Embed Size (px)
Citation preview

Vol. 29, No. 12JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1991, p. 2741-27450095-1137/91/122741-05$02.00/0Copyright C 1991, American Society for Microbiology
Isolation and Characterization of an Ehrlichia sp. from a PatientDiagnosed with Human Ehrlichiosis
JACQUELINE E. DAWSON,'* BURT E. ANDERSON,1 DANIEL B. FISHBEIN,1 JOSE L. SANCHEZ,2CYNTHIA S. GOLDSMITH,3 KENNETH H. WILSON,4' 5 AND C. WAYNE DUNTLEY6
Viral and Rickettsial Zoonoses Branchl and Ultrastructure Activity, Office of the Director, Division of Viral andRickettsial Diseases, Center for Infectious Diseases, Centers for Disease Control, Atlanta, Georgia 30333; Department of
Field Studies, Division of Preventive Medicine, Walter Reed Army Institute ofResearch, Washington, D.C. 203072;Department of Medicine, Duke University,4 and Infectious Disease Section, Veterans Affairs Medical Center,5Durham, North Carolina 27705; and Preventive Medicine Service, U.S. Army Medical Department Activity,
Ft. Sill, Oklahoma 735036
Received 14 May 1991/Accepted 20 September 1991
A new disease was recognized in the United States in 1986. The etiologic agent, although not previouslyisolated from a human, appeared to be serologically related to Ehrlichia canis, a canine leukotropic rickettsia.We obtained blood specimens from 27 febrile patients with a history of tick exposure. Leukocytes from 24patients not treated with tetracycline were placed onto a monolayer of DH82 cells. We performed indirectimmunofluorescence on sera from all 27 febrile patients as well as sera from 12 patients with previouslydiagnosed ehrlichiosis. Intracytoplasmic inclusions were first observed in culture 35 days after the addition ofinfected blood from one patient. Partial sequencing of the rRNAs from the human isolate and E. canis indicatedthat they are 98.7% related. Positive indirect immunofluorescence reactions to the human isolate were obtainedfor all 12 previously diagnosed patients and for 33% of the 27 febrile patients. Two patients were seropositivefor the human isolate but not for E. canis. No sera were positive for E. canis and negative for the human isolate.We report the isolation of a previously unrecognized Ehrlichia sp. that appears to be the etiologic agent ofhuman ehrlichiosis. Serologic data (range of antibody titers, 256 to 32,768) in combination with rRNAsequencing indicated that the newly isolated Ehrlichia sp. is similar, but not identical, to E. canis.
Human ehrlichiosis is a newly recognized disease gener-ally characterized by fever, headache, malaise, thrombocy-topenia, leukopenia, and elevated liver enzymes (2, 3, 6,8-11, 13, 14). Most patients also have a history of tickexposure (16). Serologic testing of sera from these patients,together with morphologic examination of inclusions in theleukocytes of some patients, has suggested that the etiologicagent is Ehrlichia canis or a closely related species. Sincethe recognition of human ehrlichiosis in the United States in1986, laboratory-based surveillance has identified 215 per-sons with a fourfold increase or decrease in antibody titers toE. canis in 20 states, predominantly in southeastern andsouth central areas of the United States (7, 9, 11, 15).However, because the causative agent of human ehrlichiosispreviously has not been isolated from a human, the etiologyof this disease has remained uncertain. For this reason, wedirected our efforts toward the isolation of the etiologic agentof human ehrlichiosis from blood specimens of febrile pa-tients with a recent history of tick exposure, and we reporthere the isolation and characterization of the apparentpathogenic agent from a patient with ehrlichiosis.
(This work was presented in part at the 91st GeneralMeeting of the American Society for Microbiology, 5 to 9May 1991, Dallas, Tex.)
CASE REPORTA 21-year-old male army reservist was evaluated in a
medical clinic in Ft. Chaffee, Ark., on 19 July 1990 for fever(39.4°C), headache, pharyngitis, nausea, vomiting, and de-hydration 3 days after the onset of illness. No cough or
* Corresponding author.
myalgia was reported. A physical exam revealed prominentcervical lymphadenopathy, splenomegaly, and no rash. Dur-ing field exercises he sustained multiple excoriated lesionsfrom constant (11 days) exposure to ticks, chiggers, andmosquitoes. None of the ticks, chiggers, or mosquitoes weresaved or identified. Four days after the onset of illness, the
3hematocrit was 40.1%, the leukocyte count was 2,200/mm3,and the platelet count was 100,000/mm3. The differentialrevealed a significant left shift, with 45% banded neutrophils,32% segmented neutrophils, 10% lymphocytes, 10% mono-cytes, and 2% basophils. Serum samples were obtained 3,39, and 117 days after the onset of disease. The patientdefervesced within 24 to 48 h after the initiation of tetracy-cline treatment (500 mg orally 4 times per day), which wasbegun 4 days after the onset of illness. Ehrlichia morulaewere not observed in thin peripheral blood smears.
MATERIALS AND METHODS
Collection and preparation of specinmens. A small volume ofblood (30 ml drawn with heparin and 5 ml drawn with EDTA)was obtained from each of 27 febrile patients who had ahistory of tick bites and a temperature of .38.30C and wasshipped on cold packs to the Centers for Disease Control.Patients were selected from army personnel reporting to amedical clinic in Ft. Chaffee, Ark., and from the privatesector on the basis of the additional history of thrombocy-topenia, leukopenia, or elevated liver enzymes. The leuko-cytes were separated from the erythrocytes (15 ml of hep-arinized whole blood) by 1:1 dilution of thç heparinizedwhole blood in 0.01 M phosphate-buffered saline and layer-ing on top of an equal volume of lymphocyte separationmedium (Organon Teknika-Cappel, Durham, N.C.). The
2741
on January 31, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

2742 DAWSON ET AL.
preparation was centrifuged at 400 x g for 30 min. Theleukocytes from 24 of the 27 patients (3 patients who hadreceived tetracycline therapy were excluded) were proc-essed by this technique.
In vitro cultivation. Samples were processed by the lym-phocyte separation technique approximately 24 h after col-lection. The leukocyte pellet was resuspended in 4 ml ofculture medium (minimum essential medium [GIBCO Labo-ratories, Grand Island, N.Y.] supplemented with 1% L-glu-tamine [200 mM] and 12.5% heat-inactivated fetal bovineserum), and the suspension was layered onto a previouslyestablished 25-cm2 monolayer of DH82 (continuous caninemacrophage) cells (5). The cultures were maintained at 37°Cwithout supplemental CO2. Twice weekly the supernatantwas removed and 5 ml offresh medium was added. Since themonolayer would remain intact under these conditions, blindsubpassages were not necessary. Each culture was moni-tored by direct immunofluorescence for a minimum of 5weeks with a 1:50 dilution of a fluorescein conjugate pre-
pared from the serum of a patient with a fourfold change inantibody titer to E. canis (12). The direct conjugate can alsospecifically fluoresce E. canis morulae.Acute- and convalescent-phase sera (separated by at least
10 days) were obtained from the 27 febrile patients describedabove. Anonymous control sera were obtained from twoadults at the Centers for Disease Control Blood Bank,Atlanta, Ga. The control sera showed no fluorescence in theindirect fluorescent-antibody (IFA) test.
Serologic testing. Acute- and convalescent-phase sera from12 patients (randomly selected, from a total of 11 differentstates; see Table 1) previously shown to have a fourfoldincrease or decrease in antibody titers to E. canis were
retested by the IFA test. Cells from E. canis- and humanEhrlichia-infected DH82 cultures (80 to 90% infection) were
suspended in culture supernatant as previously described(5). In brief, 1 drop (3 pi) of each antigen was placed in eachwell of a 12-well Teflon-coated slide. The slides were airdried for 1 h, stored in a slide box, and placed at -90°C. Theslides were thawed and fixed in acetone for 15 min as
needed.The IFA test was performed as previously described (9).
In brief, the serum samples were screened at a dilution of1:64 in 0.15 M phosphate-buffered saline. When distinctstaining of the ehrlichial organisms was observed at thisdilution (4), serial twofold dilutions were made. Serologicresults were reported as the reciprocal of the highest dilutionat which specific fluorescence of Ehrlichia morulae or indi-vidual organisms was observed.
All of the serum samples from the 27 febrile patients were
tested for antibodies to E. canis and the human isolate.Electron microscopy. Cell cultures were scraped from
flasks, washed in phosphate buffer, and centrifuged at 180 x
g for 10 min. The resulting pellets were fixed at 4°C in 2.5%0.2 M phosphate-buffered glutaraldehyde, postfixed in 1%buffered osmium tetroxide, dehydrated in a standard ethanolseries, and embedded in an Epon substitute-araldite mixture.Sections were stained with uranyl acetate and lead citrateand examined with a Philips EM410-LS electron microscopeat 60 kV.PCR and rRNA sequencing. DNA was extracted from the
original whole-blood (drawn with EDTA) sample as previ-ously described (18) and used as a polymerase chain reaction(PCR) template to produce amplified DNA for cloning andsequencing. DNA was also extracted from the DH82 cell lineinfected with the human isolate, DH82 infected with E. canis
(Oklahoma isolate) (5), and uninfected DH82 for similar
amplification and sequence comparisons. Samples were am-plified for three cycles at 94°C for 1 min, 48°C for 2 min, and66°C for 1.5 min and for 37 cycles at 88°C for 1 min, 52°C for2 min, and 68°C for 1.5 min in a thermal cycler withdegenerate ("universal") primers specific for the 3' half ofeubacterial 16S rRNA, roughly corresponding to Esche-richia coli 16S rRNA nucleotides 787 to 1507 (20). Theseprimers were modified to contain an XbaI site on the 5' endof the PCR product (in primer p3mod), 5' AATCTAGATTAGATACCCTDGTAGTCC 3', where D = A, T, or G, anda BamHI site on the 3' end (in primer pc5), 5' AAGGATCCTACCTTGTTACGACTT 3'. Meticulous procedures forsample handling and reagent preparation were used to avoidcontamination of specimens before and during the assemblyof the PCRs. Such contamination is problematic when uni-versal primers are used for PCR, as observed in our labora-tory and others (20). PCR products were examined by 1%agarose gel electrophoresis and stained with ethidium bro-mide. PCR products were subsequently cloned into pUC19and sequenced. All samples were amplified, cloned, andsequenced independently two or more times to prevent thereading of Taq polymerase incorporation errors. The rRNAsequences for E. sennetsu, E. equi, and E. phagocytophilawill be published elsewhere (1).
RESULTS
Isolation of an Ehrlichia sp. Intracytoplasmic morulaecontaining coccoid bacteria were first observed in the cyto-plasm of cultured macrophages 35 days after the addition ofinfected blood drawn from one patient 3 days after the onsetof illness. The morulae closely resembled those seen in E.canis-infected cells. The proportion of infected macrophagesincreased, reaching a maximum of 80% on day 48. Cultureswere subcultured when 50 to 60% of the cells were infected.Cultures with 30 to 50% infected cells could be frozen withdimethyl sulfoxide and thawed as necessary. Organismswere not observed in any of the other 23 cultured bloodsamples. Uninoculated control cultures of DH82 cells re-mained free of organisms.
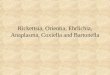
Electron microscopy. Electron microscopic examination ofthe infected cells revealed that inclusion bodies were sur-rounded by a distinct cytoplasmic membrane (Fig. 1A).Single microorganisms wrapped in vacuolar membrane werealso present in the cytoplasm (Fig. 1A, arrowheads). Eachorganism appeared to be bound by an inner plasma mem-brane and an outer cell wall (Fig. 1B). The organisms wereextremely pleomorphic, ranging in shape from oval to boo-merang to diamond.
Serologic analysis. Serum samples were obtained from theindex patient during the acute (3 days), early convalescent(39 days), and late convalescent (117 days) phases of thedisease. Both the acute- and early-convalescent-phase serawere negative for antibodies to Rickettsia rickettsia, R. typhi,Coxiella burnetii, and E. canis. The early-convalescent-phase sample was positive only for antibodies to the humanEhrlichia agent isolated from the index patient at a titer of256. The late-convalescent-phase sample was positive onlyfor antibodies to the human Ehrlichia agent and E. canis at atiter of 256.
All 12 patients for whom ehrlichiosis was previouslydiagnosed only by the E. canis IFA test were also seropos-itive for the human isolate (Table 1). Results for both the E.canis and human Ehrlichia antigens were identical or withina twofold dilution, except for one patient (number 12, Table1) who had a fourfold-higher antibody titer with the human
J. CLIN. MICROBIOL.
on January 31, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

EHRLICHIA SP. ISOLATION AND CHARACTERIZATION 2743
,tt
4es
`.rv.
* 4A
\ fi \4~._k .:
B1.F.F.
'Q.,
FIG. 1. Transmission electron micrograph of the human Ehrlichia isolate in the cytoplasm of a DH82 cell. (A) Organisms (arrows) are seenin two membrane-bound morulae as well as individually in the cytoplasm (arrowheads). Bar = 1 ,um. (B) Higher magnification of the box inpanel A. Organisms are bound by an inner plasma membrane (arrowhead) and an outer cell wall (arrow). Bar = 200 nm.
Ehrlichia antigen. Negative control sera showed no reactionwith either organism.Nine (33.3%) of the 27 patients with a history of recent tick
bites and a fever (.38.30C) had a fourfold or greater changein antibody titer to the human Ehrlichia agent. Only seven ofthese patients had antibody titers to E. canis and the humanEhrlichia agent; two patients had antibody titers only to thelatter. Both of these patients had peak titers of 1,024. Thereverse situation was not found. No sera were positive for E.canis and negative for the human isolate.Three of the nine patients with serologically confirmed
ehrlichiosis (including the index patient) had a history of tickbites at Ft. Chaffee, Ark. Isolation of an Ehrlichia sp. was,however, only successful from the index patient.PCR and rRNA sequencing. Upon electrophoresis through
a 1.0% agarose gel, PCR products measuring 733 bp in size(Fig. 2) and corresponding to the 3' half of the 16S rRNAwere observed with UV light in the original whole-blood(drawn with EDTA) sample (lane B), the human Ehrlichiaisolate (lane C), and E. canis (Oklahoma isolate) (lane D).
PCR products were not seen when DNA derived fromuninfected DH82 cells was used as a template (lane E) orwhen no DNA template was added (lane F). Lane A con-tained molecular size standards («X174 phage DNA cleavedwith HaeIII). An additional band that was seen at approxi-mately 320 bp in the infected-blood sample (lane B) was alsoseen in normal human blood (data not shown); it was found,upon sequencing, to be unrelated to eubacterial 16S rRNAand was apparently a result of nonspecific PCR amplifica-tion. Upon sequencing of the cloned 16S rRNA-derived PCRproducts from the human isolate, the patient's blood sample,and E. canis, only E. canis yielded a sequence that differedat 1 nucleotide in two independent determinations. A thirdsequence for the cloned E. canis PCR product agreed at thisnucleotide with one of the previously determined sequences;therefore, the two matching sequences were assumed to becorrect. The PCR product from the patient's blood samplematched the PCR product from the human isolate (obtainedfrom DH82 cells) for all 683 nucleotides defined within thePCR primers. Sequencing of the PCR products from the
VOL. 29, 1991
_l
,.- 1%
on January 31, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

2744 DAWSON ET AL.
TABLE 1. IFA titers of acute- and convalescent-phase sera from12 patients and tested with E. canis and the
human Ehrlichia isolate
Patient ~Tick Days IFA titera to:Patientexposure after E. Human Ehrlichia
canis isolate
1 Georgia il <64 <6451 128 256
2 Oklahoma 26 <64 <6440 512 256
3 New Jersey 7 1,024 1,02425 512 512135 256 256
4 North Carolina 8 <64 <6417 4,096 2,048
5 Wyoming 10 64 3224 512 512
6 Texas 16 4,096 4,09628 1,028 1,028
7 Missouri 13 <64 <6424 512 1,028
8 Arkansas 10 512 51224 16,384 32,768
9 Tennessee 19b <64 <6455 256 256
10 Virginia 18 32,768 32,76838 8,192 8,192
il Florida 10 1,024 2,04828 8,192 16,384
12 Oklahoma 8 <64 <6421 4,096 16,384
Reciprocal of the highest dilution of serum that showed positive fluores-cence.
b This specimen was obtained 19 days before the onset of disease.
human isolate and E. canis indicated that they were 98.7%related. Comparison with available sequence data also re-vealed that the human isolate was 86.8% related to E. risticii(GenBank accession number M21290), a recently isolatedequine pathogen. This evidence supports the previouslypublished serologic data, which revealed that sera from anehrlichiosis patient reacted much more strongly with E.canis than with E. risticii, E. equi, or E. sennetsu (13).
DISCUSSION
Several lines of evidence suggest that the Ehrlichia sp.isolated from this patient is unique and is probably theetiologic agent of human ehrlichiosis. First, serologic datashowed that all patients with a previous diagnosis of humanehrlichiosis confirmed by the E. canis IFA test were alsopositive when the human isolate was used as the antigen.Second, we detected two patients who were seronegative forE. canis but seropositive for the human isolate. Antibodiesto E. canis were not detectable in the serum from the indexpatient until 117 days after the onset of illness. Therefore,
-733 bp
ABC DF FFIG. 2. Ethidium bromide-stained agarose gel (1.0%) of the PCR
products obtained from amplification of ehrlichial templates withuniversal primers. The 733-bp band corresponding to the 16S rRNAPCR product is indicated on the right. Lane A contains molecularsize standards (4+ X174 phage DNA cleaved with HaeIII), from topto bottom, of 1,353, 1,078, 872, 603, 310, 281 or 271, 234, and 194 bp.Lanes B to F contain PCR products obtained after 40 cycles ofamplification with the following sources of templates: B, infectedhuman blood; C, human ehrlichiosis isolate cultivated in DH82 cells;D, E. canis cultivated in DH82 cells; E, uninfected DH82 cells; F,no template (negative control).
had late-convalescent-phase serum samples been drawnfrom the two E. canis-seronegative patients, perhaps E.canis antibodies would have been detected. When reviewed,the clinical features of these two patients were found to becompatible with the diagnosis of human ehrlichiosis andincluded fever, headache, malaise, myalgias or arthralgias,leukopenia, thrombocytopenia, and elevated liver enzymes.Finally, the 16S rRNA sequencing data, obtained for boththe human isolate and the whole blood (drawn with EDTA)from the index patient revealed that the newly isolatedEhrlichia sp. is similar, but not identical, to E. canis (98.7%sequence homology).Our finding that 9 (33%) of 27 patients with a history of
recent tick bites and a fever (.38.30C) had a fourfold orgreater change in antibody titer to the human isolate is higherthan any previously published figure. Because there was aselection bias for some of these patients, the proportionreported here may be inflated. Nonetheless, our findingsstrongly suggest that the diagnosis of human ehrlichiosisshould be entertained on a routine basis for patients withthese signs and symptoms. The use of the human isolate asan antigen in future serologic testing may demonstrate thatthe incidence of human ehrlichiosis is greater than previ-ously reported, as suggested by the identification of threecases in the Ft. Chaffee area during the course of this study.
Ehrlichia spp. are obligate intracellular bacteria whichrequire very specific growing conditions. A number oflaboratories, including ours, have been trying for severalyears to isolate the causative agent of human ehrlichiosis.One of the major obstacles to growing some members of thisgenus, including E. canis, has been the lack of a suitable
J. CLIN. MICROBIOL.
on January 31, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from

EHRLICHIA SP. ISOLATION AND CHARACTERIZATION 2745
continuous cell line. Historically, E. canis could only begrown in primary canine monocytes, which required aconstant source of whole blood because the cells could onlysurvive for about 2 weeks in cultures. We also tried unsuc-cessfully on numerous occasions (including blood from theindex patient) to isolate the etiologic agent of human ehrli-chiosis in human monocytes. In 1990 alone we attempted toisolate the etiologic agent from 37 people (24 of the patientswere included in this study; convalescent-phase sera fromthe others were not available). We were only successful withan isolate cultivated in continuous canine cell line DH82.The use of PCR amplification of the 16S rRNA gene,
coupled with DNA sequencing, to identify the putativeetiologic agent of human ehrlichiosis is an especially valu-able technique for the study of fastidious or noncultivatablemicroorganisms. This technique is useful for studying therickettsiae or rickettsialike organisms, as demonstrated bythe successful application to the characterization of theetiologic agent of bacillary epithelioid angiomatosis (17) andAnaplasma marginale, a member of the Rickettsiales that ispathogenic for several ruminant species (19). Further studieswith this technique are under way to determine the exactrelationship of the new human ehrlichiosis isolate to othermembers of the genus Ehrlichia.
ACKNOWLEDGMENTS
We thank T. Tzianabos for preparing the PCR samples andBrenda Paxton for collecting the blood samples. We especiallythank D. Everett and F. Satalowich for the submission of samplesfrom patients with the suspected disease. We also thank J. McDadeand S. A. Ewing for reviewing the manuscript, S. A. Ewing forscientific consultation, and Cornelia Greene for performing rickett-sial serology testing.
Contributions from the Department of Medicine, Duke Univer-sity, and the Infectious Disease Section, Veterans Affairs MedicalCenter, were supported by the Department of Veterans Affairs andthe North Carolina Biotechnology Center.
REFERENCES1. Anderson, B. E., J. E. Dawson, D. C. Jones, and K. H. Wilson.
1991. Ehrlichia chaffeensis, a new species associated withhuman ehrlichiosis. J. Clin. Microbiol. 29:2838-2842.
2. Barton, L. L., J. E. Dawson, G. W. Letson, A. Luisiri, and A. J.Scalzo. 1990. Simultaneous ehrlichiosis and Lyme disease. Pe-diatr. Infect. Dis. J. 9:127-129.
3. Centers for Disease Control. 1988. Human ehrlichiosis-UnitedStates. Morbid. Mortal. Weekly Rep. 37:270, 275-277.
4. Dawson, J. E., D. B. Fishbein, T. R. Eng, M. A. Redus, andN. R. Greene. 1990. Diagnosis of human ehrlichiosis with theindirect fluorescent antibody test: kinetics and specificity. J.Infect. Dis. 162:91-95.
5. Dawson, J. E., Y. Rikihisa, S. A. Ewing, and D. B. Fishbein.1991. Serologic diagnosis of human ehrlichiosis using two Ehr-lichia canis isolates. J. Infect. Dis. 163:91-95.
6. Dimmitt, D. C., D. B. Fishbein, and J. E. Dawson. 1989. Humanehrlichiosis associated with cerebrospinal fluid pleocytosis: acase report. Am. J. Med. 87:677-678.
7. Eng, T. R., and R. Giles. 1989. Ehrlichiosis. J. Am. Vet. Med.Assoc. 194:497-500.
8. Eng, T. R., J. R. Harkess, D. B. Fishbein, J. E. Dawson, C. N.Greene, M. A. Redus, and F. T. Satalowich. 1990. Epidemio-logic, clinical, and laboratory findings of human ehrlichiosis inthe United States, 1988. J. Am. Med. Assoc. 264:2251-2258.
9. Fishbein, D. B., A. Kemp, J. E. Dawson, N. R. Greene, M. A.Redus, and D. H. Fields. 1989. Human ehrlichiosis: prospectiveactive surveillance in febrile hospitalized patients. J. Infect. Dis.160:803-809.
10. Fishbein, D. B., L. A. Sawyer, C. J. Holland, E. B. Hayes, W.Okoroanyanwu, D. Williams, K. Sikes, M. Ristic, and J. E.McDade. 1987. Unexplained febrile illnesses after exposure toticks. Infection with an Ehrlichia? J. Am. Med. Assoc. 257:3100-3104.
11. Harkess, J. R., S. A. Ewing, J. M. Crutcher, J. Kudlac, G.Mckee, and G. R. Istre. 1989. Human ehrlichiosis in Oklahoma.J. Infect. Dis. 159:576-579.
12. Hebert, G. A., B. Pittman, R. M. Mckinney, and W. B. Cherry.1972. The preparation and physiochemical characterization offluorescent antibody reagents. Center for Disease Control,Atlanta.
13. Maeda, K., N. Markowitz, R. C. Hawley, M. Ristic, D. Cox, andJ. E. McDade. 1987. Human infection with Ehrlichia canis, aleukocytic rickettsia. N. Engl. J. Med. 316:853-856.
14. Manian, F. A., J. Weidner, J. Costello, D. B. Fishbein, and J. E.Dawson. 1989. Human ehrlichiosis. Mo. Med. 86:691-695.
15. McDade, J. E. 1990. Ehrlichiosis-a disease of animals andhumans. J. Infect. Dis. 161:609-617.
16. Petersen, L. R., L. A. Sawyer, D. B. Gishbein, P. W. Kelley,R. J. Thomas, L. A. Magnarelli, M. Redus, and J. E. Dawson.1989. An outbreak of ehrlichiosis in members of an army reserveunit exposed to ticks. J. Infect. Dis. 159:562-568.
17. Relman, D. A., J. S. Loutit, T. M. Schmidt, S. Falkow, and L. S.Tompkins. 1990. The agent of bacillary angiomatosis. An ap-proach to the identification of uncultured pathogens. N. Engl. J.Med. 323:1573-1580.
18. Tzianabos, T., B. E. Anderson, and J. E. McDade. 1989.Detection of Rickettsia rickettsii DNA in clinical specimens byusing polymerase chain reaction technology. J. Clin. Microbiol.27:2866-2868.
19. Weisburg, W. G., S. M. Barns, D. A. Pelletier, and D. J. Lane.16S ribosomal DNA amplification for phylogenetic study. J.Bacteriol. 173:697-703.
20. Wilson, K. H., R. B. Blitchington, and R. C. Greene. 1990.Amplification of bacterial 16S ribosomal DNA with polymerasechain reaction. J. Clin. Microbiol. 28:1942-1946. (Erratum,29:666, 1991.)
VOL. 29, 1991
on January 31, 2020 by guesthttp://jcm
.asm.org/
Dow
nloaded from