Embed Size (px)
Citation preview

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 1
Is there a crystal ball?
Charting a Course of
Recovery for Disorders
of Consciousness Kathryn Farris, OTR/L
By the end of the session the participant will:
define clinical and diagnostic criteria required for accurate
diagnosis for patients in disorders of consciousness.
identify key components of the interdisciplinary assessment
and prioritizing treatment options for persons in disorders of
consciousness.
identify 3 methods of predicting outcome in persons with
disorders of consciousness.

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 2
DOC Admissions Shepherd = 525
Admitted Average Days Post Injury
Consensus Statements from:
Multi-Society Task Force on
Persistent Vegetative State
(1994)
Aspen Neurobehavioral
Conference Workgroup (Giacino et al, 2002)

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 3
Coma
Vegetative State (VS)
Persistent Vegetative
State (PVS)
Minimally Conscious
State (MCS)
Definition of Coma
“Represents a state of unarousable
unresponsiveness in which the eyes remain
continuously closed and there is no
understandable response to environmental or
intrinsic stimulation.”
(Giacino & Whyte 2005)

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 4
No evidence of sleep wake
cycles on EEG
Behavioral response consists
of reflex activity
Loss of function of both
cortex and reticular system
Lasts longer than 2-4 weeks
COMA: All criteria required on
clinical examination
No spontaneous or stimulus-induced eye-opening
No command following
No intelligible speech
No purposeful movement
No discrete defensive movements or capacity to
localize noxious stimuli

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 5
“Characterized by complete absence of
behavioral evidence for awareness of self
and environment, with preserved capacity for
spontaneous or stimulus-induced arousal.” (Giacino and Kalmar, 1997)
*In 2010 the term Unresponsive Wakefulness Syndrome was
introduced to replace Vegetative State as a better way to
describe the state and move away from the negative
connotation of VS.*
Vegetative state:
All criteria must be met No evidence of sustained, reproducible, purposeful, or voluntary
behavior responses to visual auditory, tactile or noxious stimuli
No evidence of language comprehension or expression
Intermittent wakefulness manifested by evidence of sleep-wake
cycles on the EEG
Periodic eye opening
Sufficient preservation of autonomic functions to permit survival
with adequate medical care
Variable preservation of cranial nerve and spinal reflexes
Incontinent of bowel and bladder
Bedside Exam Serially - Limited behavioral responses in frequency and complexity
Results of neuroimaging and laboratory studies important but not all sufficient
Roving eye movements may be present but often thought of as visual pursuit
Head and limb movements maybe
evident but not ever purposeful
Vocalization and emotional
responses are noted but not provoked
by environment events

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 6
MSTF – 1 month after BI
ACRM – Deferred until 12
months after onset
Aspen Group – recommended
term “persistent VS” be
abandoned

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 7
Parameters for Determining
Vegetative State
Etiology Parameter
Traumatic Brain Injury After 12 Months
Non-Traumatic Brain Injury After 3 Months
Metabolic and Degenerative
Diseases
1 – 3 Months
Infants with Anencephaly At Birth
Congenital Malformations 3 – 6 Months
(AAN 1995)
“Permanent VS refers to prognosis and
identifies the point after which recovery of
consciousness is highly improbable but not
impossible.”
(Giacino et al, 2002)
Coma can result from:
o Hemispheric or brainstem
o Focal brainstem lesions involving midbrain or pons
o Isolated medullary lesions -usually short duration
o Diffuse cortical or sub-cortical white matter lesions – extensive involvement of both hemispheres
Picture Copyright © 1995-1999
Keith A. Johnson and J. Alex Becker.
Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 8
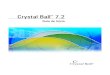
Neuropathology for those who
remain in Vegetative State
71 % w/ diffuse axonal injury (DAI)
o Of that: 80% had damage involving the thalamus
37% w/ ischemic damage in neocortex
Grade II and III DAI manifested by punctate lesions in the corpus callosum (II) and rostral brainstem (III)
Interesting facts:
50% considered VS after initial injury recovered consciousness by 1 year
15-43% of VS were found to have been misdiagnosed, they were actually MCS
(Whyte et al. 2005; Giacino &Trott 2004)
“A condition of severely altered consciousness in
which minimal but definite behavioral evidence of self
or environmental awareness is demonstrated.”
(Aspen Workgroup, Giacino et al, 2002)

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 9
Diagnostic Criteria for Minimally
Conscious StateThe key element is the requirement that there be at least one
clear cut behavioral signs of consciousness.
Simple command following
Gestural or verbal yes/no response
Intelligible verbalization
Movements or affective behaviors occur in relation to
relevant environmental stimuli
Visual or auditory tracking or sustained fixation that is in
direct response to moving stimuli
Appropriate response to the environment or situation
Minimally Conscious State
Episodes of crying, smiling or laughter in
response to linguistic or visual stimuli versus at
random times.
Vocalization or gestures that occur in direct
response to the linguistic content of comments or
gestures
Touching or holding objects in a manner that
accommodates the size and shape of the object

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 10
Severe Disabled (SD) using GOS
o Grade 2 and 3 DAI more frequent in SD cases (42% ) vs. VS (22%)
o Thalamic damage less prevalent in SD (50%) vs. VS (80%)
Studies show that visual tracking or pursuit have
higher incidence of progressing to inpatient
rehabilitation
MCS = 82% versus VS = 20% independent of time
post injury*
Of the 20% of the VS who exhibited visual pursuit,
73% went on to recover consciousness 12 months post
onset while only ½ of the VS without pursuit emerged
from VS(Giacino and Kalmar 1997; Ansell and Keenan 1989)
Overall, studies suggest MCS
appears to result in a reasonable
prognosis for recovery of function
when diagnosed early in TBI
MCS studies – patients who
continue to improve beyond 6
months and after attain
significantly better outcomes*(Giacino and Kalmer)

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 11
Coma
Vegetative
State
Minimally Conscious
State
Eye Opening No Yes Yes
Sleep/Wake Cycles No Yes Yes
Visual Tracking No No Often
Object Recognition No No Inconsistent
Command Following No No Inconsistent
Communication No No Inconsistent
Contingent Emotion No No Inconsistent
(NIDRR 2007 Conscious Consortium)
Requires reliable and
consistent evidence of:
o Functional communication –
Yes/No Responses
o Functional object use of two or
more objects
Prerequisite for meaningful
interpersonal interaction and
personal autonomy

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 12
Main Clinical Features:
Age
Severity
Duration of coma
Duration of post traumatic amnesia
Site and extent of cerebral lesions
Association with hypoxia
(Carlsson et al, Espersen et al, Frowein et al, Miller et al, Pitts et al.)
Coma Severity measured by
Glasgow Coma Scale
Glasgow Outcome Scale
(GOS) measures final outcome
Well known that GOS may
continue to change for 1 year
EYES OPENSpontaneous 4
To Touch 3
To Pain 2
None 1
BEST VERBAL
RESPONSE
Oriented 5
Inappropriate 4
Incomprehensible 2
None 1
BEST MOTOR
RESPONSE
Obeys Commands 6
Localizes Pain 5
Withdraws 4
Flexes To Pain 3
Extends To Pain 2
None 1

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 13
Glasgow Outcome Scale -Extended1 = Dead
2 = Vegetative State Condition of unawareness with only reflex responses but with
periods of spontaneous eye opening.
3 = Low Severe Disability
4 = Upper Severe Disability
Patient who is dependent for daily support for mental or physical
disability, usually a combination of both. If the patient can be left
alone for more than 8h at home it is upper level of SD, if not then
it is low level of SD.
5 = Low Moderate Disability
6 = Upper Moderate Disability
Patients have some disability such as aphasia, hemiparesis or
epilepsy and/or deficits of memory or personality but are able to
look after themselves. They are independent at home but
dependent outside. If they are able to return to work even with
special arrangement it is upper level, if not then it is low level.
7 = Low Good Recovery
8 = Upper Good Recovery
Resumption of normal life with the capacity to work even if pre-
injury status has not been achieved. Some patients have minor
neurological or psychological deficits. If these deficits are not
disabling then it is upper level of GR, if disabling then it is lower
level of GR.
Disability Rating Scale (DRS)
Eye Opening -Arousability
Communication -Awareness
Motor Response -Responsitivity
Feeding
Toileting -Cognitive Ability for Self Care Activities
Grooming
Level of Functioning - Dependence on Others
Employability - Psychosocial Adaptability
DRS CategoriesPredictor of long term severity after acute injury
Total DRS Level of Disability– 0 None
– 1 Mild
– 2-3 Partial
– 4-6 Moderate
– 7-11 Moderately Severe
– 12-16 Severe
– 17-21 Extremely Severe
– 22-24 Vegetative State
– 25-29 Extreme Vegetative State

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 14
Mild Moderate Severe
Normal structural imaging Normal or abnormal
structural imaging
Normal or abnormal
structural imaging
LOC = 0-30 minutes LOC >30 minutes and <24
hours
LOC >24 hours
AOC = a moment up to 24
hours
AOC >24 hours
Severity based on other criteria
PTA = 0-1 day PTA >1 and <7 days PTA >7 days
GCS = 13-15 GCS = 9-12 GCS = 3-8
AOC - Alteration of consciousness/mental state
LOC - Loss of consciousness
PTA - Post-traumatic amnesia
GCS - Glasgow Coma Scale DoD/VA Definition and Symptomatic
Taxonomy Working Group
Longer duration of coma is associated with
worse outcomes
Threshold values:
o Severe disability is unlikely when coma last less
than 2 weeks
oGood recovery is unlikely when coma lasts longer
than 4 weeks

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 15
Longer duration PTA is associated with worse
outcomes
Threshold values:
o Severe disability is unlikely PTA lasts less than 2
months
oGood recovery is unlikely when PTA lasts longer
than 3 months
Older age is associated with worse outcomes
Threshold values:
oGood recovery is unlikely in patients older than
65 years
Certain features (e.g., depth of lesions) are
associated with worse outcomes
Threshold values:
oGood recovery is unlikely when bilateral brainstem
lesions present on early MRI
From Kothari16Abbreviations: MRI,
magnetic resonance imaging; PTA,
post-traumatic amnesia

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 16
As determined by the GOS is unlikely when:
o Time to follow commands is less than 2 weeks
o Duration of PTA is less than 2 months
This summary of evidence-based guidelines is from Kothari.16
Reprinted with permission.
As determined by the GOS is unlikely when:
o Time to follow commands is longer than 1 month
o Duration of PTA is greater than 3 months
o Age is greater than 65 years
Dead Vegetative Severely
Disabled
Independent
At 1 Month
N=434 Adults
33% 15% 28% 24%
At 3 Months
N=218 Adults
35% 30% 19% 16%
At 6 Months
N=123 Adults
32% 52% 12% 4%
(Multi Task Force Data)
Outcome of Patients at 3, 6, and 12 months
after Non Traumatic BI
Non- Traumatic injury
(n=169)
3 Months 6 Months 12 Months
Death 24% 40% 53%
Vegetative State 65% 45% 32%
Recovery of consciousness 11% 15% 15%
- Severe Disability 6% 0% 11%
- Moderate Disability/
Good Recovery
1% 0% 4%
(Multi Task Force Data)

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 17
Assessment following severe
Brain Injury
Hierarchical system of quantitative measurements
Used for interdisciplinary treatment
Auditory, motor, and visual function
Arousal, oromotor/verbal & communication
Captures subtle clinical changes over time
Able to monitor rate of recovery
Auditory Function
Sub-scale
0 None
1 Auditory startle
2 Localization to sound
3 Reproducible movement to sound
4 Consistent movement to sound
Visual Function
Sub-scale0 None
1 Visual startle
2 Fixation
3 Pursuit eye movement
4 Object localization: Reaching

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 18
Motor Function Sub-scale
0 None/Flaccid
1 Abnormal posturing
2 Flexion posturing (instead of withdrawal)
3 Localization to noxious stimuli
4 Object manipulation
5 Automatic motor response (>50% of time)
6 Functional object use (>75% of time)
Oromotor/Verbal
Sub-scale
0 None
1 Oral Reflexive
Movement
2 Vocalization/Oral
Movement
3 Intelligible Verbalization
Communication
Sub-scale0 None
1 Non-functional:
intentional (<50%)
2 Functional: accurate
(>50%)
3 None
Arousal Sub-scale
0 Unarousable
1 Eye Opening with Stimulation
2 Eye Opening without Stimulation
3 Attention

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 19
Average CRS-R Change
Pain Assessment
First question asked “Is my loved one in pain?”
Clinical and ethical implications of evaluating
pain in persons with disorders of consciousness.
Nociception vs. PainNociception is the actual or potential tissue damaging
event transduced and encoded by nociceptors, the basic
processing of a noxious stimuli. Necessary for pain
perception but does not always lead to a conscious
experience.
Pain defined as an unpleasant sensory and emotional
experience associated with real or potential tissue damage,
a conscious 1st person experience that can be reported.
*Neuroimaging studies suggest these are mediated by
different networks.

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 20
Best tool to assess nociception
Tools developed and validated to detect pain in non-
communicative patients, newborns or people with
dementia.
FLACC - Face Legs Activity Cry Consolability
Not until recently was a tool developed for the DOC
population.
NCS-R - Nociceptive Coma Scale-Revised
Pace of research of disorders of consciousness
increased over 10 years
Advances in neuroimaging technologies for
allowing more accurate diagnosis and prediction
Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 21
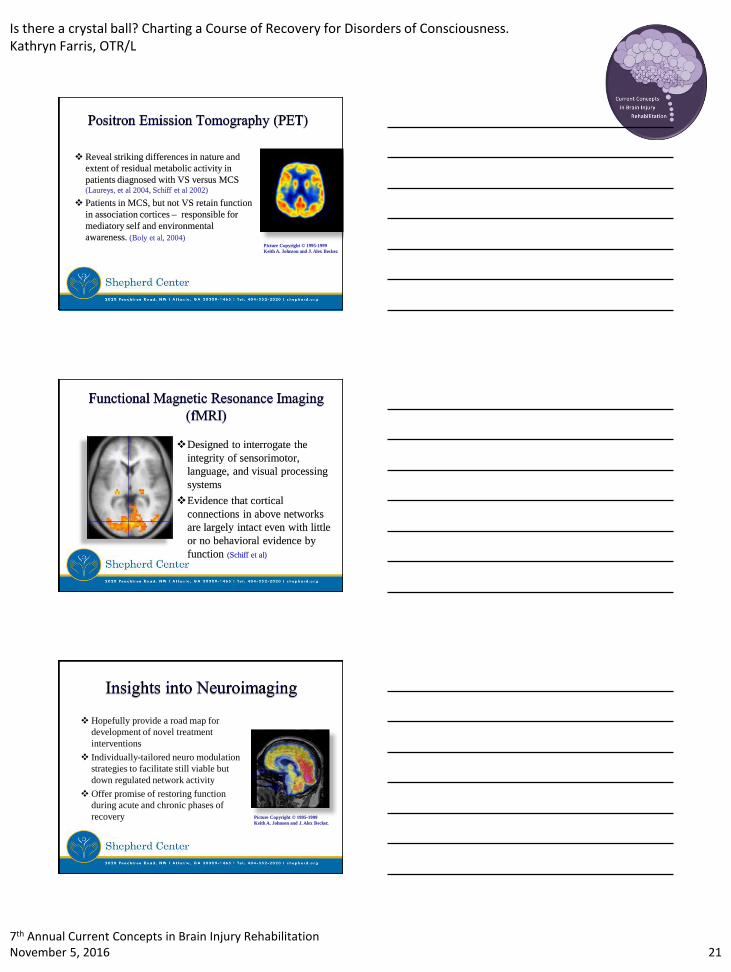
Reveal striking differences in nature and
extent of residual metabolic activity in
patients diagnosed with VS versus MCS (Laureys, et al 2004, Schiff et al 2002)
Patients in MCS, but not VS retain function
in association cortices – responsible for
mediatory self and environmental
awareness. (Boly et al, 2004)Picture Copyright © 1995-1999
Keith A. Johnson and J. Alex Becker.
Designed to interrogate the
integrity of sensorimotor,
language, and visual processing
systems
Evidence that cortical
connections in above networks
are largely intact even with little
or no behavioral evidence by
function (Schiff et al)
Hopefully provide a road map for
development of novel treatment
interventions
Individually-tailored neuro modulation
strategies to facilitate still viable but
down regulated network activity
Offer promise of restoring function
during acute and chronic phases of
recovery Picture Copyright © 1995-1999
Keith A. Johnson and J. Alex Becker.

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 22
New (or old) Directions
in Treatment Transcranial Magnetic Stimulation (TMS)
o non-invasive, task independent method of exciting/inhibiting the cortex
using electromagnetic induction
Transcranial Direct Current Stimulation (tDCS)
o non-invasive, constant weak current delivered via scalp electrodes into
cerebral cortex. Studied since 1960’s.
Intrathecal Baclofen (ITB)
o earlier use for dysautonomia and spasticity, may also have unexpected
improvements in level of consciousness, mental function and participation.
Deep Brain Stimulation (DBS)
o invasive bilateral DBS to central thalamus can induce behavioral/arousal
responses. First studied in 1968.
DOC Advocacy
Congressional Brain Injury Task Force
o The Mohonk Report
Disorders of Consciousness Task Force
o Publications
oDOC Minimal Competency Recommendations
o Education Materials
o Professional Instructional Courses
oAdvocacy McKesson Group
DOC Minimal Competency
Recommendations Specialized knowledge and skill is required to deliver optimal
care to patients with DOC.
Questions:
o If insurers were to agree to reimburse for DOC rehab, what
facilities should they look for?
o If caregivers are seeking expert care, where should they
look?
o If a facility wishes to be skilled in DOC rehab, what
attributes should they pursue?
Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 23
DOC Minimal Competency
Recommendations
Result: 21 recommendations for facilities
o Diagnosis and Prognosis
o Treatment
o Transitioning Care/Long Term Care Needs
o Management of Ethical Issues
Family Perspectives &
Decision Making
Severity of injury and associated short & long term
deficits
Limited knowledge and experience for families to
draw from
Wondering if there’s pain and suffering
Family/Caregiver feelings of guilt and loss
End of Life Conversations
Who has the difficult
conversations with
families?
When to have the
conversations?
What should be considered
with each conversation?
How should the wishes be
handled?
Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 24
Accurate differential diagnosis is an
essential first step
Consensus-based criteria
differentiating VS and MCS
Intent to minimize the risk of
misdiagnosis & inaccurate prognosis
inappropriate treatment decisions
Need for specialized care -DOC
Minimal Competency
Recommendations
New directions in interventions
Perspectives and considerations of
families
…and 2 years later.6 weeks post MVA…

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 25
The power of the mind. The strength of the
human spirit.
THANK YOU!
Kathryn Farris, OTR/L
References
• Al-Khodairy, A., Wicky, G., Nicolo, D., Vuadens, P. Influence of Intrathecal Baclofen on Level of
Consciousness and Mental Functions after Extremely Severe Brain Injury: Brief Report. Brain
Injury 2015; 29(4):527-532.
• American Congress of Rehabilitation Medicine. Recommendations for use of uniform nomenclature
pertinent to persons with alterations in consciousness. Arch Phys Med Rehabil. 1995; 76: 205-209.
• Angelakis, E., Liouta, E., Andreadis, N., Korfias, S., Ktonas, P., Stranjalis, G., Sakas, D.
Transcranial Direct Current Stimulaiton Effects in Disorders of Consciousness. Arch Phys Med
Rehabil. 2014; 95: 283-289.
• Chatelle, C., Majerus, S., Whyte, J., Laureys, S., Schankers, C., A Sensitive Scale to Assess
Nociceptive pain in Patients with Disorders of consciousness. J Neurol Neurosurg Psychiatry 2012.
• Chatelle, C., Thibaut, A., Whyte, J., De Val, M., Laureys, S., Schankers, C., Pain Issues in Disorders
of Consciousness. Brain Injury, 2014; 28(9): 1202-1208.
• Edgar, A., Kitzinger, C., Kitzinger, J., Interpreting Chronic Disorders of Consciousness: Medical
Science and Family Experience. Journal of Evaluation in Clinical Practice. 2014.
• Dufour L, Coleman K, Hauber R. Better care for the low-level brain-injured patients and their
families. J Neuroscience Nursing. 2002; 34: 20-24.

Is there a crystal ball? Charting a Course of Recovery for Disorders of Consciousness.Kathryn Farris, OTR/L
7th Annual Current Concepts in Brain Injury RehabilitationNovember 5, 2016 26
• Giacino JT, Kalmer K. Diagnostic and prognostic guidelines for the vegetative and minimally
conscious states. Neuropsychol Rehabil. 2005; 15: 166-174.
• Giacino JT, Kezmarsky MA, DeLuca J, et al. Monitoring rate of recovery to predict outcome in
minimally responsive patients. Arch Phys Med Rehabil. 1991; 72: 897-901.
• Giacino JT, Trott CT, Rehabilitative management of patients with disorders of consciousness. J
Head Trauma Rehabil. 2004; 19: 254-265.
• Giacino JT, Zasler ND, Datz DI, et al. Development of practice guidelines for assessment and
management of the vegetative and minimally conscious states. J Head Trauma Rehabil. 1997; 12:
79-89.
• Giacino JT, Zasler ND. Outcome after severe traumatic brain injury: coma, the vegetative state,
and the minimally responsive state. J Head Trauma Rehabil. 1995; 10: 40-56.
• Gossaries, O., Zasler, N., Laureys, S. Recent Advances in Disorders of Consciousness: Focus on
the Diagnosis. Brain Injury, 2014; 28(9): 1141-1150.
• Guller., Giacino, J., Potential Applications of Concurrent Transcranial Magnetic Stimulation and
Functional Magnetic Resonance Imaging in Acquired Brain Injury and Disorders of
Consciousness. Brain Injury, 2014; 28(9): 1190-1196.
• Keren O, Reznik J, Groswasser Z. Combined motor disturbances following severe traumatic brain
injury: an integrative long-term treatment approach. Brain Injury, 2001; 15: 633-638.
• Laureys, S., Celesia, G., Cohadon, F., Lavirijsen, J., Leon-Carrion, J., Sannita, W., Sazbon, L.,
Schmutzhard, E., vonWild, K., Zeman, A., Dolce, G. Unresponsive Wakefulness Syndrome: A
New Name for the Vegetative State or Apallic Syndrome. BMC Medicine, 2010, 8:68.
• Leong,B. The vegetative and minimally conscious states in children: spasticity, muscle
contracture and issues for physiotherapy treatment. Brain Injury, 2002; 16: 217-230.
• U. S. National Library of Medicine PubMed Health. AHFS consumer medication information
Atomoxetine (Strattera). Available at:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000222/. Accessibility verified September 19,
2012.
• Plum F, Posner J. The diagnosis of stupor and coma, 3rd ed. Philadelphia: FA Davis, 1982.
• Pohl M, Ruckreim S, Mehrholz J, Ritschel C, Strik H, Pause MR. Effectiveness of serial casting
in patients with severe cerebral spasticity: a comparison study. Arch Phys Med Rehabil, 2002; 83:
784-790.
• Schankers, C., Chatelle, C., Demertzi, A., Majerus, S., Laureys, S., What About Pain in Disorders
of Consciousness? American Association of Pharmaceutical Scientists 2012 Sep; 14(3): 437–
444.
• Seel, R., Douglas, J., Dennison, A., Heaner, S., Farris, K., Rogers, C. Specialized Early Treatment
for Persons with Disorders of Consciousness: Program Components and Outcomes. Arch Phys
Med Rehabil. 2013; 94: 1908-1923.
• The Multi-Society Task Force Report on PVS. Medical aspects of the persistent vegetative state.
N Engl J Med. 1994; 330: 1499-1508.
• The Quality of Standards Subcommittee of the American Academy of Neurology. Practice
parameter: assessment and management of persons in the persistent vegetative state. Neurology,
1995; 45: 1015-1018.
• Van Erp, W., Lavrijsen, J., van der Laar, F., Vos, P., Laureys, S., Koopmands, R., The
Vegetative State/Unresponsive Wakefulness Syndrome: A Systematic Review of Prevalence
Studies. European Journal of Neurology, 2014, 21: 1361-1368.
• Whyte J, Katz DI, Long D, DiPasquale MC, Polansky M, Kalmer K, Giacino JT, Childs N,
Mercer W, Novak P, Mauer P, Eifert B. Predictors of outcome in prolonged posttraumatic
disorders of consciousness and assessment of medication effects: a multicenter study. Arch Phys
Med Rehabil. 2005; 86: 453-462.