Embed Size (px)
Citation preview

Annals of Burns and Fire Disasters - vol. XXXI - n. 1 - March 2018
42
Introduction
Patients with severe burns (>20% total body surface areaburn) are at risk for developing complications such as systemicinfections and septic shock. The associated hemodynamic in-stability and perfusion failure might lead to the development ofischemic lesions that are unrelated to the burn injury. Ischemicnecrosis of cutaneous and subcutaneous tissue is a serious com-plication in critically ill patients with a high mortality rate (upto 40%) and half of survivors require major reconstruction.1,2We hereby present the case of a burn patient developing massivesoft tissue necrosis after an episode of septic shock and discussthe pathophysiology and management of this complication.
Case description
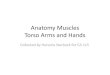
A 42-year-old overweight (BMI 30.3) female sustained afire injury from explosion of a grill and was admitted to ourburn centre with a 50% total body surface area (TBSA) burn.Past medical history was significant for hepatitis C, alcohol,and drug abuse (oral). Deep partial-thickness and full-thicknessburns were present on the face, neck, anterior thorax (partialsparing of breasts), whole abdominal area (deeper on epigas-tric, umbilical, right hypochondriac, and lumbar regions), bi-lateral upper arms (not including hands), bilateral anteriorupper thighs, and gluteal regions (Fig. 1a,b). The patient wasput under mechanical ventilation and was resuscitated accord-
ISCHEMIC THROUGH-AND-THROUGH NECROSIS OF THELATERAL WALL OF THE TORSO AND INGUINAL REGIONSUBSEQUENT TO FLAME INJURY AND SEPTIC SHOCK: ACASE REPORT AND LITERATURE REVIEWNÉCROSE ISCHÉMIQUE D’UNE EXTRÉMITÉ À L’AUTRE, DE LA PARTIELATÉRALE DU THORAX ET DE LA RÉGION INGUINALE, SECONDAIRE ÀUNE BRÛLURE ET À UN CHOC SEPTIQUE: À PROPOS D’UN CAS ET REVUEDE LA LITTÉRATURE
Tocco-Tussardi I.,1,2* Presman B.,1 Sleem Z.,1 Huss F.1
1 Department of Plastic and Maxillofacial Surgery, Uppsala University Hospital, Uppsala, Sweden2 Department of Neurosciences, University of Padova, Padova, Italy
SUMMARY. Post-burn infections still stand as the most common/serious complication of burn injuries: sepsis accounts for 50-60% ofdeaths in burn patients despite improvements in antimicrobial therapies. Among the many potential complications of sepsis/septic shockare hemodynamic instability and perfusion failure. We report the case of a patient developing massive soft tissue necrosis after an episodeof acute post-burn septic shock, with possible explanation of an overdosage of vasopressors due to significant body weight increase as aneffect of the burn resuscitation. The utility of vasopressor agents in the management of septic shock depends on the balance between in-creased perfusion pressure and the direct effect on the microvasculature. The almost inevitable body weight increase in the acute post-burnphase as an effect of the resuscitation makes this balance more difficult to maintain.
Keywords: perfusion, post-burn infection, resuscitation, sepsis, shock
RÉSUMÉ. Les infections restent les complications les plus fréquentes et les plus sérieuses des brûlures: le sepsis est responsable de 50 à60% des morts chez les patients brûlés, malgré les améliorations du traitement antimicrobien. Parmi les nombreuses complications poten-tielles de l’infection et du choc septique, figurent l’instabilité hémodynamique et l’échec des perfusions. Nous rapportons l’observationd’un patient développant une nécrose massive des parties molles après un épisode de choc septique, chez un brûlé avec comme explicationpossible, un surdosage de vaso-presseurs lors de la réanimation, responsable d’une augmentation significative du poids corporel. L’effi-cacité des agents vasopresseurs dans la prise en charge du choc septique dépend de l’équilibre entre l’augmentation de la pression perfu-sionnelle et l’effet direct sur la micro vascularisation. L’augmentation du poids corporel toujours inévitable lors de la phase aiguë de labrûlure, en relation directe avec la réanimation, rend plus difficile le maintien de cet équilibre.
Mots-clés: perfusions, infections des brûlures, réanimation, sepsis, choc
*Corresponding author: Ilaria Tocco-Tussardi, MD, Department of Plastic and Maxillofacial Surgery, Uppsala University Hospital, 751 85 Uppsala, Sweden.Tel.: +46 18 611 00 00; email: [email protected]: submitted 21/12/2017, accepted 12/02/2018.

Annals of Burns and Fire Disasters - vol. XXXI - n. 1 - March 2018
43
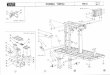
ing to the Parkland Formula without any hypotensive episodes.Of note, an amount of 14.5 L resuscitation fluid was adminis-tered within the first 7 hours only. Twenty-eight hours after theaccident, the patient’s burns on the thorax and abdomen (16%TBSA) were enzymatically debrided (NexoBrid®). The treat-ment with NexoBrid® proved to have good efficacy with theachievement of viable bleeding tissue covering the whole sur-face area (Fig. 2a,b). Wounds were subsequently covered withdonor skin (allograft). She was taken to the operating room ondays 3 and 6 for staged tangential excision and allograft appli-cation to her neck, upper extremities, thighs and buttocks. Theanterior neck was treated at the first session (day 3) to performearly tracheostomy. During this phase, the patient experiencedan increase in body weight of +43% from admission (from 82to 117 kg).
On day 4 she developed complications with a bloodstreaminfection and septic shock due to Streptococcus group C andAcinetobacter baumannii. Mean blood pressure was 50 mmHgand the patient was started on: high volume-fluid resuscitation(1000ml/h); antibiotic therapy (piperacillin-tazobactam, gen-tamicin and klindamycin); and vasopressors (norepinephrine
at 0.55 µg/kg/min and dobutamine at 6 µg/kg/min). After 13hours of continuous infusion, the norepinephrine dose was low-ered (0.35 µg/kg/min) and vasopressin (0.03 U/min) wasadded. Infusion of vasopressors continued for a total of 60hours until she stabilized.
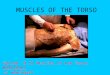
The patient returned to the operating room on day 8 for re-vision of the thorax, abdomen and thighs. On removal of theallografts, the underlying tissue appeared diffusely necrotic onthe right lateral thorax, right hemiabdomen and right inguinalregion. Ischemic non-bleeding muscular tissue was exposedwith evidence of thrombosed vessels. Necrosis also involvedthe external surface of the 7th-10th right rib (Fig. 3a,b). Speci-mens of the tissue were sent both for culture and pathologicalexamination; results from culture were negative; microscopicreports showed polymorphonuclear infiltration and edema ofdermis, subcutaneous fat and superficial fascia, and angio-thrombosis.
The debridement was semi-conservative with partial spar-ing of the necrotic rectus abdominis to allow visceral coverage,and donor skin was applied on all wounds. Angio-computedtomography (angio-CT) scan of the torso on day 9 confirmed
Fig. 1 - Clinical presentation of the flame burn injury: (a) front side; (b) right side. Note the tension of the breast tissue due to the full-thickness burnssurrounding the area (circle).
Fig. 2 - Clinical presentation after enzymatic debridement (NexoBrid®) to the thorax and abdomen: (a) right side. Note the good efficacy with theachievement of viable bleeding tissue covering the whole surface area and the release of tension (circle); (b) left side.

Annals of Burns and Fire Disasters - vol. XXXI - n. 1 - March 2018
44
necrotic tissue to the right side of the abdomen and flank in-volving rectus abdominis, rectus transversus and obliquus ex-ternus abdominis muscles, with intact peritoneum, but novascular thrombosis was detected.
Over the following two months, progressive demarcationand multiple debridements with resection of necrotic ribs left adefect of approximately 25 x 20 cm on the torso and 15 x 10cm in the groin. The patient was reconstructed with pectoralisand latissimus dorsi pedicled fasciocutaneous flaps for the rightthorax and abdomen, and a gracilis muscle pedicled flap for the
inguinal region (Fig. 4a,b). After a few revisions, healing wascompleted and the patient was discharged on day 103 (Fig. 5).
Discussion
Subcutaneous tissue necrosis is an uncommon but severecomplication of septic shock. Possible pathophysiologic mech-anisms include: increased peripheral resistance; shunting of cap-illary exchange vessels; decreased delivery of O2; impairedremoval of CO2; bacterial products activating the clotting mech-
Fig. 3 - Clinical presentation on day 8 after having sustained a bloodstream infection and septic shock from day 4 to 7: (a) after the removal of dressingsin the operating theatre. Allograft removed in central area revealing unviable tissue underneath; (b) after complete removal of allografts: evidence oftissue necrosis down to peritoneum and right lateral thorax, abdomen, and inguinal region.
Fig. 4 - After completion of the post-burn reconstruction: (a) post-burn day 90; (b) one-year follow-up.

Annals of Burns and Fire Disasters - vol. XXXI - n. 1 - March 2018
45
anisms; and capillary obstruction by micro thrombi.1 Therefore,decreased blood flow to the tissues is the result of both systemicperfusion failure and peripheral perfusion impairment.
In order to maintain mean arterial pressure ≥ 65 mmHgand sufficient cardiac output to achieve adequate tissue perfu-sion, inotropic agents are critical and should be used early.3
The Surviving Sepsis Campaign guidelines recommend vaso-pressors as first-line therapy in septic shock.4 The most fre-quently used vasopressor agent is norepinephrine (80.2%),5
which was recently indicated as superior to dopamine in termsof survival by a meta-analysis on vasopressors in septic shock.6However, these agents also hold the potential to cause a num-ber of significant complications, ranging from systemic events(hypoperfusion, dysrhythmias, myocardial ischemia, hyper-glycemia) to local effects (e.g. deepening of burns).
Ischemic skin necrosis is a rare complication of the use ofvasopressors in critically ill patients, with only seven other re-ports in the literature.2,7-12 Presumptive mechanisms include:extravasation, peripheral administration and high dose infu-sion. Complications have also been associated with infusionthrough a central venous catheter, the presence of risk factors(such as acute kidney failure, obesity, disseminated intravas-cular coagulopathy) and peripheral arterial occlusive dis-ease.12,13 The severity of lesions ranges from dry gangrene ofthe fingers and toes to extensive bruises and large exudativeblisters on extremities. Cho et al.12 recently reviewed the ex-isting reports of skin necrosis due to vasopressors in the liter-ature, highlighting how lesions appear in different areas inrelation to specific inotropic agents: while norepinephrine-in-duced skin necrosis typically occurs on fingers and toes, thewider areas of skin are more affected by vasopressin.14 This isrelated to the unique distribution of vasopressin receptor type1 (V1 receptor), which is located in smooth muscles of theblood vessels, mainly in the territory of the splanchnic circu-lation, kidney, myometrium, bladder, adipocytes, hepatocytes,platelets, spleen, testis and skin.15
In our case, vasopressors were infused centrally throughthe subclavian vein and there was no extravasation. The patient
was morbidly obese, but did not develop AKI/DIC. A combinedtherapy of inotropic agents was required to maintain adequatemean arterial pressure levels in the critical phase and vasopres-sors were administered in standard doses. However, the patientmight have been exposed to an over-dosage of inotropic agentsimputable to the significant weight gain (+43%) experiencedin the resuscitative phase. On the other hand, the distributiveand hypovolemic shock characterizing the acute post-burnphase might have contributed to the development of ischemiclesions through an additional decrease of blood flow to the tis-sues. Additionally, it must be noted that we extended the enzy-matic debridement to 16% TBSA. While current posology andmethod of administration of NexoBrid® now states that itshould not be applied to more than 15%,16 developing a largeraw area with considerable bleeding and fluid loss might havea side role in the development of hypotension. Fig. 5 illustratesthe pathophysiologic mechanisms involved. The differential di-agnosis of this complication included necrotizing soft tissue in-fection (NSTI), which was in accordance with significantpositive fluid balance within the days before septic shock pres-entation and failure of all allografts. Diagnosing NSTI is verychallenging in an acute burn patient and cannot be ruled outcompletely, as pathognomonic clinical findings (rubor, blister-ing, crepitations, pain out of proportion) are blurred in exten-sive burn injuries. Nonetheless, NSTI seems improbable in thepresent case, due to the following considerations:– NSTI following burn injuries cannot be regarded as espe-
cially common in general, and it is even more scarce inScandinavian countries (no reports of NSTI in burn pa-tients in Scandinavia);
– at admission, the clinical picture could all be explained bythe burn injury itself;
– LRINEC score on the day of development of septic shock =7 (Intermediate Risk for Necrotizing Soft Tissue Infection);17
– a biopsy from the pubic region was taken for culture ofkeratinocytes, and they grew adequately;
– there was no detection of foul smell, no dish-water fluid,no grey tissue but just dry, dead muscle and fat;
– necrosis of bones (ribs) is not a common feature in NSTI- more characteristic of coagulation/thrombi;
– history of drug abuse was not intravenous.
Conclusion
In the management of septic shock, special attention needsto be focused on the high treatment dose of vasopressors andthe ability of these agents to reduce organ and tissue blood flowthrough their vasoconstrictive actions. The utility of theseagents depends on the balance between increased specific per-fusion pressure and the direct effect on the microvasculature.Body weight increase in the acute post burn phase as an effectof the resuscitation makes this balance more difficult to main-tain. Guidelines for vasopressor dose calculation - adjustmentin burn patients with septic shock are advocated.
Fig. 5 - Pathophysiologic mechanisms involved in the development of is-chemic subcutaneous tissue necrosis in the present case.
BIBLIOGRAPHY
1. Greenhalgh DG: Sepsis in the burn patient: a different problem thansepsis in the general population. Burns Trauma, 5: 23, 2017.
2. Molos MA, Hall JC: Symmetrical peripheral gangrene and dissemi-nated intravascular coagulation. Arch Dermatol, 121: 1057-1061, 1985.
3. Beck V, Chateau D, Bryson GL, Pisipati A et al.: Cooperative antimi-crobial Therapy of Septic Shock (CATSS) Database Research Group.

Annals of Burns and Fire Disasters - vol. XXXI - n. 1 - March 2018
46
Timing of vasopressor initiation and mortality in septic shock: a cohortstudy. Crit Care, 18: R97, 2014.
4. Dellinger RP, Levy MM, Carlet JM, Bion J et al.: Surviving SepsisCampaign: international guidelines for management of severe sepsisand septic shock: 2008. Intensive Care Med, 34: 17-60, 2008.
5. Sakr Y, Reinhart K, Vincent JL, Sprung CL et al.: Does dopamine ad-ministration in shock influence outcome? Results of the sepsis occur-rence in acutely ill patients (SOAP) study. Crit Care Med, 34: 589-597,2006.
6. Zhou F, Mao Z, Zeng X, Kang H et al.: Vasopressors in septic shock: asystematic review and network meta-analysis. Therapeutics and Clini-cal Risk Management, 11: 1047-1059, 2015.
7. Dünser MW, Mayr AJ, Tür A, Pajk W et al.: Ischemic skin lesions as acomplication of continuous vasopressin infusion in catecholamine-re-sistant vasodilatory shock: incidence and risk factors. Crit Care Med,31: 1394-1398, 2003.
8. Kahn JM, Kress JP, Hall JB: Skin necrosis after extravasation of low-dose vasopressin administered for septic shock. Crit Care Med, 30:1899-1901, 2002.
9. Hayes MA, Yau EH, Hinds CJ, Watson JD: Symmetrical peripheralgangrene: association with noradrenaline administration. Intensive CareMed, 18: 433-436, 1992.
10. Bonamigo RR, Razera F, Cartell A: Extensive skin necrosis followinguse of noradrenaline and dopamine. J Eur Acad Dermatol Venereol, 21:565-566, 2007.
11. Kim EH, Lee SH, Byun SW, Kang HS et al.: Skin necrosis after a low-dose vasopressin infusion through a central venous catheter for treatingseptic shock. Korean J Intern Med, 21: 287-290, 2006.
12. Cho AR, Kim JI, Kim EJ, Son SM: Skin necrosis after high dose vaso-pressor infusion in septic shock. Korean J Crit Care Med, 27: 182-186,2012.
13. Loubani OM, Green RS: A systematic review of extravasation and localtissue injury from administration of vasopressors through peripheral in-travenous catheters and central venous catheters. J Crit Care, 30:653.e9-17, 2015.
14. Holmes CL, Patel BM, Russell JA, Walley KR: Physiology of vaso-pressin relevant to management of septic shock. Chest, 120: 989-1002,2001.
15. Yefet E, Gershovich M, Farber E, Soboh S: Extensive epidermal necro-sis due to terlipressin. Isr Med Assoc J, 13: 180-181, 2011.
16. http://www.nexobrid.com/clinical-evidence/prescribing-information/(Accessed January 2018).
17. Lancerotto L, Tocco I, Salmaso R, Vindigni V, Bassetto F: Necrotizingfasciitis: classification, diagnosis, and management. J Trauma AcuteCare Surg, 72: 560-566, 2012.
ANNALS OF BURNS AND FIRE DISASTERS
Journal of the Euro-Mediterranean Council
for Burns and Fire Disasters (MBC)
Journal of the European Burns Association (EBA)
Journal de la Société Française de Brûlologie (SFB)
On the INTERNET http://www.medbc.com/annals
for:
Contents International abstracts
Complete articles Announcements
The WHO pages MBC news
Book reviews Informatics news
Meditline (Pending Publication)