Embed Size (px)
Citation preview
SCIENTIFIC LETTER
Isolated Sinusitis of Lateral Recesses of Sphenoid Sinus
Binit Sureka & Mahesh Kumar Mittal & Aliza Mittal &Brij Bhushan Thukral
Received: 6 May 2013 /Accepted: 26 August 2013# Dr. K C Chaudhuri Foundation 2013
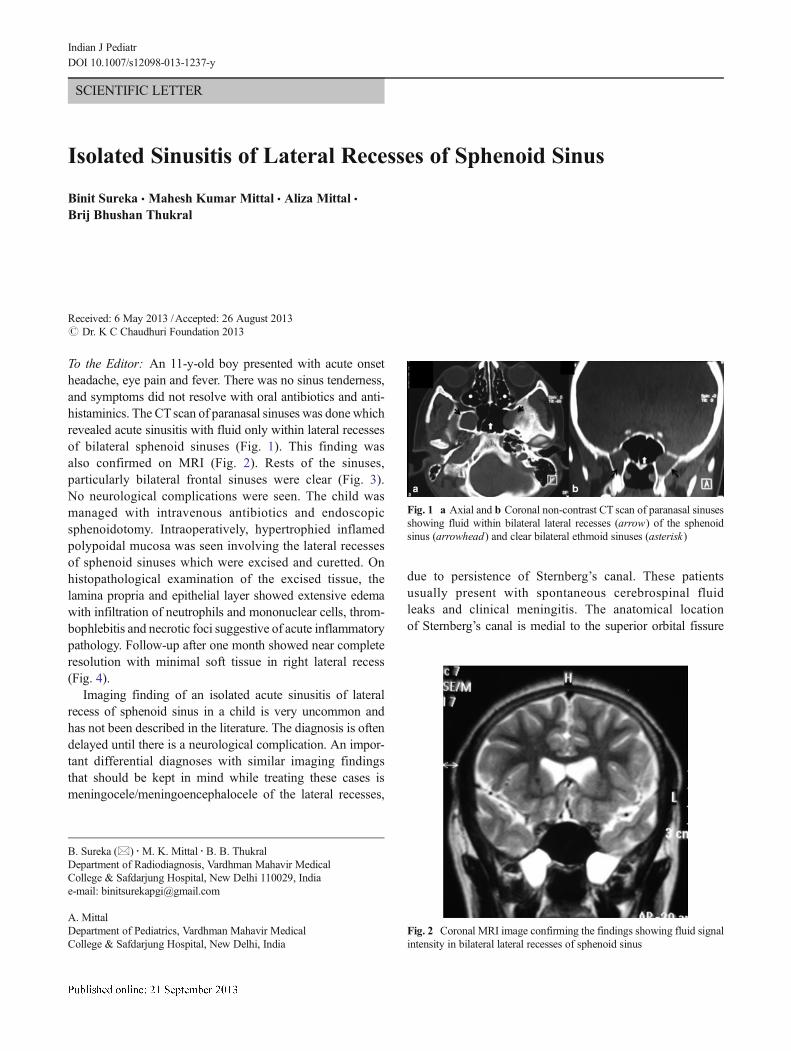
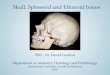
To the Editor: An 11-y-old boy presented with acute onsetheadache, eye pain and fever. There was no sinus tenderness,and symptoms did not resolve with oral antibiotics and anti-histaminics. The CTscan of paranasal sinuses was done whichrevealed acute sinusitis with fluid only within lateral recessesof bilateral sphenoid sinuses (Fig. 1). This finding wasalso confirmed on MRI (Fig. 2). Rests of the sinuses,particularly bilateral frontal sinuses were clear (Fig. 3).No neurological complications were seen. The child wasmanaged with intravenous antibiotics and endoscopicsphenoidotomy. Intraoperatively, hypertrophied inflamedpolypoidal mucosa was seen involving the lateral recessesof sphenoid sinuses which were excised and curetted. Onhistopathological examination of the excised tissue, thelamina propria and epithelial layer showed extensive edemawith infiltration of neutrophils and mononuclear cells, throm-bophlebitis and necrotic foci suggestive of acute inflammatorypathology. Follow-up after one month showed near completeresolution with minimal soft tissue in right lateral recess(Fig. 4).
Imaging finding of an isolated acute sinusitis of lateralrecess of sphenoid sinus in a child is very uncommon andhas not been described in the literature. The diagnosis is oftendelayed until there is a neurological complication. An impor-tant differential diagnoses with similar imaging findingsthat should be kept in mind while treating these cases ismeningocele/meningoencephalocele of the lateral recesses,
due to persistence of Sternberg’s canal. These patientsusually present with spontaneous cerebrospinal fluidleaks and clinical meningitis. The anatomical locationof Sternberg’s canal is medial to the superior orbital fissure
Fig. 1 a Axial and b Coronal non-contrast CT scan of paranasal sinusesshowing fluid within bilateral lateral recesses (arrow) of the sphenoidsinus (arrowhead) and clear bilateral ethmoid sinuses (asterisk)
Fig. 2 Coronal MRI image confirming the findings showing fluid signalintensity in bilateral lateral recesses of sphenoid sinus
B. Sureka (*) :M. K. Mittal :B. B. ThukralDepartment of Radiodiagnosis, Vardhman Mahavir MedicalCollege & Safdarjung Hospital, New Delhi 110029, Indiae-mail: [email protected]
A. MittalDepartment of Pediatrics, Vardhman Mahavir MedicalCollege & Safdarjung Hospital, New Delhi, India
Indian J PediatrDOI 10.1007/s12098-013-1237-y

and foramen rotundum opening in the region towards cavernoussinus [1].
Pediatricians and pediatric otolaryngologists should be awareof pathologies and anatomic variations in relation to sphenoidsinus. These include pneumatisation of anterior clinoid process,
foramen rotundum, vidian canal, pterygoid process, or themaxilloethmoid process and recesses like sphenoethmoidal re-cess, lateral recess and maxillary recesses of the sphenoid sinus[2]. Diseases of the sphenoid sinus, sella turcica and para-sellaregions pose great challenges because approach to these struc-tures is technically difficult. Endoscopic transpterygoid andtranspterygopalatine fossa approach is recommended for dis-eases of lateral recess, transnasal approach for sphenoid sinusesand trans-sphenoidal approach for pituitary surgeries. A goodknowledge of the pattern of pneumatisation of the sphenoidalsinus and a careful characterization of its relationship to vitallocal and regional neurovascular structures is essential forsurgeons to provide guidance during surgery [3].
Through this case we would like to highlight the diagnosticdilemma associated with isolated sphenoid sinusitis. Pediatricotolaryngologists should be aware of this unusual entity as itpresentswith elusive physical findings. Nasendoscopy combinedwith CT/MRI of sinuses allows for timely diagnosis. MRI isespecially useful in pediatric population as it is radiation free andexcludes meningocele, the closest differential.
Conflict of Interest None.
Role of Funding Source None.
References
1. Khattar VS, Hathiram BT, Sharma H. Sternberg’s canal and the con-troversies surrounding it. Otorhinolaryngol Clin. 2011;3:184–7.
2. Sirikci A, Bayazit YA, BayramM, Mumbuc S, Gungor K, KanlikamaM. Variations of sphenoid and related structures. Eur Radiol. 2000;10:844–8.
3. Aydin S, Cavallo LM, Messina A, Dal Fabbro M, Cappabianca P,Barlas O, et al. The endoscopic endonasal trans-sphenoidal approachto the sellar and suprasellar area: Anatomic study. J Neurosurg Sci.2007;51:129–38.
Fig. 4 Follow-up Axial CT scan image showing minimal soft tissue inright lateral recess (arrowhead) and clear left lateral recess of sphenoidsinus (arrow)
Fig. 3 a Axial CT and b Axial MRI image showing normal frontalsinuses (arrow)
Indian J Pediatr



























![Surgical management of clinoidal meningiomas: 10 cases ... · sphenoid wing or inner sphenoid wing meningiomas[1,2]. However, accumulating anatomical knowledge and clinical experience](https://img.pdfslide.net/doc/110x75/5eca8277e895a04bfa1c336b/surgical-management-of-clinoidal-meningiomas-10-cases-sphenoid-wing-or-inner.jpg)