Embed Size (px)
Citation preview
1
Issue 10 • October 1997 unicef WATERfrontWATERfrontI SSUE ␣ 10 ␣ • ␣ OCTOBER ␣ 1997
Table of Contents
4 UNICEF & UNEP SignAgreement
5 The Phungalutho: A “Peri-Urban” Sanitation Solution
6 One Hundred and FiftyWells in the South ofMadagascar
8 Household Hygiene inSanto Antao, Cape Verde
11 Water Points Committeesfor CommunityDevelopment
12 Sarasa
13 Sanitation: UNICEFExperience in Cambodia
14 Low Cost LatrineTechnology Options
16 Sanitation Promotionthrough Community BasedOrganizations
18 Health Impact of WaterSupply Interventions
20 Women Benefits fromSanitation in Vietnam
22 The Mangochi HTNWorkshop
23 Nicaragua
25 Costing of Water andSanitation Investment
26 Reducing Pests and InsectVectors
28 UNICEF and World BankJoin Forces
28 Cost Calculation
A PUBLICATION OF THE WATER, ENVIRONMENT AND SANITATION SECTION, PROGRAMME DIVISION • UNICEF
unicefUnited Nations Children’s FundFonds des Nations Unies pour l’enfanceFondo de las Naciones Unidas para la
Infancia
UNICEF-UNEP SignedMemorandum ofUnderstanding on
Environment (see page 4)
UNICEF-WHO Joint Water Supplyand Environmental Sanitation Strategy
Universal Access to Safe Drinking Water andSanitation: Basic Elements of Health for Alland the Convention on the Rights of the Child
Introduction and Backgroundince the Alma-Ata Declaration in1978, further reinforced at the WorldSummit for Children in 1990 and
through ratification of the Convention on theRight of the Child, numerous internationalfora have called for universal access to safewater and sanitation. Despite the gains madetoward universal access, WHO and UNICEFrecognize the need for new approaches andstrong advocacy for the sector and its linkagewith health, nutrition, education, safe envi-ronment and above all sustainable develop-ment. A collaborative framework ofunderstanding and complementary actionneeds to be developed by both Organizationsat global as well as at regional and countrylevels. The establishment of a joint strategyfor WHO and UNICEF is the first step in de-veloping this framework.
Strategies for EffectiveCollaborationBased on the above mandates, this joint strat-egy has been developed to operationalize the continued on page 2
common elements of strategies of both Organi-zations. The UNICEF “Strategies in Water andEnvironmental Sanitation” approved in May1995 and the “Environment and Sustainable De-velopment - UNICEF’s Response to Agenda 21"in 1993, along with WHO Global Strategy forHealth and Environment adopted by the WorldHealth Assembly in 1993 will form the basis forthis cooperation and collaboration between thetwo Organizations. Through this statement,WHO and UNICEF reiterate their intention andstrategy to collaborate with their individual re-sources and knowledge base to support capacitybuilding at country level towards sustainable na-tional programmes aimed at accelerating actiontowards the ultimate goal of universal access tosafe water and sanitation.
There are certain features of this “Joint Strat-egy” which makes it unique and renders it animportant tool in support of the development ofnational water supply and sanitationprogrammes. First, it is the first time that thetwo lead UN bodies in the field of water supply
S
UNICEF and World Bank JoinForces for Safe Water andEnvironment Sanitation in
Africa (see page 28)

2
Issue 10 • October 1997unicef WATERfront
continued on next page
■ UNICEF-WHO Joint Water Supply Strategy, from page 1
and sanitation have approached thegoals with a common sector strategy.This in itself should strengthen the posi-tion of the partners, and form a basis forthe other external support agencies, bothmultilateral and bilateral, to harmonizetheir approaches and encourage stake-holders to be part of this partnership.
Second, the emphasis on action atcountry level in support of nationalplans of action developed within theframework of the Child Summit Goals,is also unique. Collaboration exists be-tween the bodies of the UN system atthe global policy level, particularlythrough the ACC and the InteragencySteering Committee for Water Supplyand Sanitation, however, continued ef-forts are necessary to encourage practi-cal co-operation in support of individualcountry programmes.
Third, the Strategy also recognizesthe need to take a multi-faceted andmulti-disciplinary approach to water sup-ply and sanitation development. This willbe done using country and area specificstrategies for behavioural change; healthand hygiene education; community man-agement of water and environment insupport of sustainable development. Itwill be supported by a balanced mix oftechnology and with the emphasis onhealth and socio-economic benefits.
Finally, the Strategy forms an inte-gral part of the “Health for All” ap-proach and the Convention on theRights of the Child, both of which aimat specific, yet complementary, objec-tives for the later half of this decade andinto the 21st century. Within the frame-work of these global policy mandates,this Strategy is intended to reinforce theconcept that access to safe drinking wa-ter and proper sanitation is a basic hu-man right. Regional and countryspecific strategies and action plans willbe evolved depending on the situationanalysis and opportunities as providedin the respective regional/country plansof the two organizations.
Goals of the StrategyThis Strategy has three main goals:
■ delivering consistent messages con-cerning integrated approaches to wa-ter supply and sanitationdevelopment;
■ supporting the design andimplemention of sustainable watersupply and sanitation programmes atcountry level on the basis of a com-mon approach; and
■ maintaining a health and social em-
phasis within water supply and sanita-tion development at international fora,with other agencies, and with countryprogrammes and related sectors.
Main Strategy ElementsThe strategic actions necessary for theattainment of these three goals are asfollows:
1) Delivering consistent messages at alllevels of national authority concern-ing integrated approaches to watersupply and sanitation development.This will be done within the frame-work of WHO and UNICEF strate-gies and operational policies asapproved by their executive bodiesfrom time to time. These messagesshould cover all areas of sector activi-ties including health and hygiene edu-cation, operation and maintenance,women’s empowerment, applicationand promotion of technology, schoolcurricula and related activities. To thiseffect, UNICEF and WHO will:
■ strengthen the development of
common approaches globally andregionally through the routine ex-change of information, throughregular contacts and consultationin the planning process, particu-larly at country and local levelsand through a better understand-ing of the health social and eco-nomic benefits to be gained fromimproved water supply andsanitaton.
■ prioritize sanitation, hygiene andbehavioural change in theirprogrammes. Although an inte-grated approach to water supplyand sanitation development isideal, in many areas there is aneed to give priority to the imple-mentation of sanitaton and hy-giene programmes.
■ promote a strong element ofhousehold and community partici-pation with specific reference tothe role/empowerment of womenand gender-balanced approaches.
■ promote affordable, user-friendlytechnologies within the frame-work of programmes for watersupply and sanitation for the ruraland urban poor.
■ promote community-based man-agement of the environmentthrough primary environmentalcare at the household level.
■ work towards the development ofa country-level communicationsstrategy.
■ work together towards definingthe meaning and impact of variousfinancial tools commonly usedlike cost recovery, cost sharingetc. in the health and standard ofliving of poor and the unreached.
2) Supporting the design andimplemention of sustainable watersupply and sanitation programmes atcountry level on the basis of a com-mon approach. The basis for thiscommon approach will be NationalPlans of Action developed with sup-port from UNICEF within the con-
Despite the gains madetoward universal access,
WHO and UNICEF recognizethe need for new
approaches and strongadvocacy for the sector and
its linkage with health,nutrition, education, safe
environment and above allsustainable development.
3
Issue 10 • October 1997 unicef WATERfront
text of the Child Summit Goals andother national sector developmentplans. The approach will be one ofsupport to national programmes andthe attainment of their targets withparticular attention being paid topopulations at risk (women and chil-dren, marginalized urban popula-tions, rural poor, etc.) To this effect,UNICEF and WHO will:
■ provide a special focus of supportto national programmes in Africain the light of the United NationsSystem-wide Special Initiative onAfrica, the AFRICA 2000 initia-tive and National Programmes ofAction.
■ advise Regional Directors andCountry Representatives to de-velop on a systematic basis simi-lar regional/sub-regional and
country specific strategies to-wards the common goal.
■ promote collaborative approachesand joint activities at countrylevel in support of nationalprogrammes. Country level pro-gramming will be strengthenedthrough joint missions to supportgovernment planning exercisesand the development of countryprogrammes, including sector in-vestment projects specifically ad-dressing priority considerationssuch as water scarce areas, de-prived populations, vulnerablegroups and emergency activities.
■ develop country sector profiles ofwater supply and sanitation condi-tions through the Joint MonitoringProgramme at the community,district, provincial and nationallevels to enable programmes totarget activities where water-re-lated diseases and poor servicelevels are particularly acute.
■ promote environmental healththrough programmes such asHealthy Villages/Cities/Schoolsin rural and urban marginal com-munities, using, where appropri-ate, district health systems.
■ support community managementand the strengthening of local ca-
pacity to plan, operate and main-tain its systems.
■ support the strengthening of gov-ernment and NGO capacity at thelocal level.
■ advise and support standardiza-tion, local manufacturing andfield testing of equipment and/orcomponents, as appropriate, todetermine their feasibility.
■ foster the participation of appro-priate ministries in planning, en-vironmental impact assessment,and decision-making related towater resources management andprotection as they affect watersupply and sanitation.
■ support, where possible, eachother’s programmes at regionaland country levels through staffresources.
■ strengthen monitoring and infor-mation support capabilities of na-tional governments as tools forsector management with specialemphasis on the Joint MonitoringProgramme.
■ undertake joint action to enhanceresource mobilization in sector.
3) Maintaining a health and social em-
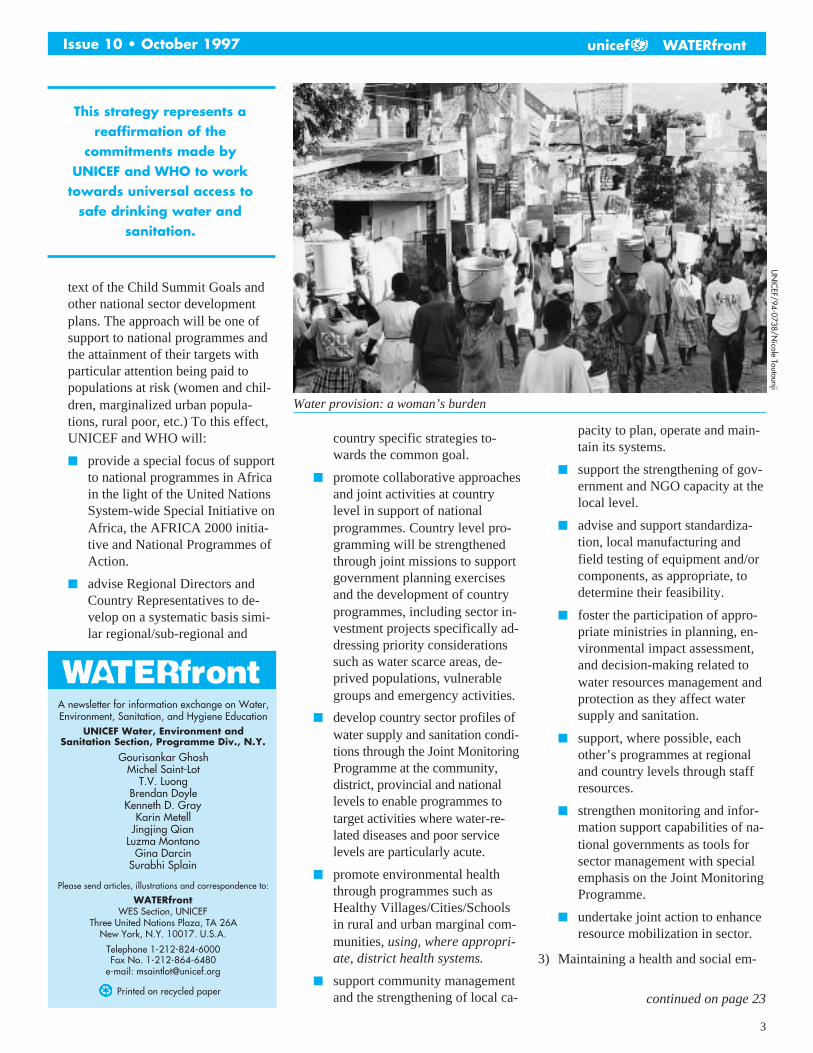
Water provision: a woman’s burden
continued on page 23
A newsletter for information exchange on Water,Environment, Sanitation, and Hygiene Education
UNICEF Water, Environment andSanitation Section, Programme Div., N.Y.
Gourisankar GhoshMichel Saint-Lot
T.V. LuongBrendan Doyle
Kenneth D. GrayKarin Metell
Jingjing QianLuzma Montano
Gina DarcinSurabhi Splain
Please send articles, illustrations and correspondence to:
WATERfrontWES Section, UNICEF
Three United Nations Plaza, TA 26ANew York, N.Y. 10017. U.S.A.
Telephone 1-212-824-6000Fax No. 1-212-864-6480
e-mail: [email protected]
Printed on recycled paper
WATERfront
UN
ICEF/94-0738/N
icole Toutounji
This strategy represents areaffirmation of the
commitments made byUNICEF and WHO to work
towards universal access tosafe drinking water and
sanitation.
4
Issue 10 • October 1997unicef WATERfront
continued on page 7
Purposes1. Protecting and managing environ-
mental resources, and ensuring that thebasic needs and rights of children aremet, constitute fundamental elements inthe concept of sustainable development.In recognition of the need to address theclose relationship and interaction be-tween the environmental factors and thesurvival, protection and development ofchildren, the United Nations Children’sFund (hereinafter called UNICEF) andthe United Nations EnvironmentProgramme (hereinafter called UNEP)agree to this Memorandum of Under-standing on Cooperation (hereinafter re-ferred to as “this Memorandum”).
2. This Memorandum provides theflexible framework for cooperation be-tween UNICEF and UNEP. It furtheroutlines several areas that will serve asthe basis for collaborative and mutuallycomplementary initiatives.
3. The cooperation under thisMemorandum will take place in areas ofcommon interests and within the scopeof the respective mandates of the twoorganizations.
4. UNICEF is mandated by theUnited Nations General Assembly to ad-vocate for the protection of children’srights, to help meet their basic needsand to expand their opportunities toreach their full potential within an over-all framework provided by the goals ofthe World Summit for Children and theConvention on the Rights of the Child.
5. Established in 1972 by the UnitedNations General Assembly followingthe United Nations Conference on theHuman Environment, UNEP is the prin-cipal environmental body within the UNsystem. UNEP is mandated by the Gen-
in UNICEF’s operations and, on theother hand, greater attention to child re-lated environmental concerns inUNEP’s programmes. One of the fieldsof cooperation will be the developmentof environmental impact assessmentpolicies and procedures provided byUNEP to support UNICEF’s develop-ment of environmental impact assess-ment guidelines appropriate to itsprogramme activities. In turn, the rel-evant field experiences gained byUNICEF could provide feed back toUNEP to inform its environmental im-pact assessment work.
10. UNEP and UNICEF willstrengthen their consultation, coordina-tion and collaboration in various UnitedNations inter-agency initiatives andmechanisms, including, but not limitedto, the United Nations System-wide Ini-tiative on Africa, the implementationmechanism for Habitat Agenda , the In-ter-Agency Committee on SustainableDevelopment, the Inter-Agency Envi-ronment Coordination Group, and therespective Inter-Agency Task Forces forfollowing up other major United Na-tions conferences and world summits.
Implementation11. Consultation between the two
parties may take place when and wherenecessary by mutual agreement in orderto promote the cooperation provided un-der this Memorandum. In this regard, therespective UNICEF regional and countryoffices and UNEP’s programme unitsand regional offices will be encouragedto maintain regular contact with eachother.
12. Subject to their respective poli-
UNEP and UNICEF Sign AgreementOn Strengthening CooperationNew York, March 5, 1997Memorandum of Understanding on Cooperation Between the UnitedNations Children’s Fund and the United Nations Environment Programme
eral Assembly to promote internationalcooperation and provide policy guidanceand coordination in the field of the envi-ronment. This mission is reaffirmed byAgenda 21, which further mandatesUNEP to take into account the develop-ment aspects of environmental questionsin its work.
Areas of Cooperation6. Areas of cooperation between
UNICEF and UNEP will fall under threebroad categories, namely a) advocacy inareas of common concern, b) scientific/technical cooperation on programme ac-tivities, and c) collaboration within thevarious United Nations system-wide ini-tiatives or inter-agency mechanisms.
7. The ultimate objective is to sup-port programme implementationthrough the best scientific and environ-mental information that bears on chil-dren and child health, especially at thefield level in developing countries.
8. Advocacy activities will be pur-sued in connection with child rights andraising environmental awareness, withinthe frameworks of the United NationsConvention on the Rights of the Childand Agenda 21 adopted at the UnitedNations Conference on Environmentand Development. In the near-term, fo-cus will be placed on working togetherto develop basic environmental and so-cial messages for the mobilization ofcommunity action, to publish an infor-mation series on pollutants and childhealth, and to promote environmentalcitizenship and environmental content inbasic education.
9. Scientific/technical cooperationwill be aimed at, on the one hand, inte-gration of environmental considerations
5
Issue 10 • October 1997 unicef WATERfront
continued on page 7
The Phungalutho: A “Peri-Urban” Sanitation Solution forKwazulu Natal, South AfricaBy Jane Devan, Consultant, UNICEF South Africa
nadi, a ‘peri-urban’ area ofPietermaritzburg, is undergoing aquiet revolution—a sanitation revo-
lution. Begun in January 1995, theSiyathuthuka Sanitation Committee hassince approved and built about 150Phungalutho toilets for its residents. Theproject, one of several started by theWater & Sanitation Technology Trans-fer Group of the Institute of Natural Re-sources just 18 months ago, has beenhanded over and is now completely runby the Committee.
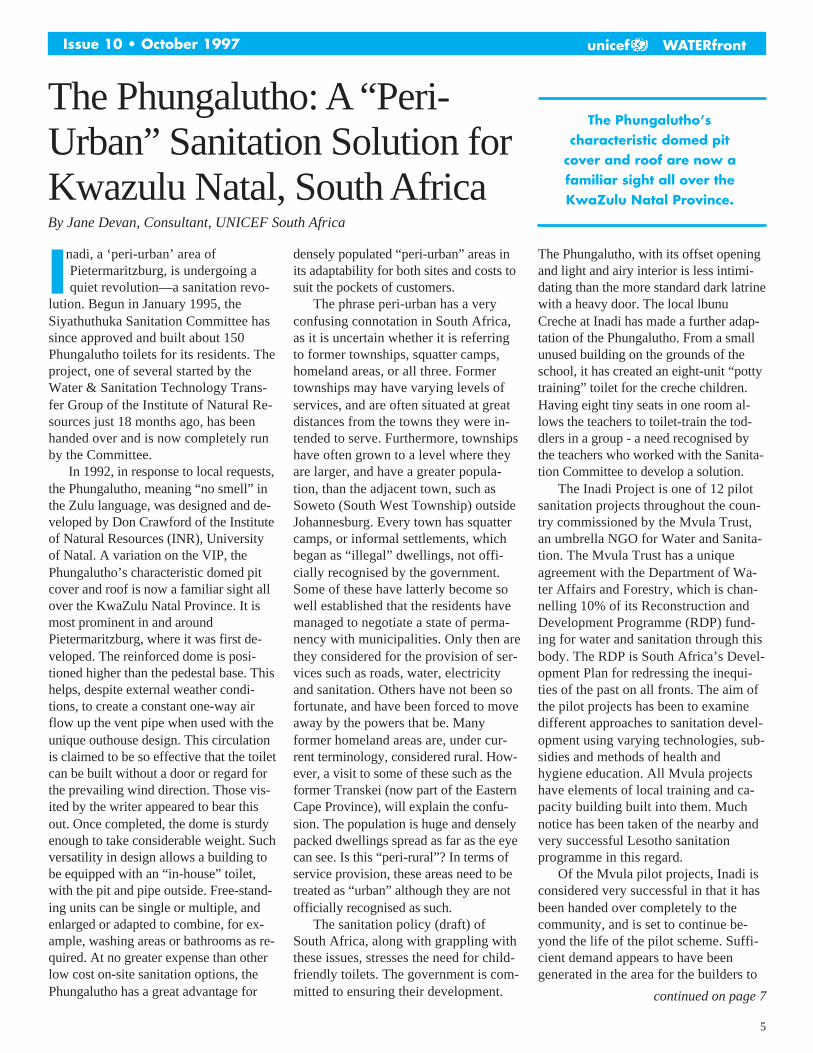
In 1992, in response to local requests,the Phungalutho, meaning “no smell” inthe Zulu language, was designed and de-veloped by Don Crawford of the Instituteof Natural Resources (INR), Universityof Natal. A variation on the VIP, thePhungalutho’s characteristic domed pitcover and roof is now a familiar sight allover the KwaZulu Natal Province. It ismost prominent in and aroundPietermaritzburg, where it was first de-veloped. The reinforced dome is posi-tioned higher than the pedestal base. Thishelps, despite external weather condi-tions, to create a constant one-way airflow up the vent pipe when used with theunique outhouse design. This circulationis claimed to be so effective that the toiletcan be built without a door or regard forthe prevailing wind direction. Those vis-ited by the writer appeared to bear thisout. Once completed, the dome is sturdyenough to take considerable weight. Suchversatility in design allows a building tobe equipped with an “in-house” toilet,with the pit and pipe outside. Free-stand-ing units can be single or multiple, andenlarged or adapted to combine, for ex-ample, washing areas or bathrooms as re-quired. At no greater expense than otherlow cost on-site sanitation options, thePhungalutho has a great advantage for
densely populated “peri-urban” areas inits adaptability for both sites and costs tosuit the pockets of customers.
The phrase peri-urban has a veryconfusing connotation in South Africa,as it is uncertain whether it is referringto former townships, squatter camps,homeland areas, or all three. Formertownships may have varying levels ofservices, and are often situated at greatdistances from the towns they were in-tended to serve. Furthermore, townshipshave often grown to a level where theyare larger, and have a greater popula-tion, than the adjacent town, such asSoweto (South West Township) outsideJohannesburg. Every town has squattercamps, or informal settlements, whichbegan as “illegal” dwellings, not offi-cially recognised by the government.Some of these have latterly become sowell established that the residents havemanaged to negotiate a state of perma-nency with municipalities. Only then arethey considered for the provision of ser-vices such as roads, water, electricityand sanitation. Others have not been sofortunate, and have been forced to moveaway by the powers that be. Manyformer homeland areas are, under cur-rent terminology, considered rural. How-ever, a visit to some of these such as theformer Transkei (now part of the EasternCape Province), will explain the confu-sion. The population is huge and denselypacked dwellings spread as far as the eyecan see. Is this “peri-rural”? In terms ofservice provision, these areas need to betreated as “urban” although they are notofficially recognised as such.
The sanitation policy (draft) ofSouth Africa, along with grappling withthese issues, stresses the need for child-friendly toilets. The government is com-mitted to ensuring their development.
The Phungalutho, with its offset openingand light and airy interior is less intimi-dating than the more standard dark latrinewith a heavy door. The local lbunuCreche at Inadi has made a further adap-tation of the Phungalutho. From a smallunused building on the grounds of theschool, it has created an eight-unit “pottytraining” toilet for the creche children.Having eight tiny seats in one room al-lows the teachers to toilet-train the tod-dlers in a group - a need recognised bythe teachers who worked with the Sanita-tion Committee to develop a solution.
The Inadi Project is one of 12 pilotsanitation projects throughout the coun-try commissioned by the Mvula Trust,an umbrella NGO for Water and Sanita-tion. The Mvula Trust has a uniqueagreement with the Department of Wa-ter Affairs and Forestry, which is chan-nelling 10% of its Reconstruction andDevelopment Programme (RDP) fund-ing for water and sanitation through thisbody. The RDP is South Africa’s Devel-opment Plan for redressing the inequi-ties of the past on all fronts. The aim ofthe pilot projects has been to examinedifferent approaches to sanitation devel-opment using varying technologies, sub-sidies and methods of health andhygiene education. All Mvula projectshave elements of local training and ca-pacity building built into them. Muchnotice has been taken of the nearby andvery successful Lesotho sanitationprogramme in this regard.
Of the Mvula pilot projects, Inadi isconsidered very successful in that it hasbeen handed over completely to thecommunity, and is set to continue be-yond the life of the pilot scheme. Suffi-cient demand appears to have beengenerated in the area for the builders to
The Phungalutho’scharacteristic domed pit
cover and roof are now afamiliar sight all over theKwaZulu Natal Province.
I

6
Issue 10 • October 1997unicef WATERfront
One Hundred and Fifty Wellsin the South of MadagascarJacques Boyer, Information/Communication Officer, UNICEF Antananarivo,Madagascar (Translated from French by Ms. Gina Darcin-St. Louis, WESSection, UNICEF NYHQ)
very day, Marinette washes upwith water from the well beforeheading out to work. She knows
a lot about wells since she was one ofthe first animators of the “150 wells inthe South of Madagascar” Project. Situ-ated in the area of Antanimora, theProject was initiated by the Govern-ment with UNICEF support after the1992–93 drought. From 1994 to 1995,UNICEF in cooperation with theBRGM company drilled 150 handpumpequipped water points throughoutAmbobombe, Beloha, Bekily andTsihombe.
The Project was the first in Mada-gascar to include a social mobilisationcomponent, supported by the effectiveparticipation of local animators. It wasalso the first to establish a system forthe operation and maintenance of thehandpumps and to maintain spare parts.Each well is overseen by a water pointcommittee, which manages a petty cashfund of MGF50,000 (approximatelyUS$10.00) collected from the villagesand targeted for maintenance.The approach has taken root and is nowused by the Japanese Cooperation in itsrural water supply project. The “150wells in the South of Madagascar”Project also served as a model in thedevelopment of the Water and Sanita-tion National Policy and the NationalPlan of Action. Additionally, the WaterDirectorate at the Ministry of Minesand Energy maintains the Project’stechnical database.
In 1996, UNICEF increased its sup-port to capacity building in hygieneand sanitation at the rural level. Thisaction was important as the Project’sthree locally recruited animators couldnot adequately cover the 150 villagesand their communication skills neededupgrading. These deficiencies would
eventually have compromised thesustainability of the project since con-tinuous community sensitization wascrucial to achieve improved sanitationand hygiene practices.
As a result the Project recruited, ac-cording to specific criteria such as theirenthusiasm, popularity and level ofeducation, thirteen main animators
from the community. They receivedtraining in communication techniquesfrom the Ministry of Communication,aided by the NGO, AFVP, which hadtaken over from BRGM in 1996. TwoAFVP volunteers, outposted inUNICEF Antanimore, monitor theproject on a daily basis.
These main animators received ba-sic training in interpersonal communi-cation, group animation, visualteaching materials, and performingskits. They were trained to use theTriple A approach and to monitor theresult of their messages using monitor-ing cards with pictographs. They thenshared their experience and knowledgewith the Rural Animation Cells (Frenchacronym: CVA). A CVA is a group oftwo women and one man chosen by thecommunity to perform the same dutiesas the main animators; they are the linkbetween the animators and the commu-nity. The objective for 1997 is to add60 “cells” to the 20 created in 1996,and to have a CVA in all 150 villages
by the end of 1998. Besides training incommunication and monitoring tech-niques, the CVA learned about waterrelated hygiene from the main anima-tors, who had been trained by UNICEFand AFVP. The CVAs transmit basicinformation on water use, maintenanceof water points and ways to keep watersafe from collection to consumption.This year’s training will also cover per-sonal and household hygiene.
At least twice a month, the mainanimators visit the 150 villages (subdi-vided into 13 branches) to collect themonitoring cards and hold discussionswith the CVAs and beneficiaries. TheAFVP volunteers pay regular visits,followed by representatives from theMinistry of Communication andUNICEF. It was discovered that someteaching materials developed duringthe first phase of the project were notalways appropriate for illiterate villag-ers; revisions were made to accommo-date the needs of the target population.
Before the creation of the CVA, theproject had limited linkages withUNICEF- assisted and non-assistedprogrammes operating in the 150 vil-lages. Using water as an entry point toother survival and development activi-ties, the coordinators of the 150 wellsProject created the CVAs to integratethe diverse activities and harmonize thevarious health and hygiene messages.In the future, CVAs may be used ascommunication vehicles for messagesabout issues such as nutrition and edu-cation.
Although still new, the results ofthe Project appear promising. This iscorroborated by the enthusiasm of thepopulation for the animation skits; thesuccess rate in maintaining the waterpoints; the reduction of water relateddiseases; and the interest of donors inextending the “150 Wells in the Southof Madagascar” Project to other partsof the country.
The Project was the first inMadagascar to include a
social mobilisationcomponent, supported by the
effective participation oflocal animators.
E
7
Issue 10 • October 1997 unicef WATERfront
fill their order books, and to make a veryreasonable income from their work. Hav-ing obtained the moulds, the technologyfor building is straightforward and adapt-able. Superstructures can be designed tosuit the pocket of the client as doors,windows, pedestals, seats and sinks areall optional extras. A further adaptationhas been a ‘pit’ above ground level, forareas that either have impenetrable bed-rock or are prone to flooding. INR hasdeveloped an illustrated constructionmanual in both English and Zulu, which,with a basic understanding of construc-tion principles, is possible to follow.
A simple bookkeeping system devel-oped over time between the INR and itsprojects allows all monies to be tracked.Details of expenditures on any single jobare recorded on the reverse of the
cheques paid and no cash changes hands.This is a particular feature of an urbansanitation programme that makes it rela-tively easy to manage financially, butthat may not be feasible in more remoteareas.
An example of how well this tech-nology travels can be seen in Oshakati,the second largest town of theneighbouring country, Namibia. An ur-ban development programme, OHSIP,imported and built several different on-site sanitation options for the residents ofthe informal settlements aroundOshakati. The Phungalutho was chosenas the most favourable option, particu-larly due to its odourless quality, but alsobecause the adapted design of the linedpit was raised above the ground level.This reduced the effects of seasonal
flooding, common in that area. The localname of “Okakedi” has developed forthis adapted Phungalutho, also meaning“no smell” in Kwanyama. Over 1300 toi-lets have now been built in Oshakati, andthey fared well during the serious flood-ing of the 1995 rainy season.
Following democratisation in 1994,South Africa is still debating its futuresanitation development policy for the es-timated 21 million people without ad-equate toilets. Decisions on thorny issuesregarding subsidies, routine maintenanceand institutional responsibility have yetto be made at a national level. A varietyof technologies and approaches need tobe available to suit differing conditionsthroughout the country. It is very likelythat the Phungalutho will form part of thesolution.
■ Phungalutho: Sanitation Solution for Kwazulu Natal, South Africa from page 5
■ UNICEF & UNEP, from page 4
cies and rules regarding disclosure of in-formation, the two parties shall en-deavor to exchange information anddocumentation in matters of commoninterest.
13. The two parties shall designatetheir respective focal points who willjointly develop annual plans of actionfor specific collaborative activities andregularly assess the effectiveness of thecooperation under this Memorandum.
14. In the implementation of the ac-tivities, the parties agree to seek partner-ships with relevant organizations withinthe UN system as well as inter-govern-
mental and non-governmental organiza-tions, development banks, the privatesector, donors, the scientific and aca-demic communities, and other civil so-ciety members.
Amendment15. The provisions of this Memoran-
dum may be amended any time by writ-ten agreement reached between the twoparties.
Termination16. This Memorandum may be ter-
minated by either party by giving theother party a six-month’s notice in writ-ing of the intention to terminate.
Entry into Force17. This Memorandum shall take ef-
fect as of the date of its signature.
In faith whereof the parties havesigned this Memorandum in the Englishlanguage in two copies in New YorkCity on this fifth day of March, Nine-teen hundred and ninety-seven.
Carol Bellamy Elizabeth DowdeswellExecutive Director Executive DirectorFor the United For the United NationsNations Children’s Environment
Fund (UNICEF) Programme (UNEP)
UNEP-UNICEF partnershipIn recognition of the need to comprehensively address the nexusbetween children and the environment, and to combine relativestrengths in this regard, UNEP and UNICEF are enhancing theircollaboration and stimulating this partnership through this flexibleMemorandum of Understanding. This MOU will serve not only asa strong joint commitment for cooperation in support of UNEP andUNICEF’s respective and complementary missions but, also signifi-cantly, as the framework within which to develop specific coopera-tive initiatives for practical implementation at the field level.
This synergistic partnership extends UNEP’s environmentalpolicy guidance role to the country level through UNICEF’s field
network. UNEP’s technical expertise will provide a substantive in-put to UNICEF’s operational activities in the areas of collaborationand assist UNICEF to adapt and disseminate environmental infor-mation for action at the field level for PEC related activities. It willencourage UNEP to incorporate child related concerns into itsprogramme activities. It will also facilitate the task of injectingchild and environment-sensitive concerns into policies and projectswithin and outside the UN system. Finally, this UNEP-UNICEFpartnership is a concrete response to the call from member Gov-ernments for enhanced effectiveness and improved UN system-wide cooperation, building on the comparative advantages ofboth organizations.
8
Issue 10 • October 1997unicef WATERfront
Social Determinants ofHousehold Hygiene inSanto Antao, Cape VerdeDominique Béhague, Research Fellow in Medical Anthropology, LondonSchool of Hygiene and Tropical MedicineNuno Egídio, WES Project Officer, UNICEF Cape Verde,Antero Pina, WES Ass. Project Officer, UNICEF Cape Verde
Introductionanto Antao, the most mountain-ous of the nine inhabited islandsof the Cape Verde archipelago, is
second in geographical size (977 km2)and third in population (43,845 inhabit-ants), 80 percent of which live in therural areas. Its rugged physical and to-pographic conditions, and the scarcityof water (annual average rainfall of 250mm), make living conditions for the ma-jority of the population, which dependon traditional agriculture and govern-ment labor intensive public works forsurvival, very difficult.
In 1986, because only 10 percent ofthe rural population of Santo Antao hadaccess to drinking water, and becausesanitation was virtually nonexistent, theGovernment of Cape Verde and UNICEFinitiated a major intervention in the is-land. Ten years later, the percentage ofthe rural population with access to drink-ing water was 72 percent and to sanita-tion, 15 percent. The great increase inaccess to drinking water, achievedthrough gravity fed systems and self-helpconstruction of rain water harvesting sys-tems at the household level; and the firstsuccessful history of self-help construc-tion and utilization of dry latrines inCape Verde (utilization rate of 72 per-cent), are considered the major accom-plishments of the intervention.
However, despite the increased ac-cess to water supply and sanitation sys-tems, and the concurrent implementationof hygiene education campaigns, a re-cent study found that Santo Antao is stillone of the islands with the highest levelof diarrhoeal prevalence in children un-der five years of age. To understand the
possible reasons for this discrepancy, anethnographic study on household hygieneand its cultural, economic, and social de-terminants was conducted. The investiga-tion of social and cultural factors isimperative since many studies haveshown that access alone does not auto-matically affect behaviour.
Objectives. conceptualframework and methodsThe study aimed to investigate specificaspects of domestic hygiene behaviourand their social, economic and culturalantecedents. In particular, excreta dis-posal, personal hygiene, water usagepatterns and hygiene, and domestic hy-giene were the foci of investigation. So-cial antecedents were explored not onlyin terms of individual cognitive factors,such as knowledge and attitudes, butalso in terms of social factors, such asthe household distribution of “health-improving” resources, kin relations,
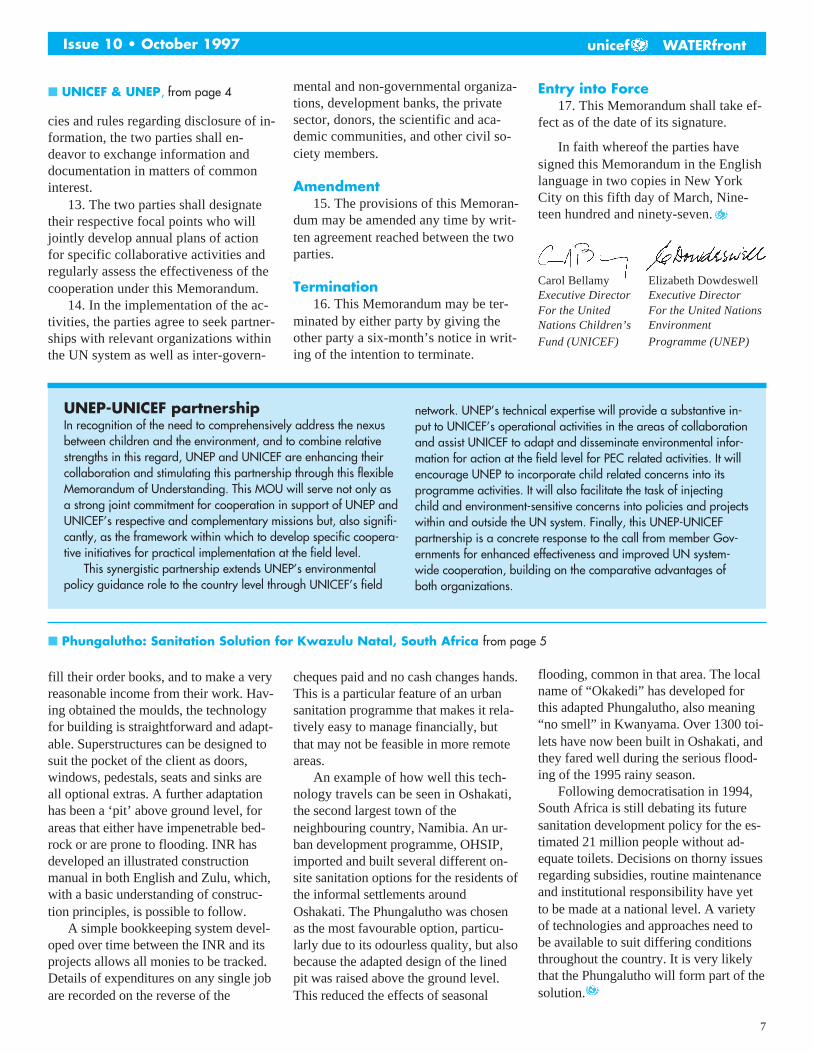
parenting and child development, socialstatus and power. Figure 1 outlines therelationship between hygienebehaviours and the possible antecedentsto hygiene behaviours that were ex-plored in this study (in italics).
Fieldwork was conducted in two ru-ral areas of Santo Antao during a 21 dayperiod. Like all research studying sensi-tive and private behaviours, data collec-tion relied heavily on triangulation andvalidation of the data by using a varietyof methods. All homes with at least onechild under five years of age in bothcommunities were included. With fullparticipation, this resulted in a total offorty-one households. Two to four mem-bers were interviewed or observed ineach home, which included grandmoth-ers, children, fathers or other kin mem-bers. In all, the views and behaviours ofapproximately 82 individuals were ex-plored. Methods included informal in-terviewing, participation in naturallyoccurring group discussions, participantobservation, six hour-long continuousstructured and unstructured observa-tions, and observational spotchecks.
ResultsChild defecation practices will be the fo-cus of this article, as it is deemed moreuseful to explore one topic in greaterdepth than all hygiene behaviours super-ficially. Children were much more indis-
continued on next page
F I G U R E ␣ 1 Preliminary Theoretical ModelTime availability Beliefs/cult norms
Activities promoting Kin structure Hshld dist. of $/unhygienic conds Household decision-making/
amount of “trafflc” Structure timenumber of peopleamount of cookingpresence of animals
Actual hygiene behaviors needed to cope with activitieswater usage patternsexcreta disposaldomestic hygienehand-washing
AccessHouse-Help
IncomePersonal prefs
Household hygiene status
S

9
Issue 10 • October 1997 unicef WATERfront
criminate about the timing and place oftheir defecation than adults, who tendedto defecate in designated areas in thesurrounding parts of their community inthe evening hours. Thirty-five defeca-tion episodes for 24 children (most ofwhom were over one year of age) wereobserved during the structured observa-tions. In 20 (57%) occasions, childrenwere observed to defecate on the floor(patio or in the home) or in the streetand in only three occasions did childrendefecate directly in a basin. Never wasthe latrine used directly by children, andin only two occasions were children’sfeces disposed of in a latrine. On 13 oc-casions (37%) the defecation site wascleaned by the mother or another adult,but in a substantial number of instances(8-23%) another child cleaned the site.In 13 (37%) instances, the site was notcleaned at all. Most of the defecationsites that were cleaned were done sowith a broom, a piece of cloth, or paper.In a significant number of instances (13-39%), the child was not cleaned at all,but when he/she was, most caretakersused a cloth (6) or plain water to cleanthe child (6). This may be because inmany instances (10) the index child ei-ther cleaned himself or was cleaned byanother child. Perhaps the most tellingfinding pertains to hand-washing. In
only two cases did the person whocleaned the site or the child wash theirhands with water or water and soap (oneof each). Simple comparative analysisshowed that single-headed homes,women with a greater number of chil-dren, a greater number of parental part-ners, and with lower schooling, allexhibited poorer hygiene behaviours re-lating to child defecation practices. Thissuggests that poor defecation practicesare indeed affected by concrete condi-tions which limit families’ abilities torespond more appropriately.
Child hygiene in the context of householddynamicsWhen one looks at mothers as imbeddedin dynamic households rather than sim-ply as “primary caretakers,” then thequestions regarding the relative impor-tance of the various elements needed tosustain the health of household members(acquisition of water, food, employ-ment) emerge. Placed into the context ofthe variety of household and child-carechores that must be done in one day, thechild’s hygiene had low priority. Theimmediacy of competing caretaking anddomestic tasks was manifest in both theinterviews and the unstructured observa-tions. Promotional campaigns mustspeak to the reality that life events areexperienced as an interaction of needs
and assessments. While it is clear fromthe literature and from this study thatpoverty affects hygiene status, it is im-portant to stress that poverty does notlead to parental negligence.
Approaches to child developmentLocal approaches to child developmentprovide a wider understanding of socialfactors. A child’s cleanliness is, to a cer-tain extent, seen to be part of his/her in-herent nature. Not only are childrenexpected to learn how to clean them-selves (and their environment) from anearly age, but the degree to which theywill take up hygienic habits is depen-dent upon their own “nature” degree ofphysical discomfort with dirtiness. Inthis way then, a child’s personal hygieneis seen by some to depend on personaltemperament rather than household en-vironment. Defecation is one of manylearned behaviours that parents andolder siblings consider their responsibil-ity to teach. Children are encouraged tolearn how to defecate alone or withminimal assistance (without the use ofdiapers) once they have learned to walk.In general, children who know how towalk and fend for themselves at an earlyage are considered easier to care for, butthis is also a sign of good child develop-ment. As such, children’s hygiene andindependence were tied to mothers’sense of pride.
Teaching older children to do house-hold chores is also considered an impor-tant part of child development. Givingolder siblings chores and responsibilitiesin the home is not only part of managinga household, but an integral part ofteaching children how to become fullmembers of society. It stimulates orderand good habits, preparing children fortheir future as workers and parents.“Simple” tasks, such as holding an in-fant, can be expected from children asyoung as 3-4 years old. In almost everyinterview, parents explained that chil-dren need greater contact with the “out-side” world and environment for strongand healthy development. Children whoare raised “in the mother’s hand” or “onthe mother’s back” grow to be weak,
continued on page 10Water Point: the ideal place for hygiene promotion

10
Issue 10 • October 1997unicef WATERfront
■ Cape Verde, from page 9
learn to sit and walk very late, and mayeven be more likely to die. If a child isto be put on the ground to play, it is gen-erally considered better that they do soon the home’s patio rather than insidethe actual home, as this provides a morestimulating and “free” environment. Al-though some of these socializing rou-tines are explicitly conscious, theyconstitute an important aspect of theCape Verdean social setting. These gen-eralized positive views of independentchild development provide a backdropfor understanding care-taking ap-proaches as something other than lackof parental attention.
We also conducted a comparativequalitative analysis to explore some is-sues affecting hygiene status that go be-yond economic difficulties, and whichmay be more amenable to change. Fourvariables were used as proxies for socio-economic status in this setting: mother’sschooling, household headship,mother’s number of parental partners1,and number of children. For this com-parative analysis, we compared thosefamilies who, despite their improvedsocioeconomic conditions, demonstratedpoorer hygiene behaviours (based onobservations and spot-checks) withfamilies who lived in poorer socioeco-nomic conditions but demonstrated betterhygiene status. The main differentiatingvariables between the two groups weresocial conflict and support. The familiesliving in poorer conditions but maintain-ing good practices were headed by olderwomen with many children. Thesewomen had little contact with the fa-thers of their children, but this causedthem little overt conflict. The homeswere the subject of constant visits byneighbors and friends, and discussionsabout infant health and community life,enthusiastically agreed to when re-quested by the interviewer, often in-volved friends and neighbors. Interviewswith these women were frequently longand intricate, indicating their self-per-ceived knowledgeable status. Indeed,some of these women were key figuresin the community, well involved in net-
works of exchange of favors andgoods.
In contrast, the homes with better so-cioeconomic conditions but worse hy-giene conditions were more sociallyisolated. Often the women of thesefamilies were new members to the com-munity and their homes were at agreater distance from most of the otherhomes. Interviews were generally heldseparated from other family membersand conversation more stilted. In each ofthe interviews, women either madenegative references to the father of theirlast child (eg. “he does not give anymoney, or, he wastes it all on alcohol”)or referred to soured friendships with
neighbors or extended family members.It is likely that women with a more ex-tensive social support system are morelikely to receive help both in completingdomestic chores and with child care. Inaddition, maintaining a home hygienicin difficult conditions consumes a con-siderable amount of time, physical en-ergy, morale, and even emotionalstamina. It could be that social conflictand isolation may affect householdmembers’ ability to maintain their homein the face of possibly more compellinghousehold dynamics that go beyond therealm of logistical issues.
ConclusionsGood hygiene maintenance is not sim-ply a matter of general carelessness or alack of appreciation for the germ theoryof disease transmission. Furthermore,just because some families demon-strated poor environmental hygiene didnot mean they would also be less in-clined to wash their hands. Comparativeresults from this study suggest that, forexample, hand-washing is a more ha-
bitual practice, child defecation part of amore global approach towards child de-velopment, general home environmentalhygiene subject to time constraints, andbodily hygiene possibly related to ac-cess and use of water sources. Each ofthese different realms of hygiene prac-tices belongs, in a sense, to different as-pects of daily living. Therefore, lumpingthem together in public health cam-paigns as part of a global effort to edu-cate people about the transmission ofdiarrhea pathogens may, in effect, ex-tract them from their local social andcultural significance. In addition, resultsfrom this study showed that householdscannot be taken as discrete, insular enti-ties. It is possible that women with moreextensive and supportive kin and non-kin social networks may be in a befterposition to counter the structural diffi-culties of maintaining a hygienic house-hold. The exchange of goods andservices, including child care, makeshouseholds not only less bounded butalso less “reliant” on factors such as“paternal presence” to seal their fate. Inaddition, what is also important aboutthis finding is that hygiene is not solelya matter of individual will, but extendsinto issues of social isolation and com-munity dynamics.
Cape Verde is characterized by an in-formal polygamous social organizationwhereby it is quite common for a womanto have her children with several differ-ent men in succession. Previous studieshave shown increased number of parentalpartners to be associated with both eco-nomic status and maternal education.
Latrine is today a household norm
Good hygiene maintenanceis not simply a matter ofgeneral carelessness or a
lack of appreciation for thegerm theory of disease
transmission.

11
Issue 10 • October 1997 unicef WATERfront
Water Points Committees forCommunity DevelopmentBy Julio M. Balde, National Officer, WES, UNICEF Guinea-Bissau.
chools and health clinics fre-quently serve as starting pointsfor activities focusing on com-munity development. However,
within Guinea-Bissau, these institutionsare spread thinly; only a minority of the3,600 villages in the country has healthcentres or schools. Therefore the impor-tant challenge remains of finding net-works and groups that could becomebases for involving the population inwater, sanitation, health and other devel-opment activities.
There are approximately 2,500 waterpoints in rural areas, most of which areboreholes with hand pumps. These aremanaged by water point committeeswho have responsibility for ensuringsanitary conditions around the waterpoints, collecting funds from users forspare parts and organizing repairs. Thesystem works fairly well. For example,a recent survey of boreholes withhandpumps showed that about 90% ofthem were operating.1 However, water isnot the only sector in this country inwhich users participate and share costs.Another example is the Bamako Initia-tive where village committees organizehealth education activities and monitorimmunization. The community contrib-utes to the purchase of essential drugs.Analogous village-based groups are be-ing formed in other sectors, such as ag-riculture and promotional activities withwomen. It is likely that community or-ganizations meant to manage infrastruc-ture and share costs, nominally viasingle-purpose committees, will prolif-erate in Guinea-Bissau. However, in anation where two-thirds of the popula-tion live in villages of less than 500
people, this can result in a multiplicityof committees, village animators andmessages often competing at the villagelevel.
To avoid this, organizational strate-gies are needed in communities to en-able the integration or closecoordination of various development ac-tivities. The water point managementcommittees could play a significant rolein this process. Presently there are 2500water points and plans to set up 1,500more in the next four years. In this con-text, water and water points could serveas entry points to address developmentproblems and the needs of communities.The water point committees can fulfillan educational role and become focalpoints for information that stimulatesbehavioral change around health, hy-giene and primary environmental careissues.
An expanded role for water pointcommittees will induce another form ofanimation. The animator, is a memberof the community and knows the people,
the challenges and daily problems of hisor her village. UNICEF is supportingthis approach via a project “Capacitationof Water Point Management Commit-tees.” The major lines of the programmewill be:
■ Technical assistance for the develop-ment of strategies to support and ac-tivate water point managementcommittees. This work will be donein collaboration with the Interna-tional Centre for Water and Sanita-tion (IRC), headquartered inHolland.
■ Capacity-building of extension work-ers (animators) from various devel-opment projects, sensitizing them tothe role that water point committeescan play in support of various com-munity development efforts.
■ Training of village-based committeesin communication methods and inthe use of educational materials re-lated to water and sanitation, hygieneand prevention of certain diseasessuch as cholera.
Elaborating follow-up strategies anddefining indicators of progress will beother components in this project whosethrust is to guarantee inter-sectoral col-laboration in rural areas.
S
1Koen van der Werf and Jan Teun Visscher,Towards sustainable water supply: eightyears of experiences from Guinea-Bissau.(Draft) IRC, 1995, 60 p. The Hague, p.21
Excerpt from UNICEF Statement to the 19th UN GeneralAssembly Special Session for Review and Appraisal ofthe Implementation of Agenda 21 from 23 to 27 June1997 in New York
UNICEF“It is children who have the biggest stake in sustainable
development.…All too often, we find that our concerns for children andwomen in the social sphere are considered separately from those in the ar-eas of environment and economic development.
…UNICEF is making a strategic shift away from pure drinking watersupply and latrine construction to household water security and commu-nity-based management of water environment. Increasingly, countryprogrammes are taking a more holistic view towards household water secu-rity stressing conservation, watershed protection and equity of access. Theapproach to sanitation has broadened to take in hygiene, behavioral changeand relevant environmental health aspects.”

12
Issue 10 • October 1997unicef WATERfront
K for Kakus or latrine, S for Sampah orgarbage and A for Air limbah or wastewater. The SARASA philosophy is toimprove R.A.K.S.A in the desa (villages)through the efforts of communitiesguided and mobilised by the santris.RAKSA is also used to classify villagesthroughout the province. The RAKSA IVtitle is accorded to villages with morethan 80% water supply and family latrinecoverage and RAKSA I to those withcoverage of less than 50%. RAKSA I andII villages were subsequently selected astargets for the SARASA activities carriedout in five phases at three month inter-vals over the past two years. Each phaselasted for 12 days, involved 150 santrisand was funded by a budget of approxi-mately US $430,000 from the provincialgovernment. The budget was used for thedevelopment of information materials,training activities, support for the workof santris in the targeted villages (trans-port and living allowance), and materialsto assist poor families. It is expected thatafter the completion of the 12-dayprogramme the santris will maintain linkswith the villagers.
Local and national media have givenextensive publicity to the SARASAprogramme, which covers a wide rangeof activities. Besides betterment of theWES facilities and increased awareness-raising activities, SARASA focuses onhousing renovations, such as floor plas-tering, ventilation improvement, sepa-rate animal pen construction, and treeplanting and vocational training for thedevelopment of cottage industries. Fromthe government side, many regionalagencies including Health, Agriculture,and Education, are involved in theprogramme. Senior officials from theseagencies are appointed patrons for dif-ferent villages and encouraged to moni-tor the progress of SARASA throughinformal visits, such as attending Fridayprayers.
The experience of BandungDistrictIn Bandung District, site of the provin-cial capital, the fifth SARASA phase
SarasaBy Hilda Winarta, WES and YD Mathur, Project Officer, WES, UNICEF Jakarta
Backgroundt is hard to reconcile the sight ofthe immaculately clean streets ofmany West Javan towns and the
lush rice paddies and plantations in theregion’s rural areas with the fact thatsanitation coverage in the province isonly 40%. A survey conducted in fourdistricts in 1993 revealed that hygienicpractices are still limited; 22% of thepeople use latrines and only 40% washtheir hands after defecation. With apopulation of almost 40 million people,West Java, administratively divided into24 districts, 526 subdistricts and 5869villages, is the second most populousprovince in the country.
The majority of people in rural com-munities in West Java consider the idealfacilities for defecation to be places withplenty of water and away from theirhomes. Streams, canals, fish ponds andother water bodies are the most preferredplaces; the local polite term for defecationis “kaca ‘i or “going to the water.” It isstill quite common to find modern lookinghouses in rural areas, perfectly constructedaccording to the prevailing building codes,having all the usual amenities, and lackingindoor toilet facilities.
A needs assessment exercise con-ducted in 1993 revealed that meeting thetarget of universal coverage in the year2000, would require building 4,346,237,or at least 700,000 family latrines peryear in West Java. This is clearly be-yond the capacity of the Government,since the sanitation development budgetcould only support the construction of afew hundred latrines annually.
The alternative is to mobilise com-munity resources. Technical and finan-cial aspects are not a major hindrance,due to the availability of lowcost appro-priate technologies, such as molds, andthe renowned craftsmanship of the WestJavan. However, social, institutional andmore than anything else, motivationalproblems remain the greatest challenges.
The Clean Friday Movement was
launched by President Soeharto in No-vember 1994 as a national effort to meetthese challenges. “Gerakan JumatBersih” or “GJB”, as the Movement islocally known, aims to promote healthyliving behaviour among the communi-ties. All institutions, governmental andnon-governmental, are involved inmobilising community resources to im-
prove their living environment. In par-ticular, the Movement calls upon reli-gious leaders, whose influence upon thecommunity is recognized to far exceedthat of government, to motivate peopleto change their behaviour.
The SARASA MovementThe West Java provincial administrationrecognized the potential benefit providedby the existence of tens of thousandssantris (Moslem scholars) in the prov-ince. Almost 90% of the West Java popu-lation is Moslem and to them santris,both male and female, have a special sta-tus. Although young, the santris arehighly respected for dedicating their livesto full time religious study as residentscholars at the pesantrens (Islamic board-ing schools) and for their future role asreligious teachers.
While most of the other provinceswere still struggling to define their re-spective provincial strategy for imple-menting the GJB, West Javaimmediately took off with a movemententitled “SARASA,” an acronym of“Santri Raksa Desa” which literallymeans “Santris to nurture villages.”R.A.K.S.A is also an acronym: R standsfor Rumah or houses, A for Air or water, continued on page 17
I
The majority of people inrural communities in West
Java consider the idealfacilities for defecation to beplaces with plenty of water
and away from their homes.
13
Issue 10 • October 1997 unicef WATERfront
Sanitation through Schools:UNICEF Experience inCambodiaBy Festo P. Kavishe, Senior Project Officer, Community Actions for SocialDevelopment (CASD) and Wan Maung, Water and Sanitation Consultant
Introductionhe environmental sanitation situa-tion in Cambodia in both urbanand rural areas is alarming. The
lack of toilets in rural dwellings, includ-ing those that are fairly modern, wouldstrike even a casual visitor. In urban ar-eas, the toilets in many buildings areadded as an after thought. The situationis starkly quantified by the 1996 demo-graphic survey of Cambodia. Less thanhalf (49.5%) of households in urban ar-eas had a toilet facility, and in the ruralareas, it was a mere 10.3%. Overall, itwas estimated that only about 15% ofhouseholds in Cambodia have toilet fa-cilities. One major explanation for thisstate of affairs can be found in the tradi-tional behaviour associated with the useof toilets.
A micro-survey conducted in se-lected rural areas found that among therespondents, defecation at the edge ofthe yard was practised by 27%, the openfield, 58%, and at the river banks, 2%.About 76% of adults used leaves foranal cleaning whereas 98% of youngchildren predominantly used water.People have the habit of burying theirfaeces or simply covering the faeceswith soil. About 87.7% of villagersidentified lack of interest as a problemfor latrine building. But clearly, this isnot an issue of lack of interest, but oneof behaviour. It is interesting to note thechange in anal cleaning practices fromadults to children. This is indicative oftwo things. First, the linking up of waterand sanitation in Cambodia is finallybearing fruits. In the past, there wasmuch debate about whether sanitationshould be linked to water as most peopledid not use sanitary facilities in whichwater was a requirement. Second, the
change of anal cleaning behaviour inchildren supports the use of schools asthe main agents for promoting soundsanitation strategies.
Changing sanitary behaviourthrough community school-based strategiesAs part of the Country Strategy for Ru-ral Water Supply and SanitationProgramme, the Royal Government ofCambodia with the support of UNICEFand several NGOs set up a sanitationawareness programme using a school-based community approach. The ap-proach was facilitated by twodevelopments in Cambodia. First, theMinistry of Education with UNICEFsupport, was successfully implementinga pilot system of community-basedCluster Schools. The system is based onselecting one school to be developed intoa resource reference school for surround-ing schools, using community manage-ment. The School Cluster systempromotes equal access to educationthrough sharing of technical and educa-tional materials. Because of its success inthe pilot areas, the system has now beenadopted nationwide. The second develop-ment was that of a Government/UNlCEFprogramme of Community-based Ac-tions for Social Development (CASD) inwhich water and sanitation form an im-portant component. This area-focusedprogramme incorporates all relevant localinstitutions, especially schools, in stimu-lating community actions for the socialdevelopment of children and women.The school-based sanitation related ac-tivities of the CASD programme includebasic sanitation and water provision toeach cluster school, and health, sanitationand environmental conservation mes-
sages in the curricula.Within this framework, in July 1995
a pilot phase of the “School SanitationProgramme,” annexed to the UNICEF-assisted Cluster School Programme, wasintroduced in two provinces. TheProgramme had the following objec-tives: (a) to help meet the immediatesanitation needs in the selected schools,(b)to serve as demonstration sites forfamily and public latrines, and (c)to pro-vide a practical forum for disseminatinghealth and hygiene information.
Collaboration with partnersThe pilot project was introduced in twoareas and implemented through two in-ternational NGOs (Refer to CambodiaMap). In Steung Treng (Northeast)province, the AICFIUSA (now PartnersIn Development, PIP) was selected as animplementing partner agency and CON-CERN was chosen for BanteayMeanchey (Northwest) province.UNICEF support focused on materialinputs for latrine construction. TheNGOs were responsible for mobilisingcommunity labour and material inputs,supervising construction sites, trainingof teachers and students in hygiene edu-cation, and where feasible, developingwater supply facilities. Governmentcounterparts from Provincial Depart-ments of Education, Health and RuralDevelopment, the agency responsiblefor rural health care, were actively in-volved by providing technical assistanceand supervising NGO staff. The centralGovernment departments contributed tothe preparation of a training module, de-sign development and overall coordina-tion. Funding was provided by theSwedish International Development Au-thority (SIDA) through UNICEF.
Criteria for selection of schoolsThe selection of the schools was de-cided cooperatively with representativesfrom the Ministries of Education, RuralDevelopment and other concerned par-ties. The schools were selected from theUNICEF-assisted cluster schools; par-ticular attention was given to ensuring a
T
continued on page 17
14
Issue 10 • October 1997unicef WATERfront
Safe Disposal of Human ExcretaLow Cost Latrine TechnologyOptions, Bangladeshby T.V. Luong, Sanitation Coordinator, WES Section, UNICEF, Bangladesh(currently the Senior Adviser on Environment and Sanitation, WES Section,UNICEF Headquarters, New York)
BackgroundToday, about 48% of the population inBangladesh have and use sanitary la-trines because of the recently acceler-ated sanitation promotion in the country.Various lowcost latrine technology op-tions, ranging from homemade pits towaterseal models, are being promoted tosuit the financial capability of thepeople. Among the families who havesanitary latrines, 60% built the home-made type and 40% the waterseal. Mostrural people are aware that diarrhoealdiseases are caused by indiscriminatedefecation, poor hygiene practices andpolluted drinking water.1 2 The introduc-tion of the homemade latrine optioncoupled with intensive social mobiliza-tion has been an important factor in theacceleration of sanitation coverage.
Promotion of sanitation inBangladesh started as early as 1962;however, until 1987 the waterseal la-trine was the only type of latrine pro-moted. In 1988 the government adoptedthe Integrated Approaches (IA), usingsafe water supply as an entry point topromote sanitation.
To provide a place to procurewaterseal latrine parts and promote sani-tation, the Department of Public HealthEngineering (DPHE) assisted byUNICEF, established in 1978 villagesanitation centres (VSCs). VSCs or pro-duction centres sell waterseal latrineparts at a subsidized price. By 1990,1000 VSCs had been established. Inspite of the subsidized cost of the la-trine, Taka 125, (US$ 3) for one rein-
forced concrete cement (RCC) slab withwaterseal pan and one concrete ring,many rural families still cannot afford it.Most of the people in rural areas arefarmers; many are landless. The dailywage for an unskilled labourer is aboutTaka 40–50 (US$ 1 –1.25).
Over the years, the demand for sani-tary latrines has stimulated the growthin latrine producers. A national surveyon latrine producers and the market situ-ation in 1994 reported that there is a to-tal of 4152 latrine producers inBangladesh. The number of private pro-ducers doubled in the last three yearsreaching more than 2500. There areabout 100 potters who make traditionalburnt clay wares such as rings, cookingpots, water pitchers, toys, etc. and are
now producing latrine parts. The burntclay rings that are traditionally used as alining for hand dug wells are now alsoused as latrine pit linings. Broken bot-tom clay water pitchers are being usedas squatting holes and pit linings bysome rural families.
Low Cost Latrine TechnologyOptionsBased on a 1994 nationwide survey3, thetypes of latrines built and used in the ru-ral and semi urban areas can be classi-fied as follows:
Type 1 Homemade (do-it-yourself) pitlatrine—direct or offset pit with andwithout lining
Type 2 Simple pit latrine with RCCslab and squatting hole and concretecover with handle (SANPLAT)—di-rect and offset pit with and withoutlining
Type 3 Simple pit latrine with concreteslab and burnt clay pan or cementpan without waterseal—direct andoffset pit with and without pit lining.
Type 4 Single pit waterseal latrine—di-rect and offset pit with or withoutlining
Type 5 Double pit waterseal latrinewith lining
The paper was prepared as a contribution tothe WHO Sanitation Collaborative CouncilWorking Group on Promotion of Sanitation,Geneva, Switzerland.
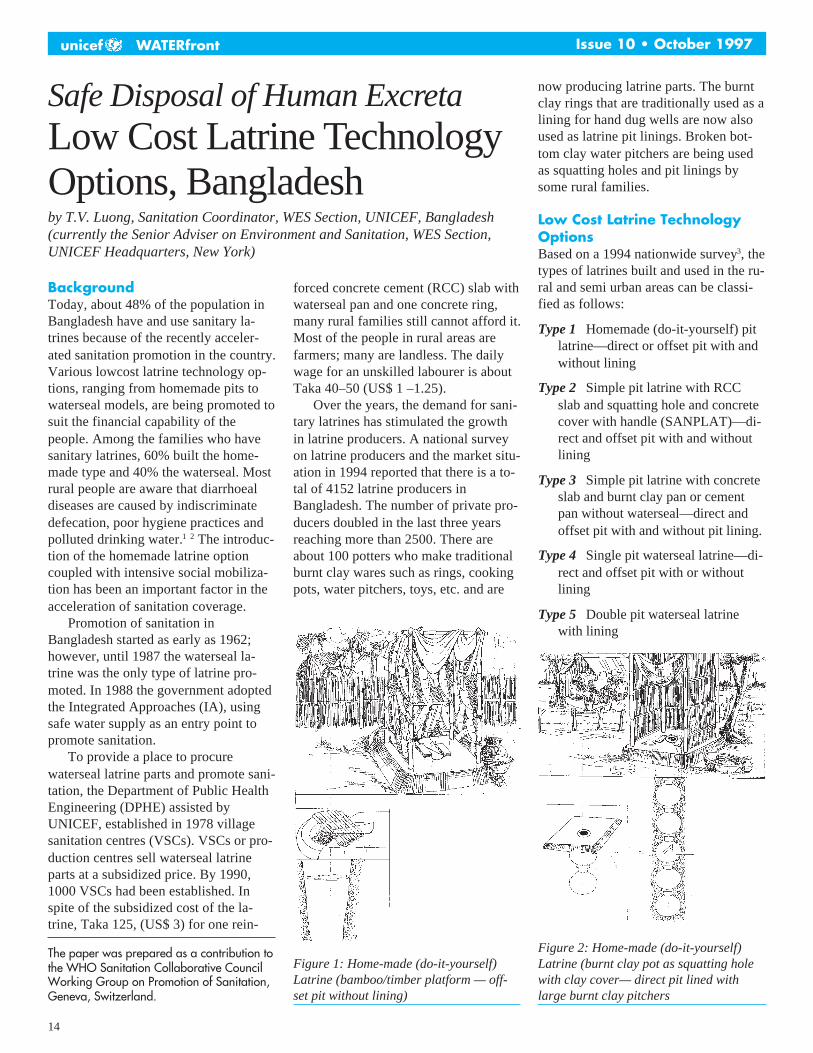
Figure 1: Home-made (do-it-yourself)Latrine (bamboo/timber platform — off-set pit without lining)
Figure 2: Home-made (do-it-yourself)Latrine (burnt clay pot as squatting holewith clay cover— direct pit lined withlarge burnt clay pitchers
15
Issue 10 • October 1997 unicef WATERfront
See illustrations of sanitary latrinesconstructed and used by the people.
Latrine Construction MaterialsThe Bangladesh people are creative.They make use of various low cost, lo-cal materials to build their latrines.These materials are summarized below:
Squatting platform– Bamboo/timber with squatting
hole;– Compacted mud platform with
burnt-clay pot as squatting holeand/or burnt clay pan with orwithout waterseal (for offset pit);
– Concrete platform (RCC slab)with squatting hole and concretecover with handle (SANPLAT);
– RCC slab with cement pan orburnt clay pan without water seal;
– RCC slab with cement pan withwaterseal.
Pit lining:– Bamboo—full, half and/or split
(mat)– Burnt-clay pitchers– Burnt-clay rings– Bricks– RCC rings
Superstructure:– Dry leaves of banana, palm and/
or trees;– Bamboo (full/half size or mat);– Thatch or dry grass;– Dry jute sticks;– Old jute cloth;– Timbers and tree branches;– Corrugated iron (CI) sheets;– Brick mud wall.
To reduce costs even further, manyrural latrines are built without roofs;roofless models are also preferred be-cause they provide better ventilation.Materials, such as thatch, tin sheets orRCC slabs are used for roofing.
Latrine Design CriteriaAlthough a range of sanitary latrinetechnology options is adopted and pro-moted in Bangladesh, the design crite-rion summarized below is among thesimplest. Most people can follow thestandards but need periodic reminders todig the pit at least 2 metres deep.
Platform:RCC slab: round shape, 1 metre di-
ameterRCC slab: square shape, 1 metre x 1
metre
Bamboo/timber or compacted mudplatform: square shape, 1 metre x1 metre
Pit:Diameter: l metre, round shapeDepth: at least 2 metres deep with
smaller diameter at the pit bottomif not lined.
Cost of Sanitary LatrineThe average cost of a concrete slabwaterseal latrine including a simple su-perstructure is Taka 200 (US$ 5) toTaka 500 (US$ 12.5) depending on thenumber of concrete rings (1 to 5) usedfor the pit lining. A do-it-yourself home-made latrine costs Taka 100 (US$ 2.5)or less and can be constructed at no costif local materials such as bamboo andtree branches are used.
The cost of one RCC slab withwaterseal pan and one concrete ring (12in. height) sold by a private producer ison average Taka 150 (US$ 3.75). Theaverage cost of one concrete ring isTaka 60 (US$ 1.5) from private produc-ers, while the cost of one burnt clay ring(6 in. high) is Taka 10–15 (US$ 0.25–0.375) from the private potters.
continued on page 19
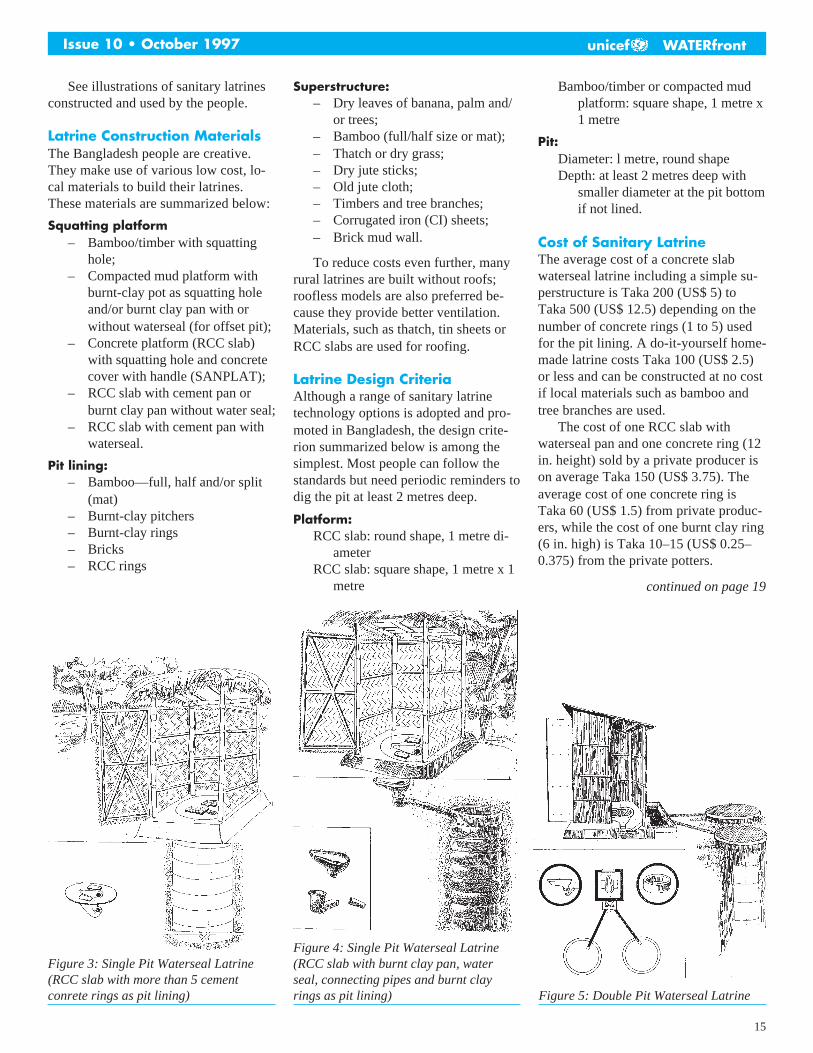
Figure 3: Single Pit Waterseal Latrine(RCC slab with more than 5 cementconrete rings as pit lining)
Figure 4: Single Pit Waterseal Latrine(RCC slab with burnt clay pan, waterseal, connecting pipes and burnt clayrings as pit lining) Figure 5: Double Pit Waterseal Latrine
16
Issue 10 • October 1997unicef WATERfront
Sanitation Promotionthrough Community BasedOrganizations: the BabuzaiExperience, NWFPBy Rajen K. Sharma, formerly Project Officer, UNICEF, Peshawar
In Pakistan, 67% of the total population stilldoes not have access to adequate sanitation1
facilities. Although efforts to improve thesituation are steadily increasing, they arelimited to a few schemes carried out byspecific government agencies and NGOs.Their impact on increasing coverage isnegligible. To bring significant improvementin a reasonable period, more and more“actors” must be involved in mass sanitationpromotion. These actors could include localNGOS, Community Organizations, villagebased social groups, school teachers andstudents. This paper describes how an activeCommunity Based Organization (CBO) wasmobilised to initiate village sanitationimprovement on a self-help basis. Although itmay be early to claim it as a significantachievement, keeping in mind the limitedefforts made to mobilise & support the CBO,the modest achievement of motivating a fewtrendsetting households to build their ownlatrines is quite encouraging.
IntroductionSituated on the foothills of the KatlangRoad, 55 kilometres from Mardan,Babuzai is a village of approximatelyone thousand households. Under thePAK-German Integrated Rural Develop-ment Programme (IRDP), a communitybased organization by the name of“SABA” was formed as part of villageinstitution building to promote self-helpinitiatives in the field of basic develop-ment and income generation. With theassistance of UMP, SABA contributeddirectly to the improvement of the com-munities’ living conditions through avariety of self-initiated projects.
Mobilization PhaseIn January 1994, members of SABA ap-proached UNICEF to support the con-struction of household latrines in thevillage. They expected a level of supportsimilar to the material support providedunder the UNICEF-assisted programmewith Local Government & Rural Devel-opment Department (LG&RDD). Rec-ognizing that the community of Babuzaihad already carried out various projectson a self-help basis, UNICEF encour-aged the CBO to mobilise the commu-nity to improve sanitation. Appreciatingthe organization’s previous efforts, itwas brought to their attention that thecommunity had solved a major problemlike water supply themselves. Therefore,if they felt the need for it, they couldbuild household latrines. Assurance wasgiven to the CBO members that if theywere ready, UNICEF would help themin creating awareness among the com-munities, demonstrating the technologyand providing technical support in la-trine construction. The following ap-proach was suggested:
■ The initial step would be to haveSABA members understand thatpeople can build their own householdlatrines according to their capacity ifthey feel the need for it and are con-vinced that they can be built cheaply.
■ UNICEF would then help createawareness by explaining in commu-nity meetings about the linkage ofpoor sanitation and disease and theimportance, especially for the pri-vacy and convenience of females, ofhaving a household latrine.
■ UNICEF would also coordinate with
LG&RDD the construction of a dem-onstration latrine in the village to fa-miliarize people with the lowcostoptions available.
■ LG&RDD would provide an initialmaterial support grant (sanitary pan& PVC pipes) for a limited numberof latrine units to enable the CBO tostart work. The CBO would sell thematerials to those motivated to buildlatrines.
■ The funds generated from the saleswould form a revolving fund enablingthe purchase of more materials fromthe market and supporting the con-struction of additional latrines.
■ Members of the CBO without la-trines would build first, setting an ex-ample for others.
■ Finally, CBO members would fol-low-up with the people in their areasregarding the construction and useof household latrines and present aprogress report in their regularmeetings.
Implementation PhaseInitially, the members of the CBO hesi-tated to motivate their people to buildlatrines without financial support froman external agency. They believed thatbuilding latrines would be expensiveand people lacked the ability to con-struct them. However, after discussionswith UNICEF and giving the mattercareful consideration, the members wereconvinced that it is the responsibility ofevery individual to improve his/herhousehold sanitation. After a 3–4 monthperiod, they agreed to start the work intheir village.
The process started with communitymeetings held in mosques and the CBOoffice. UNICEF, through LG&RDD,supported the CBO by explaining thelinkage of poor sanitation and diseaseand the importance of providing privacy& convenience in open defecation. In-formation on lowcost latrine technologywas also provided.
A one time grant of 100 sanitary Pan& PVC pipes was provided by the dis-
1Sanitation in this paper is defined as thesafe disposal of human excreta throughappropriate sanitary latrines. continued on page 19

17
Issue 10 • October 1997 unicef WATERfront
relatively even geographic distributionand the ability of the community to or-ganize and contribute to schoolprogrammes. Since the programme alsoaimed at the promotion of a sanitationconcept in the rural community, the ap-proach was designed with community-based initiatives. A series of meetingswas conducted with the community or-ganization, which consisted of villageleaders, Village Development commit-tees (VDCs), Parent-Teacher Associa-tions (PTAs), Cluster SchoolConstruction Committees and school di-rectors and teachers. A formal contractwas signed among all parties before theschool/community-based health educa-tion and latrine construction were started.
Development and use ofeducational materialsThe education package included healtheducation to promote the understandingof the importance of the latrines amongbeneficiaries, and organizational assis-tance to ensure long-term maintenanceand cleaning of the installations. Avideo documentary was produced underthe title of “Let’s Talk About HygienicLatrines” and a training module andeducation materials (lesson plans, gameboards, posters, sketch books) were pre-pared in Khmer (Cambodian language)in cooperation with UNICEF, NGOsand government counterparts. The
school teachers were given intensivetraining to enable them to educate thestudents and community.
During the pilot phase, 60 latrineunits were completed at five core and 11satellite primary schools in the nineschool clusters. About 70 teachers weretrained in health, hygiene and caringpractices and 5,030 students received hy-giene education training. Hygiene educa-tion lessons were integrated into thecurricula for testing. At the central level,an inter-ministerial committee with rep-resentatives from the Ministries of Edu-cation, Health and Rural Developmentwas created to prepare lessons to be inte-grated into the curricula development.
During the project, the latrines pro-vided the forum for the communityhealth education initiatives. Most stu-dents, teachers and community memberswere closely involved in the construc-tion of latrines and in education ses-sions. Field reports mentioned thatmany villagers regularly observed theconstruction and discussed constructiontechniques and the operation of the sep-tic system. Community Health Educa-tion workers also explained the basicbiological process involved in excretadisposal. Communities were informedabout the dangers of ground water pol-lution caused by the nonseptic “soak-age” pit latrine.
Ground water pollution was traced
to the releasing of contaminants fromthe pit latrine design.
Though this was not necessarilybad, potential risks were foreseenwhich could converge and create poorsanitary conditions. Therefore theoriginal pit latrine design, which em-ployed septic tanks and a leach field,was modified. A septic tank, entirelysealed with the exception of a smallpipe to emit methane gas and a largerpipe to discharge excess waste waterinto a leach field, was built. This modi-fication made the latrine cost 28%higher than the original design. Furthermodifications are under considerationto produce a lowcost design.
The intention of the project is thatthrough the school children, communi-ties would adopt improved hygienepractices and positive behaviouralchanges. Therefore a participatorymonitoring system was developed andtesting is taking place in the targetedschools. Since the school latrine con-structions were only recently com-pleted, it is too early to measure theirsocial and health impact. However,some communities have already re-sponded positively, particularly in theirdesire for new latrine construction. Thepilot phase has had a good beginning;the technical lessons and social compo-nent development are being dissemi-nated to other community andschool-based integrated WATSANprogrammes in Cambodia.
■ Sarasa, from page 13
continued on page 19
took place from 25 February to 8 March1997. As in previous phases, six villagesin two subdistricts were targeted. Santrisfrom the local pesantrens held a series ofevening community gatherings wherediscussions on religious matters and theimportance of hygienic behaviour tookplace. The “Water, Cleanliness andHealth According to Islamic Teachings”Handbook published under the UNICEF-MUI (Council of Islamic Scholars) Co-operation was used extensively in theseactivities.
During the day, the santris, who hadreceived prior training on the use of
FRP molds from provincial PublicWorks officers, helped families to con-struct or repair their RAKSA facilities.The “stimulant approach” was adoptedunder which the government providedfunds for procurement of cement andother non-local materials while the re-maining costs, including labour, werecontributed by the communities. Whilethe first two phases were dominated bymale santris, more female santris havebecome actively involved, not only inprayer meetings with the women’sgroups but also in construction activities.
The five phases of SARASA inBandung had the following measurable
results: 2489 new family latrines, 81public latrines, five school latrines, sixspring protection schemes, 300 dugwells and approximately 1000 refinedhouses with plastered floors, improvedventilation and separate animal pens.Each phase has reportedly managed toincrease latrine coverage in the targetedvillages from 10 to 30%. However,with starting levels as low as 9% insome villages, intensive follow-up ac-tivities have to be carried out to ensurethat the programme meets its objec-tives. The GJB principles promote on-
■ Sanitation through Schools: Experience in Cambodia, from page 13
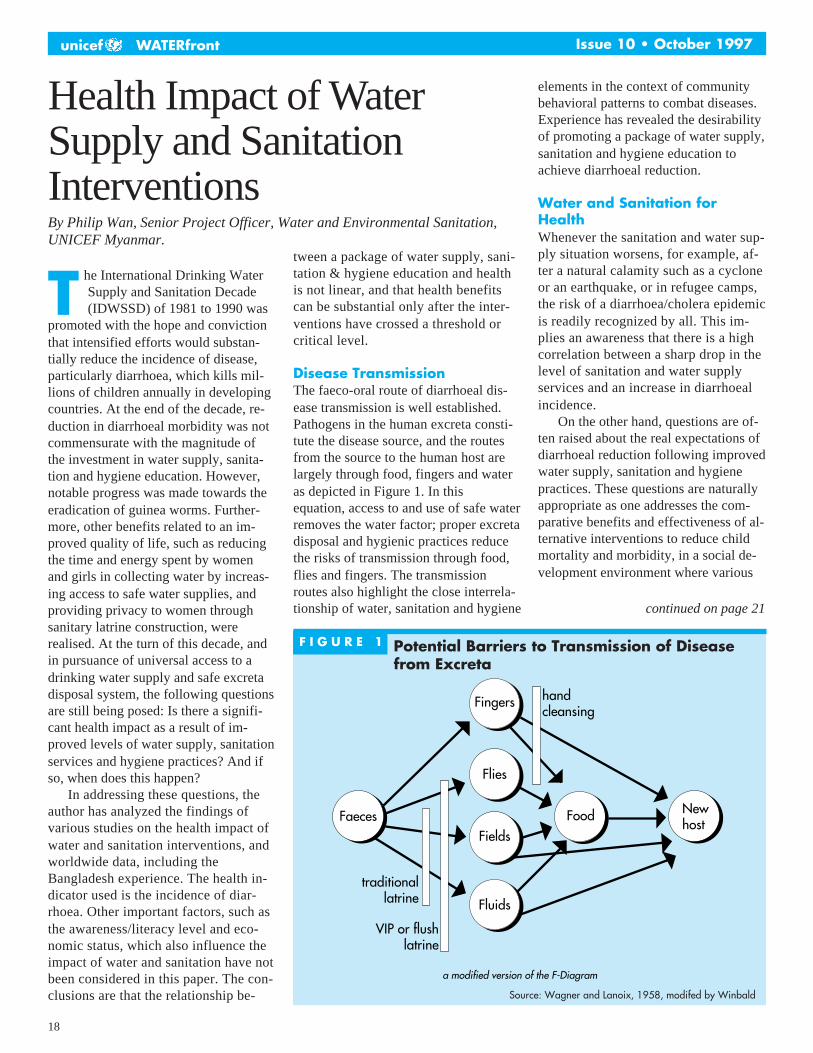
18
Issue 10 • October 1997unicef WATERfront
Health Impact of WaterSupply and SanitationInterventionsBy Philip Wan, Senior Project Officer, Water and Environmental Sanitation,UNICEF Myanmar.
he International Drinking WaterSupply and Sanitation Decade(IDWSSD) of 1981 to 1990 was
promoted with the hope and convictionthat intensified efforts would substan-tially reduce the incidence of disease,particularly diarrhoea, which kills mil-lions of children annually in developingcountries. At the end of the decade, re-duction in diarrhoeal morbidity was notcommensurate with the magnitude ofthe investment in water supply, sanita-tion and hygiene education. However,notable progress was made towards theeradication of guinea worms. Further-more, other benefits related to an im-proved quality of life, such as reducingthe time and energy spent by womenand girls in collecting water by increas-ing access to safe water supplies, andproviding privacy to women throughsanitary latrine construction, wererealised. At the turn of this decade, andin pursuance of universal access to adrinking water supply and safe excretadisposal system, the following questionsare still being posed: Is there a signifi-cant health impact as a result of im-proved levels of water supply, sanitationservices and hygiene practices? And ifso, when does this happen?
In addressing these questions, theauthor has analyzed the findings ofvarious studies on the health impact ofwater and sanitation interventions, andworldwide data, including theBangladesh experience. The health in-dicator used is the incidence of diar-rhoea. Other important factors, such asthe awareness/literacy level and eco-nomic status, which also influence theimpact of water and sanitation have notbeen considered in this paper. The con-clusions are that the relationship be-
tween a package of water supply, sani-tation & hygiene education and healthis not linear, and that health benefitscan be substantial only after the inter-ventions have crossed a threshold orcritical level.
Disease TransmissionThe faeco-oral route of diarrhoeal dis-ease transmission is well established.Pathogens in the human excreta consti-tute the disease source, and the routesfrom the source to the human host arelargely through food, fingers and wateras depicted in Figure 1. In thisequation, access to and use of safe waterremoves the water factor; proper excretadisposal and hygienic practices reducethe risks of transmission through food,flies and fingers. The transmissionroutes also highlight the close interrela-tionship of water, sanitation and hygiene
elements in the context of communitybehavioral patterns to combat diseases.Experience has revealed the desirabilityof promoting a package of water supply,sanitation and hygiene education toachieve diarrhoeal reduction.
Water and Sanitation forHealthWhenever the sanitation and water sup-ply situation worsens, for example, af-ter a natural calamity such as a cycloneor an earthquake, or in refugee camps,the risk of a diarrhoea/cholera epidemicis readily recognized by all. This im-plies an awareness that there is a highcorrelation between a sharp drop in thelevel of sanitation and water supplyservices and an increase in diarrhoealincidence.
On the other hand, questions are of-ten raised about the real expectations ofdiarrhoeal reduction following improvedwater supply, sanitation and hygienepractices. These questions are naturallyappropriate as one addresses the com-parative benefits and effectiveness of al-ternative interventions to reduce childmortality and morbidity, in a social de-velopment environment where various
T
F I G U R E ␣ 1 Potential Barriers to Transmission of Diseasefrom Excreta
a modified version of the F-Diagram
Fingers handcleansing
Newhost
FoodFields
Flies
Fluids
Faeces
traditionallatrine
VIP or flushlatrine
Source: Wagner and Lanoix, 1958, modifed by Winbald
continued on page 21

19
Issue 10 • October 1997 unicef WATERfront
trict office of LG&RDD, Mardan togive momentum to the work. Local ma-sons were provided with technicalknowledge of the simple twin-pit pourflush latrines that the programme pro-moted. During the training of masons,other interested villagers were trained inthe technology.
The initial construction of a few la-trines by some highly motivated peoplecreated interest among others for house-hold latrines. Slowly people startedcoming to the CBO members to buy thelatrine materials provided by LG&RDD.In a period of 10–11 months, 96 house-holds built latrines and a fund ofRs.26000 was generated through thesale of the materials. More important,construction of these 96 latrines on aself-help basis influenced 76 otherhouseholds to build their own latrinesby purchasing materials from the mar-ket. This replication can be attributed tothe fact that people were using their ownresources to construct latrines; no finan-cial support was provided by any out-
side agency.At the time of writing this report,
SABA is continuing its effort to im-prove the sanitation situation in the vil-lage without any outside support. Theyhave purchased latrine materials fromthe local market using the funds gener-ated from the sale of materials and havehelped others to build their latrines.Realising the need to have proper sani-tary facilities in the schools, they con-structed four latrines within the schoolpremises using the generated fund.
Finally and most important, the ef-forts made by SABA have played acatalytic role in the village. People areslowly building their latrines by pur-chasing materials from the market andnot waiting for SABA to help. Increasesin the sale of latrine materials have beennoted in the local shops in Babuzai.
Let us hope a day will come whenevery house in Babuzai will have itsown latrine so people will not have tosearch for already scarce privacy foropen defecation!
■ Low Cost Latrine Technology Options, Bangladesh, from page 17
■ Sarasa, from page 17
going community activities, ideallyweekly, towards achieving clean andhealthy living environments. A gather-ing of all santris participating inSARASA activities in Bandung was re-cently conducted to share experiencesand discuss efforts to ensure commu-nity follow-up actions.
The Impact.An evaluation has yet to be conducted ofSARASA activities to assess the effec-tiveness of mobilising community re-sources in improving the WES situationor the Project’s impact on institutional-izing healthy living behaviour. The pro-vincial Government has invited threemajor universities in the province, theInstitute for People’s Welfare, theSchool of Government Administrationand the Parahyangan Catholic Univer-sity, to conduct an in-depth study of theimpact of SARASA.
As far as quantifiable results areconcerned, it has been reported that withSARASA activities taking place in allWest Java districts, the province man-aged to build almost 100,000 family la-trines during the 1996/97 financial year,an impressive increase of 233% over theprevious year. In view of the 700,000units required per year to meet the targetof universal coverage, greater effortswill need to be made to ensure that thecommunities follow-up on the SARASAactivities.
The provincial government is com-mitted to at least meeting the RepelitaVI (the current five-year developmentplan ending in March 1999) target of60% sanitation coverage. As stated byMrs. Neni Suhaeni, Head of the Provin-cial Health Education Centre, under theleadership of Governor R. Nuriana, whohas a very strong commitment to im-proving the people’s health standard andactually invented the name SARASA,the West Java province is confident thatthe target will be met.
Operation and Maintenance ofLatrineThe routine maintenance of the latrine isdone by family members. However,when the pit is filled, most latrine userfamilies employ cleaner/sweepers toempty the pit. Often the excreta are bur-ied into another pit, is covered withearth and the latrine is used again.
Constraints encountered are summa-rized below:
1. Lack of space for shifting latrine to anew pit.
2. Building a new latrine when the pit isfilled is not cost-effective.
3. Cleaner/sweeper is not always avail-able.
4. Unlined pits collapse due to highground water table in some places orafter heavy rains.
5. Soil deposited from rat-holes accel-erates the filling up of pits.
References:1 Bangladesh Bureau of Statistics, Min-istry of Planning (1994) ProgotirPathey.2 Associates for Community and Popula-tion Research (1993) Needs Assessmentfor the Sanitation Programme, DPHE-UNICEF, Bangladesh3 WHO/DPHE/UNICEF (1994) Study toAssess the Impact of Social Mobiliza-tion Campaign for Sanitation on the Pri-vate Sector.4 House of Consultant (1994) NationalSurvey on Latrine Producers and MarketSituation in Bangladesh, DPHE-UNICEF.5 DPHE/UNICEF (1994) National Sur-vey of Sanitary Technology,Bangladesh.
■ Sanitation Promotion: The Babuzai Experience , from page 16

20
Issue 10 • October 1997unicef WATERfront
Women Benefit fromIntensive Sanitation inVietnamBy Binoy Kumar Das, formerly Project Officer, Sanitation,UNICEF Hanoi, Vietnam
and completed it in four years. Theproject was designed for Quynh PhuDistrict comprising 39 communes(population 232,000, HHs 39,000). Itwas based on the principle of self-help,without subsidies, but with particular at-tention paid to the women and girls ineach household. A loan component wasadded for income generation, leading tothe construction of sanitary facilitiesboth for the poorest families and forfamilies owning their own tubewells.With the assistance of community asso-ciations, particularly the Women’sUnion, Youth Union and the CommunePeople’s Committees (CPCs), manyprograms were promoted, for example,household hygiene education, safe stor-age and handling of food and water, im-provement of animal sheds and safedisposal of animal dung. It also encour-aged vector control (using biologicalmethods such as special kinds of smallfish, fly traps, etc., to destroy dengue fe-ver larvae in household water storagetanks), installing lowcost household wa-ter treatment units and large scale use ofsmokeless chulas (stoves). Enthusiasmwas so great for mobilizing people’sparticipation that CPCs offered the poorfamilies a few kg. of rice from their own
funds against the construction of eachtype of household sanitary facility. AnVinh commune and the WATSAN Ref-erence Centre of Medical College, ThaiBinh, took the lead.
In the same district, the Women’sUnion started the Women in Develop-ment Project to especially benefitwomen and children. Included in theproject were loans for income genera-tion programs for poor families usingthe VAC system (Vegetable, Aquacul-ture and Cage), dissemination of knowl-edge on “Facts for Life” from family tofamily, and provision of soya bean milkfor children in creches/kindergartens toeliminate malnutrition.
The net result of the District’s Inten-sive Sanitation Project and the Women inDevelopment Project (assisted byUNICEF), are the smiles on the faces ofthe women in the 39 communes. Ask awoman. She will relate the benefits shereceived from the package of sanitary fa-cilities in her house, how comfortableand economic the smokeless chula is, andwhat she gained from the VAC system.She knows the facts for life and can tellwhen the baby needs breastfeeding and,of course, the benefits of handwashingwith soap. The women can tell the cost ofeach sanitary facility, how it was ob-tained and how easy it is to build.
I was quite surprised when, on 16March 1995, I visited Quang Tho Com-mune in Thanh Hoa Province - far awayfrom Thai Binh Province. This com-mune has not received any support fromUNICEF yet. Ms. Ngo, the Chairpersonof the Commune People’s Committee,sent a team from the commune to ThaiBinh at CPC’s expense to study the In-tensive Sanitation Project. When theteam returned, the CPC became very en-thusiastic. They sold some of their oldiron junk and arranged a revolving fundto give loans to families to constructhousehold sanitary facilities. One teammember, who was especially motivated,was the Chairperson of the commune’sCommunist Party. Upon his return, hebuilt a costly, tiled-wall water seal la-trine with water storage and pumping inhis house, at his own expense. His
he people in Vietnam, particularlyin the North and Central prov-inces, traditionally use human ex-
creta as fertilizer. Since 1960, thegovernment has encouraged the use ofthe double vault compost latrine forcomposting human excreta for aboutthree months before use in the field. Thiswas, however, not adopted by the peoplemostly due to the dearth of fertilizer. Itwas common to use even raw night soiland urine in the field. As a result, basedon a survey conducted in 1990, 95% ofthe people in the North were infectedwith intestinal parasites. In 1988, waterseal latrines were promoted as an alterna-tive, but acceptance and expansion ofthat system were also poor. Mainly be-cause the implementors and advocatesthemselves, the officials from the Minis-try of Health and the Provincial HealthDepartments, needed additional orienta-tion to change their outlook towards bet-ter sanitation and hygienic practices.
Officials of the Ministry of Healthand the Provincial Health Services ofVietnam visited Medinipur, India in De-cember 1991, to study its IntensiveSanitation Project. After the visit, ateam member from Thai Binh Province,started a similar project in one district
T
1 The Intensive Sanitation Project began September 1989 in the Medinipur District of WestBengal State (India). It covered a population of 6.74 million (1.09 million households) in10,468 villages, the single largest sanitation project in India. It was designed to run on a self-sustaining basis, without subsidy, to benefit primarily the women and girls. Safe latrines,bathing/urinal platforms, soakage pits, garbage pits, smokeless chulas (stoves) were the maincomponents of the household sanitary package.The project is a success due to the selfless service of the NGO implementors, the RamaKrishna Mission Lok Siksha Parisad (RKMLP) and the cluster organizations of the village youthclubs, who launched a massive and aggressive house to house campaign. Girls were evenadvised not to marry a boy who does not have a latrine and bathroom. Club members andsome rich people purchased latrine pans and slabs on their own to give to the poor familieson loan. Now in many villages in Medinipur, 100% of the families possess safe latrines.Women and girls enjoy pride, privacy, convenience and comfort. continued on page 24
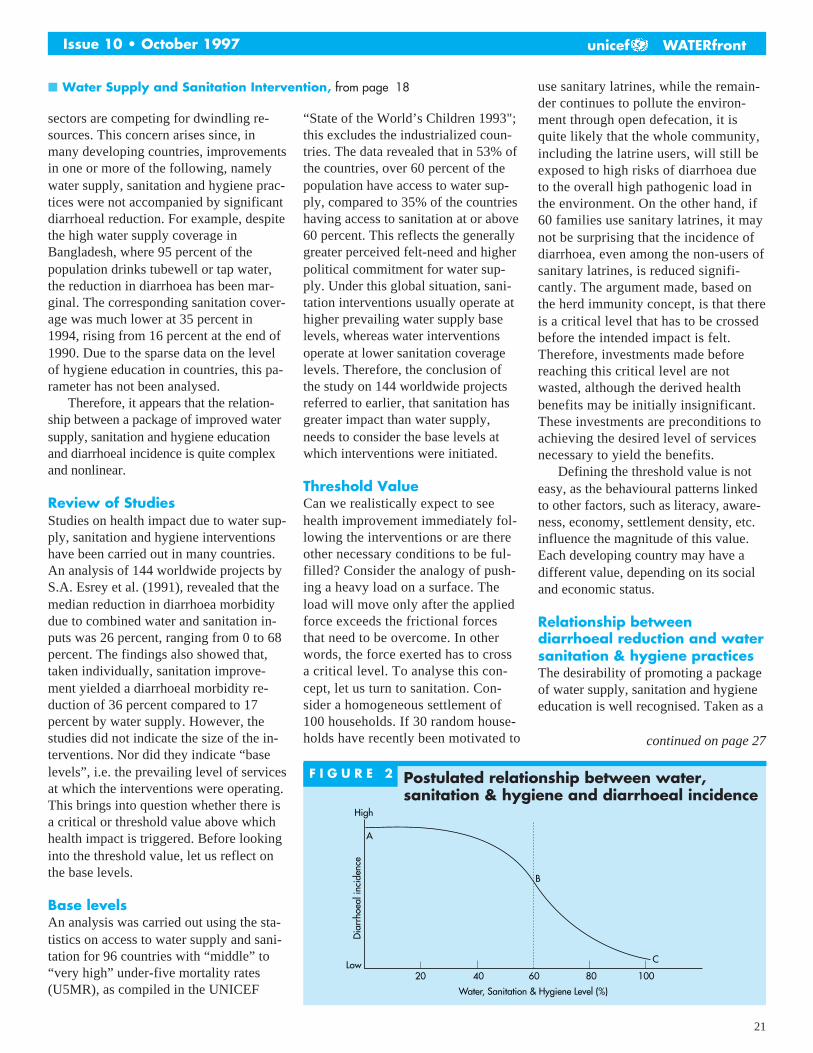
21
Issue 10 • October 1997 unicef WATERfront
sectors are competing for dwindling re-sources. This concern arises since, inmany developing countries, improvementsin one or more of the following, namelywater supply, sanitation and hygiene prac-tices were not accompanied by significantdiarrhoeal reduction. For example, despitethe high water supply coverage inBangladesh, where 95 percent of thepopulation drinks tubewell or tap water,the reduction in diarrhoea has been mar-ginal. The corresponding sanitation cover-age was much lower at 35 percent in1994, rising from 16 percent at the end of1990. Due to the sparse data on the levelof hygiene education in countries, this pa-rameter has not been analysed.
Therefore, it appears that the relation-ship between a package of improved watersupply, sanitation and hygiene educationand diarrhoeal incidence is quite complexand nonlinear.
Review of StudiesStudies on health impact due to water sup-ply, sanitation and hygiene interventionshave been carried out in many countries.An analysis of 144 worldwide projects byS.A. Esrey et al. (1991), revealed that themedian reduction in diarrhoea morbiditydue to combined water and sanitation in-puts was 26 percent, ranging from 0 to 68percent. The findings also showed that,taken individually, sanitation improve-ment yielded a diarrhoeal morbidity re-duction of 36 percent compared to 17percent by water supply. However, thestudies did not indicate the size of the in-terventions. Nor did they indicate “baselevels”, i.e. the prevailing level of servicesat which the interventions were operating.This brings into question whether there isa critical or threshold value above whichhealth impact is triggered. Before lookinginto the threshold value, let us reflect onthe base levels.
Base levelsAn analysis was carried out using the sta-tistics on access to water supply and sani-tation for 96 countries with “middle” to“very high” under-five mortality rates(U5MR), as compiled in the UNICEF
“State of the World’s Children 1993";this excludes the industrialized coun-tries. The data revealed that in 53% ofthe countries, over 60 percent of thepopulation have access to water sup-ply, compared to 35% of the countrieshaving access to sanitation at or above60 percent. This reflects the generallygreater perceived felt-need and higherpolitical commitment for water sup-ply. Under this global situation, sani-tation interventions usually operate athigher prevailing water supply baselevels, whereas water interventionsoperate at lower sanitation coveragelevels. Therefore, the conclusion ofthe study on 144 worldwide projectsreferred to earlier, that sanitation hasgreater impact than water supply,needs to consider the base levels atwhich interventions were initiated.
Threshold ValueCan we realistically expect to seehealth improvement immediately fol-lowing the interventions or are thereother necessary conditions to be ful-filled? Consider the analogy of push-ing a heavy load on a surface. Theload will move only after the appliedforce exceeds the frictional forcesthat need to be overcome. In otherwords, the force exerted has to crossa critical level. To analyse this con-cept, let us turn to sanitation. Con-sider a homogeneous settlement of100 households. If 30 random house-holds have recently been motivated to
use sanitary latrines, while the remain-der continues to pollute the environ-ment through open defecation, it isquite likely that the whole community,including the latrine users, will still beexposed to high risks of diarrhoea dueto the overall high pathogenic load inthe environment. On the other hand, if60 families use sanitary latrines, it maynot be surprising that the incidence ofdiarrhoea, even among the non-users ofsanitary latrines, is reduced signifi-cantly. The argument made, based onthe herd immunity concept, is that thereis a critical level that has to be crossedbefore the intended impact is felt.Therefore, investments made beforereaching this critical level are notwasted, although the derived healthbenefits may be initially insignificant.These investments are preconditions toachieving the desired level of servicesnecessary to yield the benefits.
Defining the threshold value is noteasy, as the behavioural patterns linkedto other factors, such as literacy, aware-ness, economy, settlement density, etc.influence the magnitude of this value.Each developing country may have adifferent value, depending on its socialand economic status.
Relationship betweendiarrhoeal reduction and watersanitation & hygiene practicesThe desirability of promoting a packageof water supply, sanitation and hygieneeducation is well recognised. Taken as a
continued on page 27
F I G U R E ␣ 2 Postulated relationship between water,sanitation & hygiene and diarrhoeal incidence
A
High
B
C
20Low
40 60 80 100
Dia
rrho
eal i
ncid
ence
Water, Sanitation & Hygiene Level (%)
■ Water Supply and Sanitation Intervention, from page 18
22
Issue 10 • October 1997unicef WATERfront
continued on page 24
The Mangochi HTNWorkshopMangochi, 17–21 March, 1997by Erich Baumann, SKAT, Switzerland
The Handpump TechnologyNetwork (HTN)Over 4 years ago in November, 1992, thelast international handpump workshop,sponsored by the UNDP/World BankWater and Sanitation Program, was heldin Kakamega, Kenya. The participantsdiscussed issues pertaining to VLOMhandpumps, maintenance strategies,manufacturing and drilling. Drawingupon India’s pioneering work in the field,the workshop placed considerable em-phasis on the promotion of low-cost wa-ter supply and sanitation technologies,including handpumps. The need for glo-bal co-ordination and collaboration be-tween governments, external supportagencies and other sector agencies wasemphasised, both to avoid duplication ofefforts and to ensure optimal utilisationof scarce resources. It overwhelminglymandated the formation of theHandpump Technology Network (HTN).
The HTN is a network open to allorganisations and individuals interestedin rural water supply who are ready tocontribute to the development of thesector. It has been functional since 1993on a small budget—funded largely bythe Swiss Agency for Development andCooperation (SDC). SKAT, located inSt. Gallen, Switzerland provides profes-sional support and runs the secretariat.Since 1995, an HTN Sector Professionalbased in UNICEF India office covers
mainly the Asia region. The current fo-cus of the network is on promoting thesustainability of handpump technolo-gies, in terms of both hardware and soft-ware issues. It has published a numberof documents, which have found wideacceptance and usage, initiated researchand provided assistance to several coun-tries on request. The organisation of theMangochi workshop was another impor-tant initiative taken by HTN.
The Mangochi WorkshopThe sector has made significant progressand many changes have taken placesince Kakamega. Handpumps continueto be the principal technology used inrural water supply. They are often themost cost-effective option for supplyinglow-income communities with safedrinking water. They are also environ-mentally friendly, relatively simple to op-erate, and manageable by the communityitself. However, maintenance of commu-nity handpumps is still a major problem.Many questions remain unanswered:How can the impact of investments inhandpump programmes be maximised?How can additional resources, especiallyat the local level, be mobilised? How canthe sustainability of water facilities beimproved? How can the different playerscooperate and interact?
Considering the need to draw to-gether experts from the field to share ex-periences and lessons learned, HTNconceived and planned the MangochiHandpump Workshop as a follow-up tothe Kakamega Workshop. It was hostedby the Government of Malawi andUNICEF Malawi under the auspices ofHTN, sponsored by SDC and UNICEF,NYHQ.
The workshop received an excellentresponse, over 150 participants from
nearly 40 countries with diverse experi-ence and expertise representing govern-ments, NGOs, the private sector, bilateraland multilateral agencies actively partici-pated and shared experiences. The work-shop provided an excellent opportunity toexchange information on an inter-re-gional basis, discuss issues affectingsustainability and make realistic recom-mendations for the sector policy. The lo-cation of the workshop, held on theshores of Lake Malawi, lent a positiveand stimulating atmosphere to the formaldaytime deliberations and facilitated aninformal and congenial interaction of theparticipants between the sessions.
The theme of the workshop “Partner-ship, Roles and Responsibilities” illus-trated that unless additional financial andnon-financial resources are mobilisedthrough user participation the goal of uni-versal access to safe water will not beachieved in the foreseeable future. Gov-ernment agencies, donors, advisors, andcommunity leaders have to recognise theprinciple that the local community itselfmust be the primary decision-maker inthe planning and up-keep of the waterpoints. With the changing role of govern-ments, the private sector has to play agreater role in service delivery.
The Workshop ObjectivesThe workshop had the goal:
■ To make recommendations on basicprinciples of implementation strate-gies related to technical, financialand institutional aspects which willpromote resource mobilisation, com-munity involvement, increased cov-erage and enhanced sustainability;
■ To adopt guidelines on technologychoice and standardisation;
■ To look for specific solutions in theAfrica Perspective, keeping in viewthe prevailing field situation in Af-rica, where most countries have dis-tinctly different conditions (industrialgrowth, technical manpower, marketdemand, availability of raw materi-als, groundwater quality, drilling ca-pacity etc.) when compared with
During his speech to inaugurate theHandpump Technology Network (HTN)Workshop in Mangochi, Malawi, the HonEdward Bwanali, Minister of Irrigation andWater Development, MP, highlighted theneed for a renewed impulse to serve thosewho were left behind. “It would be a criminalnegligence if we were not trying our utmostto bring safe water to our unserved ruralpopulation.”
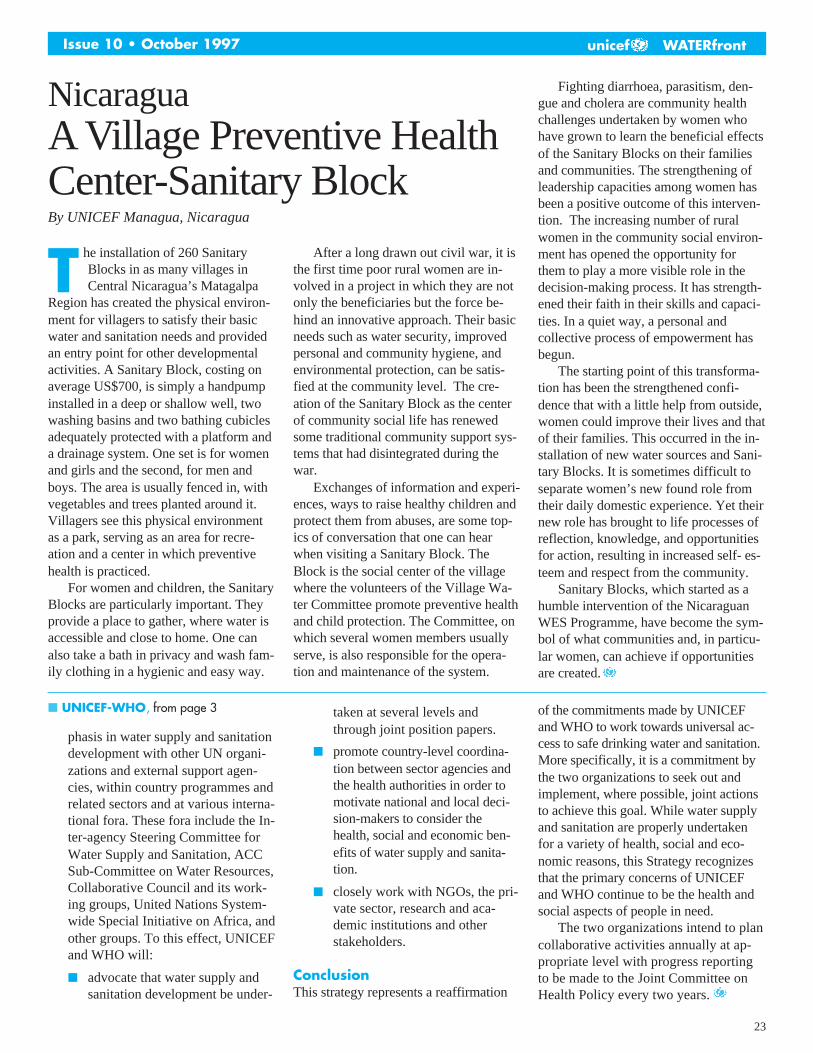
23
Issue 10 • October 1997 unicef WATERfront
NicaraguaA Village Preventive HealthCenter-Sanitary BlockBy UNICEF Managua, Nicaragua
he installation of 260 SanitaryBlocks in as many villages inCentral Nicaragua’s Matagalpa
Region has created the physical environ-ment for villagers to satisfy their basicwater and sanitation needs and providedan entry point for other developmentalactivities. A Sanitary Block, costing onaverage US$700, is simply a handpumpinstalled in a deep or shallow well, twowashing basins and two bathing cubiclesadequately protected with a platform anda drainage system. One set is for womenand girls and the second, for men andboys. The area is usually fenced in, withvegetables and trees planted around it.Villagers see this physical environmentas a park, serving as an area for recre-ation and a center in which preventivehealth is practiced.
For women and children, the SanitaryBlocks are particularly important. Theyprovide a place to gather, where water isaccessible and close to home. One canalso take a bath in privacy and wash fam-ily clothing in a hygienic and easy way.
After a long drawn out civil war, it isthe first time poor rural women are in-volved in a project in which they are notonly the beneficiaries but the force be-hind an innovative approach. Their basicneeds such as water security, improvedpersonal and community hygiene, andenvironmental protection, can be satis-fied at the community level. The cre-ation of the Sanitary Block as the centerof community social life has renewedsome traditional community support sys-tems that had disintegrated during thewar.
Exchanges of information and experi-ences, ways to raise healthy children andprotect them from abuses, are some top-ics of conversation that one can hearwhen visiting a Sanitary Block. TheBlock is the social center of the villagewhere the volunteers of the Village Wa-ter Committee promote preventive healthand child protection. The Committee, onwhich several women members usuallyserve, is also responsible for the opera-tion and maintenance of the system.
Fighting diarrhoea, parasitism, den-gue and cholera are community healthchallenges undertaken by women whohave grown to learn the beneficial effectsof the Sanitary Blocks on their familiesand communities. The strengthening ofleadership capacities among women hasbeen a positive outcome of this interven-tion. The increasing number of ruralwomen in the community social environ-ment has opened the opportunity forthem to play a more visible role in thedecision-making process. It has strength-ened their faith in their skills and capaci-ties. In a quiet way, a personal andcollective process of empowerment hasbegun.
The starting point of this transforma-tion has been the strengthened confi-dence that with a little help from outside,women could improve their lives and thatof their families. This occurred in the in-stallation of new water sources and Sani-tary Blocks. It is sometimes difficult toseparate women’s new found role fromtheir daily domestic experience. Yet theirnew role has brought to life processes ofreflection, knowledge, and opportunitiesfor action, resulting in increased self- es-teem and respect from the community.
Sanitary Blocks, which started as ahumble intervention of the NicaraguanWES Programme, have become the sym-bol of what communities and, in particu-lar women, can achieve if opportunitiesare created.
T
phasis in water supply and sanitationdevelopment with other UN organi-zations and external support agen-cies, within country programmes andrelated sectors and at various interna-tional fora. These fora include the In-ter-agency Steering Committee forWater Supply and Sanitation, ACCSub-Committee on Water Resources,Collaborative Council and its work-ing groups, United Nations System-wide Special Initiative on Africa, andother groups. To this effect, UNICEFand WHO will:
■ advocate that water supply andsanitation development be under-
taken at several levels andthrough joint position papers.
■ promote country-level coordina-tion between sector agencies andthe health authorities in order tomotivate national and local deci-sion-makers to consider thehealth, social and economic ben-efits of water supply and sanita-tion.
■ closely work with NGOs, the pri-vate sector, research and aca-demic institutions and otherstakeholders.
ConclusionThis strategy represents a reaffirmation
■ UNICEF-WHO, from page 3 of the commitments made by UNICEFand WHO to work towards universal ac-cess to safe drinking water and sanitation.More specifically, it is a commitment bythe two organizations to seek out andimplement, where possible, joint actionsto achieve this goal. While water supplyand sanitation are properly undertakenfor a variety of health, social and eco-nomic reasons, this Strategy recognizesthat the primary concerns of UNICEFand WHO continue to be the health andsocial aspects of people in need.
The two organizations intend to plancollaborative activities annually at ap-propriate level with progress reportingto be made to the Joint Committee onHealth Policy every two years.
24
Issue 10 • October 1997unicef WATERfront
daughter, a student in class IX at aboarding school inThanh Hoa City, theprovince capital, does not like living inthe boarding school because there are nosanitary latrines. She comes home asfrequently as possible with her friendsand classmates to enjoy the latrine, wa-ter facilities and clean environment inher house. Her friends enjoy it and,naturally, wish to have the same facili-ties in their own houses.
■ HTN Workshop, from page 22
developing countries in Asia.
■ To define HTN mandate and scope.
Key RecommendationsA brief summary of the results from theworkshop’s deliberations are listed be-low:
■ Changes in implementation strategiesare required to include: demanddriven approach, private sector basedservice delivery mechanism, costsharing by all stakeholders, capacitybuilding at all levels. With a corre-sponding change in the institutionalrole of the Governments—from aprovider of services to a facilitator;
■ Community management anddecentralisation of maintenance leadsto enhanced effectiveness and ac-countability;
■ User contribution is essential tomobilise additional resources;
■ The impact of investments can bemaximised by using appropriatetechnologies;
■ Standardisation renders significantbenefits;
■ An efficient service delivery can beachieved through decentralised pro-curement with the private sectorplaying the lead role, providing com-plete service delivery packages in-cluding production, supply of pumps,installation, training, spare parts sup-ply, repairs, and after sale services;
■ Support to R&D on public domainhandpumps should continue but beconfined to the fine-tuning of exist-ing pumps;
■ Drilling costs can be reduced byoptimising well design, adoption ofappropriate low cost drilling or dig-ging options;
■ HTN should expand its scope of ac-tivities beyond handpump based wa-ter supplies to include: operationalresearch, drilling and digging, envi-ronmental sanitation;
■ HTN should place more emphasis ondissemination of information.
Focus on AfricaThe workshop recommended focusingthe work on those regions where the needis the most pressing. In partnership withUNICEF, HTN intends to strengthen ef-forts in Africa by launching a CapacityBuilding Project. Funding is solicited toestablish a posting for a HTN Sector Pro-fessional (HSP) based in Africa. Within aregional framework of HTN partners theHSP will provide demand-based supportto sector agencies in the planning of de-mand driven implementation, private sec-tor based service delivery, andchangeover from centralised todecentralised maintenance.
The United Nations System-wideSpecial Initiative for Africa (UNSIA),has launched a new water strategy forAfrica that will co-ordinate the frag-mented efforts. The implementation ofthe new strategy will require substantialco-operation among all stakeholders. Inthis context, the HTN Capacity BuildingProject will help to avoid cross-purposesor duplication of each other’s efforts.
The Warm Heart of AfricaFor many of the delegates, theMangochi Workshop represented theirfirst opportunity to experience the ‘TheWarm Heart of Africa’. Malawi cer-tainly lived up to its reputation. TheUNICEF Malawi team headed by Ms.Nathalie Hahn and Christopher Zulu put
The Mangochi DeclarationThe Mangochi Workshop found thatalthough low-cost technologies are wellproven, and despite the existence ofmany examples of successful implemen-tation strategies, progress remains slow.In a declaration ratified during the finaldeliberations, the workshop proposedthat new impetus should be given to theglobal efforts in the sector. It pointed outthe need for a partnership-based ap-proach, including the creation of an ef-fective framework for co-ordination ofefforts and closer collaboration on aglobal scale.
so much hard work into the preparationand the organisation of the workshop.Even though it took place in a perfectsetting, the location presented at thesame time a logistic nightmare. The tire-less effort and the excellent supportfrom the UNICEF Malawi team createdthe pleasant atmosphere that helped tofind the consensus, which is reflected inthe Mangochi Declaration. It remainsnow our challenge to maintain the mo-mentum created by the workshop and toensure that the sense of co-operationand partnership continues in our com-mon endeavour to provide safe water tothose who are unserved.
An Infopage on the workshop can befound on the Internet: http:/www.skat.chThe full proceedings of the workshopwill be available in August 1997. Thosewho would like to receive a copy or whoare interested in further informationconcerning HTN please contact:
Mr Erich Baumann or Ms Catherine DiaSKAT, Vadianstrasse 42, CH-9000, StGallen, Switzerland. Phone: + (41) 71228 54 54. Fax: + (41) 71 228 54 55.E-mail: [email protected]
The United Nations System-wide Special Initiative for
Africa (UNSIA), has launcheda new water strategy for
Africa that will co-ordinatethe fragmented efforts.
■ Women Sanitation HealthBenefits, from page 20

25
Issue 10 • October 1997 unicef WATERfront
T
The Costing of Water andSanitation InvestmentExperience from GuatemalaOrlando Lugo, Senior Programme Coordinator UNICEF, GuatemalaJorge Mario Molina Water/Sanitation Programme Officer UNICEF, Guatemala
he Instituto de Fomento Munici-pal (INFOM), a Government ofGuatemala institution, adopted the
Unified Cost System for Water and Sani-tation (SUCAS) in March 1996, a systemdeveloped and used by UNICEF Guate-mala since 1993. A reform of the waterand sanitation sectors is underway and, islikely that INFOM will become the na-tional coordinator for those activities.
In Guatemala, the water supply andsanitation activities are managed by atotal of 330 municipalities, 12 NGOs,UNEPAR (Ministry of Health’s Execut-ing Unit for Rural Aqueducts), INFOM(National Institute for Municpal Sup-port), PAYSA (Water and SanitationProgramme for the Highlands), DSMEnvironmental Sanitation Division) andEMPAGUA (Guatemala City WaterCompany). Some smaller institutionsperform the same task. In addition, theSocial Investment Fund channels fundsfrom the World Bank and theInterAmerican Bank of Development toincrease coverage. All these bodieswork independently and lack a unifiedcost system. It is, therefore, difficult tocalculate the precise allocation of Gov-ernment funds for water and sanitationactivities.
It is estimated that the Governmentallocated 0.06 percent of the GDP in1996 for water and sanitation. Thisamount is lower than the 0.17 percentallocated in 1988. The NationalProgramme of Action, prepared by thePlanning Secretariat (SEGEPLAN), in-dicates that the end-decade goal is 82%for potable water and 82% for sanita-tion. Those estimates are based on apopulation of 8.3 million people. How-ever, according to the most recent cen-sus, the population of the country is 10
million. Some international agencies aredisputing the figures of the census, stat-ing that the real population figure is 11.2million. In any case, the coverage at theend of the century will be lower than ex-pected and the country will not achievethe goals for water and sanitation. Theabsence of a costing system, adds to theconstraints in obtaining the resourcesneeded to provide water to all the people.Cost is the missing element of the equa-tion to realistically plan end-decade goalsfor water and sanitation. This scenariorenders the goals for water and sanita-tion, a statement of good intentions.
Most cost analysis manuals or “mod-els” consist of a guide or checklist fordata collection. They are exhaustive andcomprehensive and identify data thatmay aid in calculating the total cost of awater supply system or a latrine, but arepractically impossible to obtain from theGovernment’s budgets. In contrast,SUCAS is straightforward, user-friendlyand simple. It is based on the collectionof information that is readily availablefrom three different levels: communityand municipal, regional and national. Inthis regard, the system considers pre-in-vestment, investment and costs, such asmanagement, administrative and techni-cal assistance. An important characteris-tic of this system is the participation ofthe community leaders, government of-ficials and NGOs. The application ofSUCAS involves three steps:organisation and training, collection ofdata and analysis.
The organization and training phaseincludes identifying the people who areworking on a specific project and hold-ing a national seminar to train themalong with senior staff During the semi-nar the principles of SUCAS, along with
the forms, are explained and discussedwith the participants. It is helpful toconduct an exercise to determine thecomprehensibility of the questions onthe form. If necessary, adjustments inthe questionnaires should be made.However, although the words can bechanged, the content of the questionsshould remain the same. During themeeting a work plan is prepared to fol-low up the application of the system.
In the second phase, data is collectedthrough four questionnaires, numberedone to four, administered at the three lev-els. The local committee or the watercouncil completes questionnaire one,which describes the community’s contri-bution, such as labor and materials or anypreliminary study that may have beenconducted. Questionnaire two is the re-sponsibility of the technician or health in-spector who supervises the projectlocally; information on the work of thetechnicians, masons or inspectors shouldbe included. Questionnaire three adds thecost of technical assistance and the super-visor to the information obtained throughthe first two questionnaires. The fourth isthe responsibility of the central level andconsists of a compilation of the data ofthe first three questionnaires plus admin-istrative costs (telephone, electricity, rent,vehicles, gasoline, etc.). This design en-sures that each questionnaire summarizesthe information from a lower level as ameans to consolidate the data and forquality control. Thus, the regional ques-tionnaires include data on the communityand municipal contributions and the na-tional questionnaire is a compilation ofthe available data at both the local and re-gional levels.
The third phase is the analysis of thedata using the computer programme de-veloped for this purpose. Upon request,the programme is distributed free ofcharge by the UNICEF Office in Guate-mala. The computer programme func-tions as a data bank and an instrument togenerate reports, and it allows the com-parison of each project among munici-palities or by the type of technologyused. The programme is flexible and can
continued on page 27

26
Issue 10 • October 1997unicef WATERfront
Reducing Pests and InsectVectorsby Michael Nathan & Annette Wiltshire1
n the Caribbean and Latin America,dengue is an important public healthproblem. The dengue virus is spread
by a mosquito, Aedes aegypti, whichbreeds in the water that collects in thewide variety of containers associatedwith everyday living.
There is no vaccine against dengue;prevention and control of the disease aredependent on taking measures againstthe mosquito vector. Central to these ef-forts is the involvement of communitiesin eliminating unwanted containers andmanaging others in ways that preventmosquitoes from breeding in them. Overthe past three years, 15 schools in Bar-bados, Dominica, Montserrat, St. Kitts& Nevis, and St. Lucia became involvedin the Dengue Prevention and ControlProgramme to foster young children’sawareness of and commitment to the im-provement of school, home and commu-nity environments.
Existing Health and Family LifeEducation programmes have been sup-ported by the development of action-ori-ented curricula designed to meet theidentified needs of the children, theirfamilies and communities. Teachers par-ticipated in the development of the cur-riculum and its implementation at three5 day workshops. This approach has en-abled the teaching to be infused intosubjects, such as Art, Music and Lan-guage and the regular science-basedsubjects, allowing for better use ofavailable time.
Children’s knowledge of environ-mental health issues has been enhanced,and their application of new skills andresponsibilities has led to major im-provements in the school environments.Acute littering problems have been suc-cessfully addressed as childrenrecognise the importance of keepingtheir surroundings clean and tidy. Atseveral schools the pupils separate theirgarbage at the point of disposal, e.g. intobiodegradables used for composting andapplication to vegetable and horticul-tural gardens; combustibles for on-siteincineration; and non-combustibles andplastics for reuse, or for pick-up by themunicipal authorities or burial, wherethere is no collection service. The ef-forts of one school in Barbados report-edly reduced the volume of garbage forcollection by over 90%.
Mosquito breeding sites on the schoolcompounds, such as old tires, plastic con-tainers and discarded tin cans, have beenvirtually eliminated with a simultaneousreduction in rodent and other pest prob-lems. Problems associated with stray ani-mals have been resolved in some schoolsby fencing the compounds or getting thehelp of the community to set up a watch,as has happened in Montserrat. This hasallowed the children to plant shade trees,grow decorative shrubs and flowers andcultivate vegetables. In Dominica, thesalad vegetables grown at Mahaut Schoolnow supplement the school feedingprogramme.
Through outreach activities, the chil-dren have carried the information andskills they learned at school into thewider community, directly through theirown actions and indirectly via familyand friends. Parent Teacher Associa-tions have also played an important rolein this process and, in some instances,interest and support from the local busi-ness sector has been forthcoming. In St.Kitts & Nevis, one school’s concern
over the health risks from an asbestosroof prompted the children to write tothe Minister of Health to lobby for theroofs replacement. This endeavorproved successful.
The provision of a nominal “start-up” grant for each school was dependenton their developing a programme of ac-tivities for the first year of what is now athree-year-old initiative. The seedmoney was made available through aCaribbean Dengue Prevention and Con-trol Project financed by the Governmentof Italy and managed by the Pan Ameri-can Health Organization. Any additionalinputs have been the result of theschools’ own efforts in mobilising re-sources from the wider community.
The school programme, though con-ceived in the context of a growing con-cern about dengue, was designed with amuch broader goal: fostering a sense ofpersonal and social responsibility, gain-ing a greater awareness of environmen-tal health issues; and acquiring the skillsneeded to act on the knowledge gainedabout health. The programme has re-cently expanded to schools in severalother islands of the English-speakingCaribbean.
I
1Michael NathanEntomologistOffice of CaribbeanProgram CoordinationPan American Health OrganizationP.O. Box 508 Bridgetown, Barbados
Annette WiltshireEducation Consultant2, Old Paddock Link RoadBlue Range, Diego Martin Trinidad
tation is obvious and initiatives like theSUCAS are very much welcomed. How-ever there is an apparent risk that suchsystems are created more in response todemands from donors than for increasedefficiency of the sector as a whole andthat input and reporting will be designedaccordingly. As an isolated attempt, dis-tinct from the country’s overall budget-ing, it also runs the risk of quicklybecoming obsolete and unsustainable.The institutional capacity needed to runand maintain the system needs to becarefully appraised before implementa-tion. Finally, the involvement of usersboth as providers of data and in theanalysis of data is essential from the cre-ation of a cost calculation system to en-sure its sustainability. The example ofGuatemala where the system now hasbeen adopted by the government mayprove to be a succesful one.
■ Cost Calculation from page 28

27
Issue 10 • October 1997 unicef WATERfront
■ Water Supply and Sanitation Intervention, from page 21
package, the author postulates that, insimple terms, the relationship betweenthe package intervention and diarrhoealreduction is expressed in the model dis-played in the graph of Figure 2.
The graph shows a nonlinear relationthat exhibits different steepness in theslope at different parts of the curve. Un-less the pathogen load ingested is re-duced substantially, the diarrhoealincidence will remain high. However, adramatic reduction in the incidence rateoccurs because of reduced pathogenload in the middle part of the curve. Thepathogen load in the environment ishigh in region A of the graph where theaccess to and use of the services is low.A sharp reduction in diarrhoeal inci-dence is likely to occur in region Bwhen the threshold value is crossed.
Another important feature of thenonlinear relationship is that a given in-cremental improvement need not yieldthe same magnitude of benefits. For ex-ample, a 20 percent improvement willproduce a substantial benefit, if the pre-vailing service level at the time of inter-vention is 50 percent, whereas, theimpact will be negligible if the same im-provement operated at a prevailing levelof 10 percent.
The proposed relationship can alsoexplain the wide range of impact from0 to 68 percent for water and sanitationinterventions, as revealed by the reviewof the 144 studies referred to earlier.The impact depends on the prevailingcondition and the size of the interven-tion.
Bangladesh ExperienceAgainst a background of high watersupply coverage, the significant increasein the use of sanitary latrines in recentyears combined with improvedhandwashing practices has raised expec-tations of substantial reductions in diar-rhoeal incidence. This has not beenrealised on a large scale. Earlier studiesin Mirzapur (Aziz, et al. 1990) haveshown that a package of water, sanita-tion and hygiene practices yields a diar-rhoeal reduction of about 25 percentover a period of two years.
In other project areas where sanita-tion coverage has reached 60 percentand above, e.g. in certain Thanas ofBarisal District, people have claimed asubstantial reduction in diarrhoeal inci-dence. A study is underway in Barisal toscientifically assess the health impact ofthe sanitation and hygiene interventions.
Based on the proposed model de-picted in Figure 2, the use of sanitary la-trines and hygiene practices need toreach a higher level, probably around 60to 70 percent, before the health impactcan be triggered.
Therefore, the strategy currently pro-moted by UNICEF in support of theGovernment programme is to adopt anAccelerated District Approach toachieve and sustain high sanitation andhygiene coverage through intensive so-cial mobilisation efforts in each District.The sanitation coverage has increasedsignificantly from about 20 percent in1990 to 41 percent nationally in early1995 (BBS, 1995).
ConclusionThe positive impact of water supply,sanitation and hygiene education, as anintegrated package, on diarrhoeal diseaseis supported by various field studies andaetiological consideration. Studies havealso pointed to improvements in nutri-tional status. However, it is postulatedthat the health impact of the interventionsis governed by the magnitude of the in-terventions and the prevailing servicelevels. The interventions need to be sub-stantial enough and cross a thresholdlevel to realise significant health impact.Therefore, initial investments in the sec-tor should not be considered as ineffec-tive from a health status consideration,but instead, as vital building blocks forcrossing the threshold level.
References:
1. Aziz, K.M.A, et al. “Water Supply,Sanitation and Hygiene Education:Report of a Health Impact Study inMirzapur, Bangladesh. UNDP/WorldBank, 1990.
2. Bangladesh Bureau of Statistics,“Progotir Pathey 1995”. March 1995.
3. Esrey, S.A. et al. “Effects of im-proved water supply and sanitationon ascaris, diarrhoea, dracunculiasis,hookworm infection, schistosomiasisand trachoma. “Bulletin of WHO”69(5):609-621. 1991.
4. UNICEF “State of the World’s Chil-dren”. 1993.
■ Costing of Water and Sanitation from page 27
be adapted to the local jargon.The experience of other countries in
applying the cost system indicates thatlocal jargon should be used when pre-paring the questionnaires. For example,in the Central America region, there aredifferent names for public taps. In ElSalvador, they are called “cantarero”while in Guatemala, “llave chorro.” InGuatemala the questionnaires are com-pleted by community leaders (question-
naire one), the masons or bricklayer(questionnaire two), the environmentalsanitation technician (questionnairethree), and the project supervisor(questionnaire four). In applying thesystem, it was observed that some com-munity contributions shot up unexpect-edly. A closer look at the situationrevealed that incentives were offered topeople in the community to reporttwice the labor they were contributing.
Another observation was that the dailywage reported by communities mayvary. Using standard criteria, such asthe minimum wage as a base line, mayaid in this situation. The training of allthe actors and participants has been thekey element for the successful imple-mentation of the system. Besides theseobservations, no problems in the use ofthe system have been observed. It isexpected that the experience of INFOMwill motivate other institutions in thecountry.
28
Issue 10 • October 1997unicef WATERfront
Cost Calculation:A manual for water and sanitationdeveloped by UNICEF GuatemalaKarin Metell, Assistant Programme Officer, UNICEF WES Section, New York
system for cost calculationSUCAS (Unified Cost Systemfor Water and Sanitation) and a
manual has been developed and pub-lished by the area office of UNICEF inGuatemala. The system may be appliedto the construction and use of a gravitywater supply system, a handpump watersystem or latrines. Although a system tocalculate costs does not solve the prob-lem of overall diminishing resources, itmay help to justify the right investmentsand to improve the cost-efficiency of in-vestments being made. Ideally a system-atic approach to calculate costs of waterand sanitation should:
■ enable a systematic calculation of allcosts that appear in the constructionof a project—pre-investment costs,investments, administrative costs andcosts for operation and maintenance.
■ constitute a tool for supervision andmonitoring
■ clarify and account for all contribu-tions from different parties
■ enable a comparison between differ-ent technologies and between differ-ent project components.
The manualThe cost-calculation system is presentedin the manual, which in rather detailpresents the different forms to be usedfor the three types of projects that it ap-plies to. The first section of the manualdescribes the forms, while the secondoutlines the types of reports that can begenerated using the software developedfor SUCAS.
The system distinguishes costs at dif-ferent stages of the project cycle and con-
solidates the costs, whether in cash orkind, attributed to the respective actors.Costs may arise from the purchase of ma-terial, labor (unpaid or paid) transport,fuel etc. The manual suggests that indi-rect costs should be calculated accordingto a proximate share of administrativeand overhead costs of the institutions in-volved. Benefits are consistently calcu-lated in terms of people who will benefitfrom the services provided. In that way itis possible to calculate not only the unitcost of an investment but also the costsper beneficiary.
The forms may be adapted for localuse and has been so in the case of CentralAmerica (see article in this issue). Institu-tions who already have a functioning sys-tem to calculate and monitor costs maycontinue to use it as a basis for the datawhich is required in the last form. Thelast form should however always remainthe same to allow comparison betweenprojects, institutions and even countries.
Difficulties and constraintsThe rationale for improving costing insocial sectors, including water and sani-
A
continued on page 26
UNICEF and World Bank join forces for Safe Waterand Environmental Sanitation in Africa UNICEF and the World Bank made a commitment to work to-gether to support the countries of Sub-Saharan Africa in their ef-forts to promote access to safe water, environmental sanitation,and hygiene education for the poor in rural and urban areas.
The Memorandum of Understanding (MOU) between the twoagencies was signed in Washington on 9 October 1997 by Mr.Sadig Rasheed, Director of UNICEF’s Programme Division andMr. Peter Watson, Sector Director, Infrastructure and Energy, Af-rica for the World Bank.
Over 250 million people—half of Africa’s population—arewithout access to safe drinking water and almost 300 million do nothave adequate sanitation. With the current rate of populationgrowth and extension of water and sanitation services, a “businessas usual approach” would result in over 500 million without waterand sanitation by the year 2020. Much of Sub-Saharan Africa isthreatened by growing water scarcity and deteriorating water qual-ity, increasing water costs as well as conflicts among users. The hu-man impact—especially on the poor and most particularly on
women and children—will be unprecedented, as will the environ-mental impacts in cities where almost half the population live.
Primary areas for collaboration between UNICEF and theWorld Bank under the MOU will be in the development and imple-mentation of water, environmental sanitation and hygiene educa-tion programmes in villages, small towns and poor urbanneighbourhoods and in extending sustainable services to the poor.
This is not the first time that UNICEF and the World Bank havecollaborated closely in this area. For example, in Benin, BurkinaFaso and Malawi the two organisations have worked together inthe preparation and implementation of water and sanitationprojects.
The scale of the challenge ahead, the need for innovative na-tional programmes and the complementary nature of the twoorganisations make collaboration an imperative if there is goingto be a serious effort to significantly improve the availability ofwater, sanitation and hygiene education to those that will not bereached by conventional services in the near future.