differences emerge in that, since the whole population is targeted, impacts start toappear earlier and last longer – in fact cataract cases would continue to be fewer until2100. Results are summarised in Table 2-13 and Table 2-14 following (the latterpresenting the calculations), showing lifetime net financial benefits of $96.6m inpresent value (PV) terms, to 2100, 6,620 cases of cataract avoided and 1,918DALYs averted. For only $0.9m, this represents a highly cost-saving outcome.
Table 2-13: SunSmart, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost $m Net Benefit $m $/QALY
2005-06 0.9 -0.9- infinite
2006-07 - - -
2007-08 - - -
Lifetime 0.9 96.6 cost-saving

33Investing in Sight
Tab
le 2
-14
Cos
t ef
fect
iven
ess
anal
ysis
cal
cula
tions
for
Sun
Sm
art
inte
rven
tion,
to
2100
Peo
ple
who
cha
nge
thei
r b
ehav
iour
wit
h S
unS
mar
t su
cces
s ra
te o
f 16
%
Sun
smar
t ‘0
520
1020
2020
3020
4020
5020
6020
7020
8020
9021
00
0-19
2570
1,92
864
3-
20-2
913
411,
313
1,28
52.
008
30-3
914
321,
387
1,31
34,
016
2,00
8
40-4
914
381,
435
1,38
74,
103
4,01
62,
008
50-5
912
401,
339
1,43
54,
333
4,10
34,
016
2,00
8
60-6
982
51,
032
1,33
94,
485
4,33
34,
103
4,01
62,
008
70-7
956
669
51,
032
4,18
54,
485
4,33
34,
103
4,01
62,
008
80-8
929
042
869
53,
226
4,18
54,
485
4,33
34,
103
4,01
62,
008
90+
5417
242
82,
173
3,22
64,
185
4,48
54,
333
4,10
34,
016
2,00
8
Tota
l9,
756
9,72
99,
557
28,5
3026
,357
23,1
3118
,946
14,4
6110
,128
6,02
52,
008
Red
uced
cas
es o
f ca
tara
ct ,
UV
pro
tect
ion
red
uces
inst
ance
s o
f ca
tara
ct b
y 6%
Life
tim
e
Cat
pre
v ‘0
520
1020
2020
3020
4020
5020
6020
7020
8020
9021
00B
enef
its
50-5
90.
0%1
12
22
1
60-6
90.
1%1
14
43
32
70-7
91.
4%10
1559
646+
258
5729
80-8
96.
6%28
4621
427
829
828
727
226
613
3
90+
15.2
%26
6533
048
963
568
065
762
260
930
5
Tota
l Cas
es66
127
609
836
999
1,03
098
891
774
230
56,
620
PV
cata
ract
co
st p
er d
ecad
e p
er c
ase
59,5
1143
,326
31,5
9923
,087
16,8
9712
,386
9,09
46,
687
4,92
43,
631
DA
LYs
aver
ted
per
cas
e0.
90.
70.
50.
40.
30.
30.
20.
20.
10.
1
PV
cata
ract
co
st p
er d
ecad
e to
tal
3,91
1,98
45,
520,
411
19,2
3372
019
,303
,213
16,8
81,4
7912
,762
,643
8,98
7,05
76,
134,
477
3,65
5,96
11,
106,
079
97,4
97,0
24
DA
LYs
aver
ted
to
tal
5990
334
359
335
270
202
147
9330
1,91
6

34 Investing in Sight
Currently, only1 in 3 people
who are blind uselow visionservices.
Referral to lowvision services in
Australia isthrough
optometrists andophthalmologists.
2.4 Promote low vision rehabilitation services
The World Health Organisation defines a person with low vision as someone who has animpairment of vision functioning even after treatment and/or standard refractivecorrection, and has a vision acuity of less than 6/18 to light perception or a vision fieldof less than 10 degrees from the point of fixation, but who uses, or is potentially able touse, vision for the planning and/or execution of a task” (World Health Organisation,2002). In Australia the low-vision population which receives care through low vision orrehabilitation services has been estimated at between 3% and 30% of the low visionpopulation (Lovie-Kitchin et al, 1996).
However, more recent reports from Australia, Europe and the USA suggest that lessthan 6/12 is a more relevant threshold. The significant effect of vision loss on theindependence and the length and quality of life are seen at less than 6/12 rather than atless than 6/18. Moreover 6/12 is the threshold for holding a normal driving licencewhich is a powerful measure of social and economic independence.
Low vision and rehabilitation services include assistance and support of people of allages through:
• clinical – ocular examination and assessment of vision; prescription of optical ornon-optical low vision devices;
• casework/counselling – assisting with emotional coping strategies, adjustment toand acceptance of vision loss, and group therapy on topics such as stressmanagement, grief and loss, depression and the impact of changing roles due tovision loss,
• occupational therapy – reducing the impact of vision loss by enabling peoplechildren and adults to develop skills to perform tasks independently, confidentlyand safely in the home, community, workplace and education settings.
• orientation and mobility instruction – assisting people to travel independentlywith safety and confidence, through individual and group programs of instruction inuse of mobility aids; low vision training; public transport; road crossing strategies;and consultancy in modifying environments,
• multidisciplinary approaches – including network referral to related communityservices and provision for special needs groups (e.g. rural, CALD), as well as assis-tance with acquiring and using low vision devices,
• training, low vision and peer support groups – including programs, workshops,seminars, information sessions and groups to encourage contact among peoplewho have a vision impairment as well as create support networks and provideeducation and training to increase independence.
Referral to low vision services in Australia is through:• optometrists (n=288, Lovie-Kitchin et al, 1996) – only 4.7% of their patients have
low vision and they infrequently refer (42.3% referred ‘never’ or ‘rarely), butfrequently prescribe low vision devices (34.1% ‘often’ or ‘always’ prescribe).“Optometrists do not manage many patients with low vision because the patientsare usually referred to ophthalmologists for management of the underlying eyedisease. However, many optometrists could adopt a lesser degree of vision loss as

35Investing in Sight
their referral criteria for low vision services and encourage ophthalmologists to dothe same. With improved communication between the eye care practitioners andvision loss services, patients will be referred to low vision services earlier, beforevision loss severely affects their lives.” (Lovie-Kitchin et al, 1996, p227);
• and ophthalmologists (n=164, Keeffe et al, 1996) – 67% refer their low visionpatients to services ‘often or always’ but it is less common to refer to rehabilitationservices (29%) or peer support services (18%). Only 11% prescribe low visiondevices ‘often or always,’“Differences in perceived need for low vision services indicated by the criterionused for referral, and the perceived availability, influence the rate at whichophthalmologists refer their patients for services. Ophthalmologists are encour-aged to refer patients with permanent vision loss to low vision services earlier.”(Keeffe et al, 1996).
This research also concluded that:• optometrists appear to refer low vision patients for services a little earlier than do
ophthalmologists – a higher proportion of optometrists than ophthalmologists usereferral criteria that are in the less impaired categories for both vision acuity andvision field loss (Lovie-Kitchin et al, 1996, p231);
• optometrists do not manage sufficient low vision patients to influence the referralrates of patients to low vision services; and
• earlier referral enhances adjustment processes and assists people with low visionin maintaining independent lifestyles, including delaying or even preventing earlyretirement and maintaining role functions, such as caring for themselves andothers.
Pollard et al (2003) shows from referral patterns that 28% of people with mild vision loss(<6/12 – 6/18), 37.5% with moderate visions loss (<6/18 – 6/60) and 80% of people withsevere vision loss (<6/60) were referred to low vision services (42.5% overall).
The target population is thus those who are not referred with vision impairment,excluding those where cataract and refractive error are the cause, since the bestintervention for these people is treatment to correct the vision impairment.Moreover, there is some debate about when is the best time to refer those withdeteriorating vision loss to low vision services, particularly for those with only mild andslowly progressing vision loss who are already among the oldest old. Conservativelyonly those with moderate and severe loss are thus included in the target population.The total number of these people in 2005-06 is 41,643 and, assuming an impactparameter of 50% (i.e., half those with moderate and severe vision impairment whowere previously not referred are now referred), the extra people requiring serviceswould number 20,827.
Barriers to accessing low vision services include:• awareness of the services among the general public (or failure to follow referral);• awareness/referral of the services among eye care and health practitioners;
Promote low vision rehabilitation services
Earlier referralenhancesadjustmentprocesses andassists peoplewith low vision inmaintainingindependentlifestyles.

36 Investing in Sight
Promote low vision rehabilitation services
Table 2-15: Low vision services, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost Net Benefit DALYs $/QALY
2005-06 9.1 14.4 1,199 cost-saving
2006-07 8.8 13.8 1,169 cost-saving
2007-08 8.4 13.3 1,141 cost-saving
Lifetime 61.8 120.9 9,792 cost-saving
• understanding of the benefits of the services available;• perception of the quality of local services;• poor communication between patients, optometrists, ophthalmologists and low
vision services;• acceptance of low vision;• transport to services, especially for people in rural/remote areas;• integration of services within hospitals that provide eye care. (In Victoria, for
example, there have been two main not-for-profit organisations – recently formedinto a new organisation – that provided low vision rehabilitation services, but noneof the hospitals that provide eye care provide low vision services.)
The cost of increased referral involves providing information and education toophthalmologists, and to a lesser extent optometrists, of the benefits of these services,potentially together with best practice clinical guidelines that encourage timely referral.There is also a need to remove specific barriers to accessing low vision services, suchas providing greater information to the public, better communication channels andawareness/promotion of services, and transport assistance. A recurrent programdelivery budget of $250,000 has been allocated, together with a service delivery costestimated on a per person basis of $425 per annum (based on data provided by theRoyal Blind Society, Royal Victorian Institute for the Blind and Vision AustraliaFoundation). For the 20,827 people affected and requiring additional services, the totalcost in the first year would be $9.1m, rising to $61.8m in present value terms overtheir lifetime of requiring services (estimated from average life expectancy minusaverage age of onset as 9 years).
There is no a priori reason to expect that there would be additional health system costs,since low vision services are adjunctive to medical treatment. Indeed, there may befewer secondary health system impacts since falls and accidents may be averted –however, these potential benefits were conservatively excluded in Access Economics(2004) and remain so here. Benefits are estimated (by Eye Research Australia) as 20%quality of life gains (reduced DALYs) and 20% reductions in the indirect costs fromproductivity, premature mortality and carer costs, but excluding ‘other costs’ sincethese are largely aids and low vision devices, where expenditure would be likely toremain much the same, or possibly increase. On this basis the present value of netbenefits is some $13-14m each year initially and overall the intervention is cost-saving (Table 2-15).
There is a needto remove
specific barriersto accessing lowvision services in
Australia.

37Investing in Sight
Costs: Cost data were variable and speculative in relation to an awareness program foreye injuries, so a budget allocation was based on that from the SunSmart campaign($0.9m spent wholly in the first year, 2005-06). The target population is the same (allAustralians) and the ability to impact and the change behaviour to enhance eyeprotection is likely to be similar. Delivery mechanisms would include rural and generalmedia, and sports venues (particularly tennis, cricket, squash and basketball).Messages would highlight the importance of care at work (especially on the farm), in thehome and during leisure activities, particularly racquet and bat sports.
Benefits: Eye injuries (‘ocular trauma’) can result in hospitalisation, other health costs,vision loss and the consequent associated indirect costs – such as lower productivityand loss of quality of life. Data on the extent, pattern and characteristics of eye injurieshave been gathered from Fong (1993), Fong (1994) and McCarty (1999), as well as fromsupplementary data requests from the Australian Institute for Health and Welfare forseparations data and average cost per separation for ICD-10 item S05 “Injury of the eyeand orbit”.
Parameters for benefits of the campaign included:• The same as reach (impact) as for eye examinations in the general population,
since the messages are directed similarly to increasing protective behavioursamong the general community – 5.76%;
• 16% for effectiveness, as per Quit and SunSmart, based on the average of theliterature evidence for successfully acting on tailored motivational information toreduce risky behaviour. As with SunSmart, this may be conservative in relation tochanging non-addictive behaviours.
AIHW data show that there were 2,356 hospital separations in 2002-03 for oculartrauma at an average cost per separation of $2,248. This represents a populationincidence of 0.012% per annum. Applying this incidence rate to the 2005-06population suggests an estimated 2,410 hospitalisation for ocular trauma at an averagecost (inflated annually by average health cost inflation) of $2,449 per separation (thetarget population).
The impacted population who will act on the campaign messages, however, is only5.76% * 16% * 2,410 and, moreover, since Fong (1995) found that 66% of inpatientinjuries were deemed preventable through correct eye-wear use, a further discount isapplied to estimate the preventable hospitalisation – 15 in all, costing $35,914. Theratio of outpatient to inpatient costs (36%) associated with eye trauma is derived fromAccess Economics (2004) – $12,956 averted for those 15 cases in 2005-06. Fong(1995) also found that 94% of ocular trauma was cared for through outpatient facilities(with the other 6% admitted), making 37,749 outpatient cases, of which 251 (72%,Fong, 1993 * 5.76% *16%) would be avoidable (suggesting $52 per outpatient episode,on average). Each outpatient case is estimated to require 1 follow-up ophthalmic visit,while each inpatient case is estimated to require six such visits, at $83.24 per visit (asderived for eye examinations), making $28,181 specialist costs avoided in 2005-06.
2.5 Promote the prevention of eye injuries
Eye injuries canresult inhospitalisation,other healthcosts, andvision loss.
The average costper hospitalseparation foreye trauma is$2,449approximately(in 2005).

38 Investing in Sight
Table 2-16 shows findings from Fong (1994) on the extent and persistence of visionloss. 36% of inpatients (five people impacted in this scenario) continue to havemoderate or severe visual impacts. These five people are estimated to remain havingtreatment and incurring the average of ‘other’ health systems costs for their remaining life expectancy (estimated as 29 years) – $416,216 in present value terms.
In addition to avoiding health costs, indirect benefits of preventing ocular trauma areestimated for these five people as $6,874 each in 2005-06 and $123,740 each over theirlifetime, saving 10.8 DALYs as well. Cost-effectiveness results are illustrated in Table 2-16, showing $46,342 lifetime cost effectiveness analysis, still cost-effective by mostinternational standards.
Promote the prevention of eye injuries
Table 2-16: Vision loss at time of trauma, and ongoing
Inpatient Outpatient
Severe (<6/60) 27% 0%
Moderate (<6/18 – 6/60) 15% 2%
Mild (<6/12-6/18) 18% 13%
Normal vision 40% 85%
Persisting vision loss after 3 months
Moderate and severe 36% 0%
Table 2-17: Ocular trauma, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost Net Benefit $/QALY
2005-06 0.9 -0.76 $5,172,295
2006-07 - 0.03 cost-saving
2007-08 - 0.03 cost-saving
Lifetime 0.9 -0.08 $46,342

39Investing in Sight
A generalcommunityawarenesscampaign hasinduced peopleto understandand act oninformation andbetter eye care.
Costs: There were few robust data associated with running a campaign such as thisand what was available showed an enormous range of potential budgets, with thelinkages between budget and impacts (in terms of relative behavioural change) not wellresearched. The average of the campaign costs per person targeted for interventions1.2 and 1.3 was thus used – generating a total program cost of $6.1m targeted at thewhole Australian population. Costs were modelled to be incurred evenly (in PV terms)over the three periods 2005-06, 2006-07 and 2007-08. The total cost of The VisionInitiative Project over three years (2005-2008) in Victoria is estimated to be $7.3million. This figure could be extrapolated Australia-wide to around $29.2 million.
Benefits: A general community awareness campaign has its impacts through inducingpeople to understand and act on information about better eye care. In modelling, itincreases the effectiveness of the other interventions – catalysing people to have regulareye examinations, wear sun-protection for their eyes, quit smoking, avoid injuries andutilise rehabilitation services.Parameters for benefits of the campaign included:
• The average of the other interventions for reach (impact), treating the eye examina-tions as one – 24%;
• 16% for effectiveness, as per Quit, SunSmart, based on the average of the litera-ture evidence for successfully acting on tailored motivational information to reducerisky behaviour.
Using these parameters, the additional effectiveness of a general awareness campaignis summarised in Table 2-18.
• With 2-year eye examinations for people aged 40-74 in the high risk groups (plusthe elderly and people with diabetes aged 10-74), the average price of a QALYpurchased was $16,667 in 2005-06, but only $1,297/QALY over a lifetime.
• With 2-year eye examinations limited to people aged 50-74 in the high risk groups(plus the elderly and people with diabetes aged 10-74), the average price of aQALY purchased was slightly higher at $18,690 in 2005-06, reflecting missing theopportunity to derive the extra benefits of screening 40-74 year olds, and$3,871/QALY over a lifetime.
2.6 Increase community awarenessof vision care
Table 2-18: General awareness campaign, cost effectiveness analysis summary, first 3 years and
lifetime
40-74 exams Total Cost Net Benefit $/QALY
2005-06 2.0 -1.9 16,667
2006-07 2.0 -1.7 15,910
2007-08 2.0 -1.8 17,147
Lifetime 6.1 -1.8 1,297
50-74 exams Total Cost Net Benefit $/QALY
2005-06 2.0 -2.1 18,690
2006-07 2.0 -1.9 17,871
2007-08 2.0 -2.0 19,081
Lifetime 6.1 -5.1 3,871 The Vision Initiative logo

40 Investing in Sight
Tab
le 2
-19
Sum
mar
y of
net
ben
efits
, G
roup
1 a
nd G
ener
al a
war
enes
s
Not
e: S
cena
rio 1
incl
udes
eye
exa
min
atio
ns f
or t
he e
lder
ly (7
5+),
thos
e w
ith d
iab
etes
age
d 1
0-74
, and
the
oth
er e
xam
inat
ions
for
peo
ple
age
d 4
0-74
. S
cena
rio 2
incl
udes
eye
exam
inat
ions
for
the
eld
erly
(75+
), th
ose
with
dia
bet
es a
ged
10-
74, a
nd t
he o
ther
exa
min
atio
ns f
or p
eop
le a
ged
50-
74.
Total Scenario 2
Total Scenario 1
Eye Trauma
Low Vision
Sunsmart
Smoking
Gen 50-74
Gen 40-74
Diab 10-74
Glauc 40-74
Glauc 40-74
ATSI 50-74
ATSI 40-74
Elderly 75+
Net benefits $m
Gro
up 1
2005
-06
7.3
1.1
0.7
0.2
0.2
0.2
0.7
0.3
3.6
0.9
14.4
0.8
3.6
1.5
2006
-07P
V8.
11.
00.
60.
20.
10.
40.
60.
30.
1-
13.8
0.0
7.3
2.5
2007
-08P
V9.
00.
90.
60.
20.
10.
40.
60.
30.
1-
13.3
0.0
5.6
1.0
Life
timeP
V10
2.7
9.5
5.2
1.3
1.5
57.8
4.4
2.4
39.1
96.6
120.
90.
111
1.1
25.4
DA
LY’s
2005
-06
1,44
928
157
510
626
121
-1,
199
12,
818
2,73
3
2006
-07P
V1,
397
2714
75
101
2511
2-
1,16
90
2,72
92,
648
2007
-08P
V1,
334
2614
75
9624
112
-1,
141
02,
631
2,55
5
Life
timeP
V10
,655
389
158
136
802,
119
489
193
8,46
31,
918
9,79
211
33,9
7133
,496
Gen
eral
Aw
aren
essE
ffec
tive
ness
16%
2005
-06
0.3
0.0
0.0
0.0
0.0
0.0
0.0
0.0
0.0
0.1
0.6
0.0
0.1
0.1
2006
-07P
V0.
30.
00.
00.
00.
00.
00.
00.
00.
00.
00.
50.
00.
30.
1
2007
-08P
V0.
40.
00.
00.
00.
00.
00.
00.
00.
00.
00.
50.
00.
20.
0
Life
timeP
V4.
00.
40.
20.
00.
12.
30.
20.
11.
53.
54.
70.
04.
31.
0
DA
LY’s
2005
-06
571
10
04
10
0-
470
110
107
2006
-07P
V54
11
00
41
00
-46
010
610
3
2007
-08P
V52
11
00
41
00
-45
010
310
0
Life
timeP
V41
615
65
383
198
330
7538
20
1,32
51,
307

41Investing in Sight
By 2005-06 theestimated queuefor cataractsurgery is over40,000 people.
The healthsystems costsof cataract by2005-06 areestimated as$4,965 per personper annum.
3. Models of treatment and care3.1 Reduce cataract surgery waiting lists
Data for analysing this intervention were obtained from the AIHW Australian HospitalStatistics 2002-03 database, the most recent available. Admissions for cataractextraction in 2002-03 from public waiting lists numbered 38,775, with a median wait of88 days but 390 days waited at the 90th percentile (i.e., 10% of people waited morethan 390 days for their surgery). 11.0% (4,614 people) waited for more than one year.
Waiting times are typically modelled by gamma distributions, since the distributionneeds to be non-negative and with a long right tail. The desired new distribution wasmodelled to obtain a 75% improvement in wait times (i.e. to reduce the average waittime to 25% of the current average). This corresponds with a:
• median wait time of three weeks (21 days); and a• wait time at the 90th percentile of 100 days.
Calculation involved estimating the alpha and beta parameters of each gammadistribution using a grid search tool and from them deriving the mean for the ‘before’and ‘after’ scenarios. The means calculated were thus 154.2 days (before) and 38.8days (after the intervention).
The nature of the intervention would be a regulatory change (with negligible associatedcost) – e.g. contracting private hospitals or employing more ophthalmologists in publichospitals in order to meet the backlog of surgeries to this benchmark within one year –2005-06.
By 2005-06 the estimated queue (based on prevalence growth) is 40,124 people.Multiplying the queue by the average days saved (0.32 of a year) suggests that 12,865person-years of vision impairment from cataract would be prevented. The healthsystems costs of cataract by 2005-06 are estimated as $4,965 so the value of surgerybrought forward is $199m but the value of the bring-forward is $63m (12,685 * $4,965),equivalent to the total intervention costs. This would eliminate the queue so therewould be no further additional costs required in future years.
The benefits are measured as the reduction in indirect costs (allowing for productivitygains only to the extent that 1.5% of people with cataract are aged under 65), but withsavings in all other indirect costs categories ($39.5m) and also in terms of quality of life(1,440 DALYs). In sum then, the cost effectiveness analysis shows $16,280/QALY, in thehighly cost-effective range (Table 3-1).
Table 3-1: Cataract surgery, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost Net Benefit $/QALY
2005-06 63.0 -23.4 16,280
2006-07 - - -
2007-08 - - -
Lifetime 63.0 -23.4 16,280

42 Investing in Sight
3.2 Improve access to subsidised spectacleprograms
Low-costspectacles or
subsidisedspectacles are
available foreligible residents
in all AustralianStates andTerritories.
These programsare not well
advertised, andare not wellunderstood.
In all States and Territories, low-cost spectacles or subsidised spectacles are availablefor eligible residents. The most basic of these schemes are those in Western Australiaand South Australia where a rebate of about $50 is available once every two years toeligible participants for low-cost glasses.
In Tasmania, glasses in standard frames are provided free to eligible residents. Althoughit seems to be a generous scheme, eligibility criteria are strictly applied and the uptakeof the scheme seemed to be low compared to the rates in other States and theTerritories. In the previous year, possibly 70 pairs of glasses were provided to Aboriginalpeople.
In Queensland, glasses are provided to eligible participants through public hospitals.This scheme has not worked well and is currently under review.
In New South Wales and Victoria, eligible participants are prescribed glasses byparticipating optometrists or clinics and offered a choice of standard frames. Residentsholding Health Care cards are eligible under this scheme, but in New South Wales anadditional means test is included. The costs are fixed for single focal glasses andbifocal glasses. In Victoria, extra features to glasses can be provided only if the patientagrees to pay the full cost of the glasses.
These systems or schemes are not well advertised, and are not well understood.Frequently there are caps on the number of spectacles able to be provided under thescheme and so demand outweighs supply and some people miss out. Barriers are builtinto the schemes to try to regulate demand and could be seen by many consumers andpractitioners to be insurmountable. Problems with access have led to mistrust by somepeople about the subsidised services, and State-based schemes need to reconsidertheir processes to improve access and utilisation, especially by Aboriginal and TorresStrait Islander peoples (Taylor, 1997, Chapter 4). Within Aboriginal communities theprovision of free glasses is variable, available to some but not other rural people, northose in urban areas. There is little justification for such selective provision.
A summary by State/Territory follows.ACT Spectacles Schemes
• The Free Spectacles Program - free spectacles assistance (usually governmentpensioners and beneficiaries, and low income earners).
• The Senior Spectacles Scheme - free spectacles assistance for governmentpensioners.
The NSW Spectacles Scheme provides vision correction aids at no cost to eligiblepensioners and low-income earners in NSW, delivered through Vision Care, agovernment funded subsidy available to people on pensions. This allows for a limitedrange of frames and lenses at no cost to a client.

43Investing in Sight
The Northern Territory Pensioner Concession Scheme is funded by the NTGovernment to provide a range of concessions to senior citizens and pensioners whoare permanent residents and either:
• in receipt of a pension from Centrelink or the Department of Veteran's Affairs, witha current Commonwealth Pensioner Concession card with a NT address;
• a senior citizen (male 65 years and over or female 60 years and over);• a non-pension Aged War Service Veteran; or• a low income superannuant holding a current Health Care Card from Centrelink.
Concessions available under the scheme include urban bus travel, spectacles,electricity, motor vehicle registration and driver's licences, council, water and seweragerates and garbage charges, interstate and overseas travel.
Queensland: The Spectacles Supply Scheme (SSS) assists Queensland residents byproviding a range of free basic prescription spectacles. Extras such as tinting or permaguard, that are preferred but not needed for clinical reasons, can also be privatelypurchased under the Scheme. Eligibility is achieved by having:
• held a concession card for at least six months before application;• visited an optometrist/ophthalmologist to determine whether a clinical need for
spectacles exists and acquired a prescription; and• presented the prescription to the nearest public hospital or community health
service.
The South Australian Spectacle Scheme (SASS) provides Government assistance foreither a pair of reading spectacles and a pair of distance spectacles or a pair of bifocalspectacles every 2 years, unless otherwise prescribed. Assistance in the supply ofcontact lenses may be provided through Eye Departments of the Royal AdelaideHospital, Flinders Medical Centre and Women's and Children's Hospital. For peopleliving outside the metropolitan area, assistance for contact lenses may be provided forprescriptions written by any qualified prescriber. Residents of South Australia who havehad a Health Care Card for at least 12 months or who have a Pensioner ConcessionCard, and their dependents, can apply directly to any participating optometrist. SASSreimburses optometrists with 25% of the cost of standard lenses and frames. Clientspay the difference in cost if they choose more expensive options.
Tasmania: The Spectacles Assistance Scheme provides financial assistance for thepurchase of spectacles to those people who meet the guidelines. Clients are assistedwith the cost of specific types of lenses and frames. There is a restriction on thefrequency of application. The assistance is means tested and is not available to allhealth care card holders. Applications must be accompanied by an optometrist’s scriptfor glasses.
Improve access to subsidised spectacle programs
Barriers are builtinto thesubsidisedspectacleprogram schemesso demandexceeds supply.

44 Investing in Sight
Improve access to subsidised spectacle programs
Victoria: Free eye examinations and low-cost glasses are available from the VictorianCollege of Optometry for metropolitan residents and for people living in the countrythrough the Victorian Eyecare Service.
Recommendations for this intervention are thus to:• increase the supply of low-cost glasses;• implement a subsidised glasses policy for all Aboriginal and Torres Strait Islander
people; and• evaluate the State-run, low-cost glasses schemes to assess their ease of use by
culturally and linguistically diverse (CALD) groups, people with disabilities,economically disadvantaged people, including Aboriginal and Torres Strait Islanderpeople (Brotherhood of St Laurence, 2004).
Costs: Ready-made, half-frame reading glasses are low-cost (widely available in citychemists and other shops for around $20). They are ideally suited (more so than full-frame) for supply to Aboriginal and Torres Strait Islander communities and local healthservices/clinics so that those who need them could obtain them and lost or brokenglasses can be rapidly replaced. However, in general the average price of spectacles ishigher and thus the modelling has allowed for:
• subsidy of $160 per pair (Access Economics, 2004, based on private health insur-ance allowances) every two years for those in the lowest quintile income groupwith refractive error (target population 61,649 people);
• 90% impact/effectiveness in meeting demand; and• 10% effectiveness (i.e. take-up by those who would not otherwise have had
access to spectacles).
These parameters result in direct costs of $3.7m, achieved through policy change whichhas negligible associated cost. Net benefits (prevention of indirect costs) amounts to$28m in 2005-06 and 232 DALYs avoided. The intervention is thus highly cost-saving(Table 3-2).
Table 3-2: Subsidised spectacles, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost Net Benefit $/QALY
2005-06 3.7 28.1 cost-saving
2006-07 3.6 27.0 cost-saving
2007-08 3.5 26.0 cost-saving
Lifetime 71.3 500.8 cost-saving
Western Australia: The WA Spectacle Subsidy Scheme assists with the purchase of acomplete pair of prescribed spectacles or lenses by providing a fifty percent subsidy ofthe total cost to a maximum of $50. This assistance is available once every two years,subject to eligibility criteria.
Evaluation ofState-run low-
cost glassesschemes isneeded to
assess theirease of use andaccessibility of
services.

45Investing in Sight
3.3 Sustainable funding forretinal photography
Screening fordiabeticretinopathy isjustified, andcost-effectivetreatment isavailable.
Retinalphotography fordiagnosis ofdiabeticretinopathy ismore costeffective and iseasier to educateto achieve moreeffectivediagnosis.
NHMRC (1997) sets out clinical practice guidelines including for the detection ofdiabetic retinopathy, concluding that where feasible, general practitioners, optometristsand physicians should more actively screen their patients and their ability to detectretinopathy needs to be improved by regular education and more frequent practice toexceed a sensitivity target of 60%. The NHMRC advocates (p26):
• Screening for diabetic retinopathy is justified, as it is a major health problem, itsnatural history is known, and cost-effective treatment is available.
• A satisfactory level of sensitivity of at least 60% can be achieved by personnelusing dilated ophthalmoscopy or retinal photography, or non-mydriatic retinalphotography with newer cameras, after appropriate training.
• People with diabetes should request a two-yearly eye examination to screen fordiabetic retinopathy.
While retinal photography is not necessarily superior to other methods of diagnosis bywell-practiced clinicians, it has two advantages.
• It is easier to educate to achieve more effective diagnosis.- The non-mydriatic retinal camera has long been advocated as a screening tool
(Klein et al, 1985). It covers a wide angle of the retina, is easy to use, andrequires little training. It is unlikely to miss serious retinopathy beyond the 45-degree field since in these cases background diabetic retinopathy is very likely tobe detected in the photographs (Ryder et al, 1995). Retinal photography is alsowell tolerated by patients (Siu et al, 1998).
- Lin et al (2002) also found that the sensitivity of detecting diabetic retinopathy byretinal photography was significantly higher than that of direct ophthalmoscopy.This result agrees with that of studies showing that direct ophthalmoscopyperformed by general practitioners and ophthalmologists can be ineffective (Pughet al, 1993; Buxton et al, 1991). Even when performed by an experiencedophthalmologist, direct ophthalmoscopy is limited by weaknesses inherent to theophthalmoscope (Harding et al, 1995). Retinal photography is also superior todirect ophthalmoscopy in detecting maculopathy. The poor performance ofdoctors in detecting maculopathy in this study has also been reported by Tayloret al (1990).
• It is more cost effective.- The Diabetes Control and Complications Trial Research Group (1987) advocated
seven-field stereoscopic photography and fluorescein angiography as the goldstandard, but these techniques are relatively more expensive and time-consuming, and are thus not readily available.
- In the real world, retinal photography saves ophthalmologists’ time, enablinghealth care resources to be used more efficiently and allowing for the possibilityof effective screening of every diabetic patient.

46 Investing in Sight
Sustainable funding for retinal photography
Retinalphotography is
very costeffective, saving
$33.24 in thecost of each
screen relative tomore traditional
diagnosticmethods.
When modelling the cost of eye examinations, the unit cost of an examination wasestimated as $83.24. Retinal photography, in contrast, in current Australian pilotstudies, has been shown to have a unit cost of around $50 (including the healthprofessional and the photography costs). This scenario thus models the difference intotal costs of screening using retinal photography compared to traditional dilatedophthalmoscopy. As such, there is simply a cost saving, the extent of which is basedon the following parameters:
• Difference of $33.24 in the cost of each screen;• Applying the screening cost saving to the extra people with diabetes screened as
estimated in Section 2.1.4 (92,524 per annum);• Further cost-saving is modelled relative to the earlier scenario of eye examinations
using ophthalmic screening unit costs, not relative to no intervention, so that thereis no difference in treatment effectiveness.
Results would reduce the cost of Intervention 1.1.4 by $3.1m per year (75.3m over theaverage life expectancy) for people with diabetes aged 10-74 (Table 3-3).
Table 3-3: Retinal photography, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost ($m) Net Benefit ($m) $/QALY
2005-06 -3.1 3.1 cost-saving
2006-07 -3.0 3.0 cost-saving
2007-08 -2.9 2.9 cost-saving
Lifetime -75.3 75.3 cost-saving

47Investing in Sight
3.4 Sustainable funding for cost-effectiveAMD therapies
Research anddevelopment intoAMD isparticularlyimportant as itcauses nearlyhalf of allblindness inAustralia.
As foreshadowed earlier, currently treatments for age-related macular degeneration(AMD) are limited in their effectiveness in preventing vision loss. The most effectivecurrent treatments are prevention through reduction of risk factors (notably smoking)and early intervention in neovascular cases through laser photocoagulation (LPC) andphotodynamic therapy (PDT). More research is required regarding the potentiallypromising preventive impacts of lifestyle /diet factors such as dietary intake of fish, nutsand coloured vegetables, reduction of certain fats, and control of weight and bloodpressure. These factors are recommended by some but there is as yet no firmevidential basis to promote them as a public health intervention.
As noted in Access Economics (2004), the 2002-03 Federal Budget announced newfunding for PDT with verteporfin (`Visudyne Therapy'), to treat age-related maculardegeneration and retard vision loss, thus enabling independent living for longer. Theunit cost of Visudyne as at May 2002 was $2,100 per treatment plus the medical fee.Patients may need up to ten treatments over a two to three year period. Under theBudget measure, patients are able to access the therapy under Medicare and Veterans'Benefits arrangements, with access limited to those who may benefit (as per a specialDetermination under the Health Insurance Act 1973). Total Federal costs were estimatedin May 2002 for this initiative at around $30-40m per annum, although so far therealised accuracy of these estimates is not publicly available. Evaluation of the programand its effectiveness needs to be considered in relation to the cost-effectiveness ofthe further expansion of PDT.
Research and development in relation to age-related macular degeneration is thusparticularly important, noting that AMD causes nearly half of blindness in Australia(Access Economics, 2004).
Sustainable funding for cost-effective AMD therapies is a two-step process of:• Identifying such therapies through ongoing research and development; and• Funding those that are shown to be cost-effective.
In this analysis, it is premature to argue for funding of further therapies in the pipeline.Rather, we conclude that at this stage, funding is best directed towards more researchin order to more closely analyse such therapies. We present the case for this in Section4.1.

48 Investing in Sight
3.5 Improve access for the disadvantaged
Loss of vision istwice as
commonlyreported by
indigenous thanby non-
indigenouspeople.
Diabeticretinopathy and
trachoma aremajor problems
for Aboriginaland Torres StraitIslander people.
The Workshop debate on this issue centred around the severity of the issues withdelivering much-needed services to Aboriginal and Torres Strait Islanders. Total orpartial loss of vision is twice as commonly reported by Aboriginal and Torres StraitIslanders than by non-indigenous people (ABS, 2002). Differences between Aboriginaland Torres Strait Islanders and non-indigenous people are highest in the middle adultyears. Thomson et al (2004) report the following in relation to major problems.
Cataract: Cataract surgery tends to be performed later for Aboriginal and Torres StraitIslanders than non-indigenous people – when the condition is more advanced andcausing greater vision impairment. The proportion of Aboriginal and Torres StraitIslander people who reported having cataracts in the 2001 NHS was 3% (age-adjusted),compared with 2% of non-indigenous people, with higher prevalence for males (5%)than females (2%).
Diabetic retinopathy: Diabetes is a major health problem among Aboriginal and TorresStrait Islander people but there are very limited data on the prevalence of diabeticretinopathy in the Aboriginal and Torres Strait Islander population. A cross-sectionalstudy in the Katherine region in 1993 and 1996 found that the crude prevalence rates ofdiabetic retinopathy (21%) and vision-threatening retinopathy (7-8%) among Aboriginaland Torres Strait Islander people with diabetes were similar to those reported for non-indigenous people with diabetes. In a Pilbara sample (n=328) crude prevalence was23% with nearly half requiring laser treatment.
Refractive error: Levels of hyperopia (long-sighted vision) were similar for Aboriginaland Torres Strait Islander people (23%) and non-indigenous people (22%) and the levelof myopia (short-sighted vision) reported by Aboriginal and Torres Strait Islander peoplewas slightly less (17%) than that reported by non-indigenous people (21%).Children: According to the West Australian Aboriginal Child Health Survey (WAACHS),8% of Aboriginal and Torres Strait Islander children aged 4-17 years did not havenormal vision in both eyes (a level significantly lower than the 14% of children in thegeneral population found in the 1993 WA Child Health Survey not to have normal visionin both eyes). Of the 4-17 year-old Aboriginal children without normal vision in botheyes, 58% used prescribed glasses or contact lenses.
Trachoma: In Australia, trachoma is found almost exclusively within the Aboriginal andTorres Strait Islander population. A survey in a large central Australian community in late1998 found that 40% of children aged less than 13 years had infectious trachoma. Inother places, such as Broome, Derby and Kununurra in the Kimberley region of WA, theprevalence of trachoma has declined (Mak and Plant, 2001).
The report of a Commonwealth Review into Eye Health in Aboriginal and Torres StraitIslander Communities (Taylor, 1997) found that screening for diseases such as diabeticretinopathy, or trachoma in endemic areas, is not well integrated into a comprehensiveprimary health care program. The provision of training is variable with most nurses andAboriginal Health Workers developing their eye care skills on the job. Medical Officers

49Investing in Sight
Improve access for the disadvantaged
report the need for additional training particularly for conditions that are rarely seen inurban Australia such as trachoma and trichiasis. The first of 17 key recommendations ofthe review was to develop clinical practice guidelines for primary eye care and for themto be disseminated and updated regularly. Regular in-service training would assist in theimplementation of these guidelines. The guidelines were developed in 2001 (Office forAboriginal and Torres Strait Islander Health, 2001), focusing on cataract, diabeticretinopathy and glaucoma.
The intricacies of delivery mechanisms for these detailed guidelines are beyond thelevel of detail of this report, although we consider it of utmost importance that theGovernment prioritise the issues of Aboriginal and Torres Strait Islander eye health, andindeed Aboriginal and Torres Strait Islander health more generally. Access Economicshas previously addressed the workforce implications of Aboriginal and Torres StraitIslander health needs (Access Economics, 2004b), and the approach we adopt in thisanalysis extends this to estimate the eye health workforce requirements in 2005-06 andthe budget that would be required to meet those workforce needs. This approach isfounded on the principle in indigenous health of bringing the services to the people,rather than expecting the people to go to the services.
Data for this intervention was sourced from the ABS, AIHW and RANZCO.• The ABS Standard Occupational Classifications code Optometrists as 2384 and
Specialist Medical Practitioners, Ophthalmologists, as 2312-19,• From ABS Catalogue 8553.0, total optometrists in Australia in 1997-98 were 2,410.
This number grew by 2001-02 to 3,099 (AIHW 2001-02 Labour Force statistics),Projecting this growth (6.5% per annum) results in an estimated 3,985 optometristsby 2005-06 (1 for 5,100 people),
• From a 2004 RANZCO Survey, the number of ophthalmologists in Australia is 798(1 for 25,297 people). Projecting this to 2005-06 to maintain the doctor to patientratio results in an estimated 803 ophthalmologists by 2005-06,
• Applying these doctor-patient ratios to the Aboriginal and Torres Strait Islanderpopulation suggests that there should be 20 ophthalmologists and 100optometrists to provide services for Aboriginal and Torres Strait Islander people,
• Access Economics (2004b) found that there was a need for 180 extra full timeequivalent (FTE) eye specialists of all sorts, for Aboriginal and Torres Strait Islanderpeople. Assuming the same distribution of specialists as in the Australian popula-tion (3.3%)5, suggests an under-supply of six FTE ophthalmologists (30%shortage) for Aboriginal and Torres Strait Islander people. Applying the samerate of shortage for optometrists, the shortage would be 30 optometrists in2005-06,
• Using data on average weekly earnings purchased from the ABS ($132,667 perannum for ophthalmologists and $63,439 per annum for optometrists), theadditional workforce budget per annum for eye care for Aboriginal and
5 According to the AIHW Medical Labour Force Survey there were 53,991 employed medical
practitioners in Australia in 2002, of whom 17,762 were specialists and 5,474 were specialists-in-
training.

50 Investing in Sight
Improve access for the disadvantaged
There areimportant equity
considerations inaddition toeconomic
considerations inproviding eye
services toAboriginal
people.
Torres Strait Islander people is estimated as $2.69 million in 2005-06,• ABS (2005) indicates that 27% of the Aboriginal and Torres Strait Islander
community live in remote parts of Australia. However, the workforce shortages arelikely to be more severe in remote areas. We have estimated that for 50% of therequired optometrists (14.9) and 75% of the required FTE ophthalmologists (4.5)are needed in remote areas6. This would equate to 1,038 and 3,431 fly-in daysper annum (assuming FTEs work 230 days per year on average as suggested inthe RANZCO Survey),
• The travel cost of the required workforce, at an estimated $3,000 per fly-in7 , isthus estimated as $12.75m.
In total, workforce and transportation aspects total $15.4m in 2005-06.
The present value of meeting the same unmet demand into the future is shown in Table3-4. The counter case to that of retinal photography applies. Getting the workforce tothe people is essential to being able to deliver eye examinations and eye care. So thiscost is purely additional to that from Intervention 1.1.2, net benefits are wholly negative,and $/QALY are infinite. A combined result is shown in the bottom half of the tablehowever, for Intervention 1.1.2 (40-74 years) with Intervention 2.5. It shows that, whenworkforce implications are included, the delivery of eye examinations and care toAboriginal and Torres Strait Islander people is not cost-effective. However, there areimportant equity considerations in addition to economic considerations in providingsuch services, and the annual costs are not exorbitant, under $15m per annum inpresent value terms.
Table: 3-4 Indigenous eye care, cost effectiveness analysis summary, first 3 years and lifetime
Total Cost ($m) Net Benefit ($m) $/QALY
2005-06 15.4 -15.4 undefined
2006-07 15.0 -15.0 undefined
2007-08 14.6 -14.6 undefined
Lifetime 257.6 -257.6 undefined
With 1.1.2
2005-06 17.4 -14.3 -504,839
2006-07 16.9 -14.0 -510,014
2007-08 16.4 -13.6 -515,725
Lifetime 286.3 -248.1 -638,637
6 This is based on data from AMWAC (1996) that 77.5% of ophthalmologists had their primary
practice in a capital city (63.5% of population); 9.6% in other major urban areas (8.2% of popula-
tion); and the remaining 12.9% in rural and remote areas (28.3% of population). Thus the ratio of
under-representation in rural and remote areas is 1-(12.9/28.3)= 56% and is likely to be even
higher in the remote only population.
7 This is based on enquiries of charter aircraft flight prices from Adelaide to remote communities
in SA assuming next day pickup, three eye care workers per flight and a long term contract.

51Investing in Sight
4. Other Interventions4.1 Support eye research and development
and its prioritisation
Research andDevelopmentexpenditures fordiseases of theeye and adnexawere 2.0% ofhealthexpenditure,while the averagewas 2.4%.
Access Economics (2004) noted that expenditure on health research and developmentfor vision disorders is below par – both relative to other diseases in Australia and incomparison to other national per capita expenditure (especially that of the UnitedStates). AIHW (2004b) presents data for 2000-01 for conditions by loss of well-being(Table 4-1).
• Research and development expenditures for diseases of the eye and adnexawere 2.0% of health expenditure, while the average was 2.4%. This expendituredecreased from 2.6% of eye health expenditure in 1993-94 – a proportionaldecrease of 23%,
• Research and development into congenital anomalies (16.6%), infectious andparasitic diseases (11.3%), and cancer (7.9%) ranked highest in percentage terms.
• Cancer ($215m), nervous system disorders ($204m) and cardiovascular disease($153m) ranked highest in absolute terms.
Table 4-1: Comparison of research and development expenditure by disease, 2000-01($’000)
BoD chapters Research Health expenditure by disease % Total
Congenital anomalies 37 221 16.6%
Infectious and parasitic 139 1,226 11.3%
Neoplasia 215 2,705 7.9%
Endocrine, nutritional and metabolic 68 1,594 4.3%
Diabetes mellitus 35 814 4.3%
Nervous system and sense disorders 204 4,878 4.2%
Mental disordersa 109 2,929 3.7%
Neonatal causes 11 358 3.0%
Cardiovascular 153 5,484 2.8%
Total (average for % total) 1,182 49,174 2.4%
Diseases of the eye and adnexac 31.5 1,584 2.0%
Musculoskeletal 55 4,684 1.2%
Digestive system 31 2,825 1.1%
Respiratory 35 3,654 1.0%
Skin diseases 13 1,376 0.9%
Maternal conditions 11 1,315 0.8%
Oral health 27 3,374 0.8%
Genitourinary 13 2,078 0.6%
Ill-defined conditions etcb 21 5,626 0.4%
Injuries 6 4,031 0.2%
(a) Does not include expenditure on community mental health services.(b) ‘Signs, symptoms and ill-defined conditions’ includes diagnostic and other servicesfor signs, symptoms and ill-defined conditions where the cause of the problem isunknown. ‘Other contact with the health system’ includes fertility control, reproductionand development; elective plastic surgery; general prevention, screening and healthexamination; and treatment and aftercare for unspecified disease. (c) Diseases of the eye and adnexa form part of the broader BoD category nervoussystem and sense disorders'.

52 Investing in Sight
Support eye research and development and itsprioritisation
The increase inexpenditure
required to bringeye R&D to the
average in2005-06 is
$19.7m.
Expected averageannual return
from health andmedical R&D is in
the order of 2.4times the original
investment.
Table 4-2 shows the increase in expenditure required to bring research anddevelopment for vision to the national average – $6.5m would have bridged the gap in2000-01, but by 2005-06 $19.7m is required to increase expenditure from its estimatedCY2004 level to the benchmark 2005-06 level of $56.1m.
Estimating the benefits from this extra research utilises findings from Access Economics(2003) that the long term (40 year) expected average annual return from health andmedical research and development is in the order of 2.4 times the original investment (inPV terms). Assuming a linear growth path for the benefits (in accord with AccessEconomics, 2003), the lifetime benefits (over the next 40 years) would equate to $971 min healthspan (also in accord with Access Economics, 2003). To convert this to DALYsthe financial benefit is divided by the value of a life year for each period. Financialbenefits are based on a scenario of achieving 1% of the same rate of return in netsavings (i.e. the difference between current indirect costs and direct health systemcosts). The results are summarised in Table 4-3, with negative returns early on but$257m in net benefit (in PV terms) and with research and development being cost-saving over the 40 years.
Table 4-2: Research and development new expenditure required to bring eye research
expenditure to the national average
2004 2000-01 2005-06
Eyes Eyes All Difference Eyes
conditions (Eyes)
Research and development
expenditure $m 36.4 31.5 1,182 38.1 56.1
Total health expenditure $m 1,824 1,584 49,174 1,590
% Research and development 2.0% 2.0% 2.4% 0.4%
New expenditure $m
(eye research and development) 6.5 19.7
Table 4-3: Research and development, cost effectiveness analysis summary, first 3 years and
lifetime
Total Cost Net Benefit DALYs $/QALY
2005-06 19.7 -19.7 - infinite
2006-07 19.2 -18.3 7.3 -2,512,295
2007-08 18.6 -16.9 14.6 -1,158,696
Lifetime (40yrs) 463.9 257.4 5,976.0 cost-saving

53Investing in Sight
Development of aconsultativeframework toidentify strategicpriorities isneeded.
At present thereis no clearlydefined list ofeye researchpriorities forAustralia.
Support eye research and development and itsprioritisation
Research prioritiesIt is well recognised that health and medical research and development needs to bepriority driven with the “development of a consultative framework to identify strategicpriorities” (NHMRC, 2000).
The Workshop on 21 January 2005 identified the following five broad priorities:1. Support research and development into conditions that presently cannot be
prevented/treated.2. Support research and development to remove barriers to service delivery and
uptake.3. Support research and development for improved cost-utility analyses for eye care
interventions.4. Support research and development to develop new and refine existing methods of
prevention and treatment (especially with regards to the ‘big’ 5’ diseases).5. Develop a process to prioritise and increase funding for eye research.
The final item is necessary in order to drill down the prioritisation of research projectswithin the first four steps. As noted in Section 3.4, research and development into moreeffective treatments for age-related macular degeneration is a key priority within Item 1.
In order to prioritise further within Australia, two considerations are important:• similar processes developed overseas; and• a structure within which to prioritise.
To this end, Appendix B to this report includes the research agenda of three differentorganisations – the International Council of Ophthalmology that has also been endorsedby the World Health Organisation, the National Eye Institute in the United States, andthe Royal College of Ophthalmologists in the United Kingdom.
There are many areas that research could be undertaken into eye disease, particularlybearing in mind the findings highlighted by the epidemiologic studies and outlined inEye Care for the Community and in Clear Insight. In addition, as Australia has arelatively small pool of people dedicated to eye research, the research priorities andtopics need to be tailored to meet the interests, facilities and opportunities that presentthemselves to the Australian researchers. At present there is no clearly defined list ofresearch priorities for Australia. However, there is great overlap in many areas ofprioritisation for research agenda developed in the UK, the US and internationally, asshown in Appendix B.
The establishment of a structured process for developing and periodicallyreviewing an Australian list of eye health research and development priorities isrecommended for 2005-06.

54 Investing in Sight
4.2 Professional workforce implications
To estimate workforce and training implications, the first step is to estimate the impactson prevalence of vision impairment from all the interventions (Section 4.2.1).
4.2.1 Impacts of the interventions on prevalence of vision impairmentThe reduction in the number of people with vision impairment is calculated for eachintervention, with the approach tailored to the way each intervention was designed.
• For eye examinations, the numbers impacted in each sub-population are based onthe numbers requiring treatment after being examined, multiplied by the effective-ness of and compliance with the treatment, for each eye condition, and summedfor the total. Thus the implicit assumption is that there is insubstantial co-morbidity. The reduction in prevalence is calculated for the first year (nearly 4,900people) and ‘lifetime’ of the people effectively treated, which varies for each grouptargeted, with straight line extrapolation of prevalence for the intervening years,
• For the smoking and sun-awareness interventions where vision impairment isprevented, the number of cases avoided was calculated in Sections 2.2 and 2.3.There are almost none in the early years, with the vision benefits from a singlecampaign maximised around mid-century,
• For ocular trauma, the small number of cases of vision impairment averted (5-15over the time period) from the campaign modelled are calculated in Section 2.5.For low vision services, there is no impact on prevalence of vision impairment, onlyon functionality (and thus costs). The general awareness intervention is modelledas having a proportional effect on vision impairment – 16% of the combinedeffects of the other Group 1 interventions each year,
• Cataract surgery has the single largest impact on the reduction in prevalence ofvision impairment, with the queue of 40,124 people modelled as effectively treatedin the first year,
• Providing greater access to subsidised spectacles has nearly the same impact asthe eye examinations – 4,600 cases of vision impairment from refractive erroraverted in the first year, modelled to continue over the lifetime of those with newaccess,
• Research and development investment in eye care is expected to enable a linearreduction to mid-century in the cases of vision impairment, based on conversion ofthe DALYs saved back to prevalence at the weighted average of disability weights(0.10). This is a conservative assumption, since research may be targeted at, andenable, progress in effective treatment and thus prevention of vision loss from themore disabling eye conditions, such as age-related macular degeneration anddiabetic retinopathy, that have larger disability weights,
• The other interventions impact on costs, but not on vision impairment prevalenceper se.
Cataract surgeryhas the singlelargest impact
on the reductionin prevalence of
visionimpairment in
Australia.

55Investing in Sight
4.2.1 Impacts of the interventions on prevalenceof vision impairment
The various and overall impacts on prevalence are presented in Table 4-4 on the nextpage. Projections to 2024 are compared with those from Clear Insight, in the absenceof policy interventions, in Figure 4-1 below.
• While there is a substantial dip in prevalence in the first year (the cataract surgeriesand screening in particular), unless there is ongoing capacity (e.g. surgicalworkforce) and eye examinations, the queues and prevalence will begin toaccumulate again. Also, the impact parameters do deflate the ability to detect andremove treatable VI and the preventable VI has most of its impact after 2024.
• This underscores the need for the interventions to be ongoing, rather than one-offas modelled in this report. If this were the case, the reduction in prevalence ofvision impairment over time could be sustained at a much greater level. Costeffectiveness, however, may alter over time – it may be more difficult, for example,to induce each marginal person to have an eye examination or to change theirsmoking or sun awareness behaviours.
Investing in Sight Scenario 1 includes eye examinations for the general population,people with a family history of glaucoma and Aboriginal and Torres Strait Islander peoplewho are 40-74 years old. For Investing in Sight Scenario 2, those screened in thesegroups would be aged 50-74 years.
Figure 4-1: Comparison of vision impairment prevalence projections, with and without policy
interventions, 2004-2024
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
2004 2010 2014 2020 2024Year ending June
Clear InsightInvesting in Sight 1Investing in Sight 2
Providing greateraccess tosubsidisedspectacles hasnearly the sameimpact as the eyeexaminations.

56 Investing in Sight
Tab
le 4
-4
Red
uced
cas
es o
f vi
sion
imp
airm
ent
from
the
mod
elle
d in
terv
entio
ns,
2006
-202
4
Sce
nario
1 in
clud
es e
ye e
xam
inat
ions
for
the
gen
eral
pop
ulat
ion,
peo
ple
with
a f
amily
his
tory
of
glau
com
a an
d A
bor
igin
al a
nd T
orre
s S
trai
t Is
land
er p
eop
le w
ho a
re 4
0-74
yea
rs o
ld.
For
Sce
nario
2 t
hose
scr
eene
d in
the
se g
roup
s w
ould
be
aged
50-
74 y
ears
.
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
17,1
7516
,974
16,7
7416
,573
16,3
7316
,172
15,9
7215
,771
15,5
71
448
445
443
440
437
435
432
430
427
424
422
419
416
414
411
409
406
403
401
235
233
231
229
227
225
223
221
220
218
216
214
212
210
105
105
105
104
104
103
103
103
102
102
101
101
100
100
100
9999
9998
7170
7070
7069
6969
6868
6867
6767
6666
6565
65
1,26
51,
260
1,25
51,
250
1,24
51,
240
1,23
51,
230
1,22
51,
220
1,21
51,
210
1,20
51,
200
1,19
61,
191
1,18
61,
181
1,17
6
412
411
409
408
406
405
403
402
400
398
397
395
394
392
391
389
388
386
385
187
186
185
184
184
183
182
181
180
179
178
177
176
175
174
174
173
172
171
19,4
0219
,195
18,9
8518
,775
18,5
6518
,355
18,1
4517
,935
17,7
252,
145
2,13
52,
126
2,11
62,
107
2,09
72,
088
2,07
82,
069
2,05
9
18,9
3218
,724
18,5
1518
,306
18,0
9817
,889
17,6
8117
,472
17,2
631,
685
1,67
61,
668
1,66
01,
652
1,43
61,
430
1,42
41,
417
1,41
10
01
11
1326
3953
6672
7884
9097
103
109
115
121
127
176
224
272
320
155
55
55
55
55
55
55
55
55
5
3,10
93,
076
3,04
53,
013
2,93
82,
949
2,91
72,
884
2,85
135
935
935
835
835
735
736
336
937
538
2
3,03
43,
001
2,97
02,
938
2,90
72,
875
2,84
22,
810
2,77
728
628
628
528
528
525
125
826
527
127
8
22,5
4222
,303
22,0
7421
,846
21,6
1821
,381
21,1
4520
,908
20,6
722,
606
2,60
22,
598
2,59
42,
591
2,58
72,
632
2,67
72,
722
2,76
721
,994
21,7
5621
,529
21,3
0321
,076
20,8
4120
,606
20,3
7120
,137
2,07
22,
070
2,06
82,
065
2,06
31,
820
1,86
91,
918
1,96
72,
016
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
2440
,124
40,1
24
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
44,
624
4,62
4
7414
822
329
737
144
551
959
366
874
281
689
096
41,
039
1,11
31,
187
1,26
11,
335
67,2
8967
,124
66,9
7066
,816
66,6
6266
,500
66,3
3766
,175
66,0
1348
,021
48,0
9148
,162
48,2
3248
,302
48,3
7348
,492
48,6
1248
,731
48,8
5066
,741
66,5
7866
,425
66,2
7366
,120
65,6
5965
,799
65,6
3865
,478
47,4
8747
,559
47,6
3147
,703
47,7
7547
,606
47,7
2947
,852
47,9
7548
,098
Year
end
ed J
une
1.1
Eye
Exam
inat
ion
1.1.
1 El
derly
1.2.
1 AT
SI 4
0-74
1.2.
2 AT
SI 5
0-74
1.3.
1 Gl
auco
ma
fam
40-
74
1.3.
2 Gl
auco
ma
fam
50-
74
1.4.
1 Di
abet
es 1
0-74
1.5.
1 Ge
nera
l 40-
74
1.5.
2 Ge
nera
l 50-
74
1.1
Eye
Exam
inat
ion
Scen
ario
11.
1Ey
e Ex
amin
atio
nSc
enar
io 2
1.2
Smok
ing
awar
enes
s
1.3
Sun
awar
enes
s
1.4
Low
vis
ion
serv
ices
(no
VI,f
unct
iona
lity)
1.8
Ocul
ar T
raum
a
1.6
Gene
ral A
war
enes
s 1
1.7
Gene
ral A
war
enes
s 2
Grou
p 1
Scen
ario
1Gr
oup
2 Sc
enar
io 2
2.1
Cata
ract
sur
gery
2.2
Subs
idis
ed s
pect
acle
s
2.3
DR (n
o VI
,che
aper
del
iver
y)
2.4
AMD
(no
VI)
2.5
ATSI
(no
VI,n
ec d
eliv
ery
cost
)
3.1
R&D
4.1
Trai
nWF
(no
VI)
All g
roup
s Sc
enar
io 1
All g
roup
s Sc
enar
io 2

57Investing in Sight
4.2.2 Calculations of workforce requirements
The calculation of workforce needs is applied only to professional eye care workers.Research and development, for example, has a largely different workforce; similarly, theimpacts on other support workers (such as nurses for surgeries, administrators or pilots)are not considered here.
Currently in the workforce there are estimated to be 814 practising ophthalmologistsand 2,866 practising optometrists. This report has not estimated the sufficiency of theworkforce in each case to extend itself to meeting the likely increased demandgenerated by the proposed interventions. Changing work practices, productivityimprovements and existing capacity, particularly in optometry, may enable theinterventions to be implemented without deliberate policies to expand the workforce.This report presents the estimated workforce equivalent of the workforce requirement from the proposed interventions.
The calculations are based on the estimated time to undertake each intervention andattributed to ophthalmologists and optometrists based on their current respectiveworkforce shares (31.3% and 68.7% respectively), or wholly to one group (e.g.ophthalmic surgeons to perform cataract surgeries, optometrists to fit subsidisedspectacles) as appropriate.
• In Group 1 interventions, eye examinations are estimated to require three quartersof an hour each; examinations are also the only workforce impact of the generalawareness campaign. Prevention programs and avoidance of ocular traumawould, in fact, reduce workload – however, there is inconsequential impact in thefirst year, as modelled. Low vision services are generally provided outside thespecialist eye health workforce.
• In Group 2 interventions, cataract surgeries are estimated to require 3 hours onaverage – one hour for the surgery (elapsed time on average) and one hour for theconsultation before and after the surgery. The subsidised spectacle fitting time isestimated to be the same as for eye examinations, and the flying time for eye careprofessionals is based on the shortages calculated in Section 3.5. The retinalphotography workforce impacts are included in the examinations – so they are notdouble-counted.
• Full time equivalence is based on current workforce parameters (from a 2004RANZCO survey) of an average of 46 weeks per year and an average of 44 hoursper week.
• Results are presented in Table 4-5.
Currently thereare estimated tobe 814 practisingophthalmologistsand 2,866practisingoptometrists inthe Australianworkforce.

58 Investing in Sight
Calculations of workforce requirements
The total workforce requirements would be 250 in the first year, or 239 if screensof the general population, people with a family history of glaucoma and Aboriginaland Torres Strait Islander people were for 50-74 year olds (Scenario 2) rather thanfor those aged 40-74 (Scenario 1).
• Of these 113 (110) are estimated to be ophthalmologists required and 137 (130) areestimated to be optometrists required.
There is no additional workforce cost, as it is included in the costing for eachintervention. However, there may be cost implications in terms of either:
• paying a premium for the current workforce to work more hours (ophthalmologistsare already working an average 44-hour week);
• training more workforce (not possible in the short term, but the best solution in thelonger term);
• importing doctors (this also has inherent problems, including the logistical andethical problems of recruitment);
• sharing workloads better between medical professionals and other health workers– e.g. training more nurses in retinal photography, using more optometrists andAboriginal Health workers for eye examinations (the extent of this is also limited –ophthalmic surgeons are needed to perform cataract surgery, for example); or
• combinations of these strategies.
The workforce constraint may be the single most limiting factor constraining successfulimplementation of the proposed interventions in the first year.
Table 4-5: Workforce implications for interventions, ophthalmologists and optometrists, 2005-06
Workforce Number Average Total Opthal Optom FTE FTE
Impacts Treated Time Hours -mologist -etrist Opthal- Optom-
Scenario 1 (hours) hours hours mologist etrists
1.1 Eye examinations 354,821 0.75 266,116 83,344 182,772 41.2 90.3
1.6 General awareness 56,771 0.75 42,578 13,335 29,243 6.6 14.4
2.1 Cataract surgery 40,124 3 120,372 120,372 - 59.5 -
2.2 Subs spectacles 6,165 0.75 4,624 - 4,624 - 2.3
2.5 ATSI fly time 6 30
Total Scenario 1 113.3 136.9
Workforce Impacts Scenario 2
1.1 Eye examinations 330,491 0.75 247,868 77,629 170,239 38.4 84.1
1.6 General awareness 52,879 0.75 39,659 12,421 27,238 6.1 13.5
2.1 Cataract surgery 40,124 3 120,372 120,372 - 59.5 -
2.2 Subs spectacles 6,165 0.75 4,624 - 4,624 - 2.3
2.5 ATSI fly time 8,670 6 30
Total Scenario 2 110.0 129.7
The workforceconstraint may be
the single mostlimiting factor
constrainingsuccessful
implementationof the proposed
intervention inthe first year.

59Investing in Sight
ABS Australian Bureau of StatisticsACAT Aged Care Assessment TeamAIHW Australian Institute of Health and WelfareAMD Age related macular degenerationBEACH Bettering the Evaluation and Care of Health, a database collected by the
University of Sydney Family Medicine Research Centre – GeneralPractice Statistics and Classification Unit.
BMES Blue Mountains Eye StudyBoD Burden of DiseaseCBA Cost-Benefit AnalysisCI confidence intervalCME continuing medical educationcost-saving net benefits are positive so DALYs do not have to be ‘purchased’DALY Disability Adjusted Life YearDM diabetes mellitusDR diabetic retinopathyECP eye care professionalFTE full time equivalentGDP gross domestic productGP general practitionerHCP health care professionalICD-10 International Classification of Disease, Tenth RevisionICPC2 International Classification of Primary Care Version TwoMBS Medicare Benefits ScheduleMVIP Melbourne Visual Impairment ProjectNHMRC National Health and Medical Research CouncilNOHSC National Occupational Health and Safety CommissionNTC National Tobacco CampaignOECD Organisation for Economic Cooperation and DevelopmentPDT photodynamic therapyPIP Practice Incentive SchemePR public relationsPV present valueQALY Quality Adjusted Life Year (1-DALY)QoL quality of lifeRANZCO Royal Australian and New Zealand College of OphthalmologistsRE refractive errorUS United StatesUV ultra-violet, a type of light that can damage the eyeVA visual acuityVI vision impairment (<6/12); blindness <6/60 and/or a visual field of <10o
VLY Value of a life yearVSL Value of a statistical lifeWHO World Health OrganisationYLD Years of Life Lost due to DisabilityYLL Years of Life Lost due to Premature Mortality
List of abbreviations

60 Investing in Sight

61Investing in Sight
References
Access Economics (2004) Clear Insight: The Economic Impact and Cost of Vision Lossin Australia, Report for Eye Research Australia, August.
Access Economics (2004b) Indigenous Health Workforce Needs, report for theAustralian Medical Association, Canberra.
Access Economics (2003) Exceptional Returns: The Value of Investing in HealthResearch and Development in Australia, report for the Australian Society for MedicalResearch.
American Academy of Ophthalmology, October 2003, www.aao.org
Australian Bureau of Statistics (2005) Australia Now :Year Book Australia ABS Cat No1301.0-2005, Article: “Selected findings from the 2002 National Aboriginal and TorresStrait Islander Social Survey”,www.abs.gov.au/ausstats/[email protected]/0/294322bc5648ead8ca256f7200833040
Australian Bureau of Statistics (2004) Deaths, Australia Cat No 3302.0, December.
Australian Bureau of Statistics (2003) Population Projections, Australia Cat No 3222.0,September.
Australian Bureau of Statistics (2002) National Health Survey 2001, Summary of ResultsCat. No. 4364.0, Canberra, 25 October.
Australian Institute of Health and Welfare (2004) Health Expenditure, Australia, 2002-03, Cat No HWE 27, Health and Welfare Expenditure Series No 20, Canberra,September.
Australian Institute of Health and Welfare (2004b) Health system expenditure on diseaseand injury in Australia, 2000–01, AIHW Cat No HWE 26, Health and Welfare ExpenditureSeries No 19), Canberra, May (and later data revisions).
Australian Institute of Health and Welfare (2003) Health and community services labourforce 2001, Cat No HWL 27 and ABS Cat No 8936.0, National Health Labour ForceSeries, Canberra.
Australian Medical Workforce Advisory Committee (1996) The Ophthalmology workforcein Australia: Supply, requirements and projections AMWAC Report 1996.6, September,Sydney.
Brotherhood of St Laurence (2004) Seeing Clearly: Access to Affordable Eye Care forLow Income Victorians ISSN 1326 2963.
Buxton MJ, Sculpher MJ, Ferguson BA, et al (1991) “Screening for treatable diabeticretinopathy: a comparison of different methods” Diabet Med 8:371-7.

62 Investing in Sight
References
Department of Health and Ageing (2004) 1997-2003 National Tobacco Campaign:Evaluation Response and Recall Measures Among Smokers and Recent Quitters,Canberra, April.
Department of Health and Ageing (2000) Australia’s National Tobacco Campaign:Evaluation Report Volume 2, Canberra, May.
Harding SP, Broadbent DM, Neoh C, White MC, Vora J. (1995) “Sensitivity andspecificity of photography and direct ophthalmoscopy in screening for sight threateningeye disease: the Liverpool Diabetic Eye Study” Br Med J 311:1131-5.
Heijl A, Leske C, Bengtsson B, Hyman L, Bengtsson B, Hussein M for the EarlyManifest Glaucoma Group (2002) “Reduction of intraocular pressure and glaucomaprogression” Arch Ophthalmol 120:1268-1279.
Hopley C, Salkeld G, Mitchell P (2004) “Cost utility of photodynamic therapy forpredominantly classic neovascular age related macular degeneration” Br J Ophthalmol88:982-987.
Kass MA, Heuer DK, Higginbotham EJ, Johnson CA, Keltner JL, Miller JP, Parrish RK II,Wilson MR, Gordon MO (2002) “The Ocular Hypertension Treatment Study: Arandomized trial determines that topical ocular hypertensive medication delays orprevents the onset of primary open-angle glaucoma” Arch Ophthalmol 120:701-713.
Keeffe JE, Weih LM, McCarty CA, Taylor HR (2002) “Utilisation of eye care services byurban and rural Australians” Brit J Ophthalmol 86:24-27.
Keeffe JE, Lovie-Kitchin JE, Taylor HR (1996) “Referral to low vision services byophthalmologists” ANZ J Ophthalmol 24.
Klein R, Klein BE, Neider MW, Hubbard LD, Meuer SM, Brothers RJ (1985) “Diabeticretinopathy as detected using ophthalmoscopy, a nonmydriatic camera and a standardfundus camera” Ophthalmol 92:485-91.
Lin DY, Blumenkranz MS, Brothers RJ, Grosvenor DM (2002) The sensitivity andspecificity of single-field nonmydriatic monochromatic digital fundus photography withremote image interpretation for diabetic retinopathy screening: a comparison withophthalmoscopy and standardized mydriatic color photography. Am J Ophthalmol;134:204-213.
Lovie-Kitchin JE, Keeffe JE, Taylor HR (1996) “Referral to low vision services byoptometrists” Clin Exp Optom 79:227-234.
Mak D and Plant A (2001) “Trichiasis in Aboriginal people of the Kimberley region ofWA” Clin Exp Ophthalmol 29:7-11.
McCarty C, Nanjan MB, Taylor HR (2000) “Attributable risk estimates for cataract to

63Investing in Sight
References
prioritise medical and public health action” Inv Ophthalmol Vis Sci 41(12):3720-3725.McKay R, McCarty CA, Taylor H (2000) “Diabetic Retinopathy in Victoria, Australia: theVisual Impairment Project” Brit J Ophthalmol, 84(8), 865-870.
Miller M and Wood L (2001) Smoking cessation interventions: review of evidence andimplications for best practice in health care settings, Commonwealth Department ofHealth and Ageing (Coordinated by the National Heart Foundation as part of theNational Tobacco Strategy 1999 to 2002-03), Canberra, August.
Mitchell P, Chapman S, Smith W (1999) “Smoking is a major cause of blindness: A newcigarette pack warning?” Med J Aust editorial 171:173-174.
Mitchell P, Smith W, Attebo K, Wang JJ (1995) “Prevalence of age-related maculopathyin Australia - The Blue Mountains Eye Study” Ophthalmol 102:1450-1460.
National Health and Medical Research Council (2000) Health and Medical ResearchStrategic Review: Implementation of the Government’s Response, Final Report, October.
National Health and Medical Research Council (1997) Management of DiabeticRetinopathy: Clinical Practice Guidelines Commonwealth of Australia, June.
Nottle HR, McCarty CA, Hassell JB, Keeffe JE (2000) “Detection of vision impairment inpeople admitted to aged care assessment centres” Clin Exp Ophthalmol 28:162-164.
Office for Aboriginal and Torres Strait Islander Health (2001) Specialist Eye HealthGuidelines for use in Aboriginal and Torres Strait Islander populations: Cataract, DiabeticRetinopathy, Glaucoma, Commonwealth of Australia.
Pollard T, Simpson JA, Lamoureux EL, Keeffe JE (2003) “Barriers to accessing lowvision services” Ophthal Physiol Opt 23:321-327.
Pugh JA, Jacobson JM, Van Heuven WA, et al (1993) “Screening for diabeticretinopathy. The wide-angle retinal camera” Diabetes Care 16:889-95.
Ryder RE, Vora JP, Atiea JA, Owens DR, Hayes TM, Young S (1985) “Possible newmethod to improve detection of diabetic retinopathy: Polaroid non-mydriatic retinalphotography” Brit Med J (Clin Res Ed) 291:1256-7.
Siu SC, Ko TC, Wong KW, Chan WN (1998) “Effectiveness of non-mydriatic retinalphotography and direct ophthalmoscopy in detecting diabetic retinopathy” Hong Kong Med J 4:367-70.
Smith W, Assink J, Klein R, Mitchell P, Klaver CCW, Klein BEK, Hofman A, Jensen S,Wang JJ, deJong PTVM (2001) “Risk factors for age-related macular degeneration:pooled findings from three continents” Ophthalmol 108:697-704.

64 Investing in Sight
References
Smith W, Mitchell P, Seeder SR (1996) “Smoking and age-related maculopathy”Arch Ophthalmol 114:1518-1523.
Stewart WC, Konstas AGP, Pfeiffer N (2004) “Patient and ophthalmologist attitudesconcerning compliance and dosing in glaucoma treatment” J Oc Pharm Ther 20(6):461-469.
SunSmart (2002) “SunSmart Program 2003-2006” Submission to the VicHealth reviewof the SunSmart Program, July.
Taylor HR, Vu HT, McCarty CA, Keeffe JE (2004) “The need for routine eyeexaminations” Inv Ophthalmol Vis Sci, 2539-42
Taylor S, Galbraith S, Mills R (2002) “Causes of non-compliance with drug regimens inglaucoma patients: a qualitative study” J Oc Pharm Thr 18(5):401-409.
Taylor HR (1997) “Eye Health in Aboriginal and Torres Strait Islander Communities” The Report of a review commissioned by the Commonwealth Minister for Health andFamily Services, Commonwealth of Australia, Canberra.
Taylor R, Lovelock L, Tunbridge WM, et al (1990) “Comparison of non-mydriatic retinalphotography with ophthalmoscopy in 2159 patients: mobile retinal camera study”Brit Med 301:1243-7.
The Diabetes Control and Complications Trial Research Group (1987) “Colorphotography vs fluorescein angiography in the detection of diabetic retinopathy in thediabetes control and complications trial” Arch Ophthalmol;105:1344-51.
Thomson N, Burns J, Burrow S, Kirov E (2004) Overview of Indigenous health:December. www.healthinfonet.ecu.edu.au/html/html_keyfacts/overview.pdf
Turner R, Holman R, Stratton I, Cull C, Frighi V, Manley S, Matthews D, Neil A, McElroyH, Kohner E, Fox C, Hadden D, Wright D (1998 ) “Tight blood pressure control and riskof macrovascular and microvascular complications in type 2 diabetes: UK ProspectiveDiabetes Study Group” Brit Med J;317:703-713.
Van Newkirk MR, Nanjan MB, Wang JJ, Mitchell P, Taylor HR, McCarty CA (2000) “ThePrevalence of Age-related Maculopathy: The Visual Impairment Project” Ophthalmol107:1593-1600.
Van Veldhuisen PC, Ederer F, Gaasterland DE, Sullivan EK, Beck A, Prum BE Jr, CyrlinMN, Weiss H (2000) “The Advanced Glaucoma Intervention Study (AGIS): 7. Therelationship between control of intraocular pressure and visual field deterioration” Am JOphthalmol 130:429-440.
World Health Organisation (2002) Low Vision Care in the Asia-Pacific, WHO, Geneva.

65Investing in Sight
Appendix ASummary of workshop agenda and participants
VISUAL IMPAIRMENT INTERVENTIONS PACKAGE (VIIP)WORKSHOP
Friday 21 January 2005Lucy Jones Hall, Albert St, East Melbourne
(Aubrey Bowen Wing, Royal Victorian Eye and Ear Hospital)
AGENDA
This companion report to Clear Insight will aim to formulate, in consultation with key stakeholders, a costed platform of strategic policy interventions to: • provide a comprehensive assessment of additional spending required, and where it might be directed, and to • eradicate preventable blindness and vision loss and its impact through early detection, prevention, rehabilitation, education and research.
10.00 Welcome and introductions Professor Hugh Taylor AC, Managing Director, Centre for Eye Research Australia.
10.10 Presentation of the findings of Clear Insight Prof Taylor
10.30 Questions and answers re the Clear Insight presentation Fielded by Prof Taylor; Lynne Pezzullo, Senior Economist, Access Economics
10.45 Costing A VIIP: outline of the proposal Prof Taylor – intro; Lynne Pezzullo – presentation
11.15 General discussion of the VIIP proposal Goal: A grouped itemised list, for the small group discussions after lunch Facilitated by Lynne Pezzullo with Sarah Nesbitt, Economist, Access Economics
12.00 LUNCH BREAK
12.45 Small groups to detail interventions Goal: Consideration and specification of intervention details, in table format Each group to select a spokesperson/scribe
2.30 AFTERNOON TEA
2.45 Summary of the small group sessions and discussion of findings Goal: Finalisation of an agreed detailed list of interventions for costing Facilitated by Lynne Pezzullo with Sarah Nesbitt
3.45 Next steps, including further consultative processes Led by Prof Taylor with Lynne Pezzullo
4.00pm WORKSHOP CONCLUDES
Figure A-1: Workshop agenda

66 Investing in Sight
Participation was excellent and broad – a list of participants is provided below.
Summary of workshop agenda and participants
Table A-1 Workshop participants
Mr Ian Bluntish National President, Optometrists Association Australia
Mr Joe Chakman Executive Director, Optometrists Association Australia
Ms Margaret Cox Office for an Ageing Australia, Department of Health
and Ageing
Ms Sally Fearn Australian Community Manager, Vision 2020 Australia
Ms Chris Faulks Director, Member Organisation Services, Diabetes Australia
Ms Bernadette Funnell McPhersons Promotions
Ms Jayne Gallo General Manager, Community Services Vision
Australia Foundation
Dr Robert Grogan Executive Director, Clinical Services, Royal Victorian
Eye and Ear Hospital
Mr Bob Guest Chief Executive Officer, Royal Australian and New Zealand
College of Ophthalmologists
Ms Julie Heraghty Chief Executive Officer, Macular Degeneration Foundation
Mr Tony Hill Managing Director, Capital Hill Consulting
Dr Masum Hossain Medical Director, Pfizer Australia
Hon Dr Barry Jones AO Chairman, Vision 2020 Australia
Associate Professor Jill Keeffe Director, Population Health DivisionCentre for Eye Research
Australia
Ms Paris Kostakos Adviser to the Hon Tony Abbott MP, Minister for Health and
Ageing, Leader of the House of Representatives
Dr Tamara Mackean Aboriginal and Torres Strait Islanders Health Education,
Department of Medical Education Flinders Medical Centre
Dr Mark McGree McCullough Specialist Centre, Sunnybank, QLD
Mr Patrick Moore President, Macular Vision Loss Support Society
Dr Andreas Muller Head, Eye Health Promotion Unit, Population Health
DivisionCentre for Eye Research Australia
Ms Sarah Nesbitt Economist, Access Economics
Ms Lynne Pezzullo Senior Economist, Access Economics
Professor Richard Smallwood AO Director, Vision 2020 Australia
Ms Laurie Staub Executive Director, Eye Research Australia Foundation
Dr John Stokes Business Unit Head, Ophthalmics, Novartis
Pharmaceuticals Australia
Ms Irene Tam Retinal Vascular Unit, Clinical Epidemiology Division Centre
for Eye Research Australia
Professor Hugh R. Taylor AC Managing Director, Centre for Eye Research Australia
Dr Michael Treplin Vice PresidentRoyal Australian and New Zealand College of
Ophthalmologists
Mr Rod Watts Director, Corporate Services Division, Centre for Eye
Research Australia
Associate Professor Tien Wong Director, Clinical Epidemiology Division, Centre for Eye
Research Australia
Mr David Yates National Sales Manager, Bausch and Lomb

67Investing in Sight
Workshop outcomes
The Workshop discussed the grouping and contents of the interventions, asfollows.
1. Awareness, detection and prevention1.1 Increase community awareness of the importance of eye health and vision care.1.2 Promote the cessation of smoking (cataract, AMD), possibly linked to the QUIT.1.3 Promote the use of sunglasses/ protective eye-wear (cataract, general), possibly
linked to the SunSmart campaign.1.4 Promote regular vision testing for general population.1.5 Promote more frequent vision testing for those in high risk groups (family history
of glaucoma; diabetics; Aboriginal and Torres straight Islander people; theelderly.
1.6 Educate the public on the importance of prevention, early intervention andrehabilitation programs.
1.7 Focus on prevention of eye injuries, especially at home, sport and rural areas.
2. Models of treatment and care2.1 Testing of vision to be a routine part of aged-care assessments (refractive error;
cataract) – through GPs and by Aged Care Assessment Teams.2.2 Improve access to optimal rehabilitation for all those with vision loss.2.3 Improve access to services for specific disadvantaged groups, such as
Aboriginal and Torres Strait Islander people, rural and remote communities andthose from culturally and linguistically diverse backgrounds.
2.4 Improve access to subsidised spectacle programs across Australia.2.5 Increase awareness and utilisation of the pathways to eye health and rehabilita-
tion services for those with low vision.2.6 Improve efficiency and capacity of cataract surgery services with reduction in
waiting lists.2.7 Sustainable funding for retinal photography (a Medicare item number) for DR.2.8 Sustainable funding for cost-effective therapies for AMD.
3. Research and development3.1 Support research and development into conditions that presently cannot be
prevented/treated.3.2 Support research and development to remove barriers to service delivery and
uptake.3.3 Support research and development for improved cost-utility analyses for eye
care interventions.3.4 Support research and development to develop new and refine existing methods
of prevention and treatment (especially with regards to the ‘big’ 5’ diseases).3.5 Develop a process to prioritise and increase funding for eye research.
4. Professional education and workforce4.1 Update training of ECPs so that patient management follows clinical practice
guidelines (DR, glaucoma, AMD and low vision referrals).4.2 Increase awareness of services, roles and responsibilities among HCPs.

68 Investing in Sight
Workshop outcomes
4.3 Support prioritisation of eye care in medical training schools.4.4 Support prioritisation of eye care in primary care/GPs (e.g. PIP, CME).4.5 Plan for the funding of workforce implications of other initiatives (including
distribution of the workforce).
This list was agreed by the group as a whole and then discussed in the smaller workinggroups. There were four working groups, one for each of the above areas.
The working groups were asked to discuss and complete, to the extent they were able,a table for each intervention with the headings as illustrated below.
Specific Delivery Take-up rates, Second round Special
details of Target setting/ likely (flow on) issues/
intervention Population mechanism(s) effectiveness impacts comments
This process identified some areas of overlap and redundancy from the original list, aswell some areas where more research would be required in order to identify keyparameters such as likely effectiveness or impacts. The resulting spreadsheets wereuseful inputs in the process for costing the interventions.
Other more general issues raised included:• timeframes for implementation of interventions may vary (2020 is a key date but
annual costings were considered important);• regional disparity and cross-jurisdictional hurdles may complicate delivery;• interventions for Aboriginal and Torres Strait Islanders need to be placed high on
the list;- the needs and requirements of Aboriginal and Torres Strait Islander people are
very different and Government has yet to re-energise an already existing programthat targets these differences;
- while there is a lot of information about the barriers to implementing recommen-dations from Aboriginal and Torres Strait Islander health studies, there has been alack of progress in implementation of services to overcome those barriers;
- mainstream services need to be more responsible to Aboriginal and Torres StraitIslander communities and be held more accountable for theirshortcomings;
- Aboriginal and Torres Strait Islander considerations should be integrated acrossthe spectrum of policy interventions in this project;
• prevention and public health research and interventions are also priorities;• since people have a fear of losing vision, there may be a good community
response to prevention messages, especially in an ageing population who vote;• a large PR campaign, similar to ‘Slip, Slap, Slop’, may be simple and effective in
relation to eye care – it can take over ten years for messages to sink in and theurgent must not displace the important;- disadvantaged/less educated individuals are less likely to act on campaigns;

69Investing in Sight
Workshop outcomes
- The Vision Initiative has a key role in raising awareness of eye care in Australia;- the baby boomer generation is more likely to question a doctor’s advice and
diagnosis and this should be considered in a campaign;- an imaginative campaign presented by a famous figure with eye problems may be
effective, together with memorable advertising.• it is important to find out why Australians do not make full use of the excellent eye
care services in Australia (the Visual Impairment Project is starting to build up apicture), plus market research as to what works in the way of advertising;
• the main boost needs to come in eye examinations, which can identify manyconditions at the same time;- the emphasis for regular exams should be on those aged over 40 or 50 years;- ‘the elderly’ should be modelled as those aged 75 years and over;- vision testing might be linked to renewal of drivers’ licenses;- five-year exams were generally considered adequate for ‘normal risk’ and two
year exams for high risk groups;• GPs have the potential to be the linkage between the community and eye health
services, e.g. through routine health checks, but many do not feel confident toconduct eye examinations (80% of GPs will refer if a patient’s problem is eyerelated), partly because they may have just two weeks in five years training on eyesand too many other competing needs;
• Similarly, Aged Care Assessment Teams may not feel equipped to carry out eyetests, but could also be important referral points;
• the cervical screening register whereby patients sign-up to be sent reminders to betested every two years may be a useful comparator;
• there are problems with setting research priorities in Australia in that theseresearch areas can be small when investigator driven;- directing research needs to be done on a large scale with large groups;- research into better models of care is important, as is research into those condi-
tions that cannot be prevented or treated;• a National Vision Plan by Vision 20208 has been presented to Government and
there is a strong coalition of interest in the eye care community regarding the nextsteps;- this is an opportunity for Government and the eye health care community to work
in unity together for better eye health outcomes.
8 Vision 2020, a global coalition of international agencies to eliminate avoidable blindness and
vision loss by the year 2020. This reference is to Vision 2020 Australia, launched in 2000.
www.vision2020australia.org.au

70 Investing in Sight

71Investing in Sight
Appendix B International research agenda
International Council of Ophthalmology - A Research Agenda for GlobalBlindness and Prevention – 2003; Endorsed by World Health Organisation20049
1. Cataract• Short-term. Analytical research to estimate the loss of well-being and the cost
benefit of different models, and to identify reasons for regional variation in cataractsurgery rules and outcomes
• Short to medium term. Operational research directed at increasing the amount ofeffective, high-quality cataract surgery provided to those presently underserved,primarily by identifying ways in which to reduce the marginal costs of cataractsurgery and increase geographical and financial access to effectivesurgical services
• Medium to long term. Progress in understanding lens biology and developinginterventions that reduce the incidence/progression of cataract
• Twenty-three specific targets for cataract research are also listed
2. Trachoma• Improving surgical outcome of trichiasis surgery. At present, the relapse rate, even
for well-trained ophthalmic surgeons, is high• Elucidating the role of acute/recurrent/chronic infection in the pathogenesis of
conjunctival scarring• Documenting the dynamics of infection/reinfection (e.g., what serves as the reser-
voir of C. trachomatis following mass antibiotic treatment; how is it reintroducedinto a community; how does it spread between individuals?)
• Determining what is required to sustain the reduction in prevalence of infection andactive disease following antibiotic treatment (and thereby block development ofblinding trachoma?)
• Demonstrating how SAFE can be most effectively delivered
3. Onchocerciasis (Research Priorities Not Relevant for Australia)
4. Xerophthalmia (Research Priorities Not Relevant for Australia)
5. Glaucoma• Develop practical techniques for effectively screening populations to identify eyes
at high risk of vision impairment and blindness from angle closure glaucoma• Determine the value of laser iridotomy as long-term prophylaxis in those who never
previously suffered angle closure• Evaluate the cost-efficiency of screening and prophylaxis interventions in popula-
tions of varying risk• Develop screening techniques to identify subgroups at particularly high risk of
primary open angle glaucoma
9 Downloaded from http://www.nei.nih.gov/strategicplanning/nationalplan1.pdf, 7 March 2005

72 Investing in Sight
International research agenda
6. Diabetic Retinopathy and Age-Related Macular Degeneration• Documenting population variations in risk (AMD, DR) to elucidate genetic and
environmental markers/pathogenetic mechanisms• Study the nature of angiogenesis and its relation to antioxidant intake in micronu-
trient poor populations• Develop better tools for defining risk, early disease, and tracking progression• Conduct operational research on extending retinal photocoagulation to poor
populations suffering from diabetic retinopathy
7. Refractive Error• Identify social and cultural constraints to utilizing refractive services and spectacles• Develop protocols for the education, training, and certification of low-cost
spectacle providers• Experiment with alternative organisational systems and infrastructural support for
the sustainable provision of appropriate low-cost spectacles (e.g., micro-creditenterprises, formal refraction vs. patient self-selection from among spectacles ofvarying correction, individually ground lenses vs. snap-in spherical equivalents)
• Enrol high risk populations into epidemiologic studies and randomized clinical trialsseeking environmental/behavioural etiologic factors and effective strategies forreducing the incidence/progression of refractive error
• Analyse the cost-benefit and cost-effectiveness of alternative interventions(including spectacles), considering their economic impact on education (andsubsequent earning power)
• Investigate the value of social marketing of refraction/spectacles• Identify the origins of myopia• Investigate alternative interventions for reducing the incidence/progression of
refractive error• Apply evolving technologies to the treatment of refractive error in poor populations
• Confirm early treatment/prophylaxis interventions make a long-term difference inthe risk of glaucomatous vision impairment and blindness
• Confirm epidemiologic studies to identify environmental/behavioural factors thatcontribute to (seemingly) societal variations in risk of open angle glaucoma
• Develop simplified and sensitive measures of progression of optic nerve damageto test alternative interventions and improve the benefits of intervention/manage-ment
• Develop new and novel treatment approaches, particularly neuroprotection(beyond medical and surgical approaches targeting IOP)

73Investing in Sight
International research agenda
National Plan for Eye and Vision Research, U.S. Department of Health andHuman Services, National Eye Institute 1999 - 2003
1. Retinal Disease• With regard to macular degeneration, understand the molecular and biochemical
bases for its different forms, improve early diagnosis, characterize environmentaleffects on its etiology, and develop new treatments
• Understand the pathogenesis of DR and other vascular diseases of the retina anddevelop strategies for primary prevention and improved treatment
• Identify the genes involved in both inherited and retinal degenerative diseases(including RP), determine the pathophysiological mechanisms underlying thesemutations, and determine new potential therapeutic strategies for treatment suchas gene transfer, tissue and cell transplantation, growth factor therapy, andpharmacological intervention
• Establish the causes and etiology of uveitis and improve methods for its diagnosis,treatment, and prevention
• Use both molecular and physiological approaches to study light adaptation inphotoreceptors, with particular emphasis on the visual cycle, and identify thepostphotoreceptor neural components of adaptation
• Build on knowledge gained from retinal neuroscience to understand how retinalnetworks process visual images, a central unanswered question of modern neuro-biology
• Understand the genetic, cellular, and immunologic changes characterizing eyecancers and develop innovative methods of diagnosis and treatment
2. Corneal Disease• Explore the biology of the ocular surface as a physiological system, consisting of
the tear film, cornea, conjunctiva, lacrimal and meibomian glands, eyelids, andtheir innervations, to gain a better understanding of the interaction and regulationof these components under normal and pathological conditions
• Investigate corneal infectious and inflammatory processes and immunologicalresponses to develop treatments to reduce keratitis and prevent blindness
• Apply the knowledge acquired from discoveries in the basic science of the corneaand other tissues of the ocular surface to the diagnosis, prevention, and treatmentof ocular injury and disease
3. Lens and Cataract• Understand the physiological, biochemical, and biophysical bases of lens trans-
parency on the cellular and molecular levels• Determine the causes and mechanisms of age-related changes in the lens that
lead to cataracts and presbyopia• Understand lens development and the diseases associated with defects in this
process

74 Investing in Sight
International research agenda
4. Glaucoma• Develop diagnostic methodologies and treatment regimens that lead to improved
patient outcomes and prevent vision loss from glaucoma and other opticneuropathies
• Understand the basic biology underlying the pathophysiology of glaucoma andother optic neuropathies
5. Strabismus, Amblyopia, and Visual Processing• Determine the etiology of myopia in humans, identify the risk factors associated
with myopia and other refractive errors, and identify the biochemical pathwaysassociated with the control of eye growth
• Understand how the visual system develops, its capacity for plasticity, and ways topromote its regeneration
• Investigate the development of visual function in children at high risk for amblyopiaand strabismus, determine underlying mechanisms, and develop and disseminateinformation about detection methods and therapeutic interventions for restoringnormal vision
• Analyze visual performance in normal and dysfunctional states and develop clini-cally useful diagnostic tests for assessing visual performance, particularly in infantsand young children
• Understand the neural circuitry and muscular mechanisms that control gaze underenvironmental conditions and discover the mechanisms that provide plasticity tothe oculomotor system
• Understand how the brain processes visual information, how neural activity isrelated to visual perception, and how visual processing interacts with other brainsystems underlying cognition
6. Low Vision and Blindness Rehabilitation• Improve understanding of CNS structure and function, neural plasticity, and the
performance of everyday tasks so that the perceptual processing capabilities ofpeople with low vision or blindness can be optimized
• Develop assistive devices, environmental modifications, and rehabilitation strate-gies to minimize the impact of vision impairment in everyday life and reducedisability and societal limitations in visually impaired persons
• Determine which interventions are most effective and develop research tools sothat the approaches can be scientifically evaluated, leading to improved clinicaland rehabilitative care for the visually impaired population
• Establish the scope of impaired vision and blindness in U.S. society and its ramifi-cations for everyday life, identifying the prevalence of vision impairment, itsfunctional limitations, and the risk factors for visual disability. These efforts willpermit interventions to be targeted to high-risk and underserved subpopulations ofindividuals with vision impairments and blindness

75Investing in Sight
International research agenda
• Create a network for the dissemination of research findings to rehabilitationspecialists, educators, clinicians, and technology developers. Establish the meansand avenues for adapting research for use in clinical and rehabilitation settings
• Build an infrastructure for developing future generations of researchers who areconcerned with a broad range of topics in vision impairment and rehabilitation.Encourage the multidisciplinary collaboration and training of researchers from otherareas about issues pertinent to vision impairment
7. National Eye Health Education Program• Increase awareness of glaucoma, diabetic eye disease, and low vision in selected
high-risk target audiences in the United States• Increase awareness of the importance of early detection of glaucoma, diabetic eye
disease, and low vision services, with the ultimate goal of effecting appropriatebehavior change
• Increase health care providers’ awareness of the need for regular, comprehensiveeye examinations with dilated pupils for those at risk for glaucoma and diabeticeye disease and the need for referrals to low vision services, with the ultimate goalof effecting appropriate behavior change
• Encourage these groups to take appropriate action based on their increasedawareness
A National Research Strategy for Ophthalmology, Royal College ofOphthalmologists, UK – march 2002
1. Retinal Disorders• Evaluation of novel treatments and improvement of existing treatments in AMD,
diabetic retinopathy and vein occlusion including,• Assessment of most efficient delivery of diabetic screening and ophthalmic
management in the UK diabetic population• Clinical trials of new immunosuppressive agents to control intraocular inflammation • Elucidation of novel genes and chromosomal loci causing monogenic retinal
disease• Elucidation of population genetic polymorphisms influencing the susceptibility to
age-related macular degeneration and diabetic retinopathy• Evaluation of gene function, protein structure, chemistry and interaction in cell
systems and animal models• Elucidation of novel therapies including gene replacement therapy, modulation of
retinal cell apoptosis, catalysis of harmful gene mutations in vivo (ribozymes) andretinal cell transplantation
• Characterization of molecules involved in neovascularisation occurring in AMD,diabetic retinopathy and vein occlusion (e.g. vascular endothelial growth factor)
• Identification of cytokine profiles of the infiltrating cells from ocular fluids

76 Investing in Sight
International research agenda
• Devising strategies to switch off particular cytokines by these cells using otherdownregulatory cytokines
• Identification of cytokine and other genetic polymorphisms that might influencedisease outcome
• Characterization of phenotype of AMD genetic polymorphisms (e.g. ApoE4)• Elucidation of genes conferring susceptibility of diabetics to sight-threatening
retinopathy• Phenotype-genotype characterization of ocular inflammatory disorders• Development of RPE transplantation strategies in AMD• Development of drugs to use in intraocular devices to control intraocular
inflammation
2. Vitreoretinal Disease• The use of adjunctive medications in vitreoretinal surgery especially posterior
segment trauma and PVR and slow-release vehicles for adjuncts• Analysis of the surgical management of age-related macular degeneration. • Further investigation of the causes and management of retinal detachment and
proliferative vitreoretinopathy (PVR), including a fundamental study into combinedgliosis and fibrosis
3. Lens and Cataract• Evaluate intraocular lens technologies for the prevention of posterior capsular
opacification after cataract surgery• Evaluate strategies for the effective delivery of resources to patients with cataract• Evaluate strategies to reduce the impact of the major complications of cataract
surgery• Identify environmental risk factors for age related cataract formation and under-
stand their influence on lens homeostasis • Determine how markers of cataractogenesis interact with environmental influences
to confer a susceptibility to age-related cataract• Determine if there are genetic factors that interact with environmental influences to
confer a susceptibility to age-related cataract• Characterize the mechanism of scarring responses following cataract surgery at a
cellular and molecular level
4. Glaucoma• Natural history of glaucoma and risk factors for progression• Optimal treatment strategies to arrest disease progression • Mechanisms for raised intraocular pressure• Genotype/phenotype correlation• Cellular mechanisms of optic nerve damage

77Investing in Sight
International research agenda
5. Cornea and External Eye Disease• Identification of risk factors for iatrogenic disease such as refractive surgery,
contact lens wear and inappropriate use of topical medications• Rapid diagnosis and improved treatment strategies for ocular infections • Corneal wound healing mechanisms• Factors affecting corneal graft survival and strategies to prevent rejection• Molecular genetic analysis of the corneal dystrophies and degenerations
6. Ocular Adnexal Diseases• The epidemiology and risk factors for ocular and adnexal tumours • Research into the mechanisms of tumour induction• Studies in the immunological mechanisms causing orbital inflammatory disease• Studies into the mechanisms of scar formation following eyelid trauma
7. Neuro-ophthalmology• Visual rehabilitation in untreatable neural blindness• Protection of vision in chronic raised intracranial pressure syndromes• Rehabilitation of binocular function in neurogenic squint• Immunotherapies for inflammatory optic neuropathies
8. Vision Impairment and Rehabilitation• Examine the effectiveness of rehabilitation processes for the visually impaired,
especially in terms of which strategies are most (vs. least) effective for various sub-populations of patients
• Establish the prevalence and incidence of vision impairment, visual disability and ofsub-populations at heightened risk
• Carry out research on the visual mechanisms underlying object recognition,locomotion and mobility, skilled movement, and reading, and on the interaction ofvision with sensory, motor, and cognitive systems in these complex behaviours.This research should include an examination of neural plasticity
• Develop effective assistive devices and techniques to maximize residual visionand/or substitute for visual information, in order to facilitate the performance ofeveryday tasks by the visually impaired
• Develop environmental designs and modifications that facilitate access in thehome and workplace, and while travelling in public places, in order to enhanceindependence among the visually impaired

78 Investing in Sight
9. Paediatric Ophthalmology• Understand the extent and the causes of childhood vision impairment • Conduct randomized controlled trials of treatment of amblyopia and strabismus• Conduct randomized controlled trials of screening for amblyopia • Health-care delivery in management of strabismus and amblyopia• Effects of childhood vision impairment: educational, emotional and social • Visual rehabilitation • Identification of disease causing mutations• Investigation of disease mechanisms of inherited eye disease• Development of novel treatment strategies for inherited eye disease• Multidisciplinary research to understand the mechanism of brain injury• Investigation of visual development and visual performance in brain injured children
10. Squint and Amblyopia• Determining whether very early squint surgery gives better outcomes for binocular
function• Determining the optimum management of intermittent squints• Determining optimum management for thyroid eye disease• Cost-benefit analysis of visual screening in children and determining the optimum
age(s) for screening • Understanding the changes in the brain underlying amblyopia and determining why
some children fail to respond to patching• Understanding why binocular function breaks down in some children• Understanding mechanisms underling development of correct focusing of the eye
and why this fails in some children.
International research agenda

79Investing in Sight
Eye Research Australia is one of Australia’s leading eye research centres. It is renowned globally for its work in preventing and establishing the causes and treatment of eyedisease, vision loss and blindness through teaching and research. It was established in1996 around the University of Melbourne’s Department of Ophthalmology.
Eye Research Australia was established as a collaborative undertaking between theUniversity, the Royal Victorian Eye and Ear Hospital, the Royal Australian and NewZealand College of Ophthalmologists, the Ansell Ophthalmology Foundation, ChristianBlind Mission International, the Lions Clubs of Victoria and RBS.RVIB.VAF Ltd.
A core partner of Vision CRC, it is the only centre in Australia designated by the WorldHealth Organisation as a WHO Collaborating Centre for the Prevention of Blindness.
Eye Research Australia commissioned the independent economic analysts, AccessEconomics Pty Limited to undertake a full analysis of vision impairment in Australia andreport on the economic impact and cost to governments, industry and the communityat large. Clear Insight - The Economic Impact and Cost of Vision Loss in Australia wasthe first such independent study of this issue which was released in August, 2004.
Investing in Sight - Strategic Interventions to Prevent Vision Loss in Australia, is acomprehensive assessment of spending required to eliminate preventable blindness andvision impairment in Australia. The report outlines where additional spending might bestbe deducted to have impact through easy detection, prevention, rehabilitation,education and research.
Access Economics Pty Limited provides independent, credible and high quality servicesin three broad areas:
• Economic publications and model-based forecasting• Investment advisory services to institutional investors• Economic advising across all areas of economic policy, including
- health and welfare advisory services such as disease cost and burdenanalyses, health financing and workforce modelling.
The skill mix required to deliver this unique combination of services and the strongsynergies between them, means Access Economics Pty Limited offers an unmatchedlevel of in-house expertise.
Eye Research Australia and Access Economics

80 Investing in Sight
Notes