-
Page 1 of 32
Return on Investment (ROI) Project
Final Report 26th October 2012
Authors: Dr Alex Collie, Chief Research Officer
Ms Pauline Zardo, Research Translation Officer Dr Sue Gargett,
Health Economist
Ms Jane Monk, Consultant
For further information regarding this report please contact: Dr
Alex Collie
Chief Research Officer Institute for Safety Compensation and
Recovery Research
Level 11, 499 St Kilda Road, Melbourne 3004 VIC, Australia
Email: [email protected]
Telephone: +61 (0) 3 9097 0610
mailto:[email protected]
-
Page 2 of 32
EXECUTIVE SUMMARY A primary objective of the Institute for
Safety Compensation and Recovery Research (ISCRR) is to conduct
excellent health and safety, compensation and recovery research
that positively impacts the performance of WorkSafe Victoria and
the Transport Accident Commission. Assessment of its impact,
including return on investment is one of ISCRRs key performance
indicators. In late 2011, the ISCRR Board initiatied a Return on
Investment (ROI) project to assess the impact of ISCRRs research on
WorkSafe and the TAC, and to establish a method for assessing the
impact of ISCRRs research that can be embedded in ongoing
operations of the institute. The ROI project has three components,
including:
1. A series of nine detailed case studies of ISCRR research
projects to assess in depth the qualitative and quantitative impact
of the projects on WorkSafe, the TAC and their stakeholders.
2. A content analysis of information captured in ISCRRs project
management system to (a) assess the extent of adoption of ISCRR
research by WorkSafe, the TAC and their stakeholders and (b)
identify factors that lead to adoption of ISCRR research.
3. A content analysis of ISCRR project level information and the
findings of the case studies to determine the number of projects
for which impact could be demonstrated as well as the types of
impact.
The total financial investment in the nine case studies to date
is $725,000. The financial return on investment has included a $1.5
million actuarial release from the Noise Induced Hearing Loss
project (a five fold ROI), a $1.8 million cost avoided from the
Implantable Pain Therapies evidence review, and costs avoided of up
to $6.8 million for the Body Weight Supported Treadmill Training
evidence review. The financial impact of three TAC focussed
projects is yet to be determined. These estimates will be known in
coming months as the impact of the research on claims costs at TAC
become clearer. In addition, the non-financial value of the
projects has been substantial, and includes positive changes in the
culture of evidence-based decision making at both WorkSafe and the
TAC, increasing the understanding within the TAC of the impact of
claims management processes on TAC clients, improvements in
research capability amongst leading injury research group at
Monash, enabling the implementation of Recovery model at the TAC,
establishing a basis for important health policy positions at
WorkSafe and the TAC, and enabling enhanced interactions between
rehabilitation coordinators and TAC clients. The research has also
enabled the continuance of an important workplace safety debate in
the community (i.e., quad bikes safety devices). The impact of the
case studies is summarised in the table below. Analysis of data
captured in ISCRRs project management system identified evidence of
use of ISCRRs research in 27 of 30 individual projects that had
produced output by end August 2012. In 17 of these projects
qualitative information demonstrating the impact of the projects on
WorkSafe, the TAC or their stakeholders has been collected. Content
analysis identified five major types of impact, being financial
impacts (such as reductions in actuarial liabilities and costs
savings), claims processing and claims decision making impacts,
impacts on employers and the broader community. In addition, one
ISCRR project has demonstrated an impact on the health and
wellbeing of compensable clients with severe injury.
-
Page 3 of 32
-
Page 4 of 32
Table: Summary of ROI from nine case studies
CASE STUDY INVESTMENT RETURN
Noise Induced Hearing Loss
$312,000 $1.5 million actuarial release
Allowed WorkSafe to focus its strategic response to growing
hearing loss costs
Quad bike Safety Devices $10,500 Re-ignited public debate around
important workplace safety issue
Contributed to a 'case for change' in safety standards
Contributed to community behavioural change
Client Perceptions of Recovery
$37,700 Enhanced understanding of TAC role in improving client
experience
Provided information for the education of claims officers
Provided opportunity for key researcher to engage with TAC
Contributed to capacity building in research team at Monash
Implantable Pain Therapies
$73,400 $1.8 million in costs avoided consisting of $0.65m in
costs saved over 3 years to June 2012 and $1.16 million in future
costs avoided.
Contributed to change in culture towards evidence based decision
making
Helped WorkSafe to contain a potential "cost-blowout"
Leant credibility of WorkSafe policy of reviewing IPT
requests
Body Weight Supported Treadmill Training
$65,600 Contributed to a shift towards evidence-based decision
making in TAC.
Provided a foundation for an important health services policy
position.
$17k to $342k in current costs avoided, depending on scenario
modelled.
Potential liability saving of up to $6.8 million in costs
avoided.
Musculoskeletal Disorders Toolkit
$71,600 In one participating organisation, involvement in the
research led to:
increased knowledge and skills re work-related MSK
disorders,
increased communication on OHS in the workplace,
increased involvement of staff in OHS issues, and
the introduction of initiatives to enhance skill
development.
Pelvic Ring Fractures $36,000 Improved physical and mental
health outcomes for severely injured TAC clients where there was a
surgical intervention.
Financial impact yet to be determined.
-
Page 5 of 32
Evaluation of the Client Conversational Tool
$106,300 Provides TAC Rehabilitation Coordinators with a greater
insight into client needs.
The CCT-revised is more usable, more likely to be administered
in specified timeframes and more likely to be completed by
rehabilitation coordinators than the CCT.
Financial impact yet to be determined.
Return to Work Predictive Model
$10,000 plus $500 in ongoing operational costs p.a.
Enabled Recovery model implementation
Led to earlier interactions with TAC clients
Facilitated enhanced client / rehabilitation coordinator
relationships.
Financial impact yet to be determined.
Content analyses identified eight factors that influence the
adoption of ISCRRs research including engagement and interactions,
alignment with partner strategic priorities, timeliness of
research, ease of implementation, partner organisations structure
and processes, risk and issue prioritisation, the presence (or
absence) of an internal champion for the research, and the
credibility of the research method and source. This analysis
provide substantial value to ISCRR, as it informs ongoing
development of our project development and translation system to
ensure that research findings are more likely to be adopted. This
analysis identified a substantial return on investment from ISCRR
projects to date. While there is some inherent uncertainty in the
financial estimates, the financial ROI calculated for three of the
case studies demonstrates a return on investment that is many times
the investment in the research. Other projects have demonstrated
the substantial non-financial value for WorkSafe and the TAC from
ISCRR research. The analysis has been undertaken on a small
proportion of completed projects from the ISCRR research portfolio.
As ISCRRs research program matures the financial and non-financial
benefits to WorkSafe and the TAC may grow.
-
Page 6 of 32
CONTENTS Section Page
1. Title Page 1
2. Executive Summary 2
3. Contents 5
4. Acknowledgments 6
5. Background and Context 7
6. Objectives 10
7. Project Governance 11
8. Methods 12
9. Impact Assessment Framework 13
10. Case studies 16
11. Adoption of ISCRR research 18
12. Impact of ISCRR research 24
13. Summary and conclusions 26
14. References 29
15. List of Appendices 30
-
Page 7 of 32
ACKNOWLEDGEMENTS Collation of a body of work such as this is
only possible with the active involvement of a large number of
people. The authors would like to acknowledge the substantial
number of individuals within ISCRRs three partner organisations who
have contributed to this report. Names and position titles of
individuals who have contributed information to the case studies
are included in the appendices. In addition we would like to
acknowledge Ms Khic Huoy-Prang from ISCRR who assisted with data
analysis for some case studies, and Mss May Cheng and Dora Qian
from Corporate Finance, Monash who assisted with financial
statements data. Of particular note we would like to thank the
members of the ISCRR Return on Investment Committee:
Mr Chris Latham (ISCRR) and Professor Niki Ellis (ISCRR) for
providing leadership throughout the ROI project including chairing
the committee meetings and ensuring the project met the diverse
needs of ISCRRs partners.
Dr Duncan Buckeridge (Monash) for critical input into the
development of the Impact Assessment Framework and methodology for
assessing quantitative impact throughout the project.
Mr David Gifford (TAC) and Ms Julie Evans (WorkSafe Victoria)
for substantial contribution to methods development and for
overseeing the quantative evaluation on a number of case
studies.
Mr Tehn Chin (WorkSafe Victoria) and Mr David Attwood (TAC) for
contributions to case studies including undertaking a number of
quantative analysis and regular engagement and interaction with the
project team.
Mr Tony Tenaglia (ISCRR) for contributions to individual case
studies and strategic input throughout the project.
Ms Gillian Syres (ISCRR) for early leadership of the ROI project
including contributions to developing the Impact Assessment
Framework.
The project would not have been possible without the substantial
contributions of the ROI group.
-
Page 8 of 32
-
Page 9 of 32
BACKGROUND AND CONTEXT
The Institute for Safety Compensation and Recovery Research
ISCRR was established in April 2009 as a joint initiative of
WorkSafe Victoria (WorkSafe), the Transport Accident Commission
(TAC) and Monash University (Monash) to provide a sound research
and evidence base to improve compensation scheme policy, practice
and performance. The collaboration provides an opportunity to
achieve a best practice model in multi-disciplinary industry-led
research and to provide support for TAC and WorkSafe strategic
directions and future operations. ISCRRs goals, as identified in
its Strategic Plan to 2015, are to:
1. Have high impact on compensation scheme performance. Set,
deliver and translate a research agenda that will positively impact
on WorkSafe and TAC scheme operations and performance, both in the
short and long-term.
2. Create a model of excellence for industry led research.
Create a best practice model for multi-disciplinary,
industry-driven research based on strong stakeholder engagement and
supported by a broad funding base.
3. Be acknowledged leaders in compensation scheme research.
Maximise the value of research undertaken by driving local and
overseas partnerships and leading the national research effort in
our areas of focus.
Measuring research impact There is a growing focus amongst
academic research organisations and research funding agencies on
conducting research with real world impact and on the measurement
of the return on research investment. This is embodied in part by
the Monash Universitys research strategy which has the goals of
conducting both excellent research and research with impact.
Increasingly, Australian and international research organisations
are developing methods of measuring return on investment (ROI) in
research (Clay et al, 2006; Collie 2010, Kingwell et al, 2006). For
example the Murdoch Childrens Research Institute (MCRI) has
developed a method that includes evaluation of eight indicators
across three categories: knowledge creation; inputs to research;
and commercial, clinical and public health outcomes (Schapper et
al, 2012). With a few notable exceptions (Insight Economics, 2006)
most efforts focus on assessing ROI in areas relevant to academic
research institutions, such as knowledge dissemination, research
income and capacity building. ISCRR is uniquely placed to assess
the impact of its research on both conventional academic indicators
and on the policies and practices of its partner funding agencies.
ISCRR conducts applied research and has established strong
collaborative relationships with WorkSafe and the TAC that should
facilitate the use of its research. This final report describes the
outcomes of the institutes ROI project to 18th October 2012.
-
Page 10 of 32
The ISCRR research pipeline At the time of writing, ISCRR had
been operating for 3 years and 6 months (April 2009 to October
2012). As per the Strategic Plan published in 2010, ISCRR is coming
towards the end of its development phase.1 A feature of this stage
was delivering short term value to the institutes partner
organisations (Figure 1, taken from the ISCRR Strategic Plan 2010
to 2015). This project seeks to assess the short term value
delivered to WorkSafe and the TAC. A second purpose for the project
is to develop an impact assessment methodology that can be
integrated into ISCRRs ongoing program management systems beyond
2012.
Figure 1. ISCRR phases of development
Evidence from previous Australian research impact evaluations
suggests that on average, evidence of economic impact requires nine
years to realise from the point of research initiation (Insight
Economics, 2006). During its 3 years of operations, ISCRR has
established a substantial research portfolio encompassing over 100
individual projects. This ROI project has focussed on those that
have reached the adoption and impact stage of the research pipeline
(Figure 2)2. These projects represent less than a quarter of all of
ISCRRs current research projects.
1 ISCRR Strategic Plan, 2010 to 2015 2 Data taken from ISCRR
June 2012 quarterly research status report. Note that projects can
be in multiple stages at any
point in time (eg, active and producing output).
-
Page 11 of 32
Figure 2. The ISCRR research pipeline as at 30 June 2012
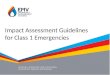
As ISCRR has developed, there has also been a substantial growth
in research output (Figure 3), measured both in terms of reports to
WorkSafe and the TAC and peer reviewed academic research
publications. Many of the instances of research use (or adoption)
and impact cited in this report have arisen from projects that
produced output during the 9/10 and 10/11 financial years. As
ISCRRs research outputs grows, it is reasonable to expect a growth
in instances of research adoption and impact, as the outputs are
used by WorkSafe, the TAC and their stakeholders.
Figure 3. ISCRR research output 2009/10 to 2011/12.
0
5
10
15
20
25
30
35
2009/10 2010/11 2011/12
Reports to Partners
Peer-reviewed Publications
-
Page 12 of 32
OBJECTIVES The ROI project was initiated by the Board of ISCRR
in late 2011 to develop a method for assessing the impact of ISCRRs
research on WorkSafe and the TAC. The output from the project is
one input to the ISCRR review being conducted in late 2012. It is
anticipated that the outcomes of the ROI project will be considered
by the review team. The ROI project has four objectives: 1. To
develop a framework for assessing research impact; 2. To determine
the impact of ISCRR research on WorkSafe and the TAC; 3. To
determine the factors that have contributed to the adoption of
ISCRR research by
WorkSafe and the TAC; and 4. To develop a model for measuring
return on investment that can be embedded in
ISCRRs ongoing operations. This document is the Final Report of
the project. It addresses all of the above objectives.
-
Page 13 of 32
PROJECT GOVERNANCE The ROI project is an initiative of the ISCRR
Board and is governed by a steering committee (the ROI committee)
that reports to the ISCRR Board. Formation of the ROI committee was
approved at the February 2012 Board meeting and noted at the March
2012 Relationship Management Committee (RMC) meeting. The committee
includes representation from WorkSafe Victoria, the TAC, Monash and
ISCRR, and is chaired by the Acting Chair of the ISCRR Board.
Members include:
Mr Chris Latham (Chair)
Mr David Gifford, Head Business Intelligence and Risk, TAC
Mr David Attwood, Senior Manager Claims Research, TAC
Ms Julie Evans, Manager Actuarial Services, WorkSafe
Victoria
Mr Tehn Chin, Actuarial Consultant, WorkSafe Victoria
Mr Duncan Buckeridge, Research Strategy Advisor, Monash
University
Prof Niki Ellis, CEO, ISCRR
A/Prof Alex Collie, Chief Research Officer, ISCRR
Mr Tony Tenaglia, Corporate Services Manager, ISCRR A project
team based at ISCRR reports to the ROI committee. The project team
is responsible for conducting the ROI project and includes the
following members:
A/Prof Alex Collie, Chief Research Officer, ISCRR
Dr Susan Gargett, Health Economist, ISCRR
Ms Jane Monk, Consultant, ISCRR
Ms Pauline Zardo, Research Translation Officer, ISCRR The ROI
committee has met monthly from February 2012 to guide the
project.
-
Page 14 of 32
METHODS The methods developed for the ROI project are described
in a separate document attached in Appendix A. In brief there are
three separate components to the project:
1. A series of nine case studies of ISCRR research projects to
assess in depth the qualitative and quantitative impact of the
projects on WorkSafe, the TAC and their stakeholders.
2. A content analysis of information routinely captured in
ISCRRs project management system to (a) assess the extent of
adoption of ISCRR research by WorkSafe, the TAC and their
stakeholders and (b) identify factors that lead to adoption of
ISCRR research.
3. A content analysis of ISCRR project level information and the
findings of the case
studies to identify types of impact. The methods document was
endorsed by the ROI Committee at their August 2012 meeting and is
provided at Appendix A.
-
Page 15 of 32
IMPACT ASSESSMENT FRAMEWORK The first component of the ROI
project entailed the development of an Impact Assessment Framework.
The Framework was adapted from models developed by Duncan
Buckeridge and further developed by the ROI project team in
collaboration with the ROI committee over the period December 2011
to March 2012. The framework was updated and finalised in September
2012. The Framework was used to guide the case studies and the
adoption and impact content analyses. In essence, the Framework
describes five stages of the research continuum and the methods
that may be used to assess research projects at each stage of the
continuum. The five stages are: 1. Planning and development of
research. 2. Conduct of research. 3. Outputs of research. 4.
Adoption of research outputs. 5. Impact of research.
At any point in time, individual research projects may be
located at one or more points along this continuum. It is
anticipated that all research projects will produce outputs, and
that most, ideally all, of these will lead to adoption and
impact.
Each of the five phases has multiple, varied components. For
example, a variety of research methods may be used in the conduct
of research. Similarly, adoption of research may be indirect (e.g.,
influencing the thinking of a person or group at WorkSafe or the
TAC) or direct (e.g., used to establish or support a policy
position). The impact of research may be measured qualitatively
(e.g., influencing a strategic discussion within the schemes) or
quantitatively (e.g., as a financial impact, reduction in claim
lodgement).
The Framework establishes a foundation for the ROI evaluation
methods, and is now the basis for ISCRRs routine research
reporting. The Framework document is provided at Appendix B, and
was endorsed by the ROI committee at their September 2012
meeting.
-
Page 16 of 32
CASE STUDIES A series of nine case studies were identified by
the ROI committee for detailed analysis of return on investment.
Cases represent a sample of the portfolio of ISCRR research
projects, selected using a set of criterion described in the
methods document. Cases could be either stand-alone research
projects or sub-studies arising from larger research projects.The
nine case studies are listed in Table 1. Table 1. List of ROI cases
agreed for inclusion
CASE STUDY TARGET ORGANISATION
RESEARCH PROGRAM
ROI METHOD
Return to Work Predictive model TAC RTW/Recovery Qual &
Quant* Noise induced hearing loss WS OHS Qual & Quant
Implantable pain therapies review WS/TAC HDSD Qual & Quant Body
weight supported treadmill training
TAC HDSD Qual & Quant
Quad bike safety devices WS OHS Qual only Client conversational
tool TAC Comp Systems Qual & Quant* Client perceptions of
recovery TAC Comp Systems Qual only Pelvic ring fractures TAC
RTW/Recovery Qual & Quant* Toolkit for MSK disorders WS OHS
Qual only Note: Qual = qualitative assessment of impact; Quant =
quantitative assessment of financial impact except for asterisked
case studies (*) where quantitative measurements included non
financial metrics.
Nine case study documents are appended to this report
(Appendices C to K). For three of the case studies the financial
impact is yet to be evaluated, including:
Pelvic Ring Fractures
Client Conversational Tool
Return to Work Predictive Model These three case studies will be
completed in coming months as the required TAC claims cost
information becomes available for analysis. Each case study
contains the background to the research project and an assessment
of the qualitative and/or quantitative impact of the research on
WorkSafe and/or the TAC and/or their stakeholders. The case studies
represent a cross section of ISCRRs research portfolio, including
projects from the Occupational Health and Safety, Health and
Disability Services Delivery and Return to Work research programs.
The case studies also include evidence reviews, a development grant
and a stand-alone project. The case studies are included as
appendices to this document.
-
Page 17 of 32
Summary of case study outcomes Table 2 summarises the output of
the case studies as at 27th October.
Table 2. Summary of case study outcomes
CASE STUDY INVESTMENT RETURN
Noise Induced Hearing Loss
$312,000 $1.5 million actuarial release
Allowed WorkSafe to focus its strategic response to growing
hearing loss costs
Quad bike Safety Devices $10,500 Re-ignited public debate around
important workplace safety issue
Contributed to a 'case for change' in safety standards
Contributed to community behavioural change
Client Perceptions of Recovery
$37,700 Enhanced understanding of TAC role in improving client
experience
Provided information for the education of claims officers
Provided opportunity for key researcher to engage with TAC
Contributed to capacity building in research team at Monash
Implantable Pain Therapies
$73,400 $1.81m in costs avoided consisting of $0.65m in costs
saved over 3 years to June 2012 and $1.16m in future costs
avoided.
Contributed to change in culture towards evidence based decision
making
Helped WorkSafe to contain a potential "cost-blowout"
Leant credibility of WorkSafe policy of reviewing IPT
requests
Body Weight Supported Treadmill Training
$65,600 Contributed to a shift towards evidence-based decision
making in TAC.
Provided a foundation for an important health services policy
position.
$17k to $342k in current costs avoided, depending on scenario
modelled.
Potential liability saving of up to $6.8 million in costs
avoided.
Musculoskeletal Disorders Toolkit
$71,600 In one participating organisation, involvement in the
research led to:
increased knowledge and skills re work-related MSK
disorders,
increased communication on OHS in the workplace,
increased involvement of staff in OHS issues, and
the introduction of initiatives to enhance skill
-
Page 18 of 32
development.
Pelvic Ring Fractures $36,000 Improved physical and mental
health outcomes for severely injured TAC clients.
Financial impact yet to be determined.
Evaluation of the Client Conversational Tool
$106,300 Provides TAC Rehabilitation Coordinators with a greater
insight into client needs.
The CCT-revised is more usable, more likely to be administered
in specified timeframes and more likely to be completed by
rehabilitation coordinators than the CCT.
Financial impact yet to be determined.
Return to Work Predictive Model
$10,000 plus $500 in ongoing operational costs p.a.
Enabled Recovery model implementation
Led to earlier interactions with TAC clients
Facilitated enhanced client / rehabilitation coordinator
relationships.
Financial impact yet to be determined.
A diverse range of impacts have emerged from the projects
studied, including both qualitative and financial or other
quantitative impacts. As at 3rd October 2012, it has been possible
to demonstrate a financial ROI in three of the case studies. These
include a $1.5 million actuarial release realised for WorkSafe from
the Noise Induced Hearing Loss project, $1.8 million cost avoided
from the Implantable Pain Therapies evidence review, and a
potential in costs avoided of up to $6.8 million for the Body
Weight Supported Treadmill Training evidence review. The total
financial investment in the nine case studies to date has been
approximately $725,000. Qualitative feedback received has
demonstrated the substantial non-financial value of ISCRRs
research. For example, in relation to the Implantable Pain
Therapies project (and other evidence reviews completed by ISCRR),
it has been observed by senior clinical convenor of the HSG that
ISCRR research has contributed to a culture of evidence based
decision making at WorkSafe and the TAC:
Evidence Service Reviews are the most applied aspect of ISCRRs
work. Evidence Service Reviews are designed to give WorkSafe and
the TAC the upper ground
in discussion on clinical decisions and sharpens the focus of
practitioners in their clinical decision making.
Dr Peter Harcourt, Clinical Convenor, Health Services Group
Other qualitative feedback indicated that ISCRR research had
sparked a public debate on an important workplace safety issue. In
relation to the evidence review on crush protection devices on quad
bikes, it was noted that the report
reignited tension in the debate regarding the use of Crush
Protection Devices in preventing Quad bike fatalities
-
Page 19 of 32
Ross Pilkington, Director, Health and Safety Operations,
WorkSafe Victoria Still other senior executives noted the potential
of ISCRRs research to influence future decision making at WorkSafe
and the TAC. For example, in relation to the Client Perceptions of
Recovery project: In my view, this is one of the most important
external pieces of research TAC has received,
from the client perspective. David Gifford, Executive Manager,
Business Intelligence, TAC
ISCRRs research program has also delivered value for Monash. In
relation to the Client
Perceptions of Recovery project, the lead researcher Associate
Professor Belinda Gabbe
noted that:
this research was the first qualitative research undertaken
within the context of the Victorian
State Trauma Registry and the Victorian Orthopaedic Trauma
Outcomes Registry. The
findings of this study have been hugely beneficial for improving
our understanding of the
trauma patients experience with the trauma system and the
impacts of injury. In addition,
the project provided a great opportunity to build capacity
within the research team to
undertake Qualitative Research. In addition to building
Qualitative Research capacity, strong
international links were established with experienced social
scientists in the field from the
University of Surrey and University College London. The
collaborations established will
extend into future projects."
The case studies provide a snapshot of the return delivered via
a relatively small series of ISCRR projects. It is anticipated that
in future, similar analyses of projects currently in the
development, activity or output stage of the research cycle will
reveal a further diversity of impact and demonstrate the value of
ISCRRs research to its partner organisations.
-
Page 20 of 32
ADOPTION OF ISCRR RESEARCH Another component of the ROI project
has been analysis of all ISCRR research projects to determine the
factors that have contributed to the adoption of research by
WorkSafe and/or the TAC. This component seeks to address two
questions, being:
What attributes of a project lead to research findings being
adopted and used to inform policy, programs and practice?
What attributes of a project lead to research findings NOT being
adopted and used to inform policy, programs and practice?
The term project is used in its broadest sense to include the
research, project management, project governance and
communications. The detailed methods for this analysis are
described in Appendix A.
Factors influencing adoption of ISCRR research Thirty (30)
projects met the criteria for inclusion in the analysis. Note that
for the purposes of this analysis, each evidence review produced
under the auspices of the Evidence Service project were considered
to be individual projects. Of these, ISCRR had recorded evidence of
adoption for 27 projects. The remaining 3 projects did not have any
evidence of adoption recorded on ISCRRs project management system.
Of those projects with evidence of adoption:
18 arose from a specific request from WorkSafe/ TAC for the
research.
4 arose from an investigator initiated processes, including
development grants.
5 arose from collaborative development of the research scope and
methods. The type of adoption was categorised according to the 3
typologies of research utilisation described by Hanney et al (2003)
following Weiss (1979). These included:
Instrumental use of research (N=17 projects). This indicates
research that was used directly in policy formation or decision
making. For example, an evidence review on intrathecal infusions
was used to review and revise a treatment payment policy by the
TAC/WorkSafe health services group.
Symbolic use of research (N=7 projects). This refers to use of
research to support a position already taken, or to support debate
for particular potential policy positions or strategic directions,
which may be to continue with existing policies or courses of
action. For example, the client outcomes evidence review confirmed
that the TACs approach to measuring client outcomes as an
organisational key performance indicator was unique within
Australia and internationally.
Conceptual use of research (N=3 projects). This refers to use of
research to provide insight into an issue or problem rather than
directly used in policy formation or
-
Page 21 of 32
decision making. For example, an evidence review on mediation
and return to work has been used to inform the WorkSafe RTW
division about the issue, without any specific action being taken
to date.
Content analysis identified eight factors as barriers or
facilitators of adoption. These are described in the table
below.
Table 2. Factors leading to adoption of ISCRR research
ADOPTION FACTORS
DESCRIPTION EXAMPLE
Engagement and Interaction
Sponsor/Contact Engagement
Researcher Engagement
Project Manager engagement
Stakeholder Engagement
Quality of Interactions
The degree and quality of engagement between the
researcher/research team and the business sponsor/contact.
Research projects with high levels of engagement between
researcher and the project business sponsor/contact were associated
with successful adoption. Low sponsor/researcher engagement
associated with adoption failure or adoption lags.
High ISCRR Project Management engagement was also associated
with effective adoption. Stakeholder engagement (other relevant
people involved other than sponsor/contact) was also associated
with adoption success. The right stakeholders need to be engaged to
enable successful adoption.
Poor quality/limited interaction between parties was associated
with lack of adoption; poor quality communication between parties
and during interactions was associated with lags or lack of
adoption.
The Quad Bike Evidence review was developed following
significant interaction and communication between the project key
contact and the researcher. The project sponsor also ensured other
key stakeholders were engaged. The researcher was responsive to the
project key contact throughout the research process, even
maintaining contact and positive communications when delivery dates
were pushed back.
Both the researcher and the project key contacts engagement and
the high quality of thier interactions was critical to the success
of this piece of research, which has been experienced as highly
relevant, timely and actionable by WorkSafe and the broader injury
prevention community.
Alignment with Partner Strategic Priorities
WorkSafe / TACs perception of the relevance of the research with
regard to their current priorities.
Research that is perceived as directly
The WorkHealth Evaluation is directly linked to deliverables of
the WorkHealth program
-
Page 22 of 32
ADOPTION FACTORS
DESCRIPTION EXAMPLE
relevant to current work being undertaken and directly related
to user needs was adopted. Research questions that were very
specific and resulted in very specific findings were experienced as
relevant and were adopted.
Research that was not considered to be well aligned with partner
strategic priorities failed to be adopted.
undertaken by WorkSafe.
The researchers measure the uptake and impact of the WorkHealth
initiative following its implementation. The on-going provision of
results have been used by the project sponsor and contact to
communicate the progress and success of the project to WorkSafe and
the Victorian community throughout the life of the WorkHealth
program.
Ease of Implementation
The extent to which the research findings were actionable, or
able to contribute to a decision. Research that provided clear,
actionable recommendations were adopted. In other words, research
that enabled a decision to be made, whether this was at the
conceptual or practical level, was more likely to be adopted.
Research where implementation was low cost or required relatively
little effort were adopted.
The Evidence Service Review on NENET was adopted quickly after
completion of the report. Implementation involved informing
clinicians and claims managers about the evidence around NENET, and
led to the development and immediate use of a NENET database to
capture information about NENET claims management.
Timeliness
Delivery of research while the issue is still being addressed or
considered by WorkSafe / the TAC.
Research findings that are delivered within policy timeframes,
or while the issue is already being addressed internally, enables
adoption. Research findings provided while an issue is considered a
hot topic are more likely to be adopted, if this window is missed
adoption is less likely. Alignment in timeframes between when
research findings are delivered and when policy decisions must be
made is important for
The NIHL project was undertaken while there was also an active
internal WorkSafe Steering committee addressing the issue. The
research was fed directly into this steering committee to inform
decision making by the key contact.
This research findings were delivered while this issue was
considered a hot topic, and when solutions had not
-
Page 23 of 32
ADOPTION FACTORS
DESCRIPTION EXAMPLE
adoption. been identified/finalised or implemented.
Partner Organisational Structures and Processes
WorkSafe and TAC organisational and structural process can
affect adoption.
Having a structure or process in place to receive the research
and process the findings facilitated adoption. For example,
evidence reviews arising from the Evidence Service project were
delivered directly to the HSG Health Policy Governance Group.
Substantial changes in organisational process and infrastructure
affecting project sponsors and contacts during the period within
which research was undertaken were predominantly experienced as a
barrier to adoption.
The Work Related Fatalities project, one that was not adopted,
experienced difficulties due to a significant organisational
restructure occurring during the project. This resulted in the
WorkSafe project sponsor and contact changing several times
throughout the life of the project. The new business sponsors had a
different perspective of the relevance of the research to those who
initiated it, contributing to lack of adoption.
Internal champion for research
Research projects that have a strong champion or sponsor for the
research within WorkSafe / the TAC have been adopted. Research
related to government directives are also likely to have a strong
internal champion and to be adopted. Where such ownership has been
lacking or where there is internal organisational disagreement
about adoption there have been barriers to adoption.
The TAC 2015 Evaluation has had consistent and strong
leadership, interest and involvement by senior managers in the TAC.
This has been critical to the swift adoption of research arising
from this project, for example the implementation of a revised
version of the TAC Client Converstional Tool.
Risk and Issue Prioritisation
Research related to areas with high/rising claims costs are more
likely to be adopted in a timely fashion.
Research focussed on low priority issues and/or competing
priorities were less likely to be adopted or to have a lag in
adoption.
Often low priority was described as not a large cost issue or
not a rising cost issue.
The Intrathecal Evidence Service Review was adopted quickly as
this issue was linked with rising claims costs. Adoption involved
the development of a policy and claims management procedure
regarding Intrathecal Infusions.
Other evidence service
-
Page 24 of 32
ADOPTION FACTORS
DESCRIPTION EXAMPLE
Negative financial impact related to implementing research was
associated with non-adoption.
reviews delivered at similar times, e.g. Benzodiapines have been
partially adopted (claims managers and clinicians have been using
the informatino to inform discussion with clients) but the actual
policy document has not been updated to reflect and reference the
evidence review because the issue is not linked rising or high
claims costs, so not viewed as priority work.
Credibility of Research Method and Source
Credibility of research methods/scientific analysis process
supports adoption. Where the researcher is considered a trusted
source that enables adoption. That research is understood as
unbiased/objective allows for decisions to be made where there is
lack of clarity or difference of opinions.
In the case of both the Art Therapy and BWSTT Evidence reviews
the credibility and the objectivity of the research was critical to
its adoption. The objective evidence provided by the review allowed
for a decision to be made where there was prior disagreement about
the efficacy of these treatments and whether or not they should be
compensated.
Comparison with prior research The factors identified in this
content analysis are aligned with factors identified in research
and systematic reviews of barriers and enablers to use of research
evidence. Engagement and Interaction, Alignment with Partner
Strategic Priorities, Timeliness and Risk and Issue Prioritisation
are clearly linked with the three factors most frequently
identified in systematic reviews: timeliness; interaction between
researchers and policy makers; and accordance between researchers
and policy maker strategies, priorities, values and interests
(Lavis, 2009). Research on use of evidence has also identified the
critical role of research champions and leaders. Internal Champion
for research reflects these findings, which has found that research
that is informed, supported and disseminated by leaders and
influential individuals
-
Page 25 of 32
is more likely to be perceived as valuable and relevant by key
stakeholders and therefore adopted into practice (Mitton, 2007;
Greenhalgh, 2004). Similarly, research has also shown that choice
of researcher and research communicator is an important influencing
factor affecting use of research.Studies have shown that where
there is poor choice of researcher or research communicator (i.e.
researcher not considered expert or experienced, or the
communicator has poor speaking or presentation skills etc) research
is unlikely to be adopted into practice (Mitton 2007; Orton et al
2011).The factor Credibility of Research Method and Source is
consistent with these findings. In a systematic review by Mitton et
al (2007) barriers and enablers to use of evidence were identified
as related to either: the individual, the organisation,
communication or time. The factors identified in this analysis can
also be associated with these categories. Factors exisiting at the
individual level and related to communication include: Engagement
and Interaction; Internal Champion for Research; and Credibility of
Research Method and Source. The organisational level factors
identified here were: Alignment with Partner Strategic Priorities;
Ease of Implementation; Partner Organisational Structures and
Processes; and Risk and Issue Prioritisation. Timeliness is related
to time.
Implications for ISCRR Information about the factors affecting
use of evidence in specific decision making contexts, such as that
provided by this content analysis, can be used to target and tailor
the design and implementation of tools, strategies and
interventions seeking to increase use of evidence and increase the
likelihood of their effectiveness (Greenhalgh, 2004; Pawson 2005;
Dobrow 2004; Scott 2012). This analysis has substantial
implications for ISCRRs future research activities. It provides a
useful framework of the factors that influence the likelihood that
research will be adopted. The challenge for ISCRR is to integrate
this knowledge into research development and project management
processes. The evolution of ISCRRs recently developed programmatic
approach to research management provides an opportunity to embed
these principles into business as usual processes at ISCRR. For
example, one can foresee a checklist of critical factors being
established as a set of go/no-go criterion for new projects under
consideration by the institutes Program Advisory Groups (PAGs) or
Board.
-
Page 26 of 32
IMPACT OF ISCRR RESEARCH The final component of the ROI project
is a content analysis of those ISCRR research projects that have
led to impact. This component seeks to address two questions:
How many ISCRR projects have had a demonstrable impact on
WorkSafe, the TAC and/or their stakeholders?
What are the types of impact that ISCRR research has had on
WorkSafe, the TAC and their stakeholders?
Once again the term project is used in its broadest sense to
include the research, project management, project governance and
communications. The detailed methods for this analysis are
described in Appendix A.
Number of projects having impact Of the twenty seven projects
for which ISCRR had documented evidence of adoption:
17 had demonstrated impact
10 had no documented evidence of impact (yet). Note that for the
purposes of this analysis, each evidence review produced under the
auspices of the Evidence Service project was considered to be an
individual project. Of those projects identified as having
impact:
11 arose from a specific request from WorkSafe/ TAC for the
research. These were all evidence reviews.
3 arose from an investigator initiated processes. These included
2 development grants and a research fellowship.
3 arose from collaborative development of the research scope and
methods. These included 2 evaluations of major WorkSafe and TAC
policy initiatives, and a mixed-methods study of noise induced
hearing loss.
Of those projects with evidence of impact, all had qualitative
evidence of impact in the form of spoken feedback obtained from
WorkSafe or TAC staff or documented feedback. The case studies
undertaken (described above) also provided quantitative evidence of
impact.
Types of impact Impacts ranged from increasing community
awareness of health and safety issues to changes in TAC claims
processes to improvements in WorkSafe scheme viability via
actuarial releases. Content analysis identified five major types of
impact. These are described in the table below with examples to
illustrate each type.
-
Page 27 of 32
Table 3. Types of impact
TYPE OF IMPACT
DESCRIPTION EXAMPLE
Community/public perception impact
Driving improvements in community perceptions, understanding and
awareness of workplace safety issues and solutions.
The Quad bike evidence review re-ignited a public debate
regarding the use of Rollover Protection Devices on quad bikes used
in agricultural settings.
Claims processing impacts
Impact related to changes in operational or decision making
processes, particularly claims handling processes.
The evaluation of the Client Conversational Tool (CCT), led to a
revision of the tool and a revised process for its administration
that was implemented by the TAC in April 2012. Similarly, the RTW
predictive model contributed to a new process for early
identification of TAC clients at-risk of poor return work
outcomes.
Claims decision making impacts
Claims managers and clinical panel members are able to make
evidence informed decisions about provision of appropriate
treatment and services, including benefits and risks to the
client.
The Body Weight Supported Treadmill Training evidence review
enabled the TAC to make a decision not to support funding of the
Lokomat service for spinal cord injured clients.
Financial impacts
Impacts related to changes in claims costs or liabilities, or
costs avoided.
The Noise Induced Hearing Loss project was considered to have
led to a $1.5 million reduction in claims liabilities for WorkSafe
Victoria.
Employer impacts Impacts around employer awareness and
perception of workplace health, safety and compensation issues.
The WorkHealth evaluation has informed employer awareness
campaigns that have raised the profile of workplace health
promotion in the state.
Client impacts Impacts on TAC client or injured worker health
and well-being.
The Pelvic Ring Fractures project demonstrated that TAC clients
receiving a certain surgical procedure had superior physical and
mental health outcomes than those managed conservatively.
-
Page 28 of 32
SUMMARY AND CONCLUSIONS This report of the ROI project sought to
determine the impact of ISCRR research on WorkSafe and the TAC and
their stakeholders. A second aim was to examine factors that led
projects to be adopted and to develop a typology of impact to
enable a more nuanced understanding of what things lead to adoption
of ISCRR research by WorkSafe and the TAC and how ISCRRs research
is being used by the two schemes. Two primary research methods have
been used, being a series of detailed case studies and a content
analysis of project level information held in ISCRRs program
management systems.
What has been the return on investment? The case studies provide
evidence of the different ways in which ISCRRs research has
delivered value for WorkSafe and the TAC. In some cases it has been
possible to measure this value using quantitative methods,
including estimation of the economic impact of the project. The
total financial investment in the nine case studies to date has
been $725,000. The financial return on investment has included a
$1.5 million actuarial release from the Noise Induced Hearing Loss
project (a five fold ROI), a $1.8 million cost avoided from the
Implantable Pain Therapies evidence review, and potential costs
avoided of up to $6.8 million for the Body Weight Supported
Treadmill Training evidence review. While there is some inherent
uncertainty in the financial estimates, the financial ROI
calculated for three of the case studies demonstrates a return on
investment that is many times the investment in the research. The
financial impact of three TAC focussed projects is yet to be
determined. These estimates will be known in coming months as the
impact of the research on claims costs at TAC become clearer. In
addition, the non-financial value of the projects has been
substantial, and includes positive changes in the culture of
evidence-based decision making at both WorkSafe and the TAC,
increasing the understanding within the TAC of the impact of claims
management processes on TAC clients, improvements in research
capability amongst leading injury research group at Monash,
enabling the implementation of Recovery model at the TAC,
establishing a basis for important health policy positions at
WorkSafe and the TAC, and enabling enhanced interactions between
rehabilitation coordinators and TAC clients. The research has also
enabled the continuance of an important workplace safety debate in
the community (i.e., quad bikes safety devices). Analysis of data
captured in ISCRRs project management system identified evidence of
use of ISCRRs research in 27 of 30 individual projects that had
produced output by end August 2012. In 17 of these projects
qualitative information demonstrating the impact of the projects on
WorkSafe, the TAC or their stakeholders has been collected. Content
analysis identified five major types of impact, being financial
impacts (such as reductions in actuarial liabilities and costs
savings), claims processing and claims decision making impacts,
impacts on employers and the broader community. A single project
also demonstrated an impact on client health and wellbeing. Content
analyses identified eight factors that influence the adoption of
ISCRRs research including engagement and interactions, alignment
with partner strategic priorities, timeliness
-
Page 29 of 32
of research, ease of implementation, partner organisations
structure and processes, risk and issue prioritisation, the
presence (or absence) of an internal champion for the research, and
the credibility of the research method and source. This analysis
provide substantial value to ISCRR, as it informs ongoing
development of our project development and translation system to
ensure that research findings are more likely to be adopted. The
analysis also identified some features of projects that are less
likely to be used by WorkSafe, the TAC or their stakeholders. The
findings are also highly relevant for the partner organisations
activities as they demonstrate that effective use or translation of
research findings requires active engagement from the research
end-user. The analysis has been undertaken on a small proportion of
completed projects from the ISCRR research portfolio. As ISCRRs
research program matures the financial and non-financial benefits
to WorkSafe and the TAC may grow.
Next Steps Apart from achieving its primary purpose of measuring
ISCRRs impact, including return on investment, as required by its
key performance indicators, the findings of this ROI project will
be applied in a number of ways. First the final report will be
provided to the ISCRR review team. It is expected that it will
receive an informed critical appraisal in this process. Secondly,
the ROI methodology developed will be incorporated into ISCRRs
ongoing project management system to continue to improve the way
ISCRR routinely captures information on adoption and impact. The
results of the analysis will be presented to industry partners to
enable a discussion about the ways in which those organisations can
facilitate translation of research. It is anticipated that this may
lead to process changes within the partner organisations. Finally,
the academic value of this exercise will be exploited via research
publications and presentations. Having reviewed the published
research literature in this field, the authors are of the opinion
that ISCRRs impact assessment methodology is a unique example of
how to assess return on research investment. Dissemination of the
methodology via conventional research avenues will help to raise
the profile of ISCRR in the research translation field.
-
Page 30 of 32
REFERENCES Clay MA, Donovan C, Butler L, Oldenburg BF. The
returns from cardiovascular research: the impact of the National
Heart Foundation of Australias investment. Med J Aust 2006; 185:
209-212.
Collie A. Gains in neurotrauma research activity and output
associated with a Victorian state government funding program.
Medical Journal of Australia 2010; 712-714. Dobrow, M.J., Goel, V.,
Upshur R.E.G. Evidence Based Health Policy: Context and
Utilisation. Social Science and Medicine 2004; 58: 207-217.
Greenhalgh, T., Robert, G., Macfarlane, F., Bate, P., Kyriakidou,
O. Diffusions of Innovations in Service Organisations: Systematic
Review and Recommendations. Milbank Quarterly 2004; 82(4):
581-629.
Insight Economics. Economic impact study of the CRC programme.
Canberra: Insight Economics, 2006.
http://www.universitiesaustralia.edu.au/documents/news/media_releases/2006/CRC_Economic_Impact_Study-Oct06.pdf
(accessed Apr 2010)
Kingwell BA, Anderson GP, Duckett SJ, et al. Evaluation of NHMRC
funded research completed in 1992, 1997 and 2003: gains in
knowledge, health and wealth. Med J Aust 2006; 184: 282-286.
Lavis, J. How Can We Support the Use of Systematic Reviews in
Policymaking? Plos Medicine 2009; 6(11).
Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review--a
new method of systematic review designed for complex policy
interventions. Journal of Health Services Research and Policy 2005:
10(1); 21-34.
Mitton, C., Adair, C.E., McKenzie, E., Patten, S.B., Waye Perry,
B. Knowledge Transfer and Exchange: Review and Synthesis of the
Literature. Milbank Quarterly 2007; 85(4) 729-768.
Orton L, Lloyd-Williams F, Taylor-Robinson D, O'Flaherty M,
Capewell S. The use of research evidence in public health decision
making processes: systematic review. PLoS One 2011; 6(7).
Schapper CC, Dwyer T, Tregear GW, Aitken M, Clay MA. Research
performance evaluation: the experience of an independent medical
research institute. Aust Health Rev. 2012 May;36(2):218-23. Scott
SD, Albrecht L, O'Leary K, Ball GD, Hartling L, Hofmeyer A, Jones
CA, Klassen TP, Kovacs Burns K, Newton AS, Thompson D, and Dryden
DM. Systematic review of knowledge translation strategies in the
allied health professions. Implementation Science. 2012;
7(1):70.
http://www.ncbi.nlm.nih.gov/pubmed?term=Pawson%20R%5BAuthor%5D&cauthor=true&cauthor_uid=16053581http://www.ncbi.nlm.nih.gov/pubmed?term=Greenhalgh%20T%5BAuthor%5D&cauthor=true&cauthor_uid=16053581http://www.ncbi.nlm.nih.gov/pubmed?term=Harvey%20G%5BAuthor%5D&cauthor=true&cauthor_uid=16053581http://www.ncbi.nlm.nih.gov/pubmed?term=Walshe%20K%5BAuthor%5D&cauthor=true&cauthor_uid=16053581http://www.ncbi.nlm.nih.gov/pubmed?term=Orton%20L%5BAuthor%5D&cauthor=true&cauthor_uid=21818262http://www.ncbi.nlm.nih.gov/pubmed?term=Lloyd-Williams%20F%5BAuthor%5D&cauthor=true&cauthor_uid=21818262http://www.ncbi.nlm.nih.gov/pubmed?term=Taylor-Robinson%20D%5BAuthor%5D&cauthor=true&cauthor_uid=21818262http://www.ncbi.nlm.nih.gov/pubmed?term=O'Flaherty%20M%5BAuthor%5D&cauthor=true&cauthor_uid=21818262http://www.ncbi.nlm.nih.gov/pubmed?term=Capewell%20S%5BAuthor%5D&cauthor=true&cauthor_uid=21818262http://www.ncbi.nlm.nih.gov/pubmed/22624645http://www.ncbi.nlm.nih.gov/pubmed/22624645
-
Page 31 of 32
Wells R, Whitworth JA. Assessing outcomes of health and medical
research: do we measure what counts or count what we can measure?
Aust New Zealand Health Policy 2007; 4: 14-17. http:/ /
www.ncbi.nlm.nih.gov/pmc/articles/PMC1929109/ (accessed Apr 2010).
Zardo P, Collie A. Use of evidence in public health policy: An
injury compensation policy content analysis. Accident Analysis and
Prevention (submitted).
-
Page 32 of 32
LIST OF APPENDICES
a. Methods document
b. Impact Assessment Framework document
c. Noise Induced Hearing Loss case study
d. Client Perceptions of Recovery case study
e. Quad Bike Safety Devices case study
f. Implantable Pain Therapies case study
g. Body Weight Supported Treadmill Training case study
h. Musculoskeletal Disorders Toolkit case study
i. Pelvic Ring Fractures case study
j. Client Conversational Tool case study
k. Return to Work Predictive Model case study
x. Calculation of overhead costs