Embed Size (px)
Citation preview

78 Am J Clin Pathol 2015;144:78-86 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
AJCP / Original Article
Isolated del(5q) in Patients Following Therapies for Various Malignancies May Not All Be Clinically Significant
Guilin Tang, MD, PhD,1 Rashmi Shivani Goswami, MD,1 Cynthia S. Liang,1 Carlos E. Bueso-Ramos, MD,1 Shimin Hu, MD, PhD,1 Courtney DiNardo, MD,2 and L. Jeffrey Medeiros, MD1
From the Departments of 1Hematopathology and 2Leukemia, The University of Texas MD Anderson Cancer Center, Houston.
Key Words: Deletion 5q; Post–cytotoxic therapy; Therapy-related myeloid neoplasm
Am J Clin Pathol July 2015;144:78-86
DOI: 10.1309/AJCPBADO22WXOFHJ
ABSTRACT
Objectives: Deletion 5q is a common chromosomal abnormality in both de novo and therapy-related myeloid neoplasms (t-MNs). The detection of isolated del(5q) in patients following therapies for various malignancies raises serious concern for an emerging t-MN.
Methods: We identified 25 patients who developed isolated del(5q) following cytotoxic therapy (n = 21) or tyrosine kinase inhibitor (TKI; n = 4) therapy. Twenty-four patients had an interstitial and one had a terminal 5q deletion. The 5q31/EGR1 gene was deleted in 20 patients and intact in five patients. The clone size as assessed by metaphase analysis was minor (10%-30%) in 12 patients and large (45%-100%) in 13 patients. After a median follow-up of 17 months, none of the 12 patients with a minor del(5q) clone developed t-MN; del(5q) disappeared in four patients and persisted in eight patients. By contrast, 12 of 13 patients with a large del(5q) clone developed t-MN, and del(5q) was persistent in all patients who had follow-up cytogenetic testing.
Conclusions: Development of del(5q) in patients following cytotoxic therapies or TKI may not always be associated with t-MN. A close follow-up seems an appropriate approach for patients who had a minor del(5q) clone.
Cytogenetic abnormalities involving chromosome 5, either monosomy 5 or a long-arm deletion del(5q), are common findings in de novo myelodysplastic syndromes (MDS) and acute myeloid leukemia (AML), as well as therapy-related myeloid neoplasms (t-MNs).1 Monosomy 5 is frequently associated with multiple cytogenetic abnor-malities (complex karyotype), whereas del(5q) may occur in isolation.2-4 Isolated del(5q) has been considered as an adverse prognostic factor in AML.5 In contrast, isolated del(5q) in de novo MDS, often referred to as 5q– syndrome in the literature, is often associated with good prognosis. The 5q– syndrome is characterized by macrocytic anemia, a normal or elevated platelet count, small and hypolobated megakaryocytes, and a low rate of progression to AML.6 This disease has been classified as a distinct entity, desig-nated as “MDS with isolated del(5q)” by the 2008 World Health Organization classification.1
t-MNs, including therapy-related AML (t-AML) and therapy-related MDS (t-MDS), are late complications of cytotoxic therapies (chemotherapy and/or radiation) used in the treatment of both malignant and nonmalignant dis-eases.1 Cytogenetic abnormalities can be detected in more than 90% of the patients with t-MN, and more than half of these patients have a complex karyotype.1,2,7 Abnormalities involving chromosomes 5 and 7 are most common, present-ing in 60% to 70% of patients with t-MDS/AML,8 and are often associated with prior exposure of alkylating agents or ionizing radiation.2,8,9 Del(5q) is the most common struc-tural abnormality detected in patients with t-MN, in approxi-mately 20% of these patients.2
Although del(5q) is a frequent abnormality encountered in MDS/AML and thought to contribute to the pathogenesis

AJCP / Original Article
Am J Clin Pathol 2015;144:78-86 79 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
in t-MN, we have observed patients who have developed isolated del(5q) following cytotoxic therapies but had not yet developed t-MN with close clinical follow-up.10 In addi-tion, many of the clonal cytogenetic abnormalities emerging after tyrosine kinase inhibitor (TKI) treatment for chronic myelogenous leukemia (CML) have been reported to be of uncertain clinical significance,11-13 whereas the detection of isolated del(5q) has not been reported in this particular clini-cal setting, and its clinical significance is unknown.
To understand the clinical significance of development of isolated del(5q) in the posttherapy setting, we retrospectively reviewed the cytogenetic archives at our hospital for patients who acquired isolated del(5q) following cytotoxic chemother-apy/radiotherapy or TKI treatment. We performed a detailed clinical, pathologic, and cytogenetic review and performed fluorescence in situ hybridization (FISH) in all patients.
Materials and Methods
PatientsWe searched the database of the Clinical Cytogenet-
ics Laboratory at The University of Texas MD Anderson Cancer Center from 2003 through 2014 for del(5q) as the sole clonal abnormality. We then selected patients who had received cytotoxic chemotherapy/radiotherapy or TKI for prior malignancies before developing del(5q). A detailed chart review was conducted in all patients, with a focus on history of malignancies and therapies, as well as patient outcomes. All samples were collected following institutional guidelines with informed consent in accordance with the Declaration of Helsinki.
Peripheral Blood and Bone Marrow AssessmentsPeripheral blood (PB) smears, bone marrow (BM)
aspirate smears, and trephine biopsy specimens were evalu-ated for morphologic evidence of dysplasia and the percent-age of blasts. BM cellularity was evaluated in BM biopsy specimens. The involvement of BM by primary cancer was evaluated by morphology, immunohistochemistry and/or flow cytometry immunophenotyping analysis, or molecular analysis (BCR/ABL in patients with CML). CBC at the time of del(5q) detection and during follow-up was reviewed.
Conventional Chromosomal AnalysisConventional chromosomal analysis was performed on
G-banded metaphases prepared from unstimulated 24-hour and 48-hour BM aspirate cultures (for primary diagnosis of myeloid neoplasms or solid tumors) or unstimulated 24-hour and mitogen-stimulated 72-hour BM aspirate cultures (for primary diagnosis of lymphoma or myeloma) using standard
techniques. Mitogens included lipopolysaccharide, oligonu-cleotides, 12-O-tetradecanoylphorbol-13-acetate, and inter-leukin 4. Twenty metaphases were analyzed, and the results were reported using the International System for Human Cytogenetic Nomenclature (2013).14
FISH Analysis or Combined Morphologic and FISH Analysis
FISH analysis alone or combined with morphologic analysis was performed in all patients with D5S721, D5S23/EGR1 probes (Abbott Molecular, Des Plaines, IL). The posi-tive cutoff value for del(5q) established in our laboratory is 4%. Two hundred nuclei were counted, and the percentage of cells with EGR1 deletion was calculated. Combined mor-phologic and FISH analysis was described previously15 with minor modifications. In brief, morphologic evaluation and image capture were performed on Wright-Giemsa–stained BM aspirate smears; smears were then destained using 1% acid alcohol, followed by protease II (Abbott Molecular) treatment and hybridization with D5S721 and D5S23/EGR1 probes. The target cell populations were captured under a fluorescence microscope.
Statistical AnalysisThe unpaired t test was used for numerical comparisons.
The c2 and Fisher exact tests were applied for categorical variables. The latency interval was estimated from the ini-tiation of chemotherapy/radiotherapy or TKI therapy to the development of del(5q). Overall survival (OS) was estimat-ed by the Kaplan-Meier method from the date of detection of del(5q) until death from any cause.
Results
PatientsDel(5q) as a sole clonal cytogenetic abnormality was
found in 117 patients during the past 12 years at our institu-tion. Among these patients, 25 acquired this abnormality in their BM after being treated with cytotoxic agents or TKI for the prior malignancies ❚Table 1❚ and formed the study group. These included 13 male and 12 female patients, with a medi-an age of 64 years (range, 45-76 years). The primary malig-nancies included chronic lymphocytic leukemia/small lym-phocytic lymphoma (CLL/SLL, n = 6), CML (n = 4), breast cancer (n = 4), diffuse large B-cell lymphoma (DLBCL, n = 2), plasma cell myeloma (PCM, n = 2), and AML with t(8;21), follicular lymphoma, peripheral T-cell lymphoma, metastatic squamous cell carcinoma, lung adenocarcinoma, and esophageal adenocarcinoma (n = 1 each; details listed in Table 1). One patient (case 18) had both DLBCL and PCM

Tang et al / Isolated Del(5q) Following Therapies for Malignancies
80 Am J Clin Pathol 2015;144:78-86 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
diagnosed 2 months apart. The prior therapies included TKI (n = 4), radiotherapy alone (n = 2), chemotherapy alone (n = 14), chemotherapy plus radiotherapy (n = 2), and chemo-therapy plus autologous stem cell transplant (SCT, n = 3) (Table 1). Two patients (cases 8 and 10) were included in a previous study.10
PB and BM FindingsAt the time of del(5q) detection, six patients (cases 4, 7,
12, and 16-18) were still receiving chemotherapy and four patients were taking TKIs (cases 1, 2, 3, and 13). BM was positive for primary cancer in seven patients: two patients (cases 5 and 7) showed 50% involvement by CLL/SLL, four patients (cases 6, 10, 17, and 18) showed minimal involve-ment (1%-5%) by CLL or PCM, and one patient (case 1) showed minimal residual CML at the molecular level with complete cytogenetic remission.
Among the 12 patients who had a minor del(5q) clone (10%-30% of metaphases), one patient (case 4) had pancyto-penia, two (cases 6 and 11) had isolated thrombocytopenia, one (case 3) had isolated anemia, and the other eight patients had a normal CBC. The median of the WBC count was 5.1
× 109/L (range, 1.8-30.6 × 109/L); hemoglobin level, 12.4 g/dL (range, 9.4-15.4 g/dL); and platelet count, 130 × 109/L (range, 28-272 × 109/L). Among the 13 patients with a large del(5q) clone (45%-100% of metaphases), three (cases 17, 21, and 22) had pancytopenia, three (cases 15, 23, and 25) had anemia and thrombocytopenia, three (cases 14, 16, and 20) had isolated thrombocytopenia, two (cases 18 and 24) had isolated anemia, one (case 19) had isolated leukopenia, and only one patient (case 13) had a normal CBC. The median of the WBC count was 6.8 × 109/L (range, 2.1-26.8 × 109/L); hemoglobin level, 10 g/dL (range, 8.3-14.5 g/dL); and platelet count, 76 × 109/L (range, 17-591 × 109/L). The hemoglobin level was significantly lower in patients with a large del(5q) clone than in patients with a minor clone (P = .0027), whereas WBC and platelet counts were comparable between patients with minor or large del(5q) clones (P = .3771 and P = .8262, respectively). Of note, two patients (cases 23 and 25) showed circulating blasts.
The median of BM cellularity was 50% (range, 5%-95%). Increased BM blasts were seen in three patients (cases 22, 23, and 25, with 16%, 41%, and 40%, respectively). Overt dysplasia was noted in nine patients (cases 14, 15, 17, 20-25),
❚Table 1❚Demographic, Clinical, and Pathologic Features and Outcomes of 25 PatientsCase No. Sex Age, y Primary Disease Therapies for Primary Disease Myelodysplasiaa
Follow-up,b mo t-MN? Outcome
1 F 47 CML Tyrosine kinase inhibitors No 8 No AWD2 M 73 CML Tyrosine kinase inhibitors No 59 No Died3 F 68 CML Tyrosine kinase inhibitors No 11 No Died4 F 74 CLL/SLL R–hyper-CVAD No 5 No AWD5 M 51 CLL/SLL R-FND No 60 No AWD6 M 53 CLL/SLL Fludarabine, cyclophosphamide, rituximab No 49 No AWD7 F 72 CLL/SLL Fludarabine, cyclophosphamide, rituximab No 92 No AWD8 F 53 DLBCL R-CHOP No 59 No AWR9 M 55 PCM Multiple chemotherapies, SCT No 38 No AWD10 M 70 PCM Multiple chemotherapies No 24 No AWD11 F 65 Breast cancer Radiotherapy Erythroblasts (mild) 40 No Died12 M 65 SCC Chemo/radiotherapy (unknown in detail) No 36 No AWR13 F 76 CML Tyrosine kinase inhibitors Small megakaryocytes 16 No AWD14 F 49 Follicular lymphoma R-CHOP, SCT Trilineage 1 t-MDS Died15 M 73 T-cell lymphoma Hyper-CVAD Trilineage 4 t-MDS Died16 M 63 CLL/SLL Fludarabine, cyclophosphamide, rituximab Megakaryocyte 3 t-MDS Died17 M 60 CLL/SLL Fludarabine, cyclophosphamide, rituximab Trilineage 17 t-MDS Died18 F 57 DLBCL, PCM CHOP, bortezomib, steroids Megakaryocyte 16 t-MDS Died19 M 45 DLBCL R-CHOP, SCT Insufficient 76 t-MDS AWR20 M 56 AML with t(8;21) Fludarabine, cytarabine, G-CSF Trilineage 19 t-MDS Died21 F 70 Breast cancer Radiotherapy Trilineage 1 t-MDS Died22 M 73 Esophageal cancer Etoposide, fluorouracil, radiotherapy Trilineage, 16% blasts 3 t-MDS Died23 F 75 Breast cancer Cyclophosphamide, doxorubicin Trilineage, 41% blasts 11 t-AML Died24 F 59 Breast cancer Adjuvant chemotherapy (unknown in detail) Trilineage 41 t-MDS AWR25 M 71 Lung cancer Etoposide, carboplatin Trilineage, 40% blasts 5 t-AML Died
AML, acutete myeloid leukemia; AWD, alive with disease; AWR, alive with remission; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; CML, chronic myelogenous leukemia; DLBCL, diffuse large B-cell lymphoma; FND, fludarabine, mitoxantrone, and dexamethasone; G-CSF, granulocyte colony-stimulating factor; Hyper-CVAD, hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with high-dose methotrexate and cytarabine; PCM, plasma cell myeloma; R, rituximab; SCC, squamous cell carcinoma; SCT, stem cell transplant; t-AML, therapy-related acute myeloid leukemia; t-MDS, therapy-related myelodysplastic syndrome.
a At the time while del(5q) was detected. b Follow-up length (months) after detection of del(5q). Cases 19, 20, and 24 received allogeneic stem cell transplant.

AJCP / Original Article
Am J Clin Pathol 2015;144:78-86 81 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
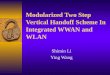
and mild/occasional dyspoiesis was noted in four patients (cases 11, 13, 16, and 18). Case 19 had a hypocellular BM and was insufficient for a complete morphologic evaluation; no evidence of dyspoiesis was seen in the other 11 cases. Small and hypolobated megakaryocytes were apparent in seven patients (cases 15, 17, 19-22, and 24) ❚Image 1A❚, mixed small and large megakaryocytes were noted in two patients (cases 14 and 16) ❚Image 1B❚, and megakaryocytes were markedly decreased in two patients (cases 23 and 25); no cases showed megakaryocytic hyperplasia.
On the basis of clinical and laboratory findings, seven patients (cases 14, 15, 17, 20-22, and 24) were diagnosed with t-MDS and two patients (cases 23 and 25) with t-AML at the time del(5q) was detected. For the remaining 16 cases, no diagnosis of t-MN was rendered since there were no clinical and/or morphologic grounds to support a diagnosis of t-MDS/AML.
Conventional Cytogenetic and FISH AnalysisThe baseline cytogenetic data before commencement of
therapy were available in 17 patients ❚Table 2❚. Four patients (CML, cases 1-3 and 13) had t(9;22)(q34;q11.2)[20]; case 20 (AML) showed 47,X,-Y,+8,t(8;21)(q22;q22),+18[20]; case 7 (CLL) showed 46,XX,add(14)(q32)[20]; case 17 (CLL) showed 46,XY,del(11)(q21q23)[4]/46,XY[16]; and the other 10 patients showed a normal diploid karyotype. None of the patients showed del(5q) prior to therapy. The median interval from the initiation of cytotoxic therapy or TKI therapy to the detection of del(5q) was 69 months (range, 5-243 months).
Detailed information for the del(5q) clone is listed in Table 2. The number of metaphases showing del(5q) by conventional chromosomal analysis ranged from two to 20 (10%-100%). Del(5q) was a minor clone (10%-30% of metaphases) in 12 patients (cases 1-12) and a major clone (55%-100%) in 11 patients (cases 13, 15, and 17-25); two patients (cases 14 and 16) showed del(5q) in 45% of meta-phases. One patient (case 10) showed terminal 5q deletion at band 5q11.2, and the other 24 cases showed interstitial 5q deletion from proximal breakpoints varying between bands of 5q11.2 and 5q22 to distal breakpoints varying between bands of 5q15 and 5q35, with the most common breakpoints at 5q13 and 5q33 (in 15 patients). There are two common (critical) deleted regions (CDRs) in 5q: 5q31 and 5q32-33. 5q31 was intact in five patients (cases 1, 4, 9, 11, and 14) and was deleted in the other 20 patients; 5q32-33 was intact in the above five patients plus case 21 and was deleted in the other 19 patients ❚Image 2❚.
FISH analysis was performed in all 25 cases. The EGR1 gene was intact in five patients (cases 1, 4, 9, 11, and 14) and deleted in 20 patients. The percentage of EGR1-deleted interphases ranged from 4% to 88%, slightly lower but proportional to the percentage of metaphases (r = 0.9403). Cases with lower del(5q) metaphases (10%-30%) had a lower percentage of EGR1-deleted interphases (4-11%), and cases with higher del(5q) metaphases (45%-100%) had a higher percentage of EGR1-deleted interphases (26%-88%) (Table 2). Of note, among the 12 patients with the minor del(5q) clone, eight had only two to three (10%-15%) meta-phases and 6% to 12% of interphases showing del(5q); the
A B
❚Image 1❚ Bone marrow biopsy specimen (H&E, ×40). Megakaryocytic morphology correlates with the deleted region in chromosome 5q. A, Case 18: megakaryocytes (arrows) are small and hypolobated; they do not form clusters. B, Case 14: dysplastic megakaryocytes (arrows). The size and morphology are variable; some are small with hypolobated nuclei, one with widely separated nuclear lobes.

Tang et al / Isolated Del(5q) Following Therapies for Malignancies
82 Am J Clin Pathol 2015;144:78-86 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
other four patients with del(5q) detected in four to six (20%-30%) metaphases had a deleted region that did not involve 5q31/EGR1, and the clone size could not be estimated by interphase FISH.
Combined morphologic and FISH analysis was per-formed on six cases with BM involvement by primary cancer (cases 5-7 and 17 with CLL and cases 10 and 18 with PCM); del(5q) was exclusively observed in myeloid and erythroid cells and not in lymphocytes or plasma cells ❚Image 3❚.
Follow-upThe median clinical follow-up after detection of del(5q)
was 17 months (range, 1-92 months). Three patients (cases 16, 18, and 19) showed worsening cytopenia and had BM rebiopsy at 2 to 5 months after del(5q) was detected. The BM exhibited convincing dysplastic features, and all three patients were diagnosed with t-MDS. In total, 12 of the 25 patients were diagnosed with t-MDS/AML. Patient 24 transformed into AML 2 years after the diagnosis of t-MDS.
Of the remaining 13 patients who were not diagnosed with t-MN, four had CML and were treated with TKIs, and nine patients had prior exposure to cytotoxic therapy. Case 13 had persistent del(5q) (35%-75% metaphases for three
times) and slightly worsening anemia (hemoglobin, 12.2 to 11.6 to 10.8 g/dL) but normal WBC and platelet counts during an 11-month follow-up; no overt dysplasia was noted in three separate BM biopsy specimens. Cases 4 and 11 showed aplastic BM and pancytopenia in PB; no overt dys-poiesis was noted. All other patients had a normal or close to normal CBC, and no dysplasia was noted in PB and BM.
Cytogenetic follow-up was available in 21 (84%) patients. Eighteen (72%) patients exhibited del(5q) in at least one follow-up BM sample (median, 2; range, 1-7). At last clinical follow-up, del(5q) disappeared in four (16%) patients and persisted in 17 (68%) patients (disappeared in three patients after allogeneic SCT), and four patients had no further cytogenetic testing (died of t-MN within 5 months prior to any repeat analysis) (Table 2). Interestingly, while del(5q) disappeared spontaneously in four patients with a minor clone, this phenomenon was not observed in patients with a large clone. The median length of detectable del(5q) was 12 months (range, 1-59 months), and patients with minor or large del(5q) clones showed a comparable del(5q) detectable time (12 vs 11 months, P = .3152). Two patients emerged with a separate new clone during clinical follow-up: case 5 with del(20q) in two metaphases and case 8 with i(5)(p10) in three metaphases. Four patients showed clonal
❚Table 2❚Cytogenetic Characters of 25 PatientsCase No. Karyotype Before Chemotherapy
Interval,a
mo Abnormal del(5q) CloneFISH for EGR1, %
Detect Times Disappear
Lasted, mo
Clonal Evolution
1 46,XX,t(9;22)(q34;q11.2)[20] 52 46,XX,del(5)(q13q22)[6] Negativeb 3 No 14 No2 46,XY,t(9;22)(q34;q11.2)[20] 72 46,XY,del(5)(q13q33)[3] 9 3 No 59 No3 46,XX,t(9;22)(q34;q11.2)[20] 80 46,XX,del(5)(q13q33)[2] 11 2 No 11 No4 46,XX[20] 21 46,XX,del(5)(q13q22)[4] Negativeb 2 No 5 No5 Unknown 80 46,XY,del(5)(q13q33)[2] 6 2 No 54 New clone6 46,XY[19] 5 46,XY,del(5)(q13q33)[2] 10 1 Yes 10 No7 46,XX,add(14)(q32)[20] 27 46,XX,del(5)(q13q33)[3] 12 2 No 34 No8 46,XX[20] 112 46,XX,del(5)(q13q33)[2] 8 4 No 57 New clone9 46,XY[20] 9 46,XY,del(5)(q15q23)[2] Negativeb 1 Yes 1 No10 46,XY[20] 71 46,XY,del(5)(q11.2)[2] 6 1 Yes 3 No11 46,XX[20] 9 46,XX,del(5)(q13q22)[6] Negativeb 5 No 21 No12 46,XX[20] 38 46,XY,del(5)(q13q33)[2] 6 3 Yes 10 No13 46,XX,t(9;22)(q34;q11.2)[20] 35 46,XX,del(5)(q15q33)[11] 35 3 No 11 No14 Unknown 243 46,XX,del(5)(q12q15)[9] Negativeb 1 NA NA No15 46,XY[20] 147 46,XY,del(5)(q13q33)[11] 26 1 NA NA No16 Unknown 109 45,X,-Y,del(5)(q15q33)[9] 35 2 No 2 No17 46,XY,del(11)(q21q23)[4]/46,XY[16] 38 46,XY,del(5)(q22q35)[13] 41 7 No 15 Yes18 Unknown 126 46,XX,del(5)(q15q33)[18] 51 2 No 11 Yes19 Unknown 67 46,XY,del(5)(q15q33)[11] 45 4 Noc 21 Yes20 47,X,-Y,+8,t(8;21)(q22;q22),+18[20] 77 46,XY,del(5)(13q33)[20] 78 4 Noc 15 Yes21 Unknown 59 46,XX,del(5)(q13q31)[17] 81 1 NA NA No22 Unknown 78 46,XY,del(5)(q13q33)[20] 76 2 No 3 No23 46,XX[20] 172 46,XX,del(5)(q13q33)[20] 85 4 No 7 No24 46,XX[20] 203 46,XX,del(5)(q22q35)[17] 36 5 Noc 33 No25 Unknown 35 46,XY,del(5)(q15q33)[20] 88 1 NA NA No
FISH, fluorescence in situ hybridization; NA, no answer (patient had only onetime chromosomal analysis).a From the initiation of chemotherapy/radiotherapy or tyrosine kinase inhibitor therapy to detection of del5q.b 5q deleted region does not involve EGR1 gene (located in 5q31).c Disappeared after stem cell transplant.

AJCP / Original Article
Am J Clin Pathol 2015;144:78-86 83 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
B
A
❚Image 2❚ Conventional cytogenetic and fluorescence in situ hybridization (FISH) analysis showing deletions of chromosome 5q (arrows). A, Case 17: karyotype 46,XY,del(5)(q22q35). B, Case 1: FISH with probes of D5S721, D5S23/EGR1 that map back a previously G-banded metaphase with del(5)(q13q22) shows a negative result of del(5q) (with two intact EGR1 signals). C-G,
Morphologic features of del(5q) at different breakpoints: case 10: del(5)(q11.2) (C), case 14: del(5)(q12q15) (D), case 1: del(5)(q13q22) (E), case 21: del(5)(q13q31) (F), and case 24: del(5)(q22q35) (G).
C D E F G

Tang et al / Isolated Del(5q) Following Therapies for Malignancies
84 Am J Clin Pathol 2015;144:78-86 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
evolution: three patients (cases 17, 19, and 20) showed a complex karyotype, and case 18 showed 46,XX,t(2;21)(p21;q22),del(5)(q15q33)[20].
Most of the 12 patients who developed t-MDS/AML (nine patients diagnosed at the time del(5q) was detected and three patients diagnosed during the follow-up) were treated with lenalidomide and hypomethylating agents. One patient (case 25) was treated with azacitidine and vorinostat (under a phase 2 clinical trial). Three patients (cases 19, 20, and 24) also received allogeneic SCT.
OutcomesAmong the 13 patients who did not develop t-MN, three
died of primary cancer or complications of BM suppression,
eight were alive with persistent disease, and two were alive with disease remission. The OS has not been reached. For the 12 patients who developed t-MN, 10 died and two were alive (cases 19 and 24 both received allogeneic SCT), with a median OS of 8 months. The OS of the patients with t-MN was significantly shorter than that of the patients who did not develop t-MN (P = .0015).
Discussion
In this study, we identified 25 patients who acquired del(5q) as a sole abnormality in their BM following cyto-toxic chemotherapy/radiotherapy or TKI therapy. Twelve
DC
BA
❚Image 3❚ Combined morphologic and fluorescence in situ hybridization (FISH) analysis with probes of D5S721, D5S23/EGR1 (×100). Del(5q) was detected in myeloid and erythroid lineages (arrows) but not in lymphocytes or plasma cells (arrowheads). A, B, Case 18, with involvement of plasma cell myeloma. C, D, Case 7, with involvement of chronic lymphocytic leukemia. A, C, Bone marrow smear stained with Wright-Giemsa. B, D, FISH analysis with probes of D5S721, D5S23/EGR1.

AJCP / Original Article
Am J Clin Pathol 2015;144:78-86 85 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
patients developed therapy-related MDS/AML, whereas this abnormality appeared to be clinically “silent” in the other 13 patients. We compared the clinical and cytogenetic charac-teristics of these patients and found several factors that may be helpful in determining the clinical significance of this cytogenetic abnormality.
Clone size of del(5q) appears to be critical. Theoretical-ly, clone size detected by interphase FISH is more accurate compared with that by counting dividing cells (metaphase analysis). Our data showed that the clone size by interphase FISH is proportional but overall smaller than abnormal metaphases identified by conventional chromosomal analy-sis. This likely is attributable to a gain of proliferative advan-tage of abnormal clones over normal cells. Nevertheless, all 12 patients with a minor del(5q) clone (10%-30% meta-phases) did not develop t-MN, while 12 of 13 patients with the del(5q) abnormality involving 45% to 100% metaphases developed t-MDS or t-AML. This finding is similar to what we have observed previously: most clinically “silent” clones present as a minor clone.10 Some of these minor del(5q) clones were transient and disappeared spontaneously (seen in four patients of our cohort); in contrast, all major del(5)q clones persisted. Furthermore, patients with a major del(5)q clone appeared to have an increased risk of clonal evolution (in four of 13 patients), whereas clonal evolution was not identified in patients with a minor del(5q) clone.
The deleted region also appears to be important. Most of the patients in our cohort and those reported in the literature showed interstitial deletion of 5q. Deletions of 5q are het-erozygous, and deleted regions can affect different genes.16 There are two CDRs on chromosome 5q, one located on 5q32-33 and the other located on 5q31. Several genes are thought to be the key players in the pathogenesis of 5q– syn-drome: (1) the RPS14 gene, located on 5q33.1, was identified as a critical gene for the erythroid phenotype of the 5q– syn-drome.17 Decreased expression of RPS14 causes a dramatic increase in total TP53 level and induces TP53 target gene expression and cell cycle arrest.18 (2) A microRNA cluster, including miR-143, miR-145, and miR-146a, located on 5q32-33, is important for the megakaryocytic phenotype of 5q– syndrome. In mice, decreased expression of both miR-145 and miR146 causes thrombocytosis and the hypolobated micro-megakaryocytes characteristic of the 5q– syndrome.19 (3) The EGR1 gene, located on 5q31, plays a role in hema-topoietic stem cell proliferation. Heterozygous loss or inactivation of the EGR1 gene increases the frequency of leukemia development.20,21 (4) Other genes located outside of CDRs, such as NPM1 (located on 5q35) and APC (located on 5q22), may also contribute to the disease phenotype and progression.22,23 In our cohort, 19 of 25 patients had both CDRs deleted, five patients (cases 1, 4, 9, 11, and 14) had both CDRs intact, and one patient (case 21) had one CDR
(5q31) deleted. Interestingly, four of five cases with both intact CDRs had a minor del(5q) clone and appeared to be clinically silent. In the only patient (case 14) who had both CDRs intact but developed t-MDS, the morphologic features were different from those of typical 5q– syndromes (Image 1B), raising the possibility that factors other than del(5q) might also play a role in the pathogenesis of t-MDS.
The type of treatment the patient received may also affect the outcome. del(5q) as a sole abnormality detected in patients with CML following TKI therapy has not been reported before. The most common chromosomal abnormalities reported in this clinical setting are loss of Y chromosome, monosomy 7/del(7q), +8, and del(20q).11-13 Interestingly, only three patients (two with monosomy 7 and one with a complex karyotype) developed t-MDS among 84 patients who developed clonal cytogenetic abnormalities during TKI therapy reported in three studies.11-13 Most of the chromosomal abnormalities were transient and of unknown clinical significance. In our cohort, four patients (cases 1-3 and 13) developed del(5q) after a median latency of 60 months. Two patients had del(5q) detected on three separate occasions over a period of 14 and 11 months, respectively (cases 1 and 13). All four patients had a close to normal or normal CBC and no overt myelodysplasia and showed major molecular responses to TKI therapy. Notably, in two of four patients, both CDRs were intact. In aggregate, del(5)q also appears to be clinically insignificant in this particular set-ting, like other clonal cytogenetic abnormalities occurring during TKI therapy.
Ten patients developed t-MDS in our cohort with a median OS of 8 months, which is similar to the OS of t-MN as a group,1,24 but is in striking contrast to a good prognosis of patients with 5q– syndrome (median OS >10 years). Stud-ies have suggested that additional factors might participate in the pathogenesis of AML and advanced forms of MDS with del(5q). For example, gene mutations have been shown to be more prevalent in t-MDS/AML, especially TP53 muta-tions. 5q– syndrome associated with TP53 gene mutations has been shown to have a significantly poorer prognosis.25 Unfortunately, most of our patients who did not develop t-MN had no molecular testing. Eight patients (cases 17 and 19-25) who developed t-MDS/AML had molecular testing for RAS, NPM1, c-KIT, JAK2, IDH1, IDH2, FLT3, and CEBPA mutations; case 23 showed an FLT3 internal tandem duplication, and case 25 showed IDH2 mutation.
In summary, isolated del(5q) developing in patients treated for a prior malignancy is not always associated with progression to a therapy-related myeloid neoplasm. Increased size of the del(5q) clone and the deletion of region 5q31 (EGR1 gene) appear to increase the risk of malignant progression. Importantly, we also identify that in patients with CML receiving TKI therapy, the development of

Tang et al / Isolated Del(5q) Following Therapies for Malignancies
86 Am J Clin Pathol 2015;144:78-86 DOI: 10.1309/AJCPBADO22WXOFHJ
© American Society for Clinical Pathology
isolated del(5)q, similar to other clonal cytogenetic abnor-malities, may not carry any clinical significance. Close follow-up and surveillance for clonal evolution rather than an immediate therapeutic intervention seem most appropri-ate for patients with a minor del(5q) clone and a morphologi-cally normal BM.
Corresponding author: Guilin Tang, MD, PhD, Dept of Hematopathology, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030-4009; [email protected].
Cynthia S. Liang conducted this project as summer intern at MD Anderson Cancer Center.
References 1. Swerdlow S, Campo E, Harris N, et al, eds. WHO
Classification of Tumors of Hematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2008.
2. Pedersen-Bjergaard J, Pedersen M, Roulston D, et al. Different genetic pathways in leukemogenesis for patients presenting with therapy-related myelodysplasia and therapy-related acute myeloid leukemia. Blood. 1995;86:3542-3552.
3. Ebert BL. Molecular dissection of the 5q deletion in myelodysplastic syndrome. Semin Oncol. 2011;38:621-626.
4. Haase D, Germing U, Schanz J, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;110:4385-4395.
5. Dohner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European Leukemia Net. Blood. 2010;115:453-474.
6. Hasserjian R, Le Beau MM, List AF, et al. Myelodysplastic syndrome with isolated del(5q). In: Swerdlow S, Campo E, Harris N, et al, eds. WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2008.
7. Qian Z, Joslin JM, Tennant TR, et al. Cytogenetic and genetic pathways in therapy-related acute myeloid leukemia. Chem Biol Interact. 2010;184:50-57.
8. Smith SM, Le Beau MM, Huo D, et al. Clinical-cytogenetic associations in 306 patients with therapy-related myelodysplasia and myeloid leukemia: the University of Chicago series. Blood. 2003;102:43-52.
9. Pedersen-Bjergaard J, Philip P, Larsen SO, et al. Therapy-related myelodysplasia and acute myeloid leukemia: cytogenetic characteristics of 115 consecutive cases and risk in seven cohorts of patients treated intensively for malignant diseases in the Copenhagen series. Leukemia. 1993;7:1975-1986.
10. Tang G, Wang SA, Lu V, et al. Clinically silent clonal cytogenetic abnormalities arising in patients treated for lymphoid neoplasms. Leuk Res. 2014;38:896-900.
11. Medina J, Kantarjian H, Talpaz M, et al. Chromosomal abnormalities in Philadelphia chromosome–negative metaphases appearing during imatinib mesylate therapy in patients with Philadelphia chromosome–positive chronic myelogenous leukemia in chronic phase. Cancer. 2003;98:1905-1911.
12. Jabbour E, Kantarjian HM, Abruzzo LV, et al. Chromosomal abnormalities in Philadelphia chromosome negative metaphases appearing during imatinib mesylate therapy in patients with newly diagnosed chronic myeloid leukemia in chronic phase. Blood. 2007;110:2991-2995.
13. Deininger MW, Cortes J, Paquette R, et al. The prognosis for patients with chronic myeloid leukemia who have clonal cytogenetic abnormalities in Philadelphia chromosome–negative cells. Cancer. 2007;110:1509-1519.
14. Shaffer LG, McGowan-Jordan J, Schmid M. An International System for Human Cytogenetic Nomenclature (2013): Recommendations of the International Standing Committee on Human Cytogenetic Nomenclature. Basel, Switzerland: S Karger; 2013.
15. Wang SA, Hutchinson L, Tang G, et al. Systemic mastocytosis with associated clonal hematological non-mast cell lineage disease: clinical significance and comparison of chromosomal abnormalities in SM and AHNMD components. Am J Hematol. 2013;88:219-224.
16. Ebert BL. Deletion 5q in myelodysplastic syndrome: a paradigm for the study of hemizygous deletions in cancer. Leukemia. 2009;23:1252-1256.
17. Ebert BL, Pretz J, Bosco J, et al. Identification of RPS14 as a 5q- syndrome gene by RNA interference screen. Nature. 2008;451:335-339.
18. Dutt S, Narla A, Lin K, et al. Haploinsufficiency for ribosomal protein genes causes selective activation of p53 in human erythroid progenitor cells. Blood. 2011;117:2567-2576.
19. Starczynowski DT, Kuchenbauer F, Argiropoulos B, et al. Identification of miR-145 and miR-146a as mediators of the 5q- syndrome phenotype. Nat Med. 2010;16:49-58.
20. Min IM, Pietramaggiori G, Kim FS, et al. The transcription factor EGR1 controls both the proliferation and localization of hematopoietic stem cells. Cell Stem Cell. 2008;2:380-391.
21. Joslin JM, Fernald AA, Tennant TR, et al. Haploinsufficiency of EGR1, a candidate gene in the del(5q), leads to the development of myeloid disorders. Blood. 2007;110:719-726.
22. Grisendi S, Bernardi R, Rossi M, et al. Role of nucleophosmin in embryonic development and tumorigenesis. Nature. 2005;437:147-153.
23. Wang J, Fernald AA, Anastasi J, et al. Haploinsufficiency of Apc leads to ineffective hematopoiesis. Blood. 2010;115:3481-3488.
24. Ok CY, Hasserjian RP, Fox PS, et al. Application of the International Prognostic Scoring System–Revised in therapy-related myelodysplastic syndromes and oligoblastic acute myeloid leukemia. Leukemia. 2014;28:185-189.
25. Kulasekararaj AG, Smith AE, Mian SA, et al. TP53 mutations in myelodysplastic syndrome are strongly correlated with aberrations of chromosome 5, and correlate with adverse prognosis. Br J Haematol. 2013;160:660-672.