Embed Size (px)
Citation preview
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 1/49
Urinary Tract Infections
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 2/49
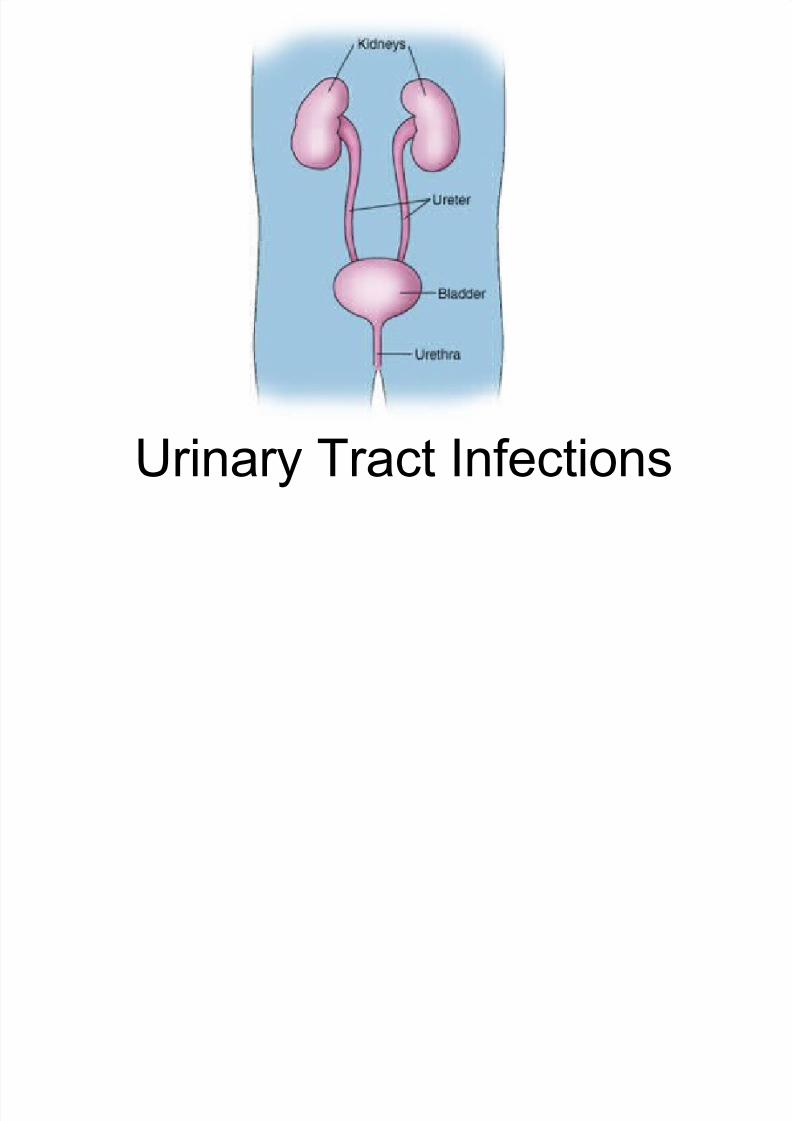
Sherwood Fig. 12-6a, p.530
Renal
vein
(a)
Ureter
Aorta
idne!
Renalarter!
Urethra
Urinar!
"ladder
#n$erior
vena %ava

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 3/49
Figure 26.1
An introduction to the UrinarySystem

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 4/49
Getting Clear on the Terminology
UTI
Asymptomatic
Bacteriuria
Symptomatic
UTI
Cystitis
Urosepsis
Asymptomatic
UTI
Pylonephritis
Pyuria
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 5/49
5
#n$e%tion#n$e%tion
Infection is defined as the entry and
multiplication of microorganism(s) in the
tissues of the host that produces injuriouseffects.

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 6/49
6
&!'titi'&!'titi'
Infection of the urinary tract limited to the
bladder usually in!ol!ing only the mucosal
surface " Most common type of UTI in the long-term care
setting

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 7/49
#
!elonephriti'!elonephriti'
Infection of the $idney usually resulting from
tra!el of the infection from the bladder to the
ureter and then to the $idney.(ascending)

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 8/49
%
Uro'ep'i'Uro'ep'i'
&epsis occurs 'hen bacteria ha!e entered the
bloodstream and lead to a 'idespread
(systemic) inflammatory response.rosepsis means the infection has stemmed
from an infection of the urinary tract

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 9/49
A'!ptoati% *a%teri+riaA'!ptoati% *a%teri+ria
*he presence of bacteria in the urine of a
person 'ithout symptoms of infection.
" Should not be called a UTI " Should not be treated with antibiotics

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 10/49
1+
!+ria!+ria
*he presence of 'hite blood cells in the urine.
" The body’s reaction to inasion by bacteria!
" "ne of the #ey differentiating points betweenUTI and assymptomatic bacteriuria

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 11/49
Getting Clear on the Terminology
Polla#isuria
Polla#isuria$dysuria
syndrome
Anuria
%ysuria
Polyuria
"liguria
Cylindruria
&ematuria

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 12/49
◙ The risk of uti in women 10x men.
Why?
the shorter distance between anus and
meatus urethrae externum.
◙ amost haf of a woen wi ha!e at east
one UTI in their i!es.◙ the risk of UTI in women increases after
meno"ause
U.T.I.

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 13/49
◙ after a UTI #0 $ %0 & wi ha!e a recurrence
◙ the recurring infections are usuay
re$infections.◙ asym"tomatic 'acteriuria in women occurs in
#.& of 1 $ #% year ods
*.+& of o!er , year ods and
#0 $ 0& of o!er -0 year ods
U.T.I.

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 14/49
UTI is rare in young and middle-aged men UTI in men is often associated with catheterisation
or urological procedures.
bacteriuria in elderly men occurs in
/ about 10% of those living at home, / about 0% of those living in nursing homes and
/ !0% of those who are in-patients in hospitals
urinary catheter increases the ris" almost ten-foldin hospitalised patients and those in other carehomes.
pyelonephritis is common in patients who havebeen catheterised for over a month.
RA/&

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 15/49
Urinary tract infection occurs when bacteriawhich colonise the anal area ascend throughurethra to the bladder
Risk factors include
/ reduced resistance oered by the mucousmembranes (e.g. after menopause
/ se!ual intercourse
/ disturbances in ureteral functioning
/ in children the re"entering of urine back into theureters (#esicoureteral re$u!% &hich predisposesthem particularly to upper UT's
athogenesis

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 16/49
athogenesis
#ther ris" factors$
benign prostatic hypertrophy
any illness% such as diabetes% &hich aectsthe emptying of the bladder
spinal in)ury (associated &ith disturbancesin bladder emptying or urinary catheter
catheterisation in hospital or residentialcare
other urological procedures
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 17/49
&a+'ative agent' o$ U#'
Escherichia coli / most common
/ about *+, of primary care infections
/ about -+, of hospital"acuired infections
/thers0
/ enterococci
/ Staphylococcus saprophyticus and
/ klebsiellas / #arious types of pseudomonas and proteus
are more rare
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 18/49
&opli%ated or +n%opli%ated
Uncomplicated& urinary tract infections are
/ occasional lower urinary tract infections inwomen &ith no predisposing factors to infections
'omplicated& infections are all other UTIs including lo&er UT's in
/ pregnant &omen
/ men
/ children / and catheter"induced infections
/ The in#estigations and treatment of these entailspecial features

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 19/49
S!pto' o$ U#' 1
'ystitis$
typical symptoms include freuency and burningsensation &hen passing urine.
(yelonephritis$
only some patients ha#e di1culties in micturition
temperature (2 3*oC and $ank or back pain
nausea in the elderly or sudden collapse in healthstatus (4o"legs4

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 20/49
Symptoms of UT's 5
incontinence or oensi#e urine in the elderly shouldnot be considered as UT' as such6 e#en though theymay be indicati#e signs of an infection
almost any signs of infection in infants may beindicati#e of a UT' )'*
in a small child a temperature alone% &ithout anyother signs of an infection% should raise a suspicion ofa UT'
UT' in children and the elderly may manifest itself asincontinence or retention.

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 21/49
iagno'i' o$ U#'
+ased on the symptoms both
a clinical diagnosis of a UT' and a dierentiation bet&een lo&er
(cystitis or upper (pyelonephritis UT'
should be made

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 22/49
&olle%ting a 'aple
in adults and older children a mid stream urine(7SU sample usually reliably represents theurine in the bladder.
samples collected from urinary bags orbedpans should not be used to diagnose UT'as they in#ariably &ill be contaminated
the most reliable sample is obtained #ia a
suprapubic puncture urine in bladder 28 hours (any shorter time
&ill increase the risk of false negati#e 9ndings

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 23/49
Clinically signi9cant pathogenconcentrations

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 24/49
iagno'i' o$ U#' 1
o need to do any urinalysis% if afemale patient% &ho does not belong to
any of the risk groups% clearly hasoccasional cystitis based on hersymptoms
Urine microscopy is not usuallynecessary to diagnose cystitis

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 25/49
ym"tomatic"atient
Uncom"icated cystitisin a woman2
no risk factorsnot a rea"se
Ty"ica sym"toms2
3 # infections 4 year2
"atient famiiar withher iness
5acteria cuture26on the s"ot6 testingto confirm diagnosis
tarttreatment'ased onresuts
7nti'ioticthera"y
4e'
/o
/o
4e'
8iagnosis agorithm
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 26/49
iagno'i' o$ U#' 2
+acterial culture of urine should be carried out in allcases, ecept in uncomplicated cystitis, e#en thoughthe results &ill not be a#ailable &hen medication iscommenced )+*
'n early pregnancy bacterial culture should be carried out inall pregnant women if only to diagnose asymptomaticbacteriuria )/*
'n adult febrile infections &ith generalised symptoms% and in children&s infections, C"reacti#e protein ('(concentration abo#e 8+ mg:l is suggesti#e of a kidneyinfection )'*

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 27/49
A'!ptoati% "a%teri+ria
esults of urine culture have repeatedlyshown
bacterial growth above 10 bacteria )cfu*2ml
possible pyuria does not aect interpretation
if se#eral bacterial strains are gro&n on culture6contamination of the sample is the likely cause
in#estigations and treatment of asymptomaticbacteriuria should be instigated only in pregnant&omen

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 28/49
Antimicrobial therapy in UT's ;
/cute uncomplicated cystitis$ / patient &ith typical symptoms% not belonging to any of the
risk groups% is treated &ithout laboratory in#estigations
/ if the symptoms are atypical% a strip test urinalysis may becarried out to support diagnosis
/ if the strip test is negati#e% the urine should be culturedand other reasons for the symptoms should be considered
/ 3irst choices$
/ trimethoprim for 3"- days
/ nitrofurantoin for -"< days or
/ pi#mecillinam for -"< or 3 days

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 29/49
Antii%ro"ial therap! in U#' 2
eserve drugs$
4uinolones (nor$o!acin% o$o!acin or cipro$o!acin for 3 days
/ if 9rst choice drugs are not suitable or
/ if the infection has not responded to 9rst choice drugs or
/ recurrent infection &ithin 8 &eeks
/ if there is a relapse% urine must be cultured and thetreatment should be continued for < days
'n special cases0
/ cefalein or cefadroil for - days (if the abo#e arecontraindicated
/ sulphatrimethoprim )567-T6* for 3 days (particularly ifthe le#el of infection is unclear
/ amoicillin for - days (particularly in enterococcalinfections
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 30/49
Single-do'e therap!
single"dose therapy is slightly less eecti#e thancon#entional therapy
eecti#e in infections caused by E. coli % but less soin S. saprophyticus infections
recommended particularly &hen practical reasons&arrant its use (e.g. self"care
=reparations0
/ phosphomycin 3 g
/ nor8oacin *++ mg
/ cipro8oacin -++ " <-+ mg
/ o8oacin 5++ mg as a single dose
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 31/49
reatent o$ p!elonephriti'
Uncomplicated pyelonephritis$
A pyelonephritis patient &ho is not unduly ill can be looked after at home )'*
Treatment &ith either a 8uoro9uinolone or
sulphatrimethoprim orally for 10-1: days
reatment o pye onep r t s

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 32/49
reatment o pye onep r t s5
An un&ell pyelonephritis patient &ith or &ithout hightemperature should be admitted to hospital
in hospital the treatment is commenced &ithcefuro!ime i.#. +.<-";.-g e#ery * hours or &ith an
$uorouinolone orally it is usually possible to change o#er to oral medication&ith 9rst"generation cephalosporins in 5"3 days% &henresponse to treatment is ob#ious
third"generation cephalosporins are usually not
recommended for the treatment of uncomplicatedpyelonephritis% but ceftria!one may be chosen as theinitial therapy% if either once a day or intramuscularadministration are considered bene9cial
aminoglycosides ha#e sho&n no additional bene9tso#er other forms of treatment

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 33/49
reatent d+ring pregnan%!
+acteriuria during pregnancy is associated with
increased ris" of premature labour andpyelonephritis
/ asymptomatic bacteriuria and cystitis are treated inthe same &ay
/ single"dose treatment is not recommended
/ drugs of choice
nitrofurantoin <- mg t&ice daily for - " < days or
beta"lactamase (mecillinam, amoicillin or 9rst"
generation cephalosporins for - > < days.
/ due to foetal risk 8uoro9uinolones should beavoided during the &hole of pregnancy% and 567-
T6 during the latter part of pregnancy

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 34/49
ower U#' in %hildren
treatment principles are the same as for adults
little e#idence to support short term treatment inchildren )'*
drugs of choice
/ nitrofurantoin - mg:kg:day or
/ trimethoprim * mg:kg:day
/ treatment to continue for - days )'*

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 35/49
ro"a"le lower U# with generali'ed
'!pto' in %hildren
treated so that any possible infection of the kidney is alsoco#ered% i.e. &ith antibiotics &ith high tissue penetrability
oral medication acceptable
drugs of choice
/ sulphatrimethoprim (trimethoprim * mg:kg:day / cefalein 3+ " -+ mg:kg:day in 3 di#ided doses
/ cefuroime aetil 5+ mg:kg:day in 5 di#ided doses or
/ mecillinam 5+ " 8+ mg:kg:day in 3 di#ided doses
/ treatment to continue for < days )'*
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 36/49
reatent o$ p!elonephriti' in %hildren
all infants with febrile UTI should be admitted tohospital
drugs of choice
/ cefuroime (;++ mg:kg:day in 3 di#ided doses or
/ ceftriaone (*+ mg:kg:day daily / intra#enous therapy until ob#ious response
/ &hen ob#ious response to treatment is obser#ed%medication is changed o#er to oral until the total
course of treatment% i.e. ;+ days% is completed
follo&"up treatment according to culture and sensiti#ityresults% &ith an antibiotic &ith good tissue penetrability
(e.g. sulphatrimethoprim or a cephalosporin

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 37/49

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 38/49

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 39/49
U#' in en
a UT' in men can be associated &ith either acute orchronic bacterial prostatitis
prostatitis or epididymitis may play a partparticularly in febrile UT'
it is ad#isable to palpate both the prostate andscrotum
chronic bacterial prostatitis% or at least the retentionof bacteria in the prostatic ducts% should besuspected in relapses &ith the same causati#ebacteria
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 40/49
U#' in en 2
/febrile lower urinary tract infection in men$
if the infection is not associated &ith urinary stricture orprostatitis%it is treated &ith the same drugs as cystitis in&omen% but the treatment should continue for ; - 10 days
nitrofurantoin should not be used in men as adeuateprostatic concentrations are not achie#ed )<*
3ebrile urinary tract infection in men is treated &ith
a long course of antibiotics &ith good prostatic and epididymalpenetration
9rst choice0 a 8uoro9uinolone for 5 &eeks

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 41/49
UT's in men 3
UTI in men associated with acute bacterialprostatitis
treatment for 8 " ? &eeks (depending ho& uicklypatient responds to treatment
to be follo&ed up &ith lo& dose prophylais &ithe.g. trimethoprim or nitrofurantoin
'hronic bacterial prostatitis
recurrent UT's and calci9cations in prostate oral 9uinolones for 5 > 3 months )<*
to be follo&ed up &ith prophylactic medication

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 42/49
reatent o$ U# in dia"eti%'
'ystitis in diabetics drugs of choice for initial treatment are same as for
uncomplicated UT'
antibiotic treatment must always be based on the resultsof urine culture
treatment to continue for < days
/cute pyelonephritis in diabetics
treatment is the same as for uncomplicated pyelonephritis
consider urological imaging earlier than normal% if there is noresponse to appropriately chosen medication
the causati#e agents of recurrent UT's in diabetics are oftenunusual% resistant microbes (species of pseudomonas%enterococci and enterobacter and #arious candida species.

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 43/49
roph!lai' o$ re%+rrent %!'titi' with
antii%ro"ial agent'
prophyla!is should be considered &henmore than ! infections per year
prophyla!is to continue for ? months if infections recur after prophylactictreatment% the prophyla!is is re"commenced for ? > ;5 months )<*

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 44/49
r+g' o$ %hoi%e in U# proph!lai'
3irst choice$
trimethoprim ;++ mg in the e#enings nitrofurantoin -+ " <- mg in the e#enings
5econd choice$
methenamine hippurate ; g t&ice daily
nor$o!acin 5++ mg daily or on 3 e#enings per &eek
nitrofurantoin (not if serum creatinine is abo#e ;-+ @mol:l
uinolones (in cases &here there is no response &ith otherprophylactic medication or tolerance to other medications ispoor
<uring pregnancy$
nitrofurantoin -+ mg daily or
methenamine hippurate ; g daily for the rest of the pregnancy
particularly if recurrent bacteriuria is diagnosed in earlypregnancy
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 45/49
edi%ation to "e ta7en a$ter inter%o+r'e
A single"dose prophyla!is taken after intercourse iseecti#e
in &omen &hose UT's are clearly associated &ith se!ual
intercourse )/*
3irst choice$
/ trimethoprim ;++"3++ mg as a single dose
/ nitrofurantoin -+"<- mg as a single dose
5econd choice$ / nor$o!acin 5++ mg% o$o!acin ;++ mg orcipro$o!acin ;++"5-+ mg
/ sulphatrimethoprim (; single"strength tablet
Th i li i i f
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 46/49
The main uality criteria forthe treatment of UT's
urine sample to be collected appropriately &heninfection is suspected
unnecessary culturing of urine samples to be
a#oided the in#estigation and treatment of asymptomatic
bacteriuria to be reser#ed for risk groups
diagnosing structural anomalies of the urinarytract in children
rational use of antibiotics
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 47/49
Antii%ro"ial therap! in a''o%iation with
a +rinar! %atheter 1
the treatment of UTI in a catheterisedpatient should always be based onthe identity and sensitivity of the
causative microbe the catheter should al&ays be remo#ed% at
least for the duration of treatment% asother&ise the bacteria &ill not be
eradicated if this is not feasible% the recommendation
is to continue treatment for < " ;+ dayse#en in lo&er UT's

7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 48/49
Antii%ro"ial therap! in a''o%iation
with a +rinar! %atheter 2
In the following patient groups antibiotics can preventserious
infective complications caused by long-termcatheterisation $
after renal transplant (for 3 months granulocytopenic patients and
possibly in diabetics
it is recommended that drugs &hich could be of bene9t inserious infections (beta"lactamases and $uorouinolones are
not used for prophyla!is/ntibiotic prophylais is not recommended$
for repeat catheterisations
for the insertion of long"term catheter
for pyuria and bacteriuria in a patient &ith a long"term
catheter but no ob#ious infection
Antimicrobial therapy in association &ith a
7/25/2019 ipd_(Slide Tahun Lalu) Isk
http://slidepdf.com/reader/full/ipdslide-tahun-lalu-isk 49/49
Antimicrobial therapy in association &ith a
urinary catheter 3
3ungal bladder infection in a catheterised patient$
systemic 8ucona=ole is slightly more eecti#e thantopical amphotericin +
remo#al of the catheter &ill impro#e the eradication ofthe microbe during therapy
5uprapubic catheter$
its use is associated &ith a lo&er incidence ofbacteriuria in postoperati#e care
any infections are treated as any other infectionsassociated &ith urinary catheters