Embed Size (px)
Citation preview

IRON METABOLISM DISORDERS

ANEMIAANEMIADefinition
• Decrease in the number of circulating ec ease t e u be o c cu at gred blood cells
• Most common hematologic disorder by farfar

ANEMIAANEMIACauses
Blood loss• Blood loss• Decreased production of red blood cells
(Marrow failure)(Marrow failure)• Increased destruction of red blood cells
Hemolysis– Hemolysis
• Distinguished by reticulocyte count– Decreased in states of decreased production– Decreased in states of decreased production– Increased in destruction of red blood cells

ANEMIAANEMIACauses - Decreased Production
• Cytoplasmic production of protein– Usually normocytic (MCV 80-100 fl) or
microcytic (MCV < 80 fl)
• Nuclear division/maturation– Usually macrocytic (MCV > 100 fl)

ANEMIAANEMIACauses - Cytoplasmic Protein Production
D d h l bi th i• Decreased hemoglobin synthesis– Disorders of globin synthesis– Disorders of heme synthesis
• Heme synthesis– Decreased Iron– Iron not in utilizable form– Decreased heme synthesis

IRON DEFICIENCY ANEMIAIRON DEFICIENCY ANEMIAPrevalence
Country Men (%) Women(%)
PregnantWomen (%)
S I di 6 35 56S. India 6 35 56N. India 64 80Latin America 4 17 38Latin America 4 17 38Israel 14 29 47Poland 22Sweden 7USA 1 13

IRON
• Functions as electron transporter; vital for life• Must be in ferrous (Fe+2) state for activity• Must be in ferrous (Fe+2) state for activity• In anaerobic conditions, easy to maintain
ferrous stateferrous state• Iron readily donates electrons to oxygen,
superoxide radicals, H2O2, OH• radicalssuperoxide radicals, H2O2, OH radicals• Ferric (Fe+3) ions cannot transport electrons or
O22
• Organisms able to limit exposure to iron had major survival advantage

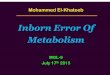
IRONBody Compartments 75 kg manBody Compartments - 75 kg man
StoresStores1000 mg
Tissue170 mg 4 mg
Absorption < 1 mg/day
Excretion < 1 mg/dayg
Red Cells2400 mgg

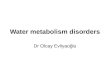
IRON CYCLE
CIRCULATING RBCs
Fe FeFe Fe
ptor
CIRCULATING RBCsMONONUCLEARPHAGOCYTES
Fe FeFeFe FerritinFe
e
Fe
Fe Fe
Ferritin Ferritinerrin
Rec
ep
Fe
Fe
Hemosiderinslow
Fe
Fe Ferritin
Tran
sfe
RBC PRECURSORRBC PRECURSOR
Fe Fe
TRANSFERRIN

INTRACELLULAR IRON TRANSPORTFe+2
Transferrin
Transferrin receptor
H+H+
LH+H+
Lysosome Fe+2

IRONCauses of Iron Deficiency
• Blood Loss– Gastrointestinal Tract– Gastrointestinal Tract– Menstrual Blood Loss– Urinary Blood Loss (Rare)– Blood in Sputum (Rarer)
• Increased Iron Utilization– Pregnancy– Infancy
Adolescence– Adolescence– Polycythemia Vera
• Malabsorption– Tropical SprueTropical Sprue– Gastrectomy– Chronic atrophic gastritis
• Dietary inadequacy (almost never sole cause)C bi i f b• Combinations of above

DAILY IRON REQUIREMENTSDAILY IRON REQUIREMENTSPregnancies
2
2.5
ay)
1
1.5
2
orbe
d Ir
on
men
t (m
g/da
0
0.5
1
Abs
oR
equi
rem
0 2
10 14 20 27 29 32 34 40 49 55 65
Males
0
Age
Males Females

IRON ABSORPTION
12
1416
)
810
12
mg/
day)
2
46
Iron
(
0
2
Iron in Diet IronSolubilized
Iron Uptake Iron Absorbed

GI ABSORPTION OF IRON

FERRITIN/TRANSFERRIN REGULATION

IRON ABSORPTION
100
1
10Iron
Absorbed (mg/day)
0.01
0.1(mg/day)
0 1 1 8 10 20 80 100 2000.1 1 8 10 20 80 100 200Iron Ingested (mg/day)

IRON DEFICIENCY ANEMIAProgression of Findings
St i bl I B M A i t• Stainable Iron, Bone Marrow Aspirate• Serum Ferritin - Low in Iron Deficiency• Desaturation of transferrin• Serum Iron dropsp• Transferrin (Iron Binding Capacity) Increases• Blood Smear - Microcytic Hypochromic;• Blood Smear - Microcytic, Hypochromic;
Aniso- & Poikilocytosis• Anemia• Anemia



IRON STORESI D fi i A iIron Deficiency Anemia
StoresStores0 mg
Tissue170 mg 3 mg
Absorption 2-10 mg/day
Excretion Dependent on Cause170 mg
Red Cells1500 mg

IRON DEFICIENCYIRON DEFICIENCYSymptoms
F ti S ti t f ti• Fatigue - Sometimes out of proportion to anemia
• Atrophic glossitis• Pica• Koilonychia (Nail spooning)• Esophageal Web• Esophageal Web

IRONCauses of Iron Deficiency
• Blood Loss– Gastrointestinal Tract– Gastrointestinal Tract– Menstrual Blood Loss– Urinary Blood Loss (Rare)– Blood in Sputum (Rarer)
• Increased Iron Utilization– Pregnancy– Infancy
Adolescence– Adolescence– Polycythemia Vera
• Malabsorption– Tropical SprueTropical Sprue– Gastrectomy– Chronic atrophic gastritis
• Dietary inadequacy (almost never sole cause)C bi i f b• Combinations of above

IRON REPLACEMENT THERAPYResponse
U ll l ll 300 900 /d• Usually oral; usually 300-900 mg/day• Requires acid environment for
absorption• Poorly absorbedy

IRON THERAPYIRON THERAPYResponse
Initial response takes 7 14 days• Initial response takes 7-14 days• Modest reticulocytosis (7-10%)
C ti f i i 2 3 th• Correction of anemia requires 2-3 months• 6 months of therapy beyond correction of
anemia needed to eplete sto es ass minganemia needed to replete stores, assuming no further loss of blood/iron
• Parenteral iron possible but problematic due• Parenteral iron possible, but problematic due to allergic reactions

Hemochromatosis-1• Disease of excess iron uptake• Disease of excess iron uptake• 2% of population has hemochromatosis;
inherited as autosomal dominant• Exists worldwide, but
– Belt across Northern Europe with increased incidenceincidence
• Ireland, Scandinavia, Russia
• Defects can be in DMT-1, more commonly in HFE (genetic defects only really studied forHFE (genetic defects only really studied for northern Europeans)
• Can also have acquired hemochromatosis, f t f i f th illfrom transfusion for other illnesses

Hemochromatosis -2
D f t i HFE d d i• Defect in HFE causes decreased iron uptake by crypt enterocytes
• Leads to increased DMT-1, causing increased iron extraction from diet & increased iron delivery to tissues
• Once iron is absorbed, very difficult to , yremove

Hemochromatosis-3• Sequence of events:• Sequence of events:
– Increased ferritinIncreased transferrin saturation– Increased transferrin saturation• Normal c. 33%; if > 60%, often marker for
disease; if > 90-95%, can start to get free iron
• Increased iron binding to other transport proteins– Albumin
• Iron deposition in tissues, leading to:p , g

Hemochromatosis 4Hemochromatosis-4• Diseases
– Skin darkening• Due to iron deposition in skin causing increased
melanin productionmelanin production– Endocrinopathy
• Diabetes, hypothyroidism, hypopituitarism, yp y , yp p– Liver damage
• Can lead to cirrhosis, hepatocellular CA– Cardiac damage
• Cardiomyopathy leading to congestive heart failurefailure

Hemochromatosis-5
T t t• Treatment– Early recognition– Phlebotomy– Iron chelation – Generally reserved for
f i i d d h h itransfusion-induced hemochromatosis

ANEMIA OF CHRONIC DISEASEFindingsFindings
• Mild, non-progressive anemia (Hgb c. 10, Hct c. 30%30%
• Other counts normal• Normochromic/normocytic (30%• Normochromic/normocytic (30%
hypochromic/microcytic)• Mild aniso- & poikilocytosisp y• Somewhat shortened RBC survival• Normal reticulocyte count (Inappropriately low for y ( pp p y
degree of anemia)• Normal bilirubin• EPO levels increased but blunted for degree of
anemia

ANEMIA OF CHRONIC DISEASECauses
• Thyroid diseaseCollagen Vascular Disease• Collagen Vascular Disease– Rheumatoid Arthritis– Systemic Lupus Erythematosus
Polymyositis– Polymyositis– Polyarteritis Nodosa
• Inflammatory Bowel DiseaseUlcerative Colitis– Ulcerative Colitis
– Crohn’s Disease• Malignancy
Ch onic Infectio s Diseases• Chronic Infectious Diseases– Osteomyelitis– Tuberculosis
F ili l M dit F• Familial Mediterranean Fever

IRON STORESA i f Ch i DiAnemia of Chronic Disease
StoresStores2500 mg
Tissue170 mg 1 mg
Absorption < 1 mg/day
Excretion < 1 mg/day170 mg g
Red Cells1100 mg

IRON CYCLEAnemia of Chronic DiseaseAnemia of Chronic Disease
MONONUCLEARPHAGOCYTESFe Fe
or
CIRCULATING RBCs
Fe FeFeFe Ferritin
F
Fe Fe
F iti Ferritinrrin
Rec
epto
FeHemosiderin
slow
Fe Ferritin Ferritin
Tran
sfer
RBC PRECURSORRBC PRECURSORFe Fe
IL-1/TNF
TRANSFERRIN


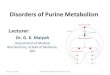
IRON DEFICIENCY versus ACD
S I T f i F itiSerum Iron Transferrin Ferritin
Iron Deficiencyy
ACD

Soluble Transferrin Receptor• Measure of ferrokinetic activity• Measure of ferrokinetic activity• Elevated in iron deficiency
N ll l d i i f• Not usually elevated in anemia of chronic inflammation (not an acute phase reactant)phase reactant)
• Still not widely availableE i• Expensive
• May replace iron binding capacity &/or f itiferritin

SUMMARYSUMMARYIron Metabolism Disorders
• Most common form of anemia• Most common form of anemia• Symptom of pathologic process
P i if i i h l i• Primary manifestation is hematologic• Treatment requires:
– Replacement therapy– Correction of underlying cause (if possible)
• Iron excess more dangerous than iron deficiency