Embed Size (px)
Citation preview

ifJa
PCt
SCCrsDcsTMp
0d
Is Accurate Intravascular Ultrasound Evaluation of the LeftCircumflex Ostium from a Left Anterior Descending to Left Main
Pullback Possible?
Carlos Oviedo, MDa, Akiko Maehara, MDa,*, Gary S. Mintz, MDa, Kenichi Tsujita, MD, PhDa,Takashi Kubo, MD, PhDa, Hiroshi Doi, MD, PhDa, Celia Castellanos, MDa,
Alexandra J. Lansky, MDa, Roxana Mehran, MDa, George Dangas, MD, PhDa,Martin B. Leon, MDa, Gregg W. Stone, MDa, Barry Templin, MBAb, Hiroshi Araki, MDc,
Masahiko Ochiai, MDc, and Jeffrey W. Moses, MDa
Treatment of left main coronary artery bifurcation lesions might depend on the ostial leftcircumflex (LC) or ostial left anterior descending (LAD) disease severity. We sought toevaluate whether intravascular ultrasound assessment of the side branch ostium requiresdirect imaging or is accurate from the main vessel. Our retrospective analysis included 126patients with left main coronary artery bifurcation disease (plaque burden >40% byintravascular ultrasound scanning). We analyzed pullbacks from the LAD and the LC.First, during the main vessel pullback (ie, from the LAD), we evaluated the side branchostium (ie, of the LC). Second, we compared this oblique view with the direct ostialmeasurements during LC pullback. Finally, we repeated this process, imaging the ostialLAD from the LC. From the LAD, the oblique LC ostial lumen diameter was 3.0 � 0.8 mmcompared to the directly measured lumen diameter of 2.9 � 0.6 mm. From the LC, theoblique LAD ostial lumen diameter was 2.9 � 1.1 mm compared to the directly measuredlumen diameter of 2.8 � 0.5 mm. However, Bland-Altman plots showed significant vari-ation in the oblique versus direct comparisons. The 95% limits of agreement ranged from�1.84 to 1.14 mm (mean difference �0.35, SD 0.75) for the LAD and �1.69 to 1.22 mm(mean difference �0.23, SD 0.73) for the LC. The “oblique view” detection of any plaquein the side branch predicted 40% or 70% plaque burden with good sensitivity but poorspecificity. In conclusion, intravascular ultrasound evaluation of a side branch ostium fromthe main vessel is only moderately reliable, especially for distal left main coronary arterylesions. For an accurate assessment of the side branch ostium, direct imaging is
necessary. © 2010 Elsevier Inc. All rights reserved. (Am J Cardiol 2010;105:948–954)mtdMMotigdiQ�lLPctisv
aCardiovascular Research Foundation and Columbia University Med-cal Center, New York, New York; bAbbott Vascular, Santa Clara, Cali-ornia; and cShowa University, Northern Yokohama Hospital, Yokohama,apan. Manuscript received October 30, 2009; revised manuscript receivednd accepted November 18, 2009.
This study was a Abbott Vascular (Santa Clara, California)-sponsoredroviding Regional Observations to Study Predictors of Events in theoronary Tree (PROSPECT) study and partnered with Volcano Corpora-
ion (Rancho Cordova, California).Drs. Leon and Stone are the members of the advisory boards for Boston
cientific Corporation, Boston, Massachusetts and Abbott Vascular, Santalara, California. Dr. Mintz is a consultant for Volcano Corporation, Ranchoordova, California. Dr. Moses is a consultant for Boston Scientific Corpo-
ation, Boston, Massachusetts. Drs. Mintz and Maehara received grants/re-earch support from Boston Scientific Corporation Boston, Massachusetts.rs. Mintz, Maehara, and Kubo received grants/research support from Vol-
ano Corporation, Rancho Cordova, California. Dr. Ochiai is a member ofpeakers’ bureau of Boston Scientific Corporation, Boston, Massachusetts. Mr.emplin is an employee of Abbott Vascular, Santa Clara, California. Drs.ehran and Dangas received honoraria for lectures from Boston Scientific Cor-
oration, Boston, Massachusetts and Abbott Vascular, Santa Clara, California.*Corresponding author: Tel: (212) 851-9371; fax: (212) 851-9230.
sE-mail address: [email protected] (A. Maehara).
002-9149/10/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2009.11.029
Percutaneous coronary intervention (PCI) to treat leftain coronary artery (LMCA) lesions might be equivalent
o coronary artery bypass graft surgery, especially in therug-eluting stent era—irrespective of lesion location. TheAIN-COMPARE (Revascularization for Unprotected Leftain Coronary Artery Stenosis: Comparison of Percutane-
us Coronary Angioplasty versus Surgical Revasculariza-ion) registry enrolled 1,102 patients who underwent stentmplantation and 1,138 patients who underwent bypass sur-ery. In the propensity score-matched cohort, no significantifference was found between stenting and bypass surgeryn the risk of death or the composite end point of death,-wave myocardial infarction, or stroke—even though50% of stent-treated patients had distal LMCA bifurcation
esions.1 These findings were supported by the prespecifiedMCA subset analysis from SYNTAX (Synergy betweenCI with Taxus and Cardiac Surgery Trial).2 Althoughoronary angiography has been the reference standard forhe evaluation of coronary artery disease, including select-ng PCI versus surgery and selecting among different PCItrategies, it has many limitations compared to intra-ascular ultrasound (IVUS) evaluations. Intravascular ultra-
ound also has limitations, including artifacts, transducer an-www.AJConline.org
g(smbtivvte(
M
wtisopbcdtgCtpp(NPvith
�c
ioAwdleTgdwo
Fda ents a
TC
V
MAHHDCP
TQ
V
R
M
D
949Coronary Artery Disease/IVUS Study of Ostial Disease
ulation or eccentric location, and anterograde-retrogradesystole-diastole) transducer movement that must be con-idered when interpreting images and making measure-ents. One concern during LMCA PCI is disease of the side
ranch ostium; however, interventionalists have been reluc-ant to perform IVUS scans of both daughter vessels, relyingnstead on an oblique view of the side branch from the mainessel. We considered whether IVUS imaging of the mainessel (typically from the left anterior descending [LAD] tohe LMCA) could reliably assess the lumen dimensions orven the disease extent at the ostium of the side branchtypically the left circumflex [LC]).
ethods
The study consisted of an inclusive group of 126 patientsho underwent diagnostic angiography and preinterven-
ional IVUS assessment of the LMCA bifurcation, includingmaging of the LAD and LC arteries. The patients wereelected if the angiographic findings suggested compromisef the LMCA bifurcation and if IVUS imaging showed alaque burden of �40% in any of the 3 components of theifurcation (distal LMCA, ostial LAD, or ostial LC). Theohort included 45 patients with an acute coronary syn-rome (not attributed to the LMCA) who were enrolled inhe multicenter, prospective, international Providing Re-ional Observations to Study Predictors of Events in theoronary Tree (PROSPECT) trial (ClinicalTrials.gov iden-
ifier no. NCT00180466) and who fit the above criteria. Allatients provided written informed consent. The remainingatients came from Columbia University Medical CenterNew York, New York; n � 48) and Showa Universityorthern Yokohama Hospital (Yokohama, Japan; n � 34).atient demographics were confirmed by hospital chart re-iew at the time of the procedure. The coronary risk factorsncluded diabetes mellitus (controlled by diet, oral medica-ion, or insulin), hypertension (medication-treated only),
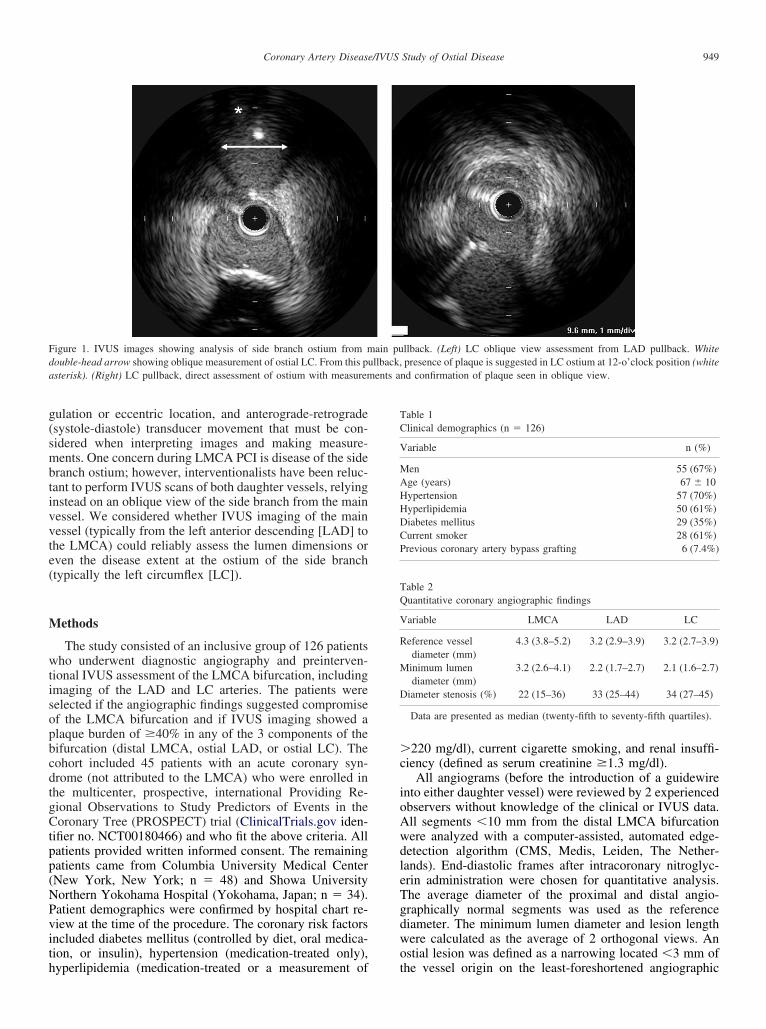
igure 1. IVUS images showing analysis of side branch ostium from mouble-head arrow showing oblique measurement of ostial LC. From this pusterisk). (Right) LC pullback, direct assessment of ostium with measurem
yperlipidemia (medication-treated or a measurement of t
220 mg/dl), current cigarette smoking, and renal insuffi-iency (defined as serum creatinine �1.3 mg/dl).
All angiograms (before the introduction of a guidewirento either daughter vessel) were reviewed by 2 experiencedbservers without knowledge of the clinical or IVUS data.ll segments �10 mm from the distal LMCA bifurcationere analyzed with a computer-assisted, automated edge-etection algorithm (CMS, Medis, Leiden, The Nether-ands). End-diastolic frames after intracoronary nitroglyc-rin administration were chosen for quantitative analysis.he average diameter of the proximal and distal angio-raphically normal segments was used as the referenceiameter. The minimum lumen diameter and lesion lengthere calculated as the average of 2 orthogonal views. Anstial lesion was defined as a narrowing located �3 mm of
llback. (Left) LC oblique view assessment from LAD pullback. Whitepresence of plaque is suggested in LC ostium at 12-o’clock position (white
nd confirmation of plaque seen in oblique view.
able 1linical demographics (n � 126)
ariable n (%)
en 55 (67%)ge (years) 67 � 10ypertension 57 (70%)yperlipidemia 50 (61%)iabetes mellitus 29 (35%)urrent smoker 28 (61%)revious coronary artery bypass grafting 6 (7.4%)
able 2uantitative coronary angiographic findings
ariable LMCA LAD LC
eference vesseldiameter (mm)
4.3 (3.8–5.2) 3.2 (2.9–3.9) 3.2 (2.7–3.9)
inimum lumendiameter (mm)
3.2 (2.6–4.1) 2.2 (1.7–2.7) 2.1 (1.6–2.7)
iameter stenosis (%) 22 (15–36) 33 (25–44) 34 (27–45)
Data are presented as median (twenty-fifth to seventy-fifth quartiles).
ain pullback,
he vessel origin on the least-foreshortened angiographic
pwa
i2Be
ctabmoi
Fo(
TQ
V
LEPME
950 The American Journal of Cardiology (www.AJConline.org)
rojection. Among multiple angiographic projections, theorst angle between the LAD and LC was measured usingprotractor.All studies were performed before PCI after the admin-
stration of 200 �g of intracoronary nitroglycerin using 1 ofcommercially available IVUS catheters (40-MHz catheter,oston Scientific, Natick, Massachusetts, and 20-MHz cath-
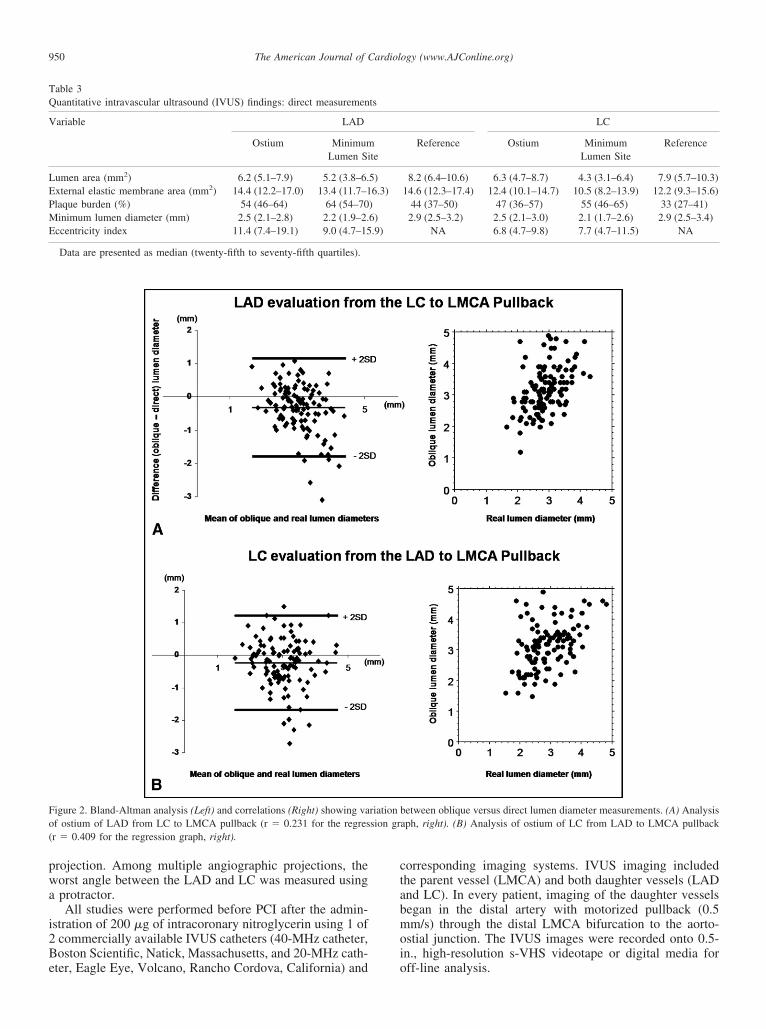
igure 2. Bland-Altman analysis (Left) and correlations (Right) showing vaf ostium of LAD from LC to LMCA pullback (r � 0.231 for the regresr � 0.409 for the regression graph, right).
able 3uantitative intravascular ultrasound (IVUS) findings: direct measuremen
ariable LAD
Ostium MinimumLumen Si
umen area (mm2) 6.2 (5.1–7.9) 5.2 (3.8–6.xternal elastic membrane area (mm2) 14.4 (12.2–17.0) 13.4 (11.7–1laque burden (%) 54 (46–64) 64 (54–70inimum lumen diameter (mm) 2.5 (2.1–2.8) 2.2 (1.9–2.
ccentricity index 11.4 (7.4–19.1) 9.0 (4.7–15
Data are presented as median (twenty-fifth to seventy-fifth quartiles).
ter, Eagle Eye, Volcano, Rancho Cordova, California) and o
orresponding imaging systems. IVUS imaging includedhe parent vessel (LMCA) and both daughter vessels (LADnd LC). In every patient, imaging of the daughter vesselsegan in the distal artery with motorized pullback (0.5m/s) through the distal LMCA bifurcation to the aorto-
stial junction. The IVUS images were recorded onto 0.5-n., high-resolution s-VHS videotape or digital media for
etween oblique versus direct lumen diameter measurements. (A) Analysisaph, right). (B) Analysis of ostium of LC from LAD to LMCA pullback
LC
Reference Ostium MinimumLumen Site
Reference
8.2 (6.4–10.6) 6.3 (4.7–8.7) 4.3 (3.1–6.4) 7.9 (5.7–10.3)14.6 (12.3–17.4) 12.4 (10.1–14.7) 10.5 (8.2–13.9) 12.2 (9.3–15.6)
44 (37–50) 47 (36–57) 55 (46–65) 33 (27–41)2.9 (2.5–3.2) 2.5 (2.1–3.0) 2.1 (1.7–2.6) 2.9 (2.5–3.4)
NA 6.8 (4.7–9.8) 7.7 (4.7–11.5) NA
riation bsion gr
ts
te
5)6.3)
)6).9)
ff-line analysis.
LesLbstcitWdlldspt
iCsitomsvesb
sstaonofamBbrpc2
R
TTt1f
T
wtao
vLmmweim�e�uostatvtt
mimA�dt(
Tdp
Fbpavtsa
951Coronary Artery Disease/IVUS Study of Ostial Disease
The analyzed segments included the distal 10 mm of theMCA and the proximal 10 mm of the LAD and LC. Inach pullback (ie., from the LAD to the LMCA), we mea-ured the ostium of the primary daughter vessel (ie, theAD) directly and the ostium of the side branch (ie, the LC)y (1) measuring its lumen diameter using a line corre-ponding to the smallest lumen diameter after visual inspec-ion and (2) assessing qualitatively the presence of signifi-ant plaque burden (yes/no; Figure 1). We then repeated thismaging process from the LC to the LMCA, with the LC ashe primary daughter vessel and the LAD as the side branch.
e then compared the oblique ostial measurements with theirect ostial measurements that included both the minimumumen diameter and the mean direct lumen diameter calcu-ated from the square root of the lumen area. Finally, weetermined whether the presence or absence of plaque in theide branch (on the oblique view from the main vessel)redicted a plaque burden of 40% and 70% when the daugh-er vessel was imaged directly.
Qualitative and quantitative analyses were done accord-ng to the American College of Cardiology Clinical Expertonsensus Document on Standards for Acquisition, Mea-
urement, and Reporting of Intravascular Ultrasound Stud-es.3 Using planimetry software (EchoPlaque, INDEC Sys-ems, Mountain View, California), the IVUS measurementsf the lumen, external elastic membrane, and plaque andedia (external elastic membrane minus the lumen) cross-
ectional areas and plaque burden (plaque and media di-ided by the external elastic membrane) were performed forach ostium (LAD, LC) and every 1 mm in the selectedegments. The eccentricity index was the maximum dividedy the minimum plaque and media thickness.
Statistical analysis was performed using StatView, ver-ion 5.0 (SAS Institute, Cary, North Carolina). The data arehown as the median and twenty-fifth/seventy-fifth quar-iles. Regression analysis and Bland-Altman assessment forgreement were used to compare the 2 measurement meth-ds. A range of agreement is shown as the mean differe-ce � 2 SDs. The Bland-Altman plot showed the agreementr disagreement between 2 different measurement methodsor the same variable, usually the reference standard versus
new one, using a plot of the difference between theethods against their mean. In the present analysis, theland-Altman plot showed how much the oblique sideranch ostium assessment was likely to differ from the di-ect assessment. If this difference was not enough to causeroblems in clinical interpretation and decision making, weould replace the direct view by the oblique view or use theinterchangeably.
esults
The clinical patient characteristics are listed in Table 1.he results of the quantitative coronary analysis are listed inable 2. The minimal diameter stenosis ranged from 1.2%
o 69.8% for the distal LMCA, 4.2% to 82.7% for the first0 mm of the proximal LAD segment, and 4.7% to 67.8%or the first 10 mm of the proximal LC segment.
The direct measurements for each ostium are listed in
able 3. On IVUS assessment, 201 ostial lesions were found 7ith a directly measured plaque burden of �40% (115 inhe LAD and 86 in the LC), of which 24 ostial LAD lesionsnd 23 ostial LC lesions had a directly measured lumen areaf �4 mm2.
The evaluation of the side branch ostium from the mainessel pullback was possible in all but 1 patient. From theAD, the oblique LC ostial lumen diameter was 3.0 � 0.8m compared to the direct-measured diameter of 2.9 � 0.6m. From the LC, the oblique LAD ostial lumen diameteras 2.9 � 1.1 mm compared to the direct-measured diam-
ter of 2.8 � 0.5 mm. However, Bland-Altman analysisndicated that the 95% limits of agreement between the 2ethods ranged from �1.84 to 1.14 mm (mean difference0.35, SD 0.75) for the LAD oblique versus the direct
valuation and from �1.69 to 1.22 mm (mean difference0.23, SD 0.73) for the LC oblique versus the direct eval-
ation (Figure 2). Although these 2 methods (direct vsblique) provided similar average measurements, we con-idered the range of differences to be clinically important;herefore, we interpreted these data as showing a lack ofgreement between the direct versus oblique view such thathe oblique view should not be used in place of the directiew (or the 2 should not be used interchangeably). Fur-hermore, Figure 2 also shows the poor correlation betweenhe direct and oblique views.
Finally an oblique lumen diameter of �2.3 mm (theean diameter that was equivalent to an area of 4.0 mm2)
ndicated a directly measured minimum lumen area of �4m2, with a sensitivity of 47% and specificity of 86%.mong patients with a confirmed minimum lumen area of4 mm2 using the direct view (n � 47), the oblique view
id not detect plaque in 34.1%; in 53.2% of these patients,he oblique view suggested a lumen diameter of �2.3 mm2
the mean diameter equivalent to an area of �4.0 mm2).The angle between the LAD and LC was 91.3 � 13.6°.
o assess the possible influence of the angle between the 2aughter vessels on the present analysis, we divided theopulation into 2 groups: those with an angle of �90° (n �
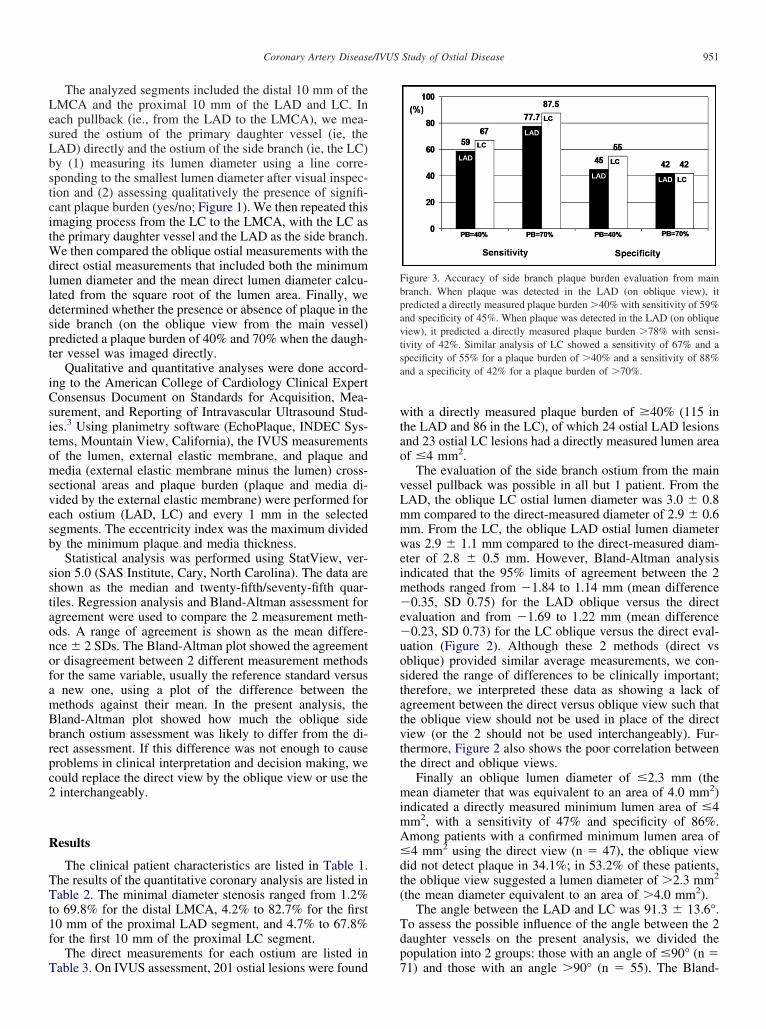
igure 3. Accuracy of side branch plaque burden evaluation from mainranch. When plaque was detected in the LAD (on oblique view), itredicted a directly measured plaque burden �40% with sensitivity of 59%nd specificity of 45%. When plaque was detected in the LAD (on obliqueiew), it predicted a directly measured plaque burden �78% with sensi-ivity of 42%. Similar analysis of LC showed a sensitivity of 67% and apecificity of 55% for a plaque burden of �40% and a sensitivity of 88%nd a specificity of 42% for a plaque burden of �70%.
1) and those with an angle �90° (n � 55). The Bland-
A(Lll
v
dLsHfw
FeF ect mea
952 The American Journal of Cardiology (www.AJConline.org)
ltman analysis showed similar results for both groupsdata not shown). Similarly, the angle between the LAD andC did not affect the sensitivity and specificity of an oblique
umen diameter of �2.3 mm to indicate a directly measuredumen area of �4.0 mm2 (data not shown).
From the main vessel pullback, the oblique side branch
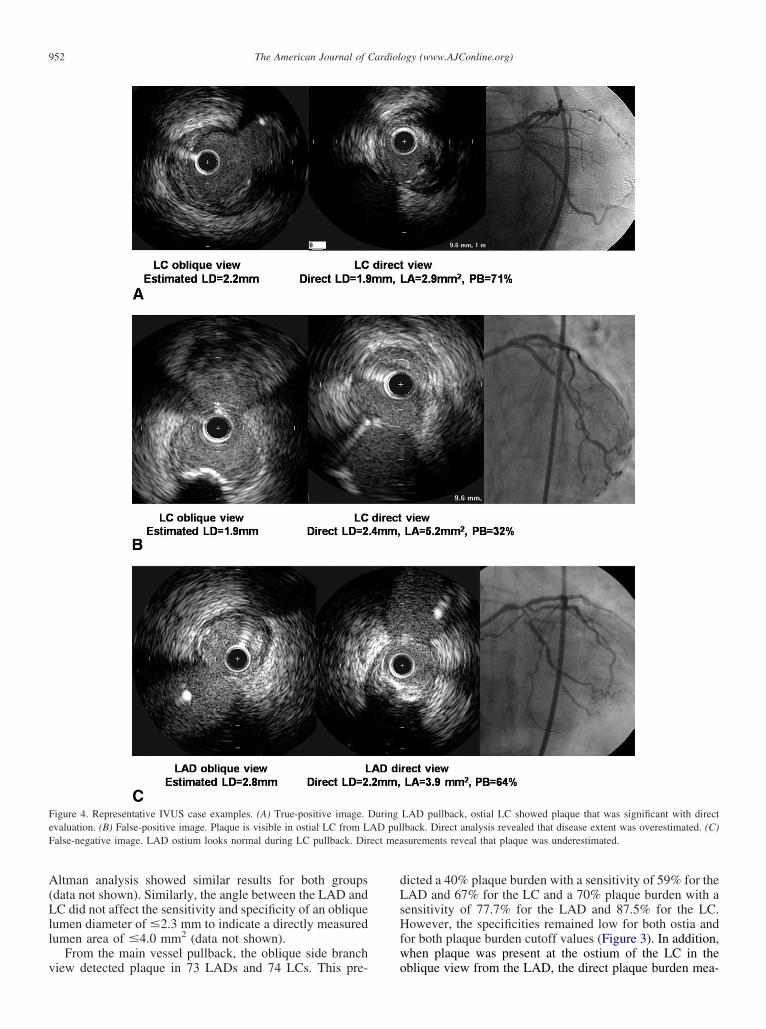
igure 4. Representative IVUS case examples. (A) True-positive image. Dvaluation. (B) False-positive image. Plaque is visible in ostial LC from Lalse-negative image. LAD ostium looks normal during LC pullback. Dir
iew detected plaque in 73 LADs and 74 LCs. This pre- o
icted a 40% plaque burden with a sensitivity of 59% for theAD and 67% for the LC and a 70% plaque burden with aensitivity of 77.7% for the LAD and 87.5% for the LC.owever, the specificities remained low for both ostia and
or both plaque burden cutoff values (Figure 3). In addition,hen plaque was present at the ostium of the LC in the
LAD pullback, ostial LC showed plaque that was significant with directlback. Direct analysis revealed that disease extent was overestimated. (C)surements reveal that plaque was underestimated.
uringAD pul
blique view from the LAD, the direct plaque burden mea-

spvtdsoasv
ciwcclf2mteQehwo2cp
D
iIpdatto
tttptIttuiabmwatLt
fistiomqdfboisatdi(lpiabr�psst
LabtwLa“wAtieMwptsr(scnomcmLIt
953Coronary Artery Disease/IVUS Study of Ostial Disease
urement was 50.1 � 13.7% (vs 42.5 � 13.8% when nolaque was evident at the ostium of the LC in the obliqueiew, p � 0.0028). In contrast, when plaque was present athe ostium of the LAD in the oblique view from the LC, theirect plaque burden measurement was 54.7 � 10.6% ver-us 54.9 � 12.9% (p � 0.9) no plaque was evident at thestium of the LAD in the oblique view from the LC. Thengle between the 2 daughter vessels did not affect the as-essment of side branch plaque burden from the obliqueiew (data not shown).
Comparing the 20-MHz (n � 45) and 40-MHz (n � 80)atheters, a better oblique assessment of the ostial LC min-mum lumen diameter from the LAD to LMCA pullbackas possible with the 20-MHz compared to the 40-MHz
atheters (r � 0.579 and r � 0.267, respectively). Theonverse was true for assessing the ostial LAD minimumumen diameter from the LC to LMCA pullback (r � 0.222or 20-MHz vs r � 0.440 for 40-MHz catheters). With the0-MHz catheter, the LAD lumen diameter was underesti-ated from the oblique view, and with the 40-MHz cathe-
er, both the LAD and LC lumen diameters were over-stimated from the oblique view (data not shown).ualitatively, no difference was found between the 2 cath-
ters in assessing the LAD plaque burden from the LC;owever, the detection of plaque at the ostium of the LCas predictive of either a 40% plaque burden (p � 0.0183)r a 70% plaque burden (p � 0.0183) when imaging with a0-MHz catheter but not when imaging with a 40-MHzatheter. Figure 4 shows examples of true-positive, false-ositive, and false-negative cases.
iscussion
By comparing the oblique/tangential IVUS imaging find-ngs of the side branch from the main vessel versus directVUS imaging of the same side branch, the results from theresent study have indicated that accurate assessment of theistal LMCA bifurcation (including the ostia of the LADnd LC) requires wiring and imaging of both the LAD andhe LC and cannot be accomplished by imaging just 1 ofhese 2 daughter vessels back to the LMCA and studying thether daughter vessel tangentially and obliquely.
Previous studies—mostly in phantoms—have assessedhe effect of transducer orientation, eccentric or noncoaxialransducer location, near-field versus far-field imaging, andhe effect on axial and lateral resolution, image angle, per-endicular versus oblique ultrasound beam angulation rela-ive to the vessel wall, and so forth, on the accuracy of theVUS measurements.3–9 In general, the greater the angula-ion, eccentric, or noncoaxial location of the transducer andhe greater the angle of incidence and distance between theltrasound beam and the vessel wall, the greater the errorsn IVUS measurements. These factors appear to be additivend to have an exponential effect such that a threshold existselow which errors in measurement are minor (the vastajority of clinical IVUS imaging situations) and abovehich the errors in measurement are exaggerated. Assessingside branch from a main vessel—in particular, assessing
he LC from the LAD-LMCA pullback or the LAD from theC-LMCA pullback because of vessel size—can represent
he worst case scenario because the side branch is in the far L
eld, does not present a perpendicular target to the ultra-ound beam, has varying degrees of angulation relative tohe path of the transducer, and is often curved, and themages are dependent on the lateral and axial resolution. Notnly are the lumen and vessel area and diameter measure-ents affected, but also the wall thickness and (conse-
uently) the plaque burden. The nonuniform extent andistribution of the atherosclerotic plaque burden at the bi-urcations are complex and have been previously describedut only in non-LMCA bifurcations. Plaques are locatedpposite the side branch takeoff, are more concentric prox-mal to the side branch, and more eccentric just distal to theide branch, spare the flow divider, maintain eccentricitycross a wide range of vessel stenoses, and are influenced byhe angle of the side branch takeoff such that plaque is alsoeposited preferentially toward an acute angle (or toward annner radius of curvature) and away from an obtuse angleor the outer radius of curvature).10–13 Eccentric plaqueocated on the inner wall at the curved coronary segments,robably because of uneven local shear stress, might havemplications for PCI for these segments. In the presentnalysis, the 95% limits of agreement in lumen diameteretween the oblique/tangential with direct measurementsanged from �1.84 to 1.14 mm (SD 0.75) for the LAD and1.69 to 1.22 mm (SD 0.73) for the LC. Assessment of the
laque burden using 2 cutoffs (40% and 70%) showed goodensitivity but poor specificity. Disease at the origin of aide branch might predict closure when performing PCI ofhe bifurcation.14
One concern that is important in performing PCI of theMCA—and especially in selecting the techniques to treatdistal LMCA bifurcation lesion—is disease of the side
ranch ostium. In the MAIN-COMPARE registry whenreating bifurcation lesions, a single-stent technique, inhich a stent was placed across the side branch (usually theC), was preferred in patients with diminutive or normal-ppearing side branches. A 2-stent technique (T-stenting,kissing” stenting, culotte technique, or crush technique)as considered in patients with diseased side branches.1
lthough no data are available to indicate that this “selec-ive” approach yields superior acute and long-term results, its dependent on assessing the vessel size and ostial dis-ase.15 An IVUS versus angiographic substudy of theAIN-COMPARE registry suggested that IVUS guidanceas superior to angiographic guidance.16 One explanationrovided by the investigators of the substudy was that (1)he systemic use of a 2-stent strategy compared to a single-tent strategy might increase the risk of stent thrombosis andepeat revascularization in bifurcation LMCA lesions, and2) a better insight into plaque configuration with IVUScanning can diminish the unnecessary use of 2-stent pro-edures by distinguishing true stenosis from the pseudoste-osis caused by various artifacts, including the device, cor-nary spasm, and calcification. Furthermore, an IVUSinimum lumen area cutoff of 4.0 mm2 is a common IVUS
riterion for deciding the significance of a stenosis in aajor epicardial vessel, including the ostium of the LAD orC. The results of the present study have indicated that the
VUS-guided decision-making process when treating a dis-al LMCA bifurcation stenosis requires imaging both the
AD and the LC.
bscwtbaBc7
aarbwsmc
1
1
1
1
1
1
1
1
1
1
2
2
954 The American Journal of Cardiology (www.AJConline.org)
One questions is whether IVUS imaging of bothranches increases the risk of the PCI procedure. Six largetudies have shown that other than transient spasm, acuteomplications appear to be rare and the long-term sequelaeere not different from those of controls.17–21 However,
hese studies did not include IVUS imaging of multipleranches and, in particular, IVUS imaging of both the LADnd the LC when treating a LMCA bifurcation stenosis.etter safety data should come from PROSPECT trial be-ause all 3 epicardial vessels were studied in approximately00 patients undergoing PCI for acute coronary syndrome.
The present study was performed in distal LMCA lesionsnd ostia of the LAD and LC. The results do not necessarilypply to non-LMCA bifurcation lesions. In addition, theseesults do not necessarily apply to the assessment of the sideranch from the main vessel after stent implantation—hether the procedure involves implantation of 1 or 2
tents. However, experience has shown that IVUS assess-ent of a bifurcation after stent implantation is more diffi-
ult than before PCI.
1. Seung KB, Park DW, Kim YH, Lee SW, Lee CW, Hong MK, ParkSW, Yun SC, Gwon HC, Jeong MH, Jang Y, Kim HS, Kim PJ, SeongIW, Park HS, Ahn T, Chae IH, Tahk SJ, Chung WS, Park SJ. Stentsversus coronary-artery bypass grafting for left main coronary arterydisease. N Engl J Med 2008;358:1781–1792.
2. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR,Mack MJ, Ståhle E, Feldman TE, van den Brand M, Bass EJ, VanDyck N, Leadley K, Dawkins KD, Mohr FW; SYNTAX Investigators.Percutaneous coronary intervention versus coronary-artery bypassgrafting for severe coronary artery disease. N Engl J Med 2009;360:961–972.
3. Mintz GS, Nissen SE, Anderson WD, Bailey SR, Erbel R, FitzgeraldPJ, Pinto FJ, Rosenfield K, Siegel RJ, Tuzcu EM, Yock PG. Standardsfor the acquisition, measurement, and reporting of intravascular ultra-sound studies: a report of the American College of Cardiology TaskForce on Clinical Expert Consensus Documents. J Am Coll Cardiol2001;37:1478–1492.
4. Chae JS, Brisken AF, Maurer G, Siegel RJ. Geometric accuracy ofintravascular ultrasound imaging. J Am Soc Echocardiogr 1992;5:577–587.
5. Kearney PP, Ramo MP, Spencer T, Shaw TR, Starkey IR, McDickenN, Sutherland GR. A study of the quantitative and qualitative impactof catheter shaft angulation in a mechanical intravascular ultrasoundsystem. Ultrasound Med Biol 1997;23:87–93.
6. Bekeredjian R, Hardt S, Just A, Hansen A, Kuecherer H. Influence ofcatheter position and equipment-related factors on the accuracy ofintravascular ultrasound measurements. J Invasive Cardiol 1999;11:207–212.
7. Kimura BJ, Bhargava V, Palinski W, Russo RJ, DeMaria AN. Distor-tion of intravascular ultrasound images because of nonuniform angularvelocity of mechanical-type transducers. Am Heart J 1996;132:328–
336.8. Engeler CE, Ritenour ER, Amplatz K. Axial and lateral resolution ofrotational intravascular ultrasound: in vitro observations and diagnos-tic implications. Cardiovasc Interv Radiol 1995;18:239–242.
9. Di Mario C, Madretsma S, Linker D, The SH, Bom N, Serruys PW,Gussenhoven EJ, Roelandt JR. The angle of incidence of the ultrasonicbeam: a critical factor for the image quality in intravascular ultra-sonography. Am Heart J 1993;125:442–448.
0. Kimura BJ, Russo RJ, Bhargava V, McDaniel MB, Peterson KL,DeMaria AN. Atheroma morphology and distribution in proximal leftanterior descending coronary artery: in vivo observations. J Am CollCardiol 1996;27:825–831.
1. Mallus MT, Kutryk MJ, Prati F, von Birgelen C, de Feyter PJ, Ro-elandt JR, Serruys PW. Extent and distribution of atheroscleroticplaque in relation to major coronary side-branches: an intravascularultrasound study in vivo. G Ital Cardiol 1998;28:961–969.
2. Badak O, Schoenhagen P, Tsunoda T, Magyar WA, Coughlin J,Kapadia S, Nissen SE, Tuzcu EM. Characteristics of atheroscleroticplaque distribution in coronary artery bifurcations: an intravascularultrasound analysis. Coron Artery Dis 2003;14:309–316.
3. Tsutsui H, Yamagishi M, Uematsu M, Suyama K, Nakatani S, Ya-sumura Y, Asanuma T, Miyatake K. Intravascular ultrasound evalua-tion of plaque distribution at curved coronary segments. Am J Cardiol1998;81:977–981.
4. Furukawa E, Hibi K, Kosuge M, Nakatogawa T, Toda N, Takamura T,Tsukahara K, Okuda J, Ootsuka F, Tahara Y, Sugano T, Endo T,Kimura K, Umemura S. Intravascular ultrasound predictors of sidebranch occlusion in bifurcation lesions after percutaneous coronaryintervention. Circ J 2005;69:325–330.
5. Teirstein PS. Unprotected left main intervention: patient selection,operator technique, and clinical outcomes. JACC Cardiovasc Interv2008;1:5–13.
6. Park S-J, Kim Y-H, Park D-W, Lee S-W, Kim W-J, Suh J, Yun S-Ch,Lee ChW, Hong M-K, Lee J-H, Park S-W; MAIN-COMPARE Inves-tigators. Impact of intravascular ultrasound guidance on Long-termmortality in stenting for unprotected left main coronary artery stenosis.Circ Cardiovasc Interv 2009;2:167–177.
7. Hausmann D, Erbel R, Alibelli-Chemarin MJ, Boksch W, CaraccioloE, Cohn JM, Culp SC, Daniel WG, De Scheerder I, DiMario C,Ferguson JJ III, Fitzgerald PJ, Friedrich G, Ge J, Görge G, Hanrath P,Hodgson JM, Isner JM, Jain S, Maier-Rudolph W, Mooney M, MosesJW, Mudra H, Pinto FJ, Smalling RW, Talley JD, Tobis JM, WalterPD, Weidinger F, Werner GS, Yeung AC, Yock PG. The safety ofintracoronary ultrasound: a multicenter survey of 2207 examinations.Circulation 1995;91:623–630.
8. Batkoff BW, Linker DT. The safety of intracoronary ultrasound: datafrom a multicenter European registry. Catheter Cardiovasc Diagn1996;38:238–241.
9. Pinto FJ, St. Goar FG, Gao SZ, Chenzbraun A, Fischell TA, AldermanEL, Schroeder JS, Popp RL. Immediate and one-year safety of intra-coronary ultrasound imaging: evaluation with serial quantitative an-giography. Circulation 1993;88:1709–1714.
0. Son R, Tobis JM, Yeatman LA, Johnson JA, Wener LS, KobashigawaJA. Does use of intravascular ultrasound accelerate arteriopathy inheart transplant recipients? Am Heart J 1999;138:358–363.
1. Ramasubbu K, Schoenhagen P, Balghith MA, Brechtken J, Ziada KM,Kapadia SR, Hobbs RE, Rincon G, Nissen SE, Tuzcu EM. Repeatedintravascular ultrasound imaging in cardiac transplant recipients doesnot accelerate transplant coronary artery disease. J Am Coll Cardiol
2003;41:1739–1743.




























