Embed Size (px)
Citation preview
Intestinal Obstruction
Prepared by Ahmad Zaki and ZurinaSupervisor : Dr Viknes
Outlines
DefinitionClassifications Pathophysiology CausesHow to diagnoseManagementTake home messages
Definition• Intestinal obstruction is a partial or complete blockage
of the bowel that prevents the contents of the intestine from passing through.
Classification
• Mechanical and functional• Partial and complete• Simple and strangulated• Acute and subacute
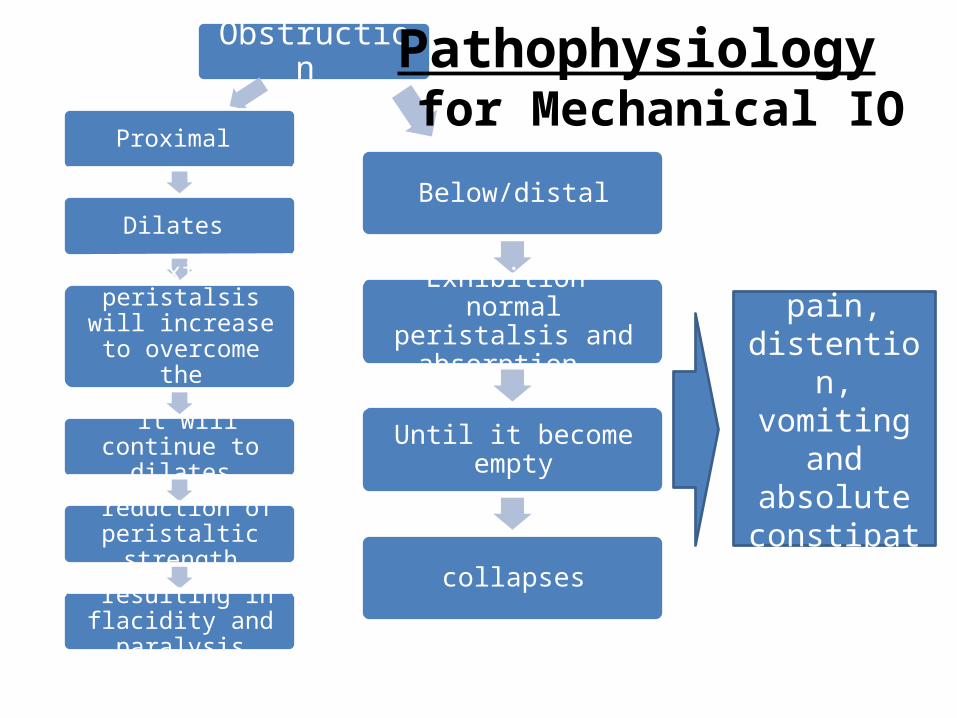
Obstruction
Proximal
Dilates
Proximal peristalsis will increase to overcome the
obstruction
it will continue to dilates
reduction of peristaltic strength
resulting in flacidity and paralysis
Obstruction
Below/distal
Exhibition normal peristalsis and absorption
Until it become empty
collapses
abdominal pain,
distention, vomiting and
absolute constipation.
Pathophysiology for Mechanical IO
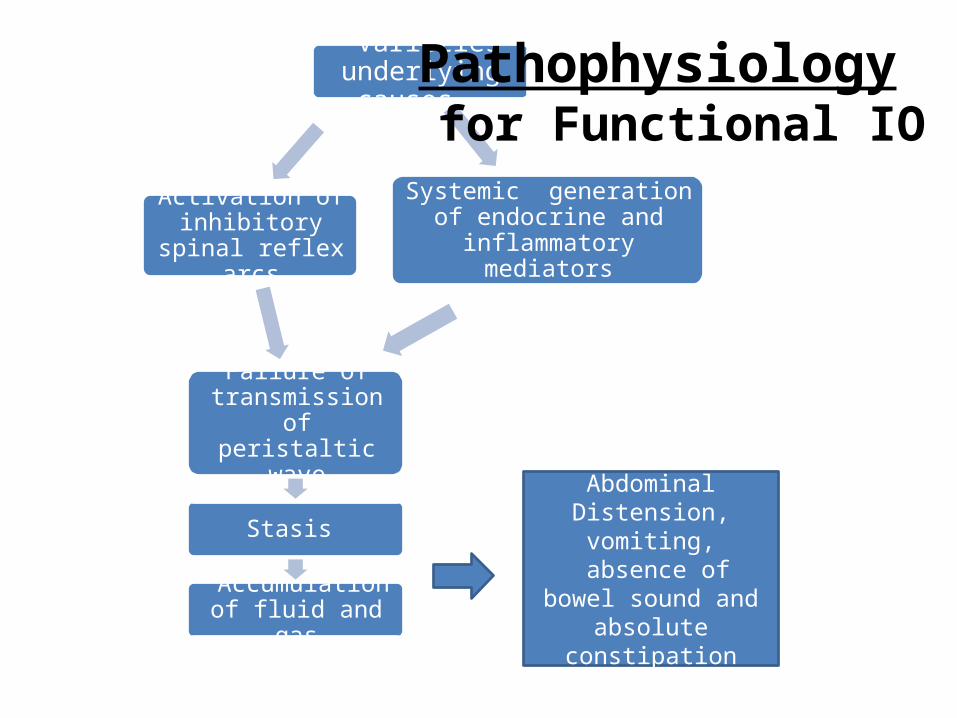
Varieties underlying causes
Systemic generation of endocrine and inflammatory
mediators
Activation of inhibitory spinal
reflex arcs
Failure of transmission of peristaltic wave
Stasis
Accumulation of fluid and gas
Abdominal Distension, vomiting,
absence of bowel sound and absolute
constipation
Pathophysiology for Functional IO
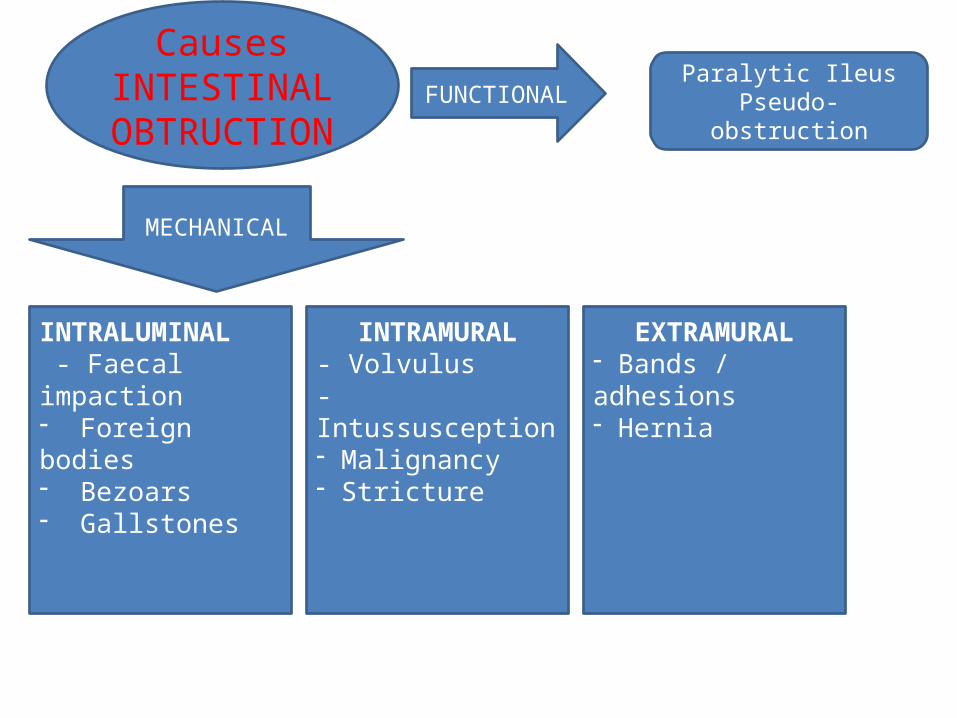
INTRALUMINAL - Faecal impaction- Foreign bodies- Bezoars - Gallstones
INTRAMURAL- Volvulus- Intussusception- Malignancy - Stricture
EXTRAMURAL- Bands / adhesions- Hernia
Causes INTESTINAL
OBTRUCTIONParalytic Ileus
Pseudo- obstructionFUNCTIONAL
MECHANICAL
• ELDERLY – carcinoma, diverticulitis, sigmoid volvulus
• ADULT – hernia, adhesion, carcinoma• PAEDIATRICS – intussusception, congenital
hypertrophic pyloric stenosis, atresia (duodenum, ileum), meconium obstruction, volvulus neonatorum
How to diagnose?
• Thorough history and clinical examination• Investigations– Biochemical test– Radiology
History
4 cardinal symptoms• Abdominal pain• Vomiting and nausea• Abdominal distention • Absolute constipation
Others: dehydrations, hypokalaemia, pyrexia, abdominal tenderness, high pitched bowel sound.
1) Pain• first symptom, occurs suddenly and usually severe. • Nature : colicky, coincide with peristalsis constant,
diffuse as distension increases.• severe pain indicative of strangulation.
2) Vomiting• The more distal the obstruction, the longer interval
between the onset of symptoms and nausea/vomiting.• As obstruction progresses the character of the vomitus
alters (digested food faeculent material; as a result of the presence of enteric bacterial overgrowth)
3) Distension• Small bowel: dependent on the site of the obstruction
and is greater the more distal the lesion.• Colonic obstruction: delayed distension • Visible peristalsis may be present.
4) Constipation• Absolute or relative.
– Absolute constipation COMPLETE intestinal obstruction.• The rule that constipation is present in intestinal
obstruction does not apply in:– Richter’s hernia; gallstone obturation; mesenteric vascular
occlusion; obstruction associated with pelvic abscess; partial obstruction (faecal impaction/colonic neoplasm) ~diarrhoea may often occur.
The clinical features vary according to:• the location of the obstruction• the age of the obstruction• the underlying pathology• the presence or absence of intestinal ischaemia.
■ In high small bowel obstruction, vomiting occurs early and is profuse with rapid dehydration. Distension is minimal ■ In low small bowel obstruction, Vomiting is delayed. pain is predominant with central distension. ■ In large bowel obstruction, distension is early and pronounced. Pain is mild and vomiting and dehydration are late.
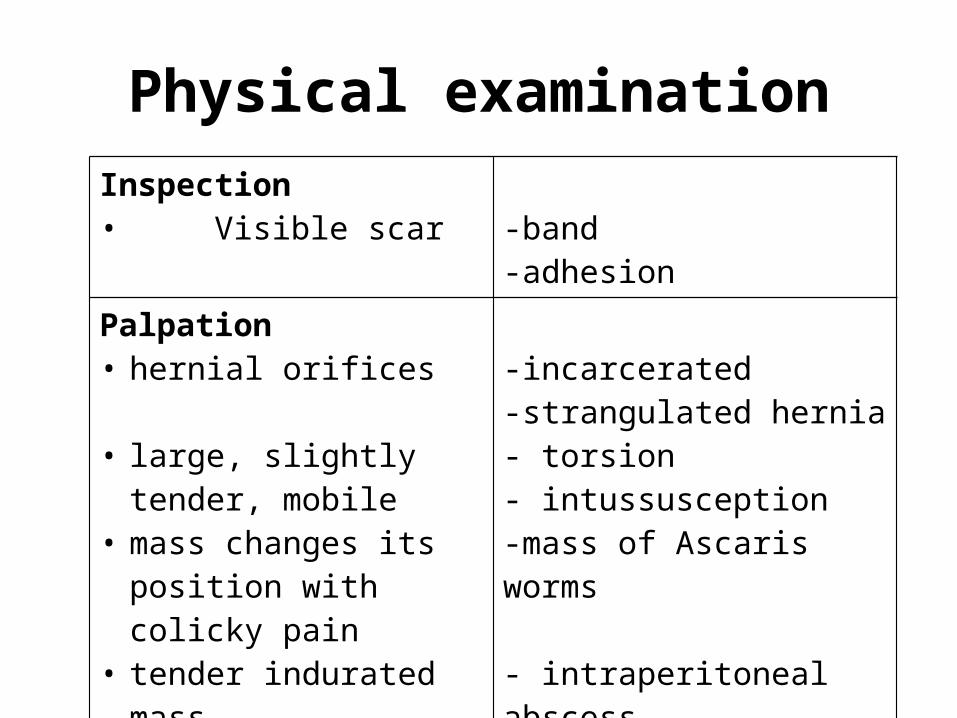
Physical examinationInspection• Visible scar -band
-adhesionPalpation• hernial orifices
• large, slightly tender, mobile
• mass changes its position with colicky pain
• tender indurated mass• hard impacted masses
-incarcerated -strangulated hernia- torsion- intussusception-mass of Ascaris worms
- intraperitoneal abscess- fecaloma
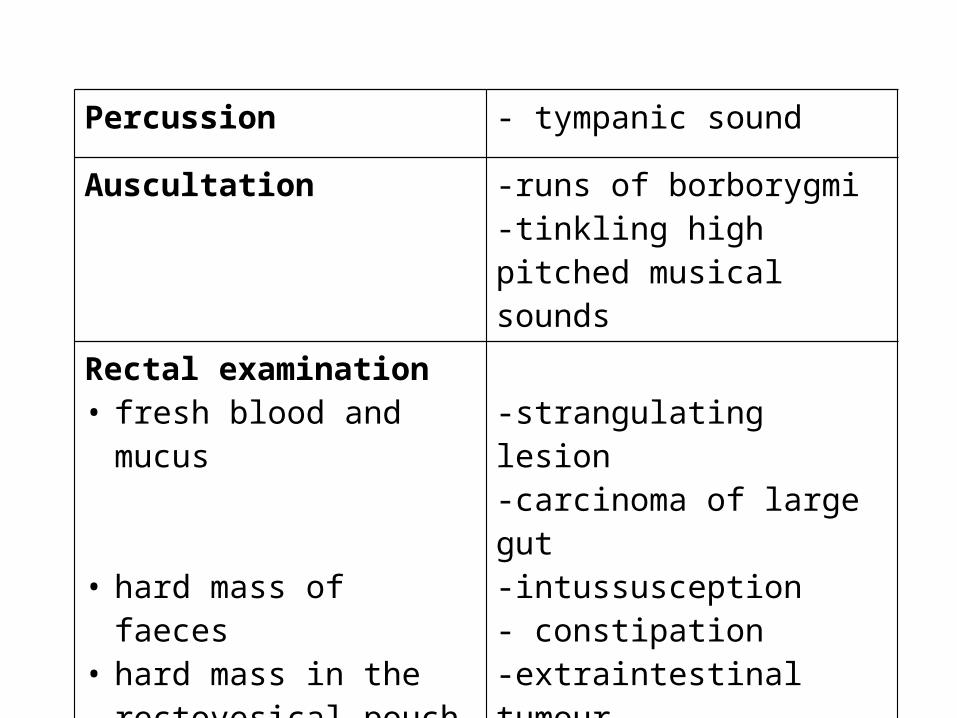
Percussion - tympanic sound
Auscultation -runs of borborygmi-tinkling high pitched musical sounds
Rectal examination• fresh blood and mucus
• hard mass of faeces• hard mass in the
rectovesical pouch
-strangulating lesion-carcinoma of large gut-intussusception- constipation-extraintestinal tumour
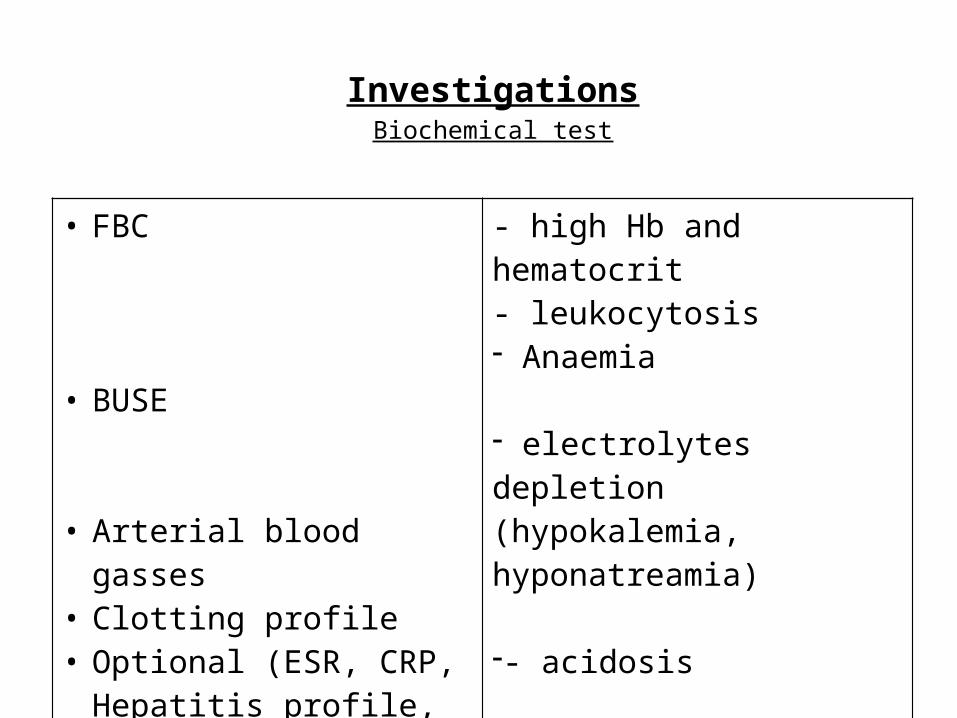
InvestigationsBiochemical test
• FBC
• BUSE
• Arterial blood gasses• Clotting profile• Optional (ESR, CRP, Hepatitis
profile, tumour markers)
- high Hb and hematocrit- leukocytosis- Anaemia
- electrolytes depletion (hypokalemia, hyponatreamia)
-- acidosis
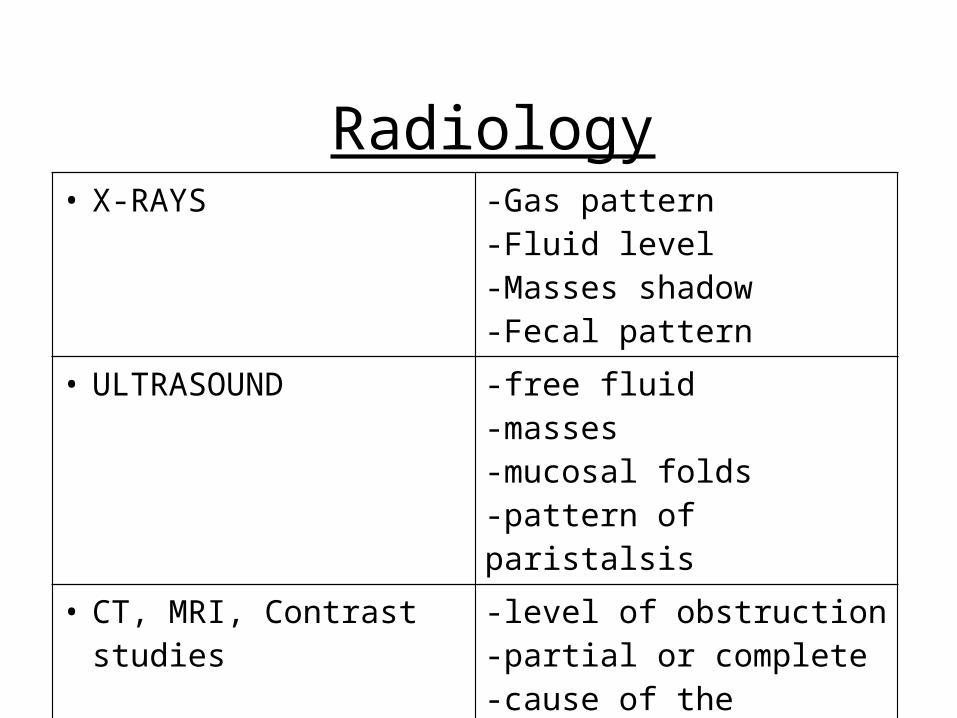
• X-RAYS -Gas pattern-Fluid level-Masses shadow-Fecal pattern
• ULTRASOUND -free fluid-masses-mucosal folds-pattern of paristalsis
• CT, MRI, Contrast studies -level of obstruction-partial or complete-cause of the obstruction
Radiology
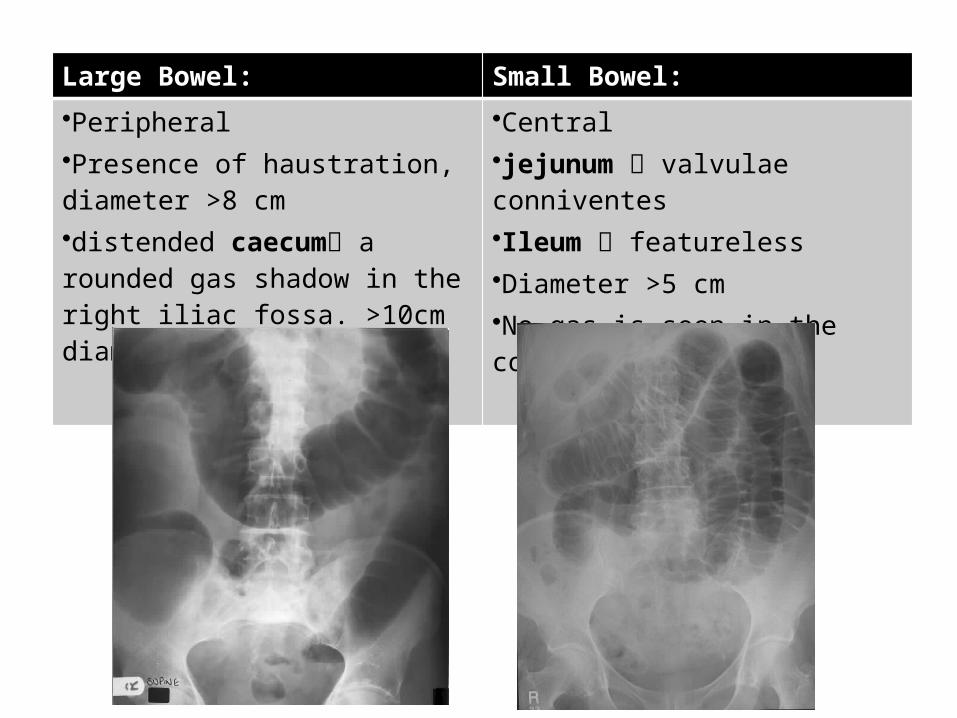
Large Bowel: Small Bowel:
•Peripheral•Presence of haustration, diameter >8 cm•distended caecum a rounded gas shadow in the right iliac fossa. >10cm diameter.
•Central•jejunum valvulae conniventes•Ileum featureless•Diameter >5 cm•No gas is seen in the colon
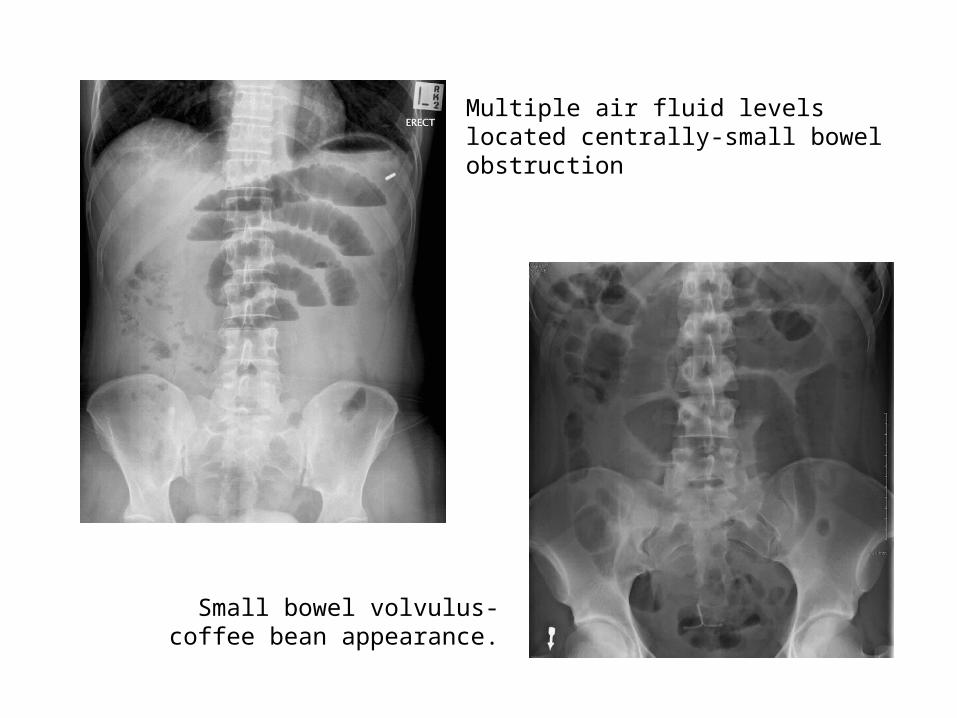
Multiple air fluid levels located centrally-small bowel obstruction
Small bowel volvulus-coffee bean appearance.
Management• Early management• Conservative• Operative
Early management• Resuscitation– Oxygen therapy (if necessary)– Correct dehydration and electrolytes– IV antibiotics-IV cefobid 1gm bd, IV flagyl 500 mg tds
• Close monitoring– Temperature,Pulse,BP,Urine output, Central venous
pressure• Regular re-evaluation • Keep nil by mouth• Nasogastric tube- 4hourly aspirate and free flow • Appropriate analgesia
Conservative If obstruction presumed to be due to adhesions and there are no features of
peritonism, conservative management may be consider.
– Nasogastric tube • to help decompress the dilated bowel
– CBD• To monitor urine output
– IV fluid• Normal saline or Hartman’s for intravascular volume depletion
– Electrolytes correction• Guided by test results
– Analgesic• Opioid pain relievers may be used for patients with severe pain
– Antibiotic• If bowel ischemia or infarction is suspected
Operative
Principles of surgical intervention for obstruction• Management of:– The segment at the site of obstruction– The distended proximal bowel– The underlying cause of obstruction
Indications for surgery
• Immediate intervention:– Evidence of strangulation (eg:hernia)– Signs of peritonitis resulting from perforation or ischemia
• In the next 24-48 hours– Clear indication of no resolution of obstruction ( Clinical,
radiological).– Diagnosis is unclear in a virgin abdomen
Take home messages
• The 4 main Cardical signs of intestinal obstruction are Abdominal pain, Abdominal distention, Vomiting and Constipation.
• Always examine for hernia orifice.• Request for Supine, Erect and CXR.• Provide adequate resusitation to the patient. • Be attentive of signs of peritonitis resulting
from perforation or ischemia of bowel.





























