Ischemic Heart Disease Dr. Emtenan AlHarbi Clinical pharmacy
department
Slide 3
Learning objectives Identify risk factors for development of
ischemic heart disease Differentiate between pathophysiology of
chronic stable angina and acute coronary syndrome (ACS) Recognize
symptoms and diagnostic criteria of IHD Identify the appropriate
therapeutic regimen and monitoring plan for management of IHD
IHD Ischemic heart disease (IHD) is primarily caused by
coronary atherosclerotic plaque formation that leads to an
imbalance between oxygen supply and demand resulting in myocardial
ischemia. Chest pain is the symptom of myocardial ischemia due to
coronary artery disease (CAD).
Slide 6
Slide 7
Epidemiology and etiology In Saudi Arabia: Overall prevalence
of CAD in KSA is 5.5% Prevalence in males and females were 6.6% and
4.4% (p< 0.0001). Urban Saudis have a higher prevalence of 6.2%
compared to rural Saudis of 4% (p< 0.001).
Slide 8
Epidemiology Men > women In women: it increase after
menopause by 2-3 fold.
Slide 9
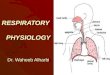
The major epicardial coronary arteries
Slide 10
Causes of Ischemia ? Narrowing of major coronary arteries by
atherosclerotic plaques. Atherosclerosis of 1 or more of the major
coronary articles or their branches is major cause. When there is
an imbalance between: The coronaries ability to supply adequate
oxygen and blood flow The myocardiums demand for oxygen Neither
factor should be thought of as more important than the other. Both
must be in balance.
Risk factors of IHD ModifiableNon-modifiable Cigarette smoking
*Male Gender* Hyperlipidemia*( Fasting cholesterol and
triglycerides) Age * 45 years or greater for males, 55 years or
greater for females Diabetes*(Fasting blood glucose) Family history
of premature CV disease Obesity* Hypertension* Physical inactivity
* statistically significant risk factors in KSARisk factors for
atherosclerotic plaques
Slide 15
Why ? Cigarette smoking accelerates coronary atherosclerosis
and increases the risk of thrombosis, plaque instability,
myocardial infarction, and death. By increasing myocardial oxygen
needs and reducing oxygen supply, it aggravates angina.
Hypertension is associated with an increased risk of adverse
clinical events from coronary atherosclerosis as well as stroke. In
addition, the left ventricular hypertrophy that results from
sustained hypertension aggravates ischemia. Diabetes mellitus
accelerates coronary and peripheral atherosclerosis Dyslipidemias
and increases in the risk of angina, myocardial infarction, and
sudden coronary death.
Slide 16
Slide 17
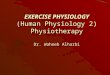
Angina symptoms Diagnostic workup History and physical Stress
test and angiography Control risk factors (HTN, metabolic syndrome
cigarette smoking obesity) Primary and secondary prevention
Anti-anginal therapy General treatment strategies for angina follow
in clockwise fashion from the top center. Treatment-general
approach
Slide 18
Clinical classification of chest pain
Slide 19
Non- Anginal CP
Slide 20
Other way to classify the chest pain
CharacteristicsCardiacGastrointestinalMusculoskeletal HistoryRF for
CADGastritis or indigestion Trauma Type of painHeavy pressure,
crushing or squeezing sensation Burning sensationSore, achy
feeling, sharp pain Precipitating factor Exertion or stressFood
consumption Physical movement Relived byRest or NGAntacidRest,
heat, or analgesia
Slide 21
Medications that may cause chest pain 1.Bisphosphonate 2.NSAIDs
3.Potassium chloride 4.Some antineoplastic e.g. flurouracil,
5.Corticosteroids. 6.Ferrous sulphate. 7.Antiarrythmics e.g.
flecainide, propafenone, quinidine
Slide 22
Angina symptoms Diagnostic workup History and physical Stress
test and angiography Control risk factors (HTN, metabolic syndrome
cigarette smoking obesity) Primary and secondary prevention
Anti-anginal therapy General treatment strategies for angina follow
in clockwise fashion from the top center. Treatment-general
approach
Slide 23
Common clinical manifestations of IHD ACS s: Occur at rest
Disruption of atherosclerotic plaque with subsequent thrombus
formation 1.Myocardial Infarction: Region of myocardial necrosis
due to prolonged cessation of blood supply. Results from acute
thrombus at side of coronary atherosclerotic stenosis. In both
NSTEMI or STEMI the Cardiac enzymes are +ve 2. Unstable Angina:
Increased frequency and duration of Angina episodes, may progress
to MI if not treated Stable Angina: chronic pattern of transient
angina pectoris precipitated by physical activity or emotional
upset, relieved by rest with in few minutes. Temporary depression
of ST segment with no permanent myocardial damage Variant or
prinzemetal angina: Typical anginal discomfort usually at rest.
Develops due to coronary artery spasm rather than increase
myocardial oxygen demand. Occur at rest Affect young people/ no RF
for CAD.. Cigarette smoking, cocaine and cold temperature are the
provoking factors. Silent Ischemia: Asymptomatic episodes of
myocardial ischemia. Detected by electrocardiogram and laboratory
studies. UA: Unstable angina, NSTEMI: Non ST Elevation Myocardial
Infarction, STEMI: ST Elevation Myocardial Infarction
Slide 24
Canadian Cardiovascular Society (CCS) grading of angina
Slide 25
Stable vs Unstable angina Angina is considered stable: When it
only occurs with prolonged exertion Or imposes a slight limitation
of ordinary activity (ie, CCS class I and II) Or when it has
stabilized with CCS class III symptoms. Angina is unstable: When it
is occurs at rest lasting more than 20 minutes Angina of at least
CCS class III severity of new-onset Or previously diagnosed angina
that increases in frequency, duration, or severity by at least one
CCS class to at least level III.
Slide 26
The clinical performance measures for chronic stable CAD
recommended by the ACC and AHA Blood pressure measurement Lipid
profile Symptom and activity assessment Smoking cessation
Antiplatelet therapy Drug therapy for lowering LDL cholesterol
-blocker therapy for prior MI ACE inhibitor therapy Screening for
diabetes.
Slide 27
Risk factors modifications Risk factorsGoalsTreatment
strategiesBenefits SmokingComplete cessationEncourage quitting.
Suggest medications to facilitate quitting. Use of the nicotine
patch in conjunction with bupropion.. Suggest smoking cessation
program. Decreased BP (decreased O 2 demand). Decreased risk of
vasospasm (increased O 2 delivery). HypertensionSystolic BP less
than 140 mm Hg. Diastolic BP less than 90 mm Hg. Antihypertensive
agents. Reduce caloric intake. Emphasize vegetable, fruit, low-fat
dairy intake. Moderate/eliminate alcohol intake. Smoking cessation
program. Weight management. Decreased myocardial O 2 demand
Hypercholesterole mia LDL less than 100 mg/dL. HDL greater than 40
mg/dL (women > 50). Triglycerides less than 150 mg/dL.
Lipid-lowering agents. Diet. Weight management. Increased physical
activity. Plaque stabilization. Halts CAD progression. Modest
plaque regression. DiabetesSystolic BP less than 130 mmHg.
Diastolic BP less than 80 mmHg. HbA1c less than 7- 6.5%. Dietary
modification. Tighter control of blood sugar levels. Exercise.
Slows disease progression. ObesityBody mass index less than 25 kg/m
2. Dietary modification. Exercise.Decreased BP. Improved glucose
tolerance and lipid profile. Others: influenza vaccine (AHA/ACC
recommendation)
Slide 28
Prognosis Prognostic indicators in patients with stable angina
are: LV function: Ejection fraction (