Embed Size (px)
Citation preview

Is there IgA of gut mucosal origin in the serum ofHIV1 infected patients?
A Quesnel, Ph Moja, F Lucht, J L Touraine, B Pozzetto, C Genin
AbstractThis study was performed in 77 HIV1seropositive adult patients to charac-terise the IgA hyperglobulinaemia seen inthe serum during the course of HIVinfection. It was shown that both IgAland IgA2 subclass concentrations were
simultaneously increased but the IgAlincrease was predominant. Secretory IgA(SIgA) concentration was significantlyincreased and IgA activity to gliadin,bovine serum albumin, and casein couldbe detected and was correlated with SIgAconcentration. In contrast, IgA activity tocytomegalovirus and to tetanus toxoiddid not correlate with total IgA con-
centration. These data suggest thepresence of IgA from gut mucosal originin the serum of these patients. Hyper IgAwas inversely correlated with the CD4+cell number. The increase of all parame-ters studied varied according to the totalIgA concentration in the serum but was
also directly related to the stage ofimmune deficiency in patients with hyperIgA.(Gut 1994; 35: 803-808)
Groupe sur l'etude desrelations entrel'immunit6 desmuqueuses et lesagents infectieux,Laboratory ofResearch inImmunologyA QuesnelPh MojaC Genin
and Laboratory ofMicrobiology,University of Saint-Etienne, INSERMU80, Lyon, FranceF LuchtB PozzettoJ L Touraine
Correspondence to:Professor C Genin,Laboratoire de Recherche enImmunologie, Faculte deMedecine J Lisfranc, 15 rueA Pare, 42023 Saint-Etiennecedex 02, France.
Accepted for publication6 October 1993
IgA hyperglobulinaemia is a classic immuno-logical abnormality seen in HIVI disease.' Incontrast with IgG concentration, whichincreases very early during the course of HIVinfection, hyper IgA is related to immunedefect progress and it has been considered tohave a prognostic value.2 It is usually assumedthat hyperglobulinaemia is consecutive topolyclonal stimulation of immunoglobulinsproduction3 by infectious agents especiallyfrom the herpes virus group4 but also by HIVitself.5
Recent data have shown, however, intestinallesions6 with an increase of intestinal mucosalmembrane permeability7 either secondary toopportunistic germ infection8 or occurring ear-
lier during the course of HIV disease directlybecause of HIV itself.9
It was hypothesised that a part of thehyper IgA seen includes IgA from mucosalorigin as a consequence of stimulation of theintestinal immune system. The structuralcharacteristics and the activity of IgA to
dietary and to non-gut derived antigenswere studied and related to the IgA concen-
tration in the serum of 77 HIV seropositiveadult patients at different stage of immunedeficiency.
803
Patients and methods
PATIENTSFrom a population with sexually or drug trans-mitted HIV1 infection, we selected 38 patientswithout immune deficiency (CD4+ cellnumber higher than 600/mm3) and 39 patientswith an immune deficiency (CD4+ cellnumber lower than 400/mm3, and lower than200/mm3 in 18 of them). They were classifieddepending on the IgA concentration in theserum: 32 patients, 28 males and 4 females ofmean age 38-5 years (22 to 75) with hyper IgA(IgA concentration :4-25 g/l) and 45 patients,35 males and 10 females of mean age 32-6years (20 to 72) with normal IgA (IgA concen-
tration <4-25 g/l). One hundred HIV sero-
negative blood donors from the Centre deTransfusion de Saint-Etienne matched for age
and sex were selected as normal controls ineach test.
METHODS
Characterisation ofIgA in the serum
Enzyme linked immunosorbent assay (ELISA)was usedl1 in all studies. Positive and negativecontrols were systematically included. Normalvalues defined by mean (2 standard deviations)were calculated from 100 blood donors serum
specimens.Measurement of IgA and IgA2 subclass
Serum samples were tested for IgAl and IgA2subclass with specific monoclonal anti-bodies" using a technique adapted fromConley et al.12 For IgA1 subclass measure-
ment, mouse monoclonal IgG to human IgAl(Becton Dickinson, Mountain View, CA,USA) were directly coated on polystyreneMicrowell immuno-Nunc plates (Nunc,Kamstrup, Roskilde, Denmark) at a concen-
tration of 3 1ig/ml in 0O1 M carbonate bufferpH 9-6 overnight at 4°C. For IgA2 subclassmeasurement, plates were coated with goatpolyclonal IgG to mouse y chain (CappelLab, Cochranville, PA, USA) at a concentra-tion of 20 pug/ml in the previous buffer. Afterwashing, mouse monoclonal IgG to humanIgA2 (Becton Dickinson) were added at a
concentration of 1 ,ug/ml in 0 05 M phos-phate buffer containing 0-05% TWEEN 20and 0 1% bovine serum albumin pH 7-3,incubated for one hour at 37°C, and thenwashed three times. Serum samples diluted1/5000 for IgAl and IgA2 assays in the same
buffer were added in triplicate and incubated
Gut 1994; 35: 803-808
on February 10, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.803 on 1 June 1994. D
ownloaded from

Quesnel, Moja, Lucht, Touraine, Pozzetto, Genin
for one hour at 37°C and then plates werewashed three times. Peroxidase conjugatedgoat polyclonal IgG to human ot chain diluted1/25 000 in the previous buffer wereincubated for one hour at 37°C. Enzymeactivity was detected by the addition to eachwell of 100 [.l substrate solution consistingof 4 mM orthophenylene diamine (Sigma,Saint-Louis, USA) in 0-02 M citrate phos-phate buffer pH 5 containing 0 04% hydro-gen peroxide. After 10 minutes at roomtemperature, 50 ,ul of 1 N HC 1 were added tostop the reaction. Absorbance of each wellwas read at 492 nm with a Titertek Multiskan(Flow Lab, Irvine, UK). Serum samples weretested in the presence of serial dilutions of apool of serum from 100 normal blood donors.The amounts of IgAl (2 g/l) and of IgA2(0-2 g/l) in the pool were determined usingstandard batch n° 5286 kindly donated by DrJ Radl (TNO Institute ofAgeing and VascularResearch, Leiden, The Netherlands). Resultwere expressed as g/l.
Measurement of secretory IgA - Plates werecoated with F(ab')2 fragments of goat poly-clonal IgG to human secretory component(kindly provided by Cl Vincent, INSERMU80, Lyon, France) at a concentration of 20pug/ml. Serum samples diluted 1/200 wereadded in triplicate for one hour at 37'C andthen incubated with peroxidase conjugatedgoat IgG to human at chain.'3 Samples weretested in the presence of serial dilutions ofhuman secretory IgA standard (Cappel).Results were expressed as pug/ml.
Detection ofIgA and IgG activity to dietaryantigens
Measurements of IgA and IgG to gliadin -Plates were coated overnight at 4°C with crudegliadin (Sigma), dissolved in ethanol 70%, anddiluted at a concentration of 10 ,ug/ml in 01M carbonate buffer pH 9-6. Uncoated siteswere saturated with a solution of gliadin at 2%in carbonate buffer for one hour at 37°C.Serum samples diluted 1/50 for IgA and 1/100for IgG in 0 05 M phosphate buffer pH 7-3containing 1% of rabbit serum (free of gliadinantibody) and 0 05% TWEEN 20 were addedin triplicate for one hour at 37°C. After wash-ing, plates were incubated with peroxidaseconjugated goat polyclonal IgG to human achain as previously described or with per-oxidase conjugated goat to polyclonal IgG tohuman ry chain diluted 1/50 000 in theprevious buffer.
Measurement of IgA and IgG to BSA - Theabove procedure was used except that BSA(Sigma) was directly coated after dilution at aconcentration of 10 ,ug/ml in 0 1 M carbonatebuffer pH 9-6. Uncoated sites were saturatedwith a solution of BSA at 5%. Serum sampleswere diluted 1/100 for IgA and 1/200 for IgGin phosphate buffer pH 7-3 containing 1%rabbit serum free of antibody to BSA and0-05% TWEEN 20.
Measurement of IgA and IgG to casein - Theabove procedure was used except that casein(Sigma) was dissolved in NaOH 01 N and
then diluted at a concentration of 10 pug/ml in0-1 M carbonate buffer pH 9-6 for coating.Uncoated sites were saturated with a solutionof casein at 2%. Serum samples were diluted1/200 for IgA and 1/400 for IgG in phosphatebuffer containing 1% rabbit serum free ofantibody to casein and 0 05% TWEEN 20.
In the three previous assays, serum sampleswere tested in the presence of serial dilutions ofa pool containing samples with antibody togliadin, BSA or casein (positive pool). Theoptical density for each serum sample wasexpressed as a percentage of the positive poolat the same dilution from a standard straightline. The pool containing serum samples fromnormal controls was itself tested as an individ-ual serum in the assay and results wereexpressed as the ratio between the testedserum and this normal pool.
Detection ofIgA and IgG activity to non-dietaryantigens
Measurement of IgA and IgG to cytomega-lovirus - IgA and IgG activity to cytomega-lovirus was determined by a sandwich typeELISA and previously described in detail. 14
Cytomegalovirus specific IgG antibodieswere detected by a commercial antibodycapture ELISA (Wellcome Laboratories,Dartford, England). Cytomegalovirus specificIgG seriology was performed by a sandwichtype ELISA: briefly, F (ab')2 fragments of goatpolyclonal IgG to human a heavy chain(Cappel) were used as solid phase capturereagents. After incubation with appropriatelydiluted samples, the presence of IgA antibodiesto cytomegalovirus was shown by addition ofperoxidase conjugated purified cytomegalovirus(Wellcome Laboratories, Dartford, England).Serum specimens with absorbance <0-200 atthe 1/16 dilution were considered as negative.
Measurement ofIgA and IgG to tetanus toxoid-Plates were coated overnight at 4°C withtetanus toxoid (500 L12mg) (Institute Pasteur,Paris, France) at a concentration of 10 ,ug/ml in0 1 M carbonate buffer pH 9 6. Uncoated siteswere blocked with a solution of gelatin at 2%o incarbonate buffer for one hour at 37°C. Serialtwofold dilutions of serum specimens in 0 05 Mphosphate buffer pH 7-3 containing 0 05TWEEN 20 and 0 1% BSA were added in trip-licate for one hour at 37°C. After washing,plates were incubated with peroxidase conju-gated goat polyclonal IgG to human ax chain orto human -y chain as previously described.The titre was taken as the highest serum
dilution that gave an optical density twice asgreat as the background.'5
STATISTICAL ANALYSISResults in hyper IgA group were comparedwith those in the normal IgA group by theMann-Whitney U test. The relation betweentotal IgA, both IgA subclass concentrations,and IgA activity to dietary antigens withsecretory IgA concentration were studied ineach patient by the Spearman rank correlationtest.
804
on February 10, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.803 on 1 June 1994. D
ownloaded from

Is there IgA ofgut mucosal origin in the serum ofHIVI iinfected patients?
p < 0-000124
0)
C04-
L-
CDC)
0.)
c,)
20
16
12
8
4
0'
200
0
C.
CN
C)
0)
160
120
80
40 2
0J
p < 0 0001
.................. ...........................
1-40
0
0
0
S
0)
C04-
4-
C.)CC._
0L)cN
0)
1 2
1 *0
0-8
06
0-4
0-2
0-
p = 0 0219
0
o 0E
0 +-f
o .
0~~~~~o c
0 ~~~~~~~0)o Cl......................H A<
I ~~fin
Normal IgA Hyper IgA
18
16
14
12
10
8
6
4.2
0
p < 0-0001
0
..................... ...... .
Normal IgA H
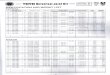
Figure 1: Serum IgAI and IgA2 subclass and secretory IgA concentration and IAratio depending on total IgA concentration. Mean value of each group is shown iunbroken line. Dotted line represents the threshold of increase (mean (2 SD)) fronormal controls. IgA 1, IgA2, SIgA concentration, and IgA 1/IgA2 ratio were velsignificantly increased in hyper IgA patients compared with the normal IgA patieby Mann-Whitney U test.
Results
MEASUREMENT OF IgAl AND IgA2 SUBCLASSAND SECRETORY IgA CONCENTRATION INSERUMTo study the structural characteristics of IgA inpatients with hyper IgA in comparison withpatients with normal IgA concentration, IgAland IgA2 subclass and secretory IgA concen-
trations were measured in the serum. IgAlconcentration was 7-43 (4-93) g/l in the hyperIgA group and 1-63 (1 11) in the normal IgAgroup (p<0-0001). IgA2 concentration was
0 35 (031) g/l in the hyper IgA group and 0- 10(0'07) in the normal IgA group (p<00001).The significant increase of IgAl/IgA2 ratio inthe hyper IgA group (40 34 (40- 13)) comparedwith the normal IgA group (18.54 (11-31))(p=00219) showed that the IgAl concentra-tion increased more significantly than the IgA2concentration (Fig 1).
Secretory IgA concentration was 6-07 (2 86),ug/ml in the hyper IgA group and 3-25 (1-14)in the normal IgA group (p<0-0001) (Fig 1).An attempt was made to find a relation
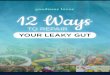
between the subclasses of IgA and secretoryIgA. A very significant correlation could beshown both with IgAl (r=0-81; p<00001)and IgA2 subclass (r=0-50; p<0-0001)(Fig 2).
MEASUREMENT OF IgA AND IgG ACTIVITY TODIETARY ANTIGENSTo study the specificity of IgA and IgG to
o dietary antigens in patients with hyper IgA ino comparison with patients with normal IgA
concentrations, IgA and IgG activity too gliadin, BSA, and casein were measured in* the serum. Anti-gliadin IgA activity index was0o 6-38 (10-9) in the hyper IgA group and 1-38o (0.73) in the normal IgA group (p<0 0001).
Anti-BSA IgA activity index was 1-88 (1-14)................... in the hyper IgA group and 1 -32 (0 6) in the
normal IgA group (p=0 0016). Anti-casein' IgA activity index was 1-64 (1-87) in the
hyper IgA group and 0-98 (0-45) in thenormal IgA group (p=0 0033) (Fig 3). IgAactivity to the three dietary antigens selectedwere significantly increased in hyper IgApatients.
0 An attempt was made to find a relationbetween the anti-dietary IgA activity and thesecretory IgA concentration in the serum. Avery significant correlation could be shown
* between secretory IgA and IgA to gliadino (r=0-82; p<0 0001), IgA to BSA (r=0 59;o p<00001), and IgA to casein (r=0144;
p<0 0001) (Fig 2).By contrast, no significant difference was
found for IgG activity to the three dietary8 antigens between the hyper IgA and normal
IgA group. Anti-gliadin IgG activity index was2-12 (1.99) in the hyper IgA group and 1-32
lyper IgA (0-46) in the normal IgA group (p=0-097).gAI/IgA2 Anti-BSA IgG activity index was respectivelyby an 2-21 (1-39) and 2-05 (1-53) (p=0-4351). Anti-)m 100 casein IgG activity index was respectively 1 00ry (0-53) and 0 95 (0.72) (p=0 2166).ent grout
MEASUREMENfT OF PREVIOUS PARAMETERS INRELATION TO CD4 + CELLS NUMBERCD4 + cell number in the peripheral blood wasexpressed in patient groups with normal IgAand hyper IgA.
In the normal IgA group, CD4 + cellnumber was higher than 600/mm3 in 31patients and lower than 400/mm3 in 14patients (six with CD4+ cells <200). 1I thehyper IgA group, CD4+ cell number washigher than 600/mm3 in seven patients andlower than 400/mm3 in 25 patients (12 withCD4+ cells <200). There was a significantdifference in CD4+ cell number between thetwo groups (p<0O0001) (Table I).
Values of IgAl/IgA2 ratio, secretory IgA,IgA to gliadin, BSA, and casein were notincreased whatever the CD4 + cell numberwhen the total IgA concentration was normal.They were increased in patients with totalhyper IgA. The increase was higher in patientswhen the number of CD4+ cells was lessthan 400/mm3 and higher than 600/mm3 witha significant difference for IgA to BSA(p=0.02), apart from the IgAl/IgA2 ratio,which decreased non-significantly. Theseresults could be only partly explained by thedifference in total IgA concentration in hyperIgA patients and a direct relation with immunedeficiency stage has to be considered(Table I).
805
on February 10, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.803 on 1 June 1994. D
ownloaded from

Quesnel, Moja, Lucht, Touraine, Pozzetto, Genin
601 r = 0-82; p < 0.0001
50
40
30
20
10
0
16
14C
.° 12
: 10C
8C
-7 20
0
0
xa)Co
~0
CD
00
r = 0-75; p < 0-00010 :-
0 V)0
0 C
0
Co
D 2 4 1 2 4161
:0 00c
0
0
lb~~~~~~~c
2 4 6 8 1012 1416 18
8
7
6
5
4
3
2
1
0
r= 0-59; p < 0.00010
00 0
00 1-0
12 r= 044; p<0-0001
x 10Ma)-0
.' 8-C
.CDcn 6
o 4
2
0'
251 r = 0-81; p < 000010
20
15'
10
5'
0
0
0
0
00
000046 8 10 12 1416180
0
2 4 6 8 10 12 14 16 18
03)
C
0
4o
C
CoC.)0
0
CN
0)
1-4
1-2
1.0
0-8
0-6
0-4
0-2
)
r = 0-50; p < 0-0001
0
00
0
0 2 4 6 8 10 12 14 16 18
SigA concentration (pg/ml) SIgA concentration (,g/ml) SIgA concentration (,ug/ml)
Figure 2: Regression lines of total IgA, both IgA subclass serum concentrations, and IgA activity to dietary antigens on
secretory IgA activity. Correlation coefficient and significance are shown.
MEASUREMENT OF IgA AND IgG ACTIVITY TONON-DIETARY ANTIGENSIn an attempt to examine the specificity to anti-gens that were not gut derived, IgA and IgGantibodies to cytomegalovirus and to tetanustoxoid were measured in the serum.
IgA antibodies to cytomegalovirus were notdetected in any tested subjects. Geometricmean titre of IgG antibodies to cytomegalo-virus was 1687 in the hyper IgA group and2336 in the normal IgA group (p=03906).IgA antibodies to tetanus toxoid were
detected with titres higher than 10 (from 10 to
50
xa)
0
0)
30
12
10
8
6
4
2
0
p < 0.0001
0
0 8
x
a)
050 .
a en(1)m
o <
, al+
.~~~I
±1
7
4
3
2
0
p = 0-0016
i
40) in five of 45 patients ( 1 %) in the normalIgA group and one of 32 patients (3 1O%) in thehyper IgA group (Table II). The difference wasnot significant (p=0 4751). IgG antibodies totetanus toxoid were detected in all subjectswith geometric mean titre 1018 in the hyperIgA group and 990 in the normal IgA group
(p=0'721 1).
DiscussionThis study, performed in HIV1 infectedpatients, classified according to the IgA
p = 0-0033
0
ol~~~
0
........................................................................
II
0 0
Normal HyperIgA IgA
entration. Mean value of each(2 SD)) from 100 normalyper IgA patients compared
120
xU1)
.
.5
U
0
0)
0
0
0
I
I
Normal Hyper Normal HyperIgA IgA IgA IgA
Figure 3: Serum anti-dietary antigen IgA activity concentration depending on total IgA conc
group is shown with an unbroken line. Dotted line represents the threshold of increase (meancontrols. IgA to gliadin, to BSA, and to casein activity were very significantly increased in hdwith the nortnal IgA patient group by Mann-Whitney U test.
11
4-
3-
2
1
0
xa)
C.a
Co0)0
806
on February 10, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.803 on 1 June 1994. D
ownloaded from

Is there IgA ofgut mucosal origin in the serum ofHIVI infected patients?
TABLE I Structure and anti-dietary specificity ofserum IgA depending on CD4+ cell number
CD4+ cells Patients Total IgA IgA I/IgA2 SIgA IgA to gliadin IgA to BSA IgA to casein(n/mm3) (n) (gil) (ratio) (,ug/ml) (index) (index) (index)
Normal IgA >600 31 2-7 (0-62) 17-35 (9-79) 3 30 (1-21) 1-36 (0-79) 1-26 (0-68) 0-92 (0 47)(n=45) <400 14 3-08 (0-7) 21-38 (14-43) 3-15 (1-00) 1-42 (0-6) 1-44 (0 35) 1-12 (0-39)
Hyper IgA >600 7 6-84 (3 37) 53-48 (40-10) 4-74 (1-33) 2-92 (2-15) 1-29 (0 57) 1-15 (0-77)(n=32) <400 25 7-26 (2-48) 36-51 (40-16) 6-44 (3 07) 7-35 (11-22) 2-04 (1-21)* 1-78 (2 07)
Results are expressed as mean (SD); *p=0-02 by Mann-Whitney U test comparing patients with hyper IgA according to CD4+cell number.
concentration in the serum, confirms therelation between the increase of serum IgAconcentration and the decrease of CD4+ cellnumber. This is in contrast with the IgG con-centration, which increases very early and theIgM concentration, which does not increaseduring the course ofHIV disease (unpublisheddata).2 This discrepancy between circulatingimmunoglobulins concentrations of differentclasses suggests that polyclonal activation of Bcell may not be the only mechanism respon-sible for the hyper IgA seen in the serum.3As it was considered that serum IgA concen-
tration could be related to mucosal immunesystem stimulation,16 IgA structural character-istics and anti-dietary antigen IgA activity werestudied. By comparison with patients withnormal IgA, IgAl and IgA2 subclass con-centrations were both found increased in theserum of hyper IgA patients with a good corre-lation but the increase of IgAl was predomi-nant. The highly significant increase ofsecretory IgA and of IgA antibody activity togliadin and at a lower activity to BSA andcasein correlated with secretory IgA concentra-tion in the serum of hyper IgA patients. Thisprovides strong evidence for the presence of cir-culating secretory IgA with anti-dietary antigenactivity in these patients. All the parametersvaried according to the total IgA concentrationbut were also directly related to the stage of theimmune deficiency in patients with hyper IgA.By contrast, IgG activity to dietary antigens wasnot increased and IgA antibodies to non-gutderived antigens like cytomegalovirus ortetanus toxoid was not detected or was very lowwhatever the total IgA concentration.A study analysing subclass distribution,
showed that an increase of total serum IgA wasaccompanied by a preferential increase of IgA 1in connective tissue diseases and to lesserextent in Berger's disease and chronic activeliver disease whereas IgA2 percentages tendedto be higher in alcoholic cirrhosis and Crohn'sdisease.'7 Serum concentration of secretoryIgA was found increased in lactating women,Crohn's disease, and especially in liverdiseases. 18
TABLE II Frequency ofIgA antibodies to tetanus toxoidwith regard to total IgA concentration
No ofpatients (%) with IgA antibodies totetanus toxoid titres
<10 10 20 40
Normal IgA 40 (88-9) 1 (2-22) 2 (4 44) 2 (4-44)(n=45)
HyperIgA 31 (96 9) 0 (0) 0 (0) 1 (3-1)(n=32)
Results expressed as mean (SD).
High titres of antigliadin IgA antibody in theserum has classically been considered as dis-tinctive of the intolerance to gliadin seen insusceptible subjects with coeliac disease.'9An increased proportion of polymeric IgA
and of secretory IgA to gliadin has also beendescribed20 with a predominance of IgAl iso-type in this disease.21
It was shown, however, that serum concen-tration of IgA antibodies to other dietaryantigens are often increased in these patients.22Moreover high titres of antigliadin IgA anti-body and to other dietary antigens wereoccasionally detected in Crohn's disease,ulcerative colitis, food allergy, and also inSjogren's syndrome, rheumatoid arthritis andin Berger's disease.23 Sensitive methods permiteven the detection of these antibodies at lowtitre in normal subjects.24
Enteropathy has been shown to beassociated with AIDS.25 Gastrointestinalmanifestations are common.26 In somepatients, diarrhoea has been shown to resultfrom specific infectious agents8 but in othersno such course is evident and a directcytopathogenic effect of HIV itself9 or anindirect local immune mechanism27 is sus-pected. Structural and functional changes,such as low grade bowel atrophy with hypore-generation, may result from the loss ofactivated regulatory T cells in the mucosa.28 Areduced number of intestinal IgA containingplasma cells has been reported in AIDSpatients.29 Decreased brush border enzymeactivities can be found in patients with AIDS30but also early in the course of HIV infection6causing a malabsorption.31
All these data argue in favour of a non-specific immunological hyper-responsivenessagainst antigens present in the gut lumenprobably associated with an increasedmucosal permeability resulting from abnor-mal small intestinal mucosa in HIV infectedpatients.7 32 Respiratory or genitourinary tractmucosa can also participate in the hyper-production of IgA. Impaired clearance ofSIgA remains an alternative mechanism.17The increased concentration of polymeric ormonomeric IgA in the serum of HIV 1infected patients is controversial.33 3 Theoriginal of serum secretory IgA antibodiesand of IgA to dietary antigens has to be eluci-dated. They may represent antibodiesproduced locally in the gut mucosa spillingover into the circulation20 or they may be pro-duced in the bone marrow and in extraintesti-nal lymphoid tissue as the result of themigration of locally stimulated lymphocytes,or both35 or result from uptake of luminalantigens into the blood.36
807
on February 10, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.803 on 1 June 1994. D
ownloaded from

808 Quesnel, Moja, Lucht, Touraine, Pozzetto, Genin
This study strongly suggests a disturbance ofthe gut mucosal immunity increasing duringthe course of HIV infection as partly respon-sible for the hyper IgA seen but probablyalso responsible for other immunologicalabnormalities and for a defect in the anti-infectious defence mechanisms.This work was presented in part at the Joint meeting of theBritish Society of Immunology and Societe Francaised'Immunologie - London, October 1991.We wish to thank F Duplat for technical assistance and E
Gagnaire for secretarial assistance. This work was supported bya grant of 'Fondation Merieux' and a grant of 'Region Ph6ne-Alpes'.
1 Pahwa SG, Quilop MTJ, Lange M, Pahwa RN, GriecoMH. Defective N-lymphocyte function in homosexualmen in relation to the acquired immunodeficiencysyndrome. Ann Intern Med 1984; 101: 757-63.
2 Fahey JL, Taylor JMG, Detels R, Hofmann B, Melmed R,Nishanian P, et al. The prognostic value of cellular andserologic markers in infection with human immuno-deficincy virus type 1. N Engl J7 Med 1990; 322: 166-72.
3 Lane HC, Masur H, Edgar LC, Whalen G, Rook AH, FauciAS. Abnormalities of B-cell activation and immunoregu-lation in patients with the acquired immunodeficiencysyndrome. NEnglJ7Med 1983; 309: 153-8.
4 Yarchoan R, Redfield RR, Broder S. Mechanisms of B cellactivation in patients with acquired immunodeficiencysyndrome and related disorders. Contribution of anti-body-producing B cells, of Epstein-Barr virus-infected Bcells, and of immunoglobulin production induced byhuman T cell lymphotropic virus, type III/lymphadeno-pathy-associated virus. J Clin Invest 1986; 78: 439-47.
5 Schnittman SM, Lane HC, Higgins SE, Folks T, Fauci AS.Direct polyclonal activation of human B lymphocytes bythe acquired immune deficiency syndrome virus. Science1986; 233: 1084-6.
6 Ullrich R, Zeitz M, Heise W, L'age M, Hoffken G, RieckenEO. Small intestinal structure and function in patientsinfected with human immunodeficiency virus (HIV):evidence for HIV-induced enteropathy. Ann Intern Med1989; 111: 15-21.
7 Lim Seng G, Menzies IS, Lee CA, Johnson MA, PounderRE. Small intestinal permeability in HIV positive patients.In: VII International conference on AIDS. [Abstract].Florence: 1991; 1: 245.
8 Laughon BE, Druckman DA, Vernon A, Quinn TC, PolkF, Modlin JF, et al. Prevalence of enteric pathogens inhomosexual men with and without acquired immuno-deficiency syndrome. Gastroenterology 1988; 94: 984-93.
9 Nelson JA, Wiley CA, Reynolds-Kohler C, Reese CE,Mergaretten W, Levy JA. Human immunodeficiency virusdetected in bowel epithelium from patients with gastro-intestinal symptoms. Lancet 1988; i: 259-62.
10 Engwall E. Enzyme immunoassay: ELISA and EMIT.Methods Enzymol 1980; 70: 419-22.
11 Engstrom PE, Norhagen G, Smith CIE, Soder PO,Hammarstrom L. An enzyme-linked immunosorbentassay for the determination of the IgA subclass distribu-tion of antigen-specific antibodies. J Immunol Methods1988; 115: 45-53.
12 Conley ME, Arbeter A, Douglas SD. Serum levels of IgAland IgA2 in children and in patients with IgA deficiency.Mol Immunol 1983; 20: 977-81.
13 Vincent C, Revillard JP. Sandwich-type ELISA for free andbound secretory component in human biological fluids. JImmunol Methods 1988; 106: 153-60.
14 Quesnel A, Pozzetto B, Touraine F, Moja P, Lucht F, DeThe G, et al. Antibodies to Epstein-Barr virus andCytomegalovirus in relation to CD4 cell number inhuman immunodeficiency virus 1 infection. J Med Virol1992; 36: 60-4.
15 Ballet JJ, Sulcebe G, Couderc U, Danon F, Rabian C,Lathrop M, et al. Impaired anti pneumococcal antibodyresponse in patients with AIDS-related persistent general-ized lymphadenopathy. Clin Exp Immunol 1987; 68:479-87.
16 Conley ME, Delacroix DL. Intravascular and mucosalimmunoglobulin A: two separate but related systems ofimmune defense? Ann Intern Med 1987; 106: 892-9.
17 Delacroix DL, Elkon B, Geubel AP. Hodgson HF, Dive C,Vaerman JP. Changes in size, subclass, and metabolicproperties of serum immunoglobulin A in liver diseasesand in other diseases with high serum immunoglublin A. JClin Invest 1983; 71: 358-67.
18 Delacroix D, Vaerman JP. Reassessment of levels ofsecretory IgA in pathological sera using a quantitativeradioimmunoassay. Clin Exp Immunol 1981; 43: 633-40.
19 Savilahti E, Perkkio M, Kalimo K. Viander M, Vainio E,Reunala T, IgA antigliadin antibodies: a marker ofmucosal damage in childhood coeliac disease. Lancet1983; i: 320-2.
20 Mascart-Lemone F, Cadranel S, Van den Broeck J, Dive C,Vaerman JP Duchateau J. IgA immune response patternsto gliadin in serum. Int Arch Allergy Appl Immunol 1988;86: 412-9.
21 Volta U, Molinaro N, Fratangelo D, Bianchi FB. IgA sub-class antibodies to gliadin in serum and intestinal juice ofpatients with coeliac disease. Clin Exp Immunol 1990; 80:192-5.
22 Scott H, Fausa 0, Ek J, Brandtzaeg P. Immune responsepatterns in coeliac disease. Serum antibodies to dietaryantigens measured by an enzyme linked immunosorbentassay (ELISA). Clin Exp Immunol 1984; 57: 25-32.
23 Troncone R, Ferguson A. Anti-gliadin antibodies. J PediatrGastroenterol Nutr 199 1; 12: 150-8.
24 Grodzinsky E, Hed J, Lieden G, Sjogren F, Strom M.Presence of IgA and IgG antigliadin antibodies in healthyadults as measured by micro-ELISA. Int Arch Allergy ApplImmunol 1990; 92: 119-23.
25 Kotler DP, Gaetz HP, Lange M, Klein EB, Holt PR.Enteropathy associated with the acquired immuno-deficiency syndrome. Ann Intern Med 1984; 101: 421-8.
26 Dworkin B, Wormser GP, Rosenthal WS, Heier SK,Braunstein M, Weiss L, et al. Gastrointestinal manifesta-tions of the acquired immunodeficiency syndrome: areview of 22 cases. Am J Gastroenterol 1985; 80: 774-8.
27 Zeitz M, Ullrich R, Riecken EO. The role of the gut-associated lymphoid tissue in the pathogenesis of theacquired immunodeficiency syndrome (HIV-infection).In: Proceeding of the Fifth International Congress ofMucosalImmunology. London: Kluwer Academic, 1990: 655-9.
28 Ullrich R, Zeitz M, Heise W, L'age M, Ziegler K, Bergs C,et al. Mucosal atrophy is associated with loss of activatedT cells in the duodenal mucosa of human immunodefi-ciency virus (HIV)-infected patients. Digestion 1990; 46(suppl 2): 302-7.
29 Kotler DP, Scholes JV, Tierney AR. Intestinal plasma cellalterations in acquired immunodeficiency syndrome. DigDis Sci 1987; 32: 129-38.
30 Cummins AG, La Brooy JT, Stanley DP, Rowland R,Shearman DJC. Quantitative histological study ofenteropathy associated with HIV infection. Gut 1990; 31:317-21.
31 Gillin JS, Shike M, Alcock N, Urmacher C, Krown S, KurtzRC, et al. Malabsorption and mucosal abnormalities ofthe small intestine in the acquired immunodeficiencysyndrome. Ann Intern Med 1985; 102: 619-22.
32 Batash S, Weinshel E, Falkenstein D, Ma T, Katz K,Hollander D, et al. HIV infection increases intestinal per-meability. Am J Gastroenterol 1991; 86: 1344.
33 Vincent C, Cozon G, Zittoun M, Mellquist M, KazatchkineMD, Czerkinsky C, et al. Secretory immunoglobulins inserum from HIV-infected patients. J Clin Immunol 1992;12: 381-8.
34 Kozlowski PA, Jackson S. Serum IgA subclasses andmolecular forms in HIV infection: selective increasesin monomer and apparent restriction of the antibodyresponse to IgAl antibodies mainly directed at envglycoproteins. AIDS Res Hum Retroviruses 1992; 8:1773-80.
35 McCaughan GW, Adams E, Basten A. Human antigen-specific IgA responses in blood and secondary lymphoidtissue: an analysis of help and suppression. 7 Immunol1984; 132: 1190-6.
36 Paganelli R, Levinsky RJ, Atherton DJ. Detection of specificantigen within circulating immune complexes: validationof the assay and its application to food antigen-antibodycomplexes formed in healthy and food-allergic subjects.Clin Exp Immunol 1981; 46: 44-53.
on February 10, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.35.6.803 on 1 June 1994. D
ownloaded from