Embed Size (px)
Citation preview

NUMBER 15 • DECEMBER 2003
Issue Brief
Healthier Kansans through informed decisionsWWW.KHI.ORG
KANSAS
HEALTH
INSTITUTE
The Growth ofSpecialty Hospitals
in Kansas:What Effects Do
They Have onCommunity
Health Services?
Charles L. Betley, M.A.R.Andrew Allison, Ph.D.
This Issue Brief focuses on thegrowth of a new kind of healthcare facility that provides servicesin a particular specialty, such ascardiology or orthopedics, and thepotential impact on the health caresystem in a community.
There are nine specialty hospitalsin five communities across Kansas,more than one would expect basedon the nationwide total.
The rapid growth of specialtyhospitals is fueled by their prof-itability. The relative ease of estab-lishing new hospitals in Kansashas contributed to their dispropor-tionate growth here.
Specialty hospitals threaten therevenue base that general hospitalshave used to subsidize unprofitablehealth services such as 24-houremergency room care, intensive careunits, and care for the uninsured.
Specialty hospital claims of high-er quality services are intriguing,but have not yet been validated.
Policymakers may have toweigh their desire for innovationand market-based solutions againstthe threat that specialty hospitalspose to the community health ser-vices provided by general hospi-tals. Avoiding this trade-off mayrequire a more explicit source offunding for such services.
Results in Brief
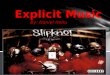
Specialty hospitals have appeared quickly in KansasSpecialty hospitals are expanding rapidly in Kansas and in many statesacross the country. As of December 2003, nine specialty hospitals wereoperating in five communities across the state (see map on page 3), a sur-prising proportion of the 100-or-so specialty hospitals nationwide. All but afew specialty hospitals are located in states like Kansas that have noCertificate of Need (CON) regulations, which require hospitals to obtainstate approval before building or expanding.
Profitability fuels the growth of specialty hospitals. Community generalhospitals that provide a full spectrum of services are most commonly orga-
What are specialty hospitals?
Specialty hospitals provideservices in a single medicalspecialty, such as cardiology ororthopedics.They can be dis-tinguished from other facilitiessuch as psychiatric, women’s,and children’s hospitals, whichprovide a broader range ofservices, and ambulatory sur-gical centers, which have fewinpatients and do not focus ona particular specialty.

2 KANSAS HEALTH INSTITUTE
nized as not-for-profit entities. Specialtyhospitals, on the other hand, are usuallyfor-profit firms, often with substantialinvestments by participating physicians.By focusing on procedures that offerhigher payments from insurers, specialtyhospitals are attractive to investors. Highpayments exist in part because Medicare,the federal health insurance program forthe aged and disabled and the predomi-nant payer for these types of procedures,may not be adjusting for changes in tech-nology which have lowered the costs ofservices. Although general hospitals arealso likely to be earning profits on theseservices, they have used these profits tocover the costs of unprofitable health careservices that benefit the community, suchas 24-hour emergency room care, inten-sive care units, and care for the uninsured.
Specialization and QualitySpecialty hospitals claim to offer highquality through newer facilities, betterequipment, and specialization. To besure, some patients will favor a new spe-cialty hospital’s amenities and location,but claims of higher quality care havenot yet been validated. New specialtyhospitals may have an opportunity toprovide newer technologies than existinghospitals. However, newer technologydoes not always lead to an improvementin quality, and general hospitals can
adopt these technologies as well. Specialty hospitals also claim higher
quality because of the notion that “prac-tice makes perfect.” Research confirmsthat experienced teams who frequentlyrepeat procedures become more profi-cient, but both general and specialty hos-pitals can benefit from high volumes ofprocedures. It is unclear whether special-ty hospitals’ narrow focus on a specificset of procedures will lead to higherpatient volume for these procedures ascompared to a community’s general hos-pitals. Moreover, even if higher volumedid lead to better quality at a particularspecialty hospital, the average quality ofcare in that community might decline ifthe newer hospital drew away cases thatthe specialist teams in general hospitalsneeded to maintain their skills.
Physician-owners of specialty hospi-tals have a financial incentive to referpatients whose conditions are less severe(which critics call “cream-skimming”) totheir hospitals. Because healthierpatients are less expensive to treat andare more likely to have good outcomes,specialty hospitals can benefit from thisselective referral both financially and inquality comparisons. The U.S. GeneralAccounting Office found evidence thatspecialty hospitals benefit from selectivereferral, which casts doubt on the qualityclaims made by specialty hospitals andleaves the impression that there is anuneven playing field in the market forspecialty patients.
Impact on CommunityHealth ServicesThe threat posed by specialty hospitalsto general hospital profitability is real,but is it a matter for public policy con-cern? The answer depends on the per-ceived value of the community servicesprovided by general hospitals. Generalhospitals not only provide their commu-nities with unprofitable health care ser-
Congress passes moratorium on new specialty hospitals
While this Issue Brief was in publication, Congress passed an 18-month mora-torium on physician self-referrals to new specialty hospitals as a part of theMedicare reform and prescription drug bill.The legislation grandfathers exist-ing specialty hospitals and those already under development, but prohibitsgrandfathered facilities from adding investors, expanding to other specialty cat-egories, or increasing beds by more than 50 percent. During the moratoriumperiod, two federal agencies will conduct analyses of the issue.This new legis-lation does not address immediate concerns about the impact of specialtyhospitals in Kansas since no changes to Medicare payments and referral lawsfor existing facilities were included.

vices, but also communityhealth services like disease pre-vention screenings and healtheducation. Many non-profit gen-eral hospitals care for the poorand underserved in fulfillmentof their mission. For-profit gen-eral hospitals may also provide acertain level of charity care.General hospitals may benefitfrom the goodwill generated byproviding such services, but thecost of providing them is implic-itly subsidized by the marginsearned on profitable health careservices. The growth of special-ty hospitals threatens the use ofthese implicit subsidies to fundcommunity health services.
In the communities where they exist,specialty hospitals already threaten thesesubsidies, but we do not yet knowwhether community services have beenaffected. The threat to general hospitalscould lead some of them to developstrategies to compete with or pre-emptspecialty hospitals. For example, theycould change the way they operate surgi-cal units, upgrade facilities or partnerwith physicians to build their own spe-cialty hospitals. Their alternative is to tryto scale back or find other sources offunding for the community services theyprovide. In communities where the threathas yet to emerge, policymakers maywish to maintain the system of subsidiz-ing unprofitable services with overallprofit margins within full-service hospi-tals. Maintaining this traditional methodof financing community health servicesmay require that policymakers raise bar-riers for specialty hospitals to make itmore difficult for them to compete.
Policy OptionsThere are a number of responses to theemergence of specialty hospitals thatpolicymakers could consider:
A. Wait and see.Before taking any action, policymakersmay want better information about thefinancial status and quality of care atgeneral hospitals and specialty hospitals.These data may not be available forsome time and could require additionalreporting by hospitals of both types. Inthe meantime, federal reform ofMedicare payments might reduce the rel-ative profitability of specialty hospitals.If Congress does not step in, though,more specialty hospitals could be built.
B. Remove the conflict of interestfor physician-owners of hospitals.Another option for policymakers is tolevel the competitive playing field byremoving the incentive physician-own-ers have to divert patients towards spe-cialty hospitals. Medicare forbidsphysicians from referring patients tohealth care facilities in which theyhold a direct investment, under provi-sions of federal law attributed toRepresentative Pete Stark (D-CA).However, the ban does not apply tophysicians who have invested in hos-pitals. The Medicare reform and pre-scription drug bill recently passed byCongress temporarily extends the ban
3KANSAS HEALTH INSTITUTE
Allen
Anderson
Atchison
Barber
Barton
Bourbon
Brown
Butler
Chase
ChautauquaCherokee
Cheyenne
Clark
ClayCloud
Coffey
Comanche Cowley
Crawford
Decatur
Dickinson
Doniphan
Douglas
Edwards
Elk
Ellis
Ellsworth
Finney
Ford
Franklin
GearyGove
Graham
Grant
Gray
Greeley
Greenwood
Hamilton
Harper
Harvey
Haskell
Hodgeman
JacksonJefferson
Jewell
Johnson
Kearny
KingmanKiowa
Labette
Lane
Leavenworth
Lincoln
Linn
Logan
Lyon
Marion
Marshall
McPherson
Meade
Miami
Mitchell
Montgomery
Morris
Morton
Nemaha
Neosho
Ness
Norton
Osage
Osborne
Ottawa
Pawnee
Phillips
Pottawatomie
Pratt
Rawlins
Reno
Republic
Rice
RileyRooks
Rush
RussellSaline
Scott
Sedgwick
Seward
Shawnee
SheridanSherman
Smith
Stafford
Stanton
Stevens Sumner
Thomas
Trego WabaunseeWallace
Washington
Wichita
Wilson
Woodson
Wyandotte
3
1
1 1
3
Specialty Hospitals in Kansas
Kansas Health Institute, 2003

on physician self-referrals to newspecialty hospitals (See box onpage 2). Nevertheless, states coulddecide for themselves to makesuch a moratorium permanent andwhether or not to extend themoratorium to existing facilities.Legislatures in Ohio, Illinois, NewMexico, and Washington, amongothers, have introduced legislationthat would prohibit physicianinvestment in specialty hospitals.
C. Require specialty hospitals toexpand services.Requiring specialty hospitals to pro-vide broader emergency services orto meet some specified level ofcommunity or charity care wouldspread the costs for these services,but could also weaken any advan-tages that stem from specialty hospi-tals’ narrow focus. The initial finan-cial success of specialty hospitalshas raised the question of whether itis more efficient for health carefacilities to specialize or to providecentralized delivery of a wide rangeof health care services. Requiringspecialty hospitals to broaden theirmission could make it more difficultto answer this question.
D. Re-establish certificate ofneed requirements.Another option for preserving criti-cal community health care servicesis to reinstate a Certificate of Need(CON) process to regulate construc-tion of new specialty hospitals.Kansas, among other states, elimi-nated CON in 1985 in favor of amarket-oriented approach to theallocation of health care invest-ments, patients, and profits. Statesthat retained CON, such asMissouri, have a regulatory tool tolimit the spread of specialty hospi-tals, and very few specialty hospi-
tals have been built in those states.However, it may be difficult to limitthe scope of CON to the specialtyhospital issue, just as it may be dif-ficult to insulate the CON processfrom undue political influence.
E. Provide direct financing forcommunity health services.Implicit subsidies within generalhospitals are not the only way tofinance community health services.Alternatives include increasingdirect subsidies to hospitals fortreating large numbers of poor anduninsured patients. Other optionsfor ensuring access to critical healthcare services include expandinghealth insurance coverage and pro-viding additional funding to localhealth departments for health careand community health services.
ConclusionSpecialty hospitals have made quickinroads in Kansas’ relatively openhealth care markets. Claims of high-er quality in specialized facilitieshave come up against fears thatthese new hospitals are disruptingthe flow of health care dollars tocritical health services. Policy-makers must decide whether to takeaction to limit the impact of thesehospitals in markets where theyhave already been built, and whetherthey should prevent their spread intonew communities. The market-based innovation of specialty hospi-tals can be weighed against thethreat they pose to the communityservices offered by general hospi-tals. To avoid this trade-off, policy-makers may need to identify a moreexplicit source of funding for theseservices, a difficult proposition inthe current fiscal environment.
Healthier Kansans through informed decisionsWWW.KHI.ORG 4
KANSAS
HEALTH
INSTITUTE
The Kansas Health Institute is anindependent, nonprofit healthpolicy and research organizationbased in Topeka, Kansas.Established in 1995 with a multi-year grant from the KansasHealth Foundation, the KansasHealth Institute conductsresearch and policy analysis onissues that affect the health ofKansans.
KANSAS HEALTH INSTITUTE
212 S.W. Eighth Avenue, Suite 300Topeka, Kansas, 66603-3936Telephone (785) 233-5443Fax (785) 233-1168www.khi.org
Copyright© Kansas Health Institute 2003.Materials may be reprinted with writtenpermission.
NUMBER 15 • DECEMBER 2003
“The market-basedinnovation of
specialty hospitalscan be weighed
against the threatthey pose to the
community servicesoffered by general
hospitals.”