Embed Size (px)
Citation preview

About Mediware
+ Rehabilitation and Respiratory Care Division + 25+ years in business
+ Specialists – Knowledge & Experience
+ Acute, IRF, SNF, LTAC, Home + Outpatient Rehab + Respiratory
+ Solution – MediLinks + Compliance + Outcomes + Revenue + Efficiency
+ ONC Meaningful Use – Stage 2 + ICD-10 Prepared
Chandler, AZ headquarters

Why MediLinks for IRF is Gold!
+ Documentation and Workflow Specific To IRF requirements
+ Improve compliance, patient and financial outcomes and efficiency
+ Pre-Admission / Post-Admission / Therapy Evaluations – Real-time reporting
+ Billing is a by-product of Documentation – Increase Charge Capture & Revenue
+ FIM Scoring Integrity – Results = Improved Revenue Accuracy
+ IRFPAI Integration – Automated to select appropriate FIM scores
+ 3 hour rule compliance – Monitor 3/5 or 15/7 real-time
+ Interdisciplinary Plan of Care – Common view/document to meet CMS regulations
+ Goals Management – Short/Long Term goals - patients barriers to discharge
+ Task list - Data driven watch-dog custom for each user

Complementing Hospital Information Systems
Pre-built HL7 Interfaces • ADT In
• Orders In/Out
• Results In/Out
• Billing Out
• Narrative In/Out
• Scheduling In/Out
Experience with all HIS
Improved Workflow
MEDITECH

IRF PPS FY 2015
Final Rule 42 CFR Part 412 [CMS-1608-F]
Darlene D’Altorio-Jones, PT, MBA-HCM
Senior Consultant, Strategist

2015 IRF Final Rule
+ Attendee will recognize standard payment and adjustments proposed for 2015 Federal Fiscal Year (FFY) along with impact from 2014 changes.
+ Attendee will understand how the areas for presumptive compliance has changed; & how data will be captured in the future (IRF PAI capture) to help delineate presumptive compliance
+ Attendee will become familiar with areas of change to the IRF PAI; from 3 to 8 pages beginning 10/1/2014
+ Attendee will be exposed to quality reporting changes for the 2015 year and recommendations for future years
+ Attendee will understand impact of proposed changes to future tracking of therapy services
+ Attendee will receive valuable links to download files and information on how to comment toward final rule considerations.

CMS – 1608 - F
+ http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/List-of-IRF-Federal-Regulations.html

IRF PPS = IRF PAI Data Set Guides Payment
IRF PAI DATA TOOL – Drives CMI DETERMINATION – 353 Possibilities
Impairment Group Codes
(Condition)
Special Codes that identify the main reason for rehab clinical condition –
subsets of RIC
Rehabilitation Impairment
Categories
(RIC)
21 - Major Diagnostic Divisions of which 13 have capacity to declare
REHAB intensive (60% rule). There are 87 ‘levels’, each with 4 tiers
reflect resource expectations to manage the pt. Stroke 10 levels each with 4
tiers = 40 different payment types. LEVELS equate to Case Mix Groups (CMG) –
353 includes the 5 special CMG’s. Together (tier + CMG) = HIPPS code. This
code with date of transmission to CMS is transferred to the
UNIFORM BILL.
Functional Measurement
& Assignment of Case
Mix Groups
Functional assessment based on 17 of the 18 items measured –
determined within 3 days of admission (excludes tub/shower
transfers); 85% of CMG acuity (Case Mix Index – CMI) is driven
by MOTOR SCORE alone, some reference age &/cognition to
drive payment.
Co-morbidities
(4 Tiers)
A condition secondary to principal diagnosis; represents resource costs to
manage patient above & beyond expected conditions within that level.
5 SPECIAL CMG’s Special conditions / short stays – patient expiration codes

Payment Component Impacts
FACILITY and FEDERAL Adjustments – Annually
• Case Mix Indices include:
• Wage, Labor Share
• Budget Neutrality
• Rural or Urban Location Status
• ACA Amendments (Accountable Care Act Amendments) & other rules
• LIP Adjustments
• Teaching Status
• Teaching hospitals add steps 11 – 16.
• Acknowledge variations in costs of care that is not specifically
represented in IRF PAI data aggregation alone. Participation in
Quality Data reporting prevents a 2% reduction to your base
payment formula.

2015 FORMULA – Standard Payment
+ 2014 to 2015 Change
+ $14,846 to $15,198

Impact for Non-Participation QRP
+ Non-participation conversion factor (Starts fresh – not a cumulative penalty)
+ 2013 Calendar year of Non-Participation
+ 2% Payment Reduction based on 2015 Market Basket Value
+ - $297 less payment per 1.0 CMI treated or $14,901
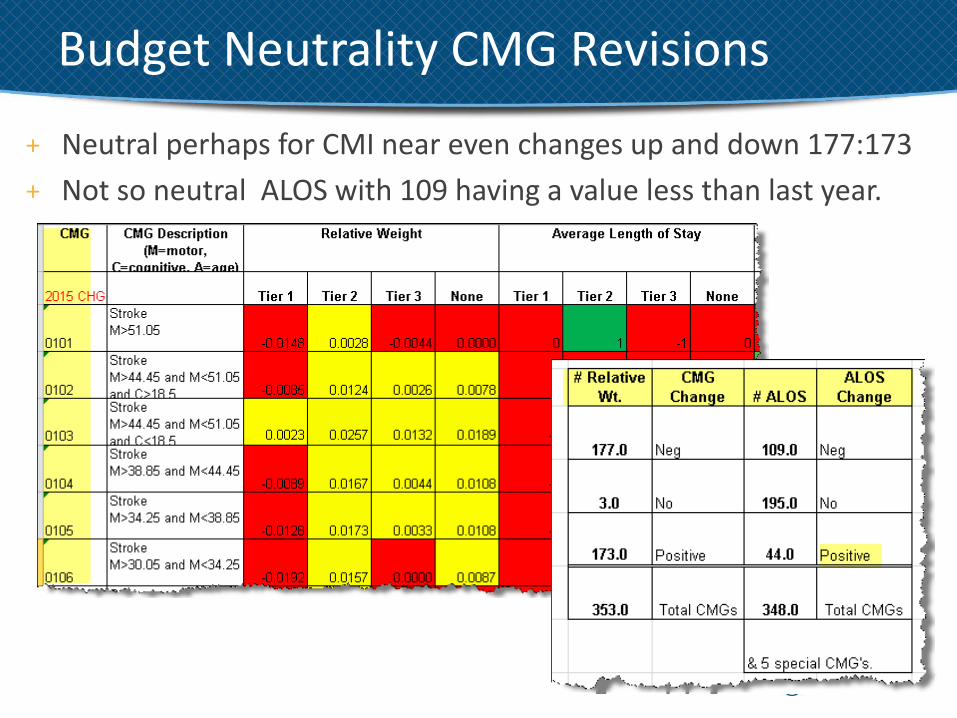
Budget Neutrality CMG Revisions
+ Neutral perhaps for CMI near even changes up and down 177:173
+ Not so neutral ALOS with 109 having a value less than last year.

Standard Payment & Facility Adjustment Formula
Facility-Level Adjustment Factors at FY
2015 Levels.
A0110:
$ 15,198.00
X 2.1425
$ 32,561.72
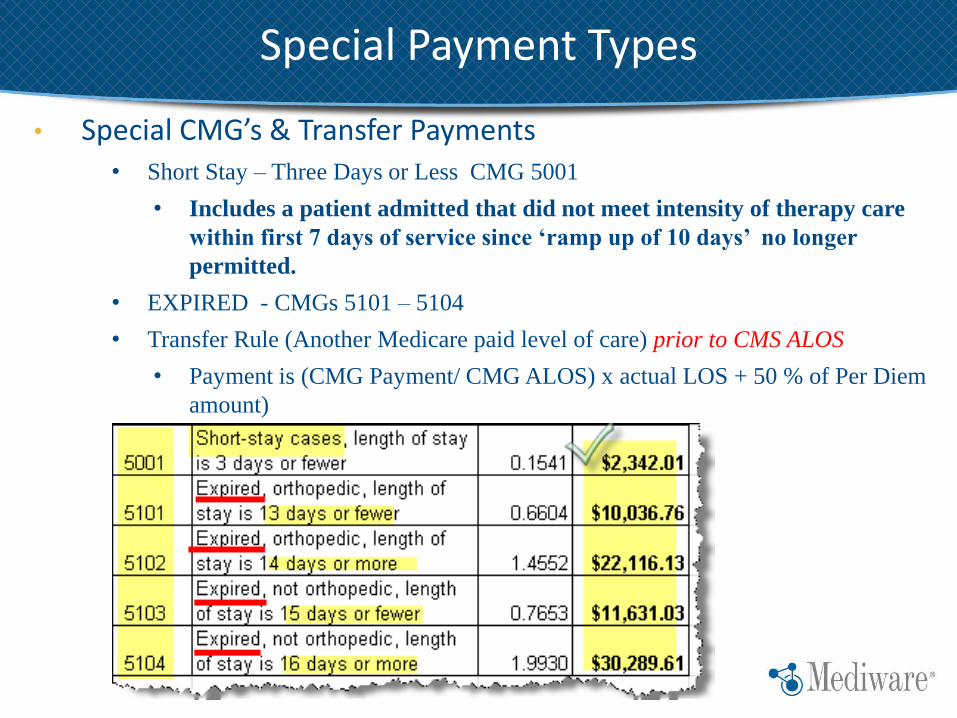
• Special CMG’s & Transfer Payments • Short Stay – Three Days or Less CMG 5001
• Includes a patient admitted that did not meet intensity of therapy care
within first 7 days of service since ‘ramp up of 10 days’ no longer
permitted.
• EXPIRED - CMGs 5101 – 5104
• Transfer Rule (Another Medicare paid level of care) prior to CMS ALOS
• Payment is (CMG Payment/ CMG ALOS) x actual LOS + 50 % of Per Diem
amount)
Special Payment Types

• Medicare Claims Processing Manual: Chapter 3, Section 140.3
? Tolerating Intensive Therapy Week # 1 !!!

• Outlier threshold in 2014 was $9,272
CMS updated the 2015 outlier threshold amount to $8,848 to maintain estimated outlier payments at approximately 3 percent of total estimated aggregate IRF payments for FY 2015.
• FY 2015, we estimate a national average CCR of 0.569 for rural IRFs, by taking an average of the CCRs for all rural IRFs using recently submitted cost report data.
• Estimate a national average CCR of 0.443 for urban IRFs, by taking an average of the CCRs for all urban IRFs using most recently submitted cost report data.
Outlier Payments & Cost to Charge Ratio’s 2015

• Specifically, to be classified for payment under Medicare’s IRF prospective payment system, at least 60 percent of a facility’s total inpatient population must require IRF treatment for one or more of 13 conditions listed in 42 CFR 412.29(b)(2).
• SURVEY Excluded IRF PPS Unit Criteria and worksheet:
• http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/som107ap_a_hospitals.pdf
Presumptive Compliance 60% Rule

• There are 1,029 Diagnosis ICD-9 codes that meet presumptive compliance.
• Translated to ICD-10 and specificity general equivalent mappings (GEMS), that would be 4,035 codes that enable presumptive coding for 60% IRF Rule criteria.
• http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/Data-Files.html
Presumptive ICD-9’s and ICD-10 Codes

• PREVIOUSLY • 28 codes
• October 2014
(2015 Rule) • 16 codes
• (3 with age criteria)
• 12 CODES that were PREVIOUSLY without exclusions NOW have exclusions making it more difficult to meet COMPLIANT IGC’s!
Presumptive IGC’s Without Exclusions
Proposed
FINAL

• CODES removed from Presumptive Compliance Criteria (automatic)
Amputation Codes not Presumptively Compliant
CMS states that:
• Only 2 percent of all IRF patients are currently coded with these diagnoses or 0.3 percent of the time to meet the rule criteria.
• The removal of these codes from the presumptive compliance method does not necessarily mean that a patient with one of these diagnosis codes cannot be included in the IRF’s population that meets the 60 percent rule = MANUAL MEDICAL REVIEW determination
Eliminating Amputation Codes from Presumptive Compliance

2004 Changed eligible conditions removing poly arthritis and replacing it with three more descriptive conditions; 1.) Active Polyarticular, 2.) Systemic Vasculidities, 3.) Severe or advanced osteoarthritis. These were each described as having to have significant functional impairment of gait and ADL’s. Each of these conditions must also have not shown improvement after an appropriate sustained course of outpatient therapy just immediately preceding the rehabilitation admission. Because the facts of these requirements would only be discovered on a retrospective chart audit. CMS felt that the factors indicating these conditions were met requires some disclosure to enable conditional application of the rule. (Future IRF PAI information)
CONDITIONAL COMPLIANCE ??

• PROPOSED 24 A. to be added to the IRF PAI to help VALIDATE conditions for Presumptive Compliance and reduce need for manual audits.
FUTURE IRF PAI – 2016 PROPOSED

• CMS stated that a patient’s need for intensive inpatient rehabilitative services for the treatment of one or more of these conditions would depend on the presence of additional comorbidities that caused significant decline in his or her functional ability to an extent that would necessitate treatment in an IRF.
• If the patient has one or more of the comorbidities on the list of “ICD-9-CM Codes that Meet Presumptive Compliance Criteria,” then the patient would already qualify as meeting the presumptive compliance criteria.
When Might These Be Included?

• Payment tier based on the patient’s comorbidities
• Presumptive compliance method, whether an IRF presumptively meets the 60 percent rule requirements in §412.29(b).
When Federally Mandated: ICD-9-CM to ICD-10-CM, conversion will use the General Equivalence Mappings (GEMs) developed as a tool to assist in these conversions.
ICD -10 WHEN?

IRF PAI Changes as Noted
Final Rule 2015

NON-Quality related IRF PAI changes – Effective October 1st, 2014 (2015 RULE)
The following will be amended items in the IRF-PAI:
● Item 15A: Admit From (Formerly item 15)
● Item 16A: Pre-Hospital Living Situation (Formerly item 16)
● Item 44D: Patient’s Discharge Destination/Living Setting
(Formerly item 44A) Each will be the following listed options:
● 01- Home (private home/apt., board/care, assisted living, group home)
● 02- Short-term General Hospital
● 03- Skilled Nursing Facility (SNF)
04 – Intermediate Care
06 Home under care of organized home health
● 50- Hospice (home)
51 Hospice (institutional care)
61 Swing Bed
● 62- Another Inpatient Rehabilitation Facility
● 63- Long-Term Care Hospital (LTCH)
● 64- Medicaid Nursing Facility
● 65- Inpatient Psychiatric Facility
● 66- Critical Access Hospital
● 99- Not Listed
IRF PAI Data Field Changes –10/2014

• Added the following status code options, which are equivalent to the options on the UB-04 claim/billing form
15A: Admit From & 16A: Pre-hospital Living Setting; and 44D:
Patient’s discharge destination/living setting:
• 04- Intermediate Care Facility
• 06- Home under care of organized home health service organization
• 51- Hospice (Institutional Facility)
• 61- Within institution to swing bed
IRF PAI Data Field Changes – 10/2014

Item 20 A & 20 B: Primary and Secondary Source of Payment -
● 02- Medicare- Fee for Service
● 51- Medicare- Medicare Advantage
● 99- Not Listed
Following Items Added:
● Item 25A: Height (To make presumptive compliance BMI decision based on IRF PAI)
● Item 26A: Weight (To make presumptive compliance BMI decision based on IRF PAI)
● Item 24: Comorbid Conditions (15 additional spaces)
● Item 44C: Was the patient discharged alive?
● Signature of Persons who ‘collected or coordinated collection of this information on dates specified.’ Collection of Data and Submission of Data
IRF PAI Data Field Changes –10/2014

Deleted the following items from the IRF-PAI:
● Item 18: Pre-Hospital Vocational Category
● Item 19: Pre-Hospital Vocational Effort
● Item 25: Is patient comatose at admission?
● Item 26: Is patient delirious at admission?
● Item 28: Clinical signs of dehydration
Technical corrections at items 44D, 44E and 45 to conform to the additions above. Added language to these items indicating that the question can be skipped depending upon how item 44C (discharged alive) is answered: to help reduce errors.
Quality vs Non-Quality IRF PAI Changes – Oct 2014

• Signature page for person(s):
“that I collected or coordinated collection of this information on the dates specified.”
Quality vs Non-Quality IRF PAI Changes – Oct 2014

Quality Initiatives

• Although the IRF PAI was enlarged – NOT all sections are MANDATORY.
• Review the training materials provided after the day long 05/12/2014 Quality Seminars
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/index.html

2015 – IRF PAI Manual Updates

Claims DATA Extracted
IRF PAI DATA Extracted
NHSN – CDC hosted software - Extracted
Quality Data – 3 Camps of Collection

INDICATORS:
1.) Catheter-Associated Urinary Tract Infection (CAUTI) for Intensive Care Unit Patients (NQF#0138). Collected by the CDC via the NHSN.
2.) Percent of Residents with Pressure Ulcers That Are New or Worsened (Short-Stay) (NQF #0678). However, “Quality Indicator” section of the IRF-PAI did not contain the data elements that would be needed to calculate a risk-adjusted quality measure. Collected on IRF PAI.
3.) Influenza Vaccination Coverage among Healthcare Personnel (NQF #0431) 2014 Rule currently collected by the CDC via the NHSN. (Through May 15th of each year)
October 1, 2014

INDICATORS Continued:
4.) All-Cause Unplanned Readmission Measure for 30 Days Post-Discharge from Inpatient Rehabilitation Facilities. Collected in CMS data mining capabilities. NQF #2502, Review Pending
5.) Percent of Residents or Patients Who Were Assessed and Appropriately Given the Seasonal Influenza Vaccine (Short-Stay) (NQF #0680); collected by the CDC via the NHSN. (Through March 31st, each year.) The revised IRF-PAI will become effective on October 1, 2014 so that data elements require this reporting via the IRF PAI will then be available.
October 1, 2014

• Begins 10/1/2014
Addition to IRF PAI Reporting

Begins on or after January 1st, 2015 (as all NHSN indicators are reported in a calendar year).
• Facility Wide Inpatient Hospital-Onset Methicillin-Resistant Staphylococcus Aureus (MRSA) Bacteremia Outcome Measure (NQF #1716)
• Facility Wide Inpatient Hospital-Onset Clostridium Defficile Infection (CDI)
• CMS very interested in ownership of infection. Detail to determine whether ‘present on admission’ or obtained as a result of care within a given facility.
Added Requirement NHSN Reporting

• IRFs that do not submit the required quality measure data will receive a two percentage point reduction to their annual payment update (APU) for the applicable payment year.
• Generally 2 year post applied – but not cumulative.
• Data mandated in 2013 – Reduction payment enforced in Fiscal Year 2015
• http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/Reconsideration-and-Disaster-Waiver-Requests.html
If You Choose NOT to SUBMIT QUALITY DATA

• Monitoring Compliance to Participation:
• % compliance in reporting and in Payment Adjustment Considerations 2016 and after:
• 100 percent threshold for data collected and submitted through the CDC’s NHSN.
• 95 percent for the quality indicator items on the IRF-PAI, as there has to be some margin for error related to IRF patients that have been discharged emergently or against medical advice, as these situations make it more difficult to collect and submit the mandatory IRF-PAI quality indicator items at discharge.
Threshold Definitions - Future

FY annual increase factor:
• a data completion threshold of 95 percent for those mandatory data elements collected using the quality indicator items on the IRF-PAI and submitted through QIES;
• A second data completion threshold of 100 percent for quality measure data submitted through the CDC’s NHSN.
• Data accuracy validation threshold of 75 percent, to avoid a 2 percentage point reduction to their applicable FY annual increase factor.
Validation of Quality Data

• CMS is proposing a validation of records process to randomly check accuracy of data submitted against medical records.
• 260 providers will be randomly be selected for validation, CMS proposes to request 5 charts from each selected provider for a total cost of $47,320 for all IRF providers, or $182.00 for any randomly selected IRF provider.
Validation – Random Selection Compliance Audit

Future Measures under IRF Reporting Consideration:
Stay Tuned – Provide a Voice

2015 Quality Initiatives – IRF PAI Reported

NHSN & IRF PAI – Collection Schedules

Pt. Influenza Measure – Time Schedule

• Critical instructions say ‘vaccine given in YOUR FACILITY’… means ONLY the IRF designated unit. Acute care is NOT your facility in this definition – they are at the ‘acute care unit’ prior to the IRF ADMISSION.
Influenza – Pt. (New 2015)

*The 3rd and 4th FY quarters (which consist of 04/01 to 06/30 and 07/01 to 09/30 respectively), technically fall outside the influenza vaccination season (IVS) which has been defined by the CDC as being 10/01 to 03/31 each year.
*Does an IRF have to perform a full influenza screening on each patient outside of the IVS? NO…
• Scenarios in which IRFs are required to submit full influenza vaccination screening data on the IRF-PAI between 04/01 and 09/30 (outside the IVS): ■ Patients admitted before the start of the IVS on 10/01, but
discharged during the IVS (10/01 to 03/31);
■ Patients admitted prior to 03/31 (before the end of the IVS), but not discharged until 04/01 or after (after end of the IVS);
2015 Quality Initiatives – Pt. Influenza

2015 Quality Initiatives – Healthcare Worker Influenza - Continued

• http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/Training.html
2015 Quality Initiatives

IRF PAI Version 1.2
http://www.cms.gov/Medicare/Medicare-Fee-for-
Service-Payment/InpatientRehabFacPPS/IRFPAI.html

• Unhealed Ulcers
• Stage I
• Stage 2
Quality Related IRF PAI Changes

• Unhealed Ulcers
• Stage 3
• State 4
Quality Related IRF PAI Changes

• UnStageable
• Dressing
• Slough
• Deep Tissue Injury Suspected
Quality Related IRF PAI Changes

• Pressure Ulcer RISK FACTORS PRESENT
• PVD
• PAD
• DM
• Diabetic Retinopathy
• Diabetic Nephropathy
• Diabetic Neuropathy
• Patient offered Influenza Vaccinations
Quality Related IRF PAI Changes

• 5 PAGE items sheet showing Voluntary vs. Mandatory ITEMS:
• http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/index.html
Pressure Ulcer Items not all Mandatory

http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/index.html

HELPFUL RESOURCE LINKS

PUBLIC REPORTING (2010 discussed)
+ CMS has not established procedures or timelines for public reporting of data, but they intend to make the public aware of a future strategy.
+ CMS welcomes public comments on what they should consider when developing future proposals related to public reporting.

• CMS believes that HIE (health information exchange) and the use of certified EHR technology by IRFs (and other providers ineligible for the Medicare and Medicaid EHR Incentive Programs) can effectively and efficiently help providers improve internal care delivery practices, support management of patient care across the continuum, and enable the reporting of electronically specified clinical quality measures (eCQMs).
EHR Certification Considerations

More information on the identification of EHR certification criteria and development of standards applicable to IRFs can be found at:
• http://healthit.gov/policy-researchers-implementers/standards-and-certificationregulations
• http://www.healthit.gov/facas/FACAS/health-it-policy-committee/hitpcworkgroups/certificationadoption
• http://wiki.siframework.org/LCC+LTPAC+Care+Transition+SWG
• http://wiki.siframework.org/Longitudinal+Coordination+of+Care
Links EHR

• CMS will begin collecting therapy minutes total time by treatment TYPE by discipline for individual, group Concurrent and co-treatment.
• Based on the patients 7 day cycle not the entire stay average which will make this a more complex exercise and will also allow them to see 3 hour rule compliance.
• They are looking to see TOTAL Minutes met in ‘week 1’ to most likely to apply the 5001 CMG if ‘not tolerating the required 900 minutes of intensive services since exceptions are not allowed in week one.
• They are then looking to see TOTAL Minutes in week 2 by type. To be defined in the IRF PAI Manual.
What is Proposed for 2016?
2016 REQUIREMENT to begin 10/1/2015 FY.
• Per CMS, In January 2002, Medicare began reimbursing IRFs using a set prospective payment amount that was intended to cover the costs of all treatment and services, including therapy.
• CMS feels this increased the financial incentives for IRFs to give patients more Group Therapy.
• In fact, Mediware released this blog when they heard a CMS representative discussing their speculations at the spring AMRPA conference in March. ■ http://www.mediware.com/rehabilitation/blog/item/if-this-is-
you-you-better-stop-groups-have-defined-purpose
Therapy 3 Hour Rule – Service Type Provided

http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/IRFPAI.html
2014 & 2015 IRF PAI Tools

THANK – YOU
Follow me @
http://www.mediware.com/rehabilitation/blog

• Specialists - Knowledge & Experience
• Acute, IRF & Outpatient Rehab
• Respiratory
• Service 250+ Organizations
Mediware