Embed Size (px)
DESCRIPTION
Delivery of the Five Year Plan - Right Care Right Time Right Place for approval by Governing Body. Proposes to avoid public consultation on "Right Care" proposals and introduced (probably privatised) community care services without public consultation and afterwards consult on hospital service cuts proposals.
Citation preview
Agenda Item: 6
Report To:
Date:
Calderdale Clinical Commissioning Group
Governing Body Meeting
14th August 2014
Title of Report: Delivery of the Five Year Plan - Right Care, Right
Time, Right Place
FOI Exemption Category: Open
Responsible Director: Matt Walsh, Chief Officer
Report Author and Job
Title: Jen Mulcahy, Programme Manager
Executive Summary:
This report provides an update on progress in relation to
delivery of the CCG's five year strategy. Specifically, it provides
an understanding of the feedback from engagement and
proposals for changes to Community Services in Calderdale
and Hospital Services in Calderdale and Greater Huddersfield.
The report makes recommendations in relation to: the
commissioning and phasing of these changes, including options
for Consultation; sets out the work we still have to do; and
describes the Assurance Process that we will use to validate
that these changes will bring improvement in quality, safety,
effectiveness of care and that they are clinically sustainable
within available resources.
Finance/Resource
Implications:
To Be Confirmed
Risk Assessment: To Be Confirmed
Legal Implications: To Be Confirmed
Health Benefits: To Be Confirmed
Staffing/Workforce
Implications:
To Be Confirmed
Outcome of Equality An Equality Impact Assessment has been completed in relation
2
Impact Assessment: To the Closer to Home Model.
Sub Group/Committee: None
Recommendation (s): The Governing Body is asked to make the Following
Decisions:
1. To approve the approach to the further development of
our proposals for Community Services.
2. The delegate the sign off of Hospital Standards to Quality
Committee on 28th August.
3. To approve the High level Evaluation Criteria included at
Appendix E.
4. To delegate sign off of the detailed evaluation criteria and
evaluation approach to Finance and Performance
Committee on 28th August.
5. To delay consultation and adopt a phased approach to
implementation in line with Option Two above
The Governing Body is asked to Note:
1. That in areas where there is overlap between our
proposals and the Better Care Fund schemes we would
seek to commission in an integrated way
2. That we intend to engage with the NHS England process
at the end of August and will report our progress to the
next Governing Body.
1
1.0 Purpose of the Report
This report is intended to provide the Governing Body with an update on progress in
relation to delivery of our five year strategy. Specifically, it provides an
understanding of the feedback from our engagement and our proposals for changes
to Community and Hospital Services in Calderdale.
The report makes recommendations to Governing Body in relation to: the
commissioning and phasing of these changes, including options for Consultation;
sets out the work we still have to do; and describes the Assurance Process that we
will use to validate that these changes will bring improvement in quality, safety,
effectiveness of care and that they are clinically sustainable within available
resources.
The report requests decisions to progress with our Closer to Home Model, approve
the High Level Evaluation Criteria and to adopt a phased approach to
implementation that will delay the timing of when we go to consultation.
2.0 Background
The Right Care, Right Time, Right Place Programme brings together the seven
partners across Calderdale and Greater Huddersfield to develop proposals for
transformational change across the health and social care economy of Calderdale
and Greater Huddersfield. Significant change is essential because we want to
ensure that everyone gets the right care at the right time and in the right place, whilst
responding to the challenges of:
An ageing population with increased needs;
National shortages of key elements of the workforce that mean new service
models are required
Continuing to meet ever increasing external standards
Significant financial pressures facing commissioners and providers.
As Commissioners, our contribution to the delivery of this change is set out in our
five year strategy.
Our five year strategy is based on what the people of Calderdale have told us
through our engagement. It sets out the aims we want to realise, the outcomes we
expect to achieve, the Programmes of work we intend to deliver and the metrics we
will use to measure our success.
In parallel with the development of our Strategy, three of our existing Providers have
produced a jointly developed proposal for changing the way community and hospital
services in Calderdale and Greater Huddersfield could be provided. They described
their proposals in the form of a draft Strategic Outline Case (SOC), which was
presented to members of both CCGs' Governing Bodies in January, 2014. It was
2
presented to both the Kirklees and Calderdale Health and Wellbeing Boards (HWB)
and Overview and Scrutiny Committees (OSC) in February and March. The
Providers subsequently developed the Strategic Outline Case into an Outline
Business Case (OBC). This Outline Business Case was lodged with the NHS
Procurement Portal Bravo on the 23rd June but has not yet been seen by
Commissioners.
3.0 Introduction
We have used the engagement we have done over the past three years, including
Call to Action and previous Right Care, Right Time Right Place engagement, to
develop our Closer to Home proposals.
As well as influencing our proposals for the models of Health and Social Care that
we need to commission, our engagement has also: confirmed the fundamental need
for more integrated care delivered in community and primary care settings; and
provided feedback that the people in our communities will only gain confidence in our
new model through experiencing the improvements for themselves.
Therefore, we know that we need to phase any implementation of change over at
least five years. We also know that in making these changes we create an additional
driver for change to the way our Hospital Services are configured. This would impact
across Calderdale and Greater Huddersfield.
4.0 Our Five Year Strategy
Based on the needs of the population of Calderdale and what our Public and
Patients have told us we have agreed 8 outcomes that we want to deliver over the
five year period:
Empowered citizens and resilient communities;
Reduced Health Inequalities
Improved Patient experience and perception
Ensuring quality and safety in all we commission
Reduced Preventable deaths
Improved quality of life of patients with a long term condition or illness
People are helped to recover from illness and injury
Reduce reliance on unplanned hospital based care - by shifting to planned
community services.
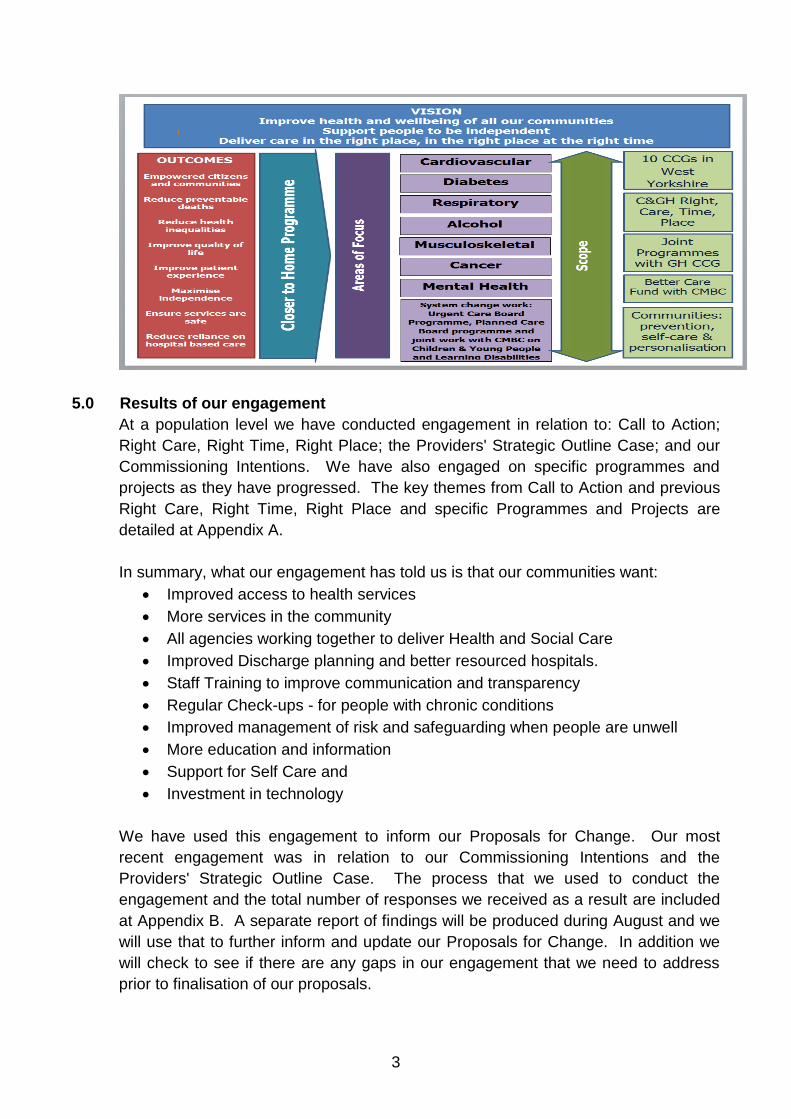
The plan is summarised below and demonstrates how the Closer to Home
Programme provides the focal point for all our priority areas.
3
5.0 Results of our engagement
At a population level we have conducted engagement in relation to: Call to Action;
Right Care, Right Time, Right Place; the Providers' Strategic Outline Case; and our
Commissioning Intentions. We have also engaged on specific programmes and
projects as they have progressed. The key themes from Call to Action and previous
Right Care, Right Time, Right Place and specific Programmes and Projects are
detailed at Appendix A.
In summary, what our engagement has told us is that our communities want:
Improved access to health services
More services in the community
All agencies working together to deliver Health and Social Care
Improved Discharge planning and better resourced hospitals.
Staff Training to improve communication and transparency
Regular Check-ups - for people with chronic conditions
Improved management of risk and safeguarding when people are unwell
More education and information
Support for Self Care and
Investment in technology
We have used this engagement to inform our Proposals for Change. Our most
recent engagement was in relation to our Commissioning Intentions and the
Providers' Strategic Outline Case. The process that we used to conduct the
engagement and the total number of responses we received as a result are included
at Appendix B. A separate report of findings will be produced during August and we
will use that to further inform and update our Proposals for Change. In addition we
will check to see if there are any gaps in our engagement that we need to address
prior to finalisation of our proposals.
4
In addition, Calderdale Council has established a People’s Commission that will give
local people an opportunity to debate what services are needed now and in the
future. We would seek to incorporate the views from The Commission as part of our
Engagement Approach.
6.0 Proposals for change
Based on the intentions in our five year strategy and the feedback from our
engagement, we know that significant changes are required in order to ensure health
and social care services are fit for the future. There is a national need to centralise
key services to improve outcomes for patients. The Right Care Programme is
developing proposals for what these future Community and Hospital services in
Calderdale and Greater Huddersfield could look like. There are three interlinked
pieces of work: Calderdale Closer to Home Programme; Greater Huddersfield Care
Closer to Home Programme; and the In Hospital Model.
Community Services
The Calderdale Closer to Home Programme and The Greater Huddersfield Care
Closer to Home Programme both set out proposals for the future of Community
Services. These proposals continue the shift of services and resources from
unplanned hospital care to the delivery of more supported self-care and more
integrated care delivered in community and primary care settings. The Calderdale
Closer to Home - Commissioning Intentions document (Appendix C) provides an
early view of the draft proposals for Calderdale. Whilst the high level model is
unlikely to change substantially, detailed work will continue on the expectations
around quality and outcomes. We are planning to further develop these proposals,
including dialogue with commissioners in Calderdale MBC and links with the Better
Care Fund, and also to reflect our most recent engagement and undertake any
further engagement to address any gaps. An early draft of the Commissioning
Intentions document will be shared at the Quality Committee on 28th August, with a
final version signed off at the Quality Committee on 25th September.
In-Hospital Services
Our requirements for In-Hospital Services are being developed jointly by Calderdale
and Greater Huddersfield CCGs and will, in the first instance, be a set of joint
standards. These joint standards set out the High level Outcomes we want to
achieve, the scope of In Hospital Services and the standards that we want to apply to
these Services. The standards are based on established best practice and are
additional to and do not replace existing CQC, NICE, CQUIN and standard contract
targets. The scope of the services is set out at Appendix D. We are currently
assuring these standards through a quality assurance group comprising
representation from both Calderdale and Greater Huddersfield CCG. We are
planning to gain sign off by the assurance group on 7th August and to present to
Quality Committee for sign off on 28th August.
5
7.0 Approach to Commissioning of Community Services
It is intended that the commissioning of Community Services will be done in a
phased manner, with the first phase comprising those services already provided in
the community. We would then seek to add further services that are currently
hospital based but could more appropriately be provided in the community.
We believe that the development of integrated commissioning is necessary to ensure
effective collaborative working across health and social care and in particular, ensure
patients, service users and carers experience integrated care across health and care
services. There are a number of services where we would seek to integrate our
commissioning arrangements in line with the Better Care Fund (BCF) and our shared
objectives of reducing demand for urgent and emergency acute hospital care and for
permanent admissions to care homes, so enabling and supporting people to live in
their own homes for as long as possible.
National guidance in relation to BCF has identified four priority areas:
Protecting social care services,
7- day services to support discharge and to minimise delayed transfers of
care,
Data sharing, including consistent use of the NHS number; and
Joint assessments and accountable lead professional.
The previous £1bn Payment for Performance framework has been revised so that
the proportion of the £1bn now linked to performance is based solely on an area’s
scale of ambition in reducing total emergency admissions.
Four schemes have been jointly designed with Calderdale Council to deliver the aims
of BCF:
Scheme 1- Hospital support services (Hospital Avoidance & Complex Discharge
Coordination),
Scheme 2 – 7 days a week working (7 day social work teams, Single Point of
Access to Intermediate Care, OOH Emergency Duty Scheme)
Scheme 3 – Locality Co-ordinated care (Single point of access (Gateway to Care)
Intermediate supported care and assessment (Heatherstones) Locality
Support and Independence teams, & Targets community support (CVD
– including stroke, diabetes, respiratory, mental health including
dementia, cancer and musculoskeletal.
Scheme 4 – Resilient communities and individuals (Prevention and self-care
programmes, Systematic identification and risk profiling, Self-care
optimising Assistive Technologies, Neighbourhood Peer Support
6
Networks, Carers emergency back up and peer networks, Extra-care
Hubs and adapted supported living environments scheme).
In areas where there is overlap between these schemes and our proposals for
change, we would seek to commission in an integrated way.
8.0 Approach to Market
Approach to Market is the process by which the CCG decides on the most
appropriate provider of services, but is not meant to imply that this is necessarily a
competitive process.
There are four elements to our Approach to Market
Commissioner confidence in the future capacity and capability of
providers and system co-production - we would undertake an assessment
of the capability of the current providers to deliver the service model,
integration and improvements required by the commissioner based on their
current delivery performance and track record of implementing systems
change.
Use of competitive procurement or not - we are not required to tender all
services, however we would need to demonstrate: that the selected provider is
either the only or most capable provider of required services; how not
undertaking procurement will provide the benefits of our service changes; that
we have considered the impact of our actions on the resilience of providers
and on associated services and; that all potential providers have been treated
equally and have had the opportunity to express an interest in providing the
services. There would also be an inherent risk of challenge should we not
procure competitively and that the duration of the contract would be limited to
three years (as opposed to seven years for a competitively tendered contract)
Commissioner's Governing Body Decision - Having considered the first
two elements in our Approach to Market, the Governing Body would be
required to make a decision regarding whether to re-commission the services
using competition or not
Invitation to Tender setting out Commissioner's requirements –
irrespective of whether the CCG decides to re-commission the services using
competition or not, the commissioner's requirements will be need to be set out
within formal Invitation to Tender (ITT) /Invitation to Commence Dialogue
(ITCD) documents and the process to receive a formal response to the
ITT/ITCD and a full and robust evaluation of whether or not the potential
provider(s) will deliver the expected service, outcomes and benefits required.
This will require the development of robust benefit realisation projections,
evaluation criteria and standards along with appropriate weightings.
7
As part of our approach to market we need to consider the timing of when we should
consider the Providers' Outline Business Case (OBC). This document was lodged
with the NHS Procurement Portal Bravo in June but has not yet been seen by
Commissioners.
At the time of writing, the commissioners have not looked at the OBC because in a
sense it has been produced and provided to the commissioners outside of due
procurement process. Monitor's advice is that the point in time at which we look at
the OBC is just one factor that may be relevant to whether our approach is open and
treats all providers equally.
In Calderdale CCG, we go some way to mitigating the risk of challenge by setting out
a clear view of our requirements prior to opening the OBC. This document sets out
those requirements at Appendix C.
9.0 Approach to Evaluation
As outlined in our Approach to Market, regardless of whether we decide to use a
competitive process, we will still set out our requirements (for both Community
Services and In-Hospital Services) in a formal Invitation to Tender (ITT) / Invitation to
Commence Dialogue (ITCD) process. There are three elements to our approach to
evaluation:
The first element identifies the accountabilities and responsibilities of the roles
and groups involved in the evaluation
The second element defines the Process we will use to identify, evaluate and
notify potential providers;
The third element is the Criteria we will use to undertake the evaluation.
We have drafted our high level evaluation criteria and these are set out at Appendix
E. We have grouped our criteria into seven high level categories and 20 sub-
categories.
It is proposed that we will gain sign off for our detailed Evaluation Approach through
the Finance and Performance Committee on 28th August.
10.0 Consultation
We know that significant changes are required in order to ensure health and social
care services are fit for the future. Condition specific programmes of change started
in 2012/13 and are continuing. One by one these changes, which are underpinned
by a programme of engagement activities, contribute to our evolving community
model. The changes to Community Services developed through our Closer to Home
8
Programme continues this shift of services from the hospital to the community.
Collectively, these changes mean that over the five years of our strategy we will
need to make changes to the way our Hospital Services are configured. Change to
the way our Hospital Services are configured can only be implemented following
formal public consultation.
There are two options on the timing of our consultation. Option One is to continue
developing our proposals and to go to public consultation in 2014 on proposals for
both Community Services and In-Hospital Services.
Option Two is to adopt a phased approach by continuing to develop and implement
changes to our Community Services to enable people to gain confidence in them
through direct experience of the improvements. We would then go to public
consultation at a later date in relation to In-Hospital Services.
There are strengths and weaknesses to both options.
Option One (consultation in 2014) would be in line with the timeline we have
previously published. It would provide an early opportunity for people to have their
say, and would allow us to start to address current workforce issues and reduce the
financial pressures facing Providers and Commissioners. However, it could delay
the implementation of our proposed changes to Community Services and it is likely
that the new model for Community Services would not be fully up and running before
we start to make changes to the In-Hospital services and brings the risk of a
deterioration in care until those services catch up. The absence of a direct
understanding of the improvements that the new community model would bring,
means that the consultation is likely to be focused on changes to Hospital services.
Additionally and importantly we would have to have demonstrated our readiness for
consultation by having satisfied all the external assurance requirements laid out by
NHS England through the engagement of the Clinical Senate and having satisfied
checkpoints one and two of the NHS Change Assurance Process.
Option Two (Consultation later) would be a change to our shared timeline. It would
allow us to continue our changes to community services so that we could provide
direct experience of an effective Community Model and demonstrate that we have
listened to the public. It would also allow us time to maximise the opportunity offered
through the Better Care Fund and incorporate the findings from the People's
commission. However, it would require us to demonstrate that we have conducted
sufficient engagement in relation to our proposed changes to community services;
potentially delay changes to hospital services, increasing the risk of a deterioration in
the quality of services our hospitals are able to provide, would mean that we could
not start to address current workforce issues, and there would be a need to fund and
resource double running of services. Importantly, there is a risk that this option
begins to have an effect on the motivation and morale of clinicians, particularly those
9
in secondary care who have worked so hard in partnership with the CCG to move
forward the dialogue about the need for change.
Having considered the strengths and weaknesses of both options, we believe that
we should change our timeline, delay consultation and adopt a phased approach to
implementation. In so doing, we are mindful of the risks, and will need to make
strenuous efforts to assure colleagues across the system that this in no way
represents a diminution in our ambition to deliver transformational change. It is the
considered view of the CCGs that this approach is more likely to deliver the long
term prize which we are seeking than to take the alternative approach.
11.0 Assurance Process
In support of our decision making, NHS England has a Strategic Change Assurance
Process that will consider our proposed changes to Community Services and In-
Hospital Services prior to any consultation exercise. The Strategic Change
Assurance Process will also validate that these changes will bring improvement in
quality, safety, effectiveness of care and that they are financially sustainable during
transition and post transition. We intend to engage with the NHS England process at
the end of August and will report our progress to the next Governing Body. As part
of the NHS England Strategic Change Assurance Process we will also engage with
the Yorkshire and Humber Clinical Senate. The Clinical Senate is a source of
independent advice and guidance to commissioners to help them make the best
decisions about healthcare.
12.0 Further work
We have set out above the engagement we have done, the changes we are
proposing, our approach to the commissioning and procurement of these changes,
the options in relation to Consultation and the Assurance Process that will support
our work.
There is also a number of underpinning pieces of work that we will need to complete
to support our Proposals.
We have commissioned work on the development of a Financial and Economic
model that will produce a financial case for change to demonstrate the economic and
financial sustainability of any proposed changes both during transition and post
transition.
We will also need to undertake work to understand the implications for our
Workforce, Technology and Estates.
10
13.0 Summary
In essence the CCG position is this;
1) We understand (indeed we have jointly authored with our partners) the
compelling case for change.
2) We have reflected carefully on the findings of engagement so far.
3) We believe that we will only persuade people of the need for changes in the
way that hospital services are configured by putting in place enhanced and
integrated community services in advance of those changes
4) We are persuaded that changes in hospital service configuration will be
required.
5) We believe that the timing of formal consultation on acute hospital service
configuration is crucial and that to attempt to commence consultation now
risks losing the opportunity for change.
5) At the time of writing we have not viewed the OBC, it is our understanding that
the OBC articulates clearly the providers' view on system risk.
6) We need to carefully assess the OBC presented to us by our providers in the
light of the standards and service models we are developing, and we will need
to be clear about how we mitigate existing and emerging risks to finance and
safety as we progress.
7) We intend to maintain our focus upon satisfying NHS England Change
Assurance processes and seek the Yorkshire and Humber Clinical Senate
view on our change proposals. Once we have demonstrated we are ‘ready for
consultation’ we can determine when that consultation should commence.
14.0 Recommendations
The Governing Body is asked to make the Following Decisions:
1. To approve the approach to the further development of our proposals for
Community Services.
2. The delegate the sign off of Hospital Standards to Quality Committee on 28th
August.
3. To approve the High level Evaluation Criteria included at Appendix E.
4. To delegate sign off of the detailed evaluation criteria and evaluation approach
to Finance and Performance Committee on 28th August.
5. To delay consultation and adopt a phased approach to implementation in line
with Option Two above
The Governing Body is asked to Note:
1. That in areas where there is overlap between our proposals and the Better
Care Fund schemes we would seek to commission in an integrated way
2. That we intend to engage with the NHS England process at the end of August
and will report our progress to the next Governing Body.
Matt Walsh
Chief Officer
Calderdale CCG
11
Appendices
Appendix A: Key Engagement Themes.
Appendix B: Engagement Process
Appendix C: Calderdale Closer to Home - Commissioning Intentions and High Level Model
Appendix D: The Services covered by our Hospital Standards
Appendix E: High Level Evaluation Criteria
Appendix A Key Engagement Themes
1
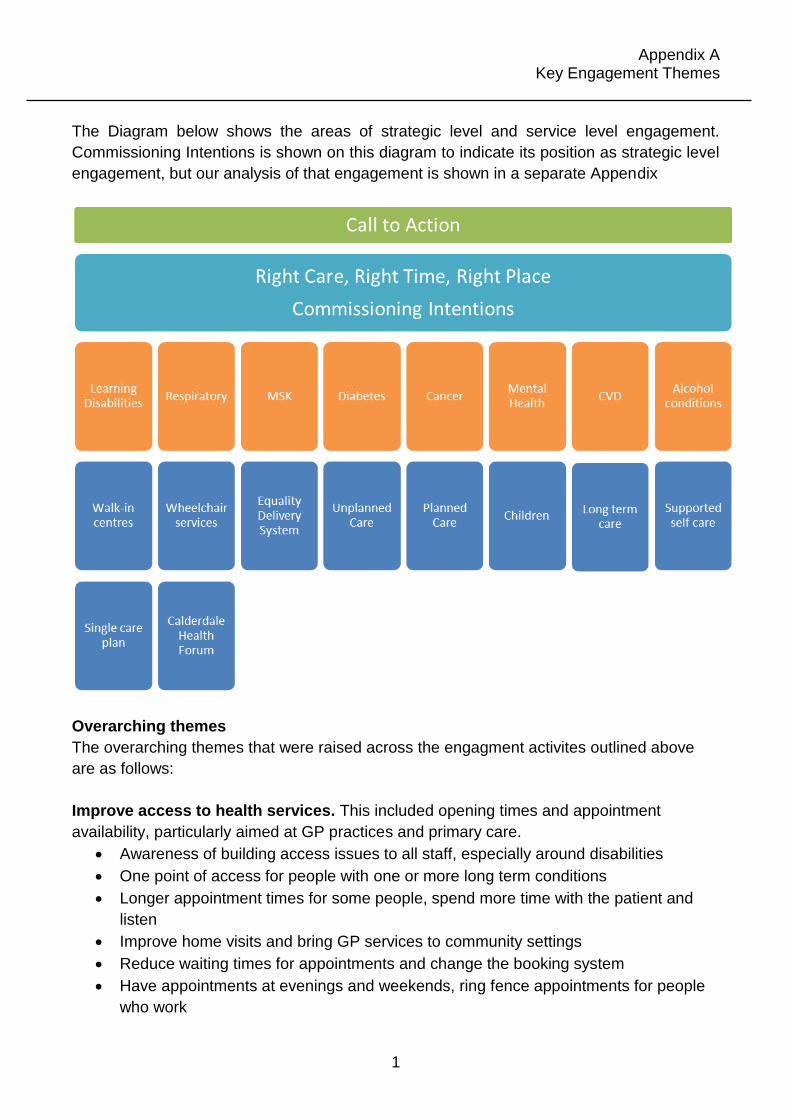
The Diagram below shows the areas of strategic level and service level engagement.
Commissioning Intentions is shown on this diagram to indicate its position as strategic level
engagement, but our analysis of that engagement is shown in a separate Appendix
Overarching themes
The overarching themes that were raised across the engagment activites outlined above
are as follows:
Improve access to health services. This included opening times and appointment
availability, particularly aimed at GP practices and primary care.
Awareness of building access issues to all staff, especially around disabilities
One point of access for people with one or more long term conditions
Longer appointment times for some people, spend more time with the patient and
listen
Improve home visits and bring GP services to community settings
Reduce waiting times for appointments and change the booking system
Have appointments at evenings and weekends, ring fence appointments for people
who work
Appendix A Key Engagement Themes
2
Have specialist staff in GP practices
More services in the community, the public would like to see more staff working with and
supporting local people in their own home and community.
More health assistants, social workers and nurses
Better home care
Named community staff for individual people
Better access to equipment to use in your own home
More day care and respite care for carers
Working together, all agencies, not just health, should work together to improve health
and wellbeing.
Joint teams that are managed centrally, not just teams that work together
Sharing of information and the ability to access a shared, patient owned record for
those that need to
Working with the third sector, as partners to improve health and wellbeing
Discharge planning and better hospitals. The public told us some of the things we
should consider to improve our hospitals there was a lot of focus on discharge.
Ensure that when people are discharged they have a robust plan that is backed up
with a health and social care services 24/7.
Ensure patients are fully recovered before they are discharged
Assign a professional to keep regular daily contact in the first week, fund and use
local VCS organisations to support the individual
Train and support carers in their duties so they can manage more safely and
effectively
More staff in hospitals, under resourced
Hospitals need to be clean and serve nutritional food to support recovery
Bring hospital services into community settings
Staff Training including changing the culture of the NHS, communication and
transparency.
Improve communication with patients and ensure they understand their condition
and treatment options and are able to make informed choices about their care
Make the NHS transparent at all levels
Train specialist staff (or have a matron lead)who understand different disabilities
and mental health
Regular check-ups for people with Chronic Conditions including annual check-ups or
possibly more frequent depending on the age and condition for everybody.
To be offered a wide variety of health and wellbeing checks, many people described
this as an MOT or health review
Appendix A Key Engagement Themes
3
Also a call for more targeted check-ups for those groups at particular risk
More routine scans and screening
Early diagnosis to ensure early intervention including self help
Manage risk and safeguarding, to the public this meant keeping people safe when they
were unwell.
Increase community staff and more regular house calls
More nurses on medical elderly wards
Make sure interpreters are available so people can understand information
Provide more emotional and social support at home
Prevent isolation, regular contact with local community
Consistent staff and named key workers with skills
Education and information. All information from the NHS should be available in easy to
understand formats and use a variety of different methods to reach the appropriate
audience.
There needs to be more information about how to maintain health and wellbeing and
how to avoid preventable conditions
More information on the services available and how to access them
Education courses should be available for specific conditions and general health and
wellbeing, preferably delivered by people with the condition themselves to provide
peer support
More education and information for young people – start at school, use Sure Start
centres
Self Care, including prevention, was a theme arising from strategic as well as project
specific engagement and included the following:
Care that is personalised with the support of specialist staff; patients being able to
access the right services at the right time
Getting support in being healthy and to be encouraged to self care by providing
access to information, advice and support with regards to diet, exercise, support
groups/networks and contacts for ongoing support
Ensuring patients are involved in the development of their care plan and informed so
they know what to expect, who to contact and provision of ongoing care and support
Involvement of wider networks such as carers and families and considering their
needs
‘Self Care’ to support those who are well to ensure prevention – well-being courses
for the community, particularly for young people
Care navigators and co-ordinators to support individuals
Invest in technology. Use technology better and invest in future technology, especially for
monitoring and sharing information between services and patients.
Appendix B Engagement Process: Commissioning Intentions and Providers' Strategic Outline Case
1
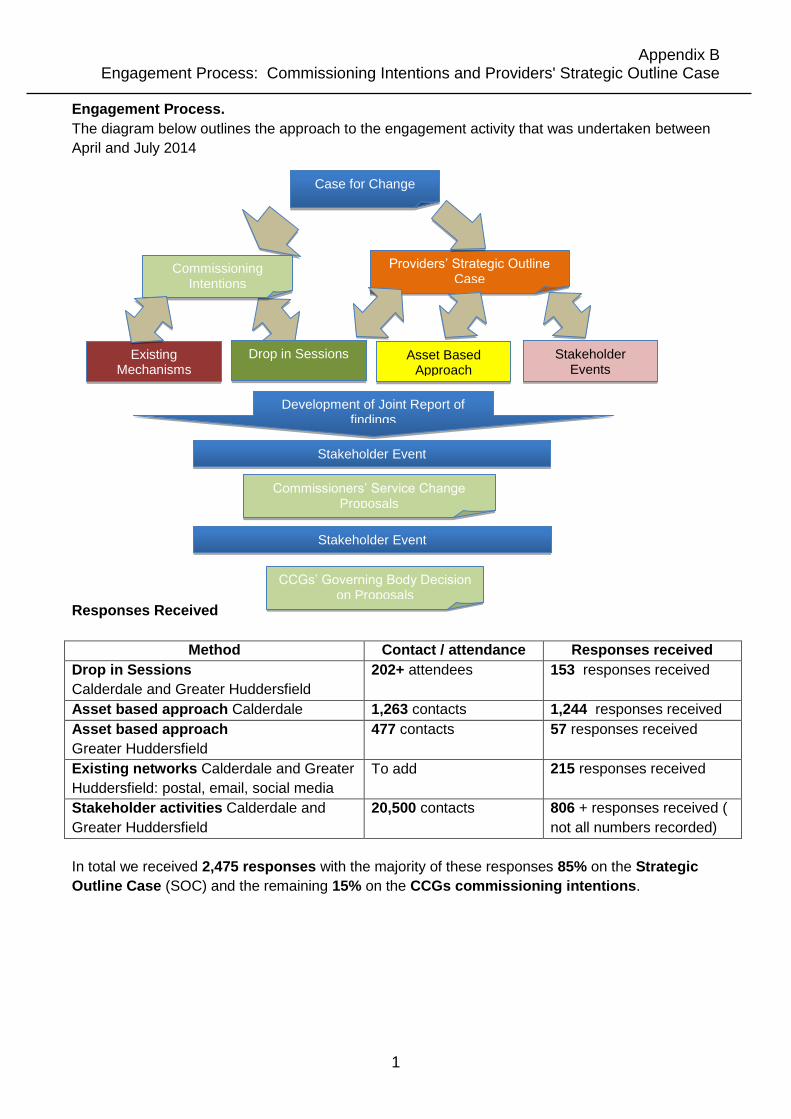
Engagement Process.
The diagram below outlines the approach to the engagement activity that was undertaken between
April and July 2014
For Change
Responses Received
Method Contact / attendance Responses received
Drop in Sessions
Calderdale and Greater Huddersfield
202+ attendees
153 responses received
Asset based approach Calderdale 1,263 contacts 1,244 responses received
Asset based approach
Greater Huddersfield
477 contacts 57 responses received
Existing networks Calderdale and Greater
Huddersfield: postal, email, social media
To add
215 responses received
Stakeholder activities Calderdale and
Greater Huddersfield
20,500 contacts
806 + responses received (
not all numbers recorded)
In total we received 2,475 responses with the majority of these responses 85% on the Strategic
Outline Case (SOC) and the remaining 15% on the CCGs commissioning intentions.
Case for Change
Providers’ Strategic Outline Case
Asset Based Approach
Stakeholder Events
Commissioning Intentions
Drop in Sessions Existing Mechanisms
Development of Joint Report of findings
Stakeholder Event
Commissioners’ Service Change Proposals
CCGs’ Governing Body Decision on Proposals
Stakeholder Event
2 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Appendix C
Calderdale Closer to Home - Commissioning Intentions and High Level Model NHS Calderdale Clinical Commissioning Group
Date: 5th August 2014 Version: V7.0
Status: In draft
3 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
CONTENTS
1. Executive Summary
2. Introduction 2.1. Introduction to Calderdale 2.2. Introduction to the Calderdale Closer to Home Model 2.3. Major service transformation 2.4. National Policy Context 2.5. What local people have told us about services 2.6. What local clinicians have told us about services 2.7. Working with partners 2.8. Description of current service provision 2.9. Lessons learnt from previous service change
3. Why do we need to change?
3.1. Population and health outcomes 3.2. Current model of care 3.3. Responding to the needs of the local community 3.4. Finance 3.5. Quality of care 3.6. Workforce 3.7. Social Capital 3.8. Summary of case for change
4. What are our ambitions for the future?
4.1. Design Principles 4.2. Aims of the new model 4.3. High level model
4.3.1. Access and Triage 4.3.2. Functions of the new model
4.4. Case studies 4.5. Services in scope 4.6. Quality Outcomes 4.7. Quality and Safety Standards
5. How will we assess the impact of any service change proposals?
5.1. Impact on Quality for service users 5.2. Equality Impact Assessment 5.3. Outline economic modelling of the case
6. Engagement Plan
6.1. Engagement with the public, patients and service users 6.1.1. Our strategic approach to engagement 6.1.2. Our approach to delivering engagement for closer to home
6.2. Alignment with partners’ strategic plans
4 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
7. Appendices
Appendix A- Case studies Appendix B- Quality Outcomes
5 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
1.0 Executive Summary
Calderdale is one of the smallest metropolitan districts in terms of population, but at 140 square miles, one of the largest in terms of area. Despite being a metropolitan district, Calderdale has very distinct rural elements; most of the area is classified as rural and while definitions vary, up to a quarter of its population lives in rural areas. Combined with the topography of the area, this pattern of settlement clearly has major implications for the location of facilities, for transport, and for how close people are to health and other care services. We have seen improvements in health outcomes over the last decade, life expectancy has increased for both men and women in Calderdale, death rates from ‘all causes’ and early death rates from cancer, heart disease and stroke have improved. We have seen a reduction in smoking rates and teenage pregnancies. We have seen improvements in the childhood immunisation coverage rates, flu vaccine uptake rates and the successful introduction of new vaccine programmes. However, the case for change presented in this document sets out the rationale for large scale change in Calderdale. The focus of our change programme over the next 5 years will continue the shift of services and the resources required to support unplanned hospital admissions to promote the delivery of care through integrated health and social care models - delivered in community and primary care settings. This forms the basis for our Closer to Home Programme. This work will also ensure that the resources invested in planned care are effective and are also provided in the most suitable setting – either in hospital or closer to home. This will transform the way our system currently works so that empowered citizens can access integrated community, social and primary care services that are connected by effective pathways into acute settings. This will ensure people can receive the right care at the right time in the right place
6 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
2.0 Introduction
This proposal demonstrates the case to transform Health and Social Care across Calderdale. The aims of this Service Change Proposal are to: Make the case for developing fit for purpose community services in Calderdale
underpinned by strong clinical evidence Describe the future model of care and how it has been developed
Give detail of the engagement to date that has been undertaken with the public, clinicians, staff and stakeholders in developing the future model of care and any future plans for engagement
The Service Change Proposal starts to address the Department of Health four tests for major service reconfiguration which comprise:
Strong public and patient engagement Consistency with current and prospective need for patient choice A clear clinical evidence base; and Support for proposals from clinical commissioners
2.1 Introduction to Calderdale
The metropolitan borough of Calderdale has a population of 203,000 people (2011 Census) and is a metropolitan borough of West Yorkshire. Calderdale is made up of both urban and rural areas with six distinct towns and communities (Brighouse, Elland, Halifax, Hebden Bridge, Sowerby Bridge and Todmorden). It is one of the smallest metropolitan districts in terms of population, but at 140 square miles, one of the largest in terms of area. Despite being a metropolitan district, Calderdale has very distinct rural elements; most of the area is classified as rural and while definitions vary, up to a quarter of its population lives in rural areas.
7 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Combined with the topography of the area, this pattern of settlement clearly has major implications for the location of facilities, for transport, and for how close people are to health and other care services.
Over the coming years we know that the size of the population in Calderdale (203,000) is set to increase. The projections indicate a period of relatively rapid population growth over the coming years, with the total district population projected to grow by around 17,000 by 2021 (an 8% increase).
The largest growth is expected to occur in the older age groups with a 35% increase in those aged 85 plus by 2021, a 27% increase in those aged 65 to 74 and a 26% increase in those aged 74 to 84. The improvement in treatments has resulted in a dramatic ageing of the overall population and a substantial increase in people living with long term conditions. There is also expected to be a substantial increase in children. As well as these increases there will also be greater and sometimes more complex variations in the range of needs expressed in the different communities and ethnic groups that make up Calderdale. As a consequence this will have implications for the types of services we need to commission. Deprivation, low income and associated unemployment and benefit dependency are closely correlated with a wide range of indicators of poor health or low levels of well-being. 2.2 Introduction to the Calderdale Closer to Home Model
The services currently commissioned for patients and service users in Calderdale are disjointed and inconsistent, we have duplication of service delivery and inappropriate hospital admission. There is a need for effective joined up working between acute, community care, primary care, social care and third sector organisations. We have made significant efforts to engage with our population to ensure we create the right blend of services in a community setting. The Closer to Home Model as described in section 4.0 allows us an opportunity to reorganise services to meet the needs of our population (section 3.1) ensuring they are treated with dignity and compassion and supporting them closer to and at home. Our aim is to make services more integrated, easier to access and less fragmented for users and carers. We will integrate services, deliver them as close to home as possible utilising multidisciplinary teams and make access to these services easier via the provision of a single point of access.
We intend to commission these services on a locality basis. More work is needed to determine the optimal number and geography for the locality teams, including integrated working with the Local authority. The areas covered by a locality team will be aligned with primary care/general practice (providing proactive co-ordination of care, particularly for people with long-term conditions and more complex health problems).
8 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
To deliver the integrated services proposed, we will utilise and enhance existing buildings within community and primary care settings.
Ultimately, by commissioning integrated high quality health and social care services we can be certain primary and community care can provide the right care in the right place, at the right time, first time, by staff with the competencies and skills to meet the needs of our patients and service users 2.3 Major service transformation
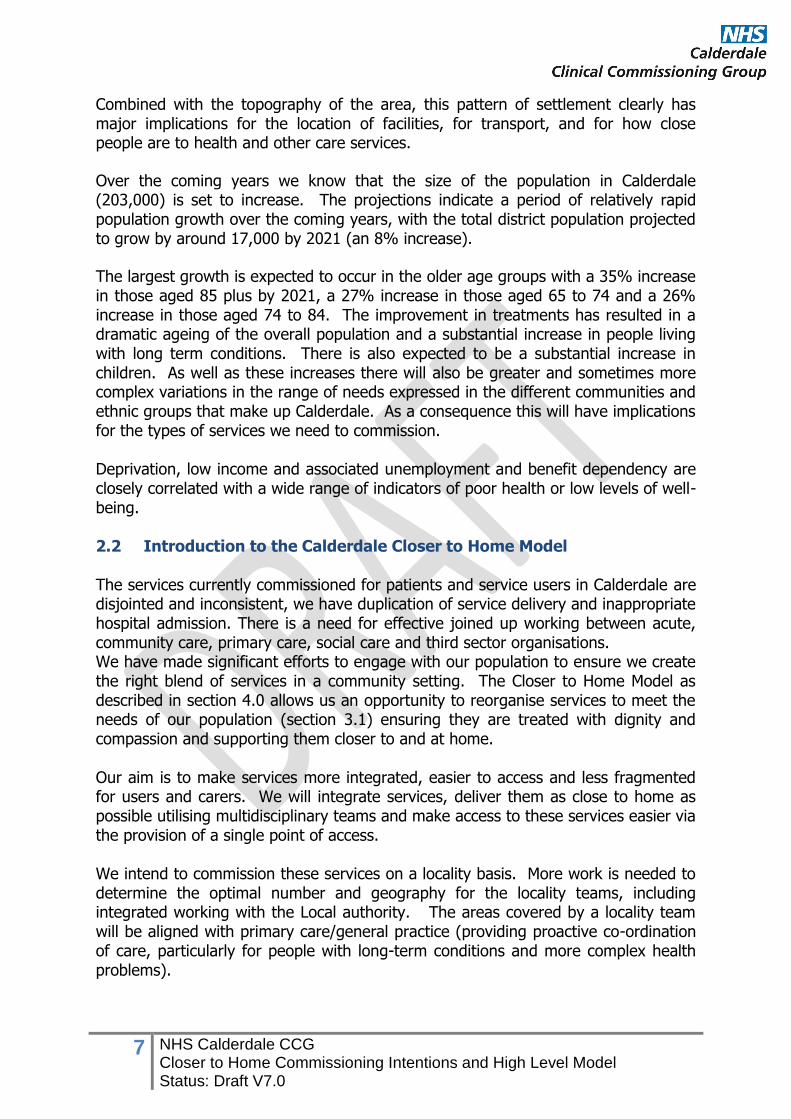
Over the past two years the seven health and social care organisations in Greater Huddersfield and Calderdale have been working together through the Strategic Review. The purpose of this is to encourage innovation and transformation to address the shared challenge of meeting the increasing needs of ageing population with limited and reducing resources. At the start of the Review, four care streams were set up looking at: children’s care, long-term care, planned care, and unplanned care. The care streams engaged local patients, carers, the third sector, public representatives and staff. The findings from this engagement, informed the development of a number of plans for improvements to the health and social care system. This work also highlighted a number of themes that impact on all areas of health and social care and which, between them, have the potential to really transform the way services are delivered, improving people’s outcomes and reducing costs further. The themes identified were: making the most of existing capacity and capability, digitising the health and social care economy, integrated services delivered in the community, integrated commissioning and personalisation, and taking forward the work of the children’s care stream. The work resulted in the development of a vision and model to underpin delivery of our ambitions: “The people of Calderdale will live healthy and independent lives secure in the knowledge that, if they need them, services will be there to keep them safe, supported and cared for.”
9 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
2.4 National Policy Context National policy for integrated care has changed significantly over the years and as a result of these changes new models of care have developed focusing on personalised services to address inequalities, prevention and early intervention. Users of health and social care services currently face a multiplicity of access points for services that are often uncoordinated and fragmented across the public sector. A report by the National Collaboration for Integrated Care and Support highlights that too often; we don’t communicate properly with each other, don’t work together as a team or don’t treat people as whole individuals. As a result, care and support is often fragmented, delayed or duplicated, which can result in missed opportunities to prevent needs from escalating and intervening early. This leads to poorer outcomes and experiences for the people who use our services. (National Collaboration for Integrated Care and Support– Integrated Care and Support: Our Shared Commitment - 2013) A high quality, efficient and sustainable health and social care system has a breadth reaching beyond the traditional hospital. In order to respond to the challenges that the system faces it needs to unite primary, secondary, community, social and preventative care in order to deploy professionals from these specialities in multi-disciplinary teams (MDTs). By working seamlessly together within local communities the MDTs can help tackle the health and social inequalities on the frontline and support people to be as independent and in control of their own lives as possible.
Whilst not exhaustive, at the time of preparing these Commissioning intentions, there are a number of key areas of important national policy or best practice that have particularly informed the development of proposals. These are shown in the table below:
Policy area/Issue Summary
NHS England: Everyone Counts Planning for Patients 2014/15 to 2018/19
The guidance emphasises how transformational change and new models of care are required to deliver great outcomes and better services now and for future generations. With a focus on providing high quality care, the guidance outlines stretching ambitions for the NHS that include:
Securing additional years of life for local communities
Improving the health related quality of life for people with long term conditions
Reducing the amount of time people spend in hospital through better and more integrated care in
10 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
the community and outside of hospital
Increasing the proportion of people living independently at home following discharge from hospital
Increase the number of people who have a positive experience of care, be it in hospital, outside of hospital, in general practice, or in the community
Make significant progress towards eliminating avoidable deaths in hospitals.
The ambitions outlined here will underpin the development of the change proposals described in this document.
The Keogh Urgent and Emergency Care Review
The need to improve urgent and emergency care services has been set out as a clear case for change described in the Keogh Review. The change proposals in this document will enable and prepare us to respond to this national strategic direction.
The Report of Mid Staffordshire NHD Trust – The Francis Enquiry
The report of the failings at Mid Staffordshire Trust and the associated reports by Sir Bruce Keogh (Review into the Care and Quality of Treatment provided by 14 Hospital Trusts in England) and Don Berwick (Improving the Safety of Patients in England) describe the actions needed to ensure there is a clear focus on providing safe and compassionate care. This document describes change proposals that could deliver this ambition.
NHS Belongs to the People - A Call to Action
NHS England called on patients, the public and staff to join in a discussion about the future of the NHS, so it can plan how best to deliver services, now and in the years ahead. This call to action set out the facts about future demands on NHS services, how the budget is currently spent and how services are delivered. This Call to Action was an opportunity for everyone who uses or works in the NHS to have their
11 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
say on its future. The views of the public collected through this nation debate have informed the development of the change proposals in this document.
The Better Care Fund Nationally it has been agreed that £3.8bn of NHS funding will transfer to Local Authorities to create a single pooled budget for health and social care. The aim of this it that the fund should be an important catalyst for change, and enable the move towards more preventative community- based care to help to keep people out of hospital and in the community settings for longer. This document describes change proposals that could deliver this ambition.
Future Hospital: Caring for Medical Patients
The Publication by the Royal College of Physicians provides a clinical evidence base and case studies of the benefits associated with changing the way we care for people with medical needs by integrating care across hospital, community and social care services. The document describes change proposals for doing this.
The draft Health and Social Care Bill and ‘Dilnot’ Report
The government’s proposals for social care funding reform (due to come into effect in 2016) will place a cap on the social care costs paid by an individual. The impact of this will further increase funding pressures for Local Authorities. The change proposals described in this document could mitigate the impact of this funding pressure.
Information Management and Technology
There are a number of national policy directives that set a clear direction and evidence base for increased use of technology in health and social care delivery to improve, patient safety, experience and efficiency of services. The change proposals described in this document include plans for optimising the use of technology to enhance the effectiveness and efficiency of service
12 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
provision.
National economic context Nationally the country continues to recover from the economic crisis, public spending continues to be reduced in key areas. The national spending review in 2013 identified further reductions for local government and no growth for health. The financial context for delivery of health and social care will continue to be challenging.
2.5 What local people have told us about Services
Over the past three years we have delivered a number of engagement activities which have enabled us to talk to local people on a range of healthcare services and topics. This information has been recently pulled together and analysed so the key overarching themes could be identified from what people have already told us. These themes from the engagement activity carried out over the last three years are summarised below but highlight the main issues for local people. As engagement has been extensive there are consistent themes on what people have told us about services and what is important to them. The themes are: Improve access to health services. This included opening times and
appointment availability, particularly aimed at GP practices and primary care
More services in the community, the public would like to see more staff working with and supporting local people in their own home and community.
Working together, all agencies, not just health, should work together to improve health and wellbeing.
Discharge planning and better hospitals. The public told us some of the things we should consider improving our hospitals there was a lot of focus on discharge
Staff Training including changing the culture of the NHS, communication and transparency
Regular check-ups including annual check-ups or possibly more frequent depending on the age and condition for everybody
Manage risk and safeguarding, to the public meant keeping people safe when they were unwell
Education and information. All information from the NHS should be available in easy to understand formats and use a variety of different methods to reach the appropriate audience
Self Care the term used by respondents was not ‘Self Care’ but self-help, self-management (manage) or ‘helping people cope’. Self-management (care) was a strong theme, this is how it was described
Invest in technology. Use technology better and invest in future technology,
especially for monitoring and sharing information between services and patients
13 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
The information gathered has helped inform the design of the future service model for Closer to Home. Using the key themes we have aligned our model to ensure the views of public, service users and carers have been used at the development stage. Due consideration for the things people want to see in our service model is demonstrated throughout. Going forward we will continue to use the information provided to further inform the service specification. This will include new information from our most recent engagement activity.
2.6 What local clinicians have told us about services
The Closer to Home Programme was invited to attend the Calderdale CCG Practice Leads forum on the 25th June and 10th July 2014. The attendees were made up of practice managers and GPs from all the GP practices in Calderdale. A presentation and workshop were delivered on both occasions. The group were asked to consider the following questions in the first session on the 25th June;
What services do you want to see in the community in the future? What changes would the system need to make for this to become a reality?
What is the role of General practice in this new model
The workshop on the 10th July was used to report back the findings and to test that the information was accurate. The feedback included a list of services that they want to see in the community in the future. This list of services will be used when developing the Closer to Home Model and specification. The group also identified a number of key enablers and functions that they identified as being required to support moving services closer to home. The themes are listed below and are in no particular order:
Information sharing Shared records Workforce development Timescale for recruiting Organisation development
Culture shift Estates- need investment in premises Third sector Communications – MDT and GP holding responsibility Telephone Consultations
Sign posting- enable patients/carers etc. Co –commissioning of GP services – NHS England Accountability and responsibility – decision makers are key/ who holds the
risk at which points in the model?
2.7 Working with Partners
Calderdale has a long and successful history of joint working – with commissioners and providers – both locally and regionally. There a number of key agendas, emerging locally which will have a direct impact on the development of a future model of community services:
14 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Joint Better Care Fund Plans Alignment of view on the planning geography for Calderdale – identifying a
consistent approach to defining localities and ‘neighbourhoods’.
Developing a new Preventative Strategy for Calderdale – focused on; smoking, alcohol, nutrition and physical exercise.
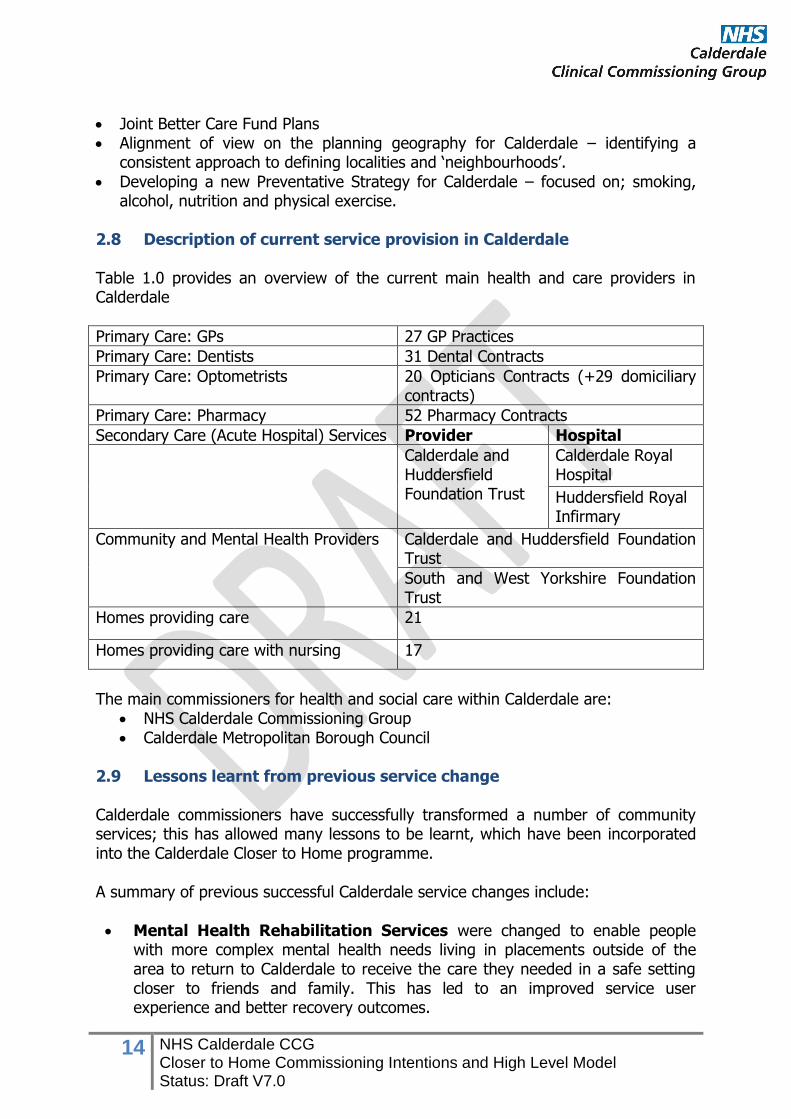
2.8 Description of current service provision in Calderdale
Table 1.0 provides an overview of the current main health and care providers in Calderdale
Primary Care: GPs 27 GP Practices
Primary Care: Dentists 31 Dental Contracts
Primary Care: Optometrists 20 Opticians Contracts (+29 domiciliary contracts)
Primary Care: Pharmacy 52 Pharmacy Contracts
Secondary Care (Acute Hospital) Services Provider Hospital
Calderdale and Huddersfield Foundation Trust
Calderdale Royal Hospital
Huddersfield Royal Infirmary
Community and Mental Health Providers Calderdale and Huddersfield Foundation Trust
South and West Yorkshire Foundation Trust
Homes providing care 21
Homes providing care with nursing 17
The main commissioners for health and social care within Calderdale are:
NHS Calderdale Commissioning Group Calderdale Metropolitan Borough Council
2.9 Lessons learnt from previous service change
Calderdale commissioners have successfully transformed a number of community services; this has allowed many lessons to be learnt, which have been incorporated into the Calderdale Closer to Home programme. A summary of previous successful Calderdale service changes include:
Mental Health Rehabilitation Services were changed to enable people with more complex mental health needs living in placements outside of the area to return to Calderdale to receive the care they needed in a safe setting closer to friends and family. This has led to an improved service user experience and better recovery outcomes.
15 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Integrated Intermediate Tier Services is an initiative to develop better and lower cost preventative care through integrated teams which enable people to get the advice, support and care needed to make faster recovery from illness and prevents the need for avoidable hospital or care home admissions.
Quest for Quality in Care Homes is an initiative on improving the quality of
care in care homes in Calderdale through dedicated Multi-disciplinary teams working across the care homes to support anticipatory care planning to ensure standards are applied consistently through the Care Homes in Calderdale.
As Commissioners we recognise that significant change is essential in order to ensure that everyone gets the right care at the right time and in the right place, whilst responding to the challenges we face. Calderdale has a long standing clear vision for developing better community based services, but has been repeatedly frustrated by the dominance of hospitals in planning decisions. The relative poverty in out of hospital services is now so great that it requires urgent correction. In developing the Closer to Home Model we will be clear on the deliverables, benefits and outcomes and how these will be measured in order to ensure that the changes deliver the right outcomes for the people of Calderdale.
3.0 Why do we need to change?
As commissioners of health and social care services in Calderdale, we recognise that the coming years will bring significant challenges in the ability of the current system to sustain and improve the quality of care delivered to the local population. The scale of the challenge has been well documented nationally by a range of organisations such as the Institute for Fiscal Studies (IFS), The King’s Fund, the OECD and the Health Select Committee. This case for change in Calderdale is built on our response to the pressures and drivers for change in the health and social care system that will enable us to transform the way services will be delivered by commissioning and designing services that:
improve health and social care outcomes for a growing and ageing population
support people to maintain their health as well as their independence provide the best possible care closer to home enhance the experience of health and care services across the local
population when people need to access them maximise the value obtained from every pound we spend on health and social
care so that services are sustainable in the long term
16 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
There are a number of system drivers for change: 3.1 Population and Health Outcomes • The size of the population of Calderdale is set to increase in the next 10 years,
and this increase will be greatest in the over 65+ age group (8,000 people) • The population of children and young people is also set to rise in the next 10
years, with the greatest increase in the 0 to 15-year-old age group (3,600). The proportion of children from South Asian origin will rise from 10% to 15%
• Life expectancy in Calderdale has improved for men in line with the rate for England, however it has levelled off for women and is below the national and regional average
• Despite this there is a growing health gap between the average and most deprived areas in Calderdale. Those living in Calderdale’s most disadvantaged communities experience greater ill-health than elsewhere in the district. There are differences in life expectancy between wards within Calderdale of up to seven years. When we compare the most affluent 10% of the population with the bottom 10% the gap is 10.9 years for men and 8.5 years for women
• An increasingly ageing population is leading to more people living for longer, increasing the prevalence of age-related diseases. Modern lifestyles are also creating problems, as certain lifestyles predispose people to ill-health. Smoking, for example, is the UK’s single greatest cause of preventable illness and early death. Unhealthy eating and lack of exercise are also known to contribute to increasing rates of obesity, diabetes and cardiovascular disease.
• Calderdale has a significantly higher Infant Mortality Rate than England. Over the last five years the IMR for the most deprived communities of Calderdale is more than double that of the least deprived
• Rising obesity levels, alcohol use and poor oral health are key health issues for children and young people. Childhood obesity increases between the ages of 5 and 11
• Behavioural factors which relate to health are not improving. Smoking prevalence and the harm caused by alcohol and obesity is increasing
Alongside providing services to meet the growth in demand, when combined with the impact of an older population and an increasing number of people with long-term conditions this will mean that the way the healthcare is delivered will have to respond to the different needs that these age groups, communities and individuals have. As commissioners we will need to maximise the value we can obtain from health spend to ensure that services can:
provide children and young people with the best life chances meet the needs of an ageing population and more people with a long-term
condition, recognising the disproportionate costs they currently consume in the current system
address current unmet needs within local communities
deliver the quality standards desired

17 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
3.2 Current Model of Care As a patient’s level of need increases, the current pattern of care (activity) tends to be episodic and reactive in responding to the health needs of individuals. This can escalate to crisis and ultimately hospitalisation where investment in acute services dominates health care spend in Calderdale. Patients may be receiving individual elements of care that is very good, but the whole pathway of care can be disjointed and fragmented, particularly when different providers of health and social care are involved. All patients require high quality and coordinated services, but nearly all have experience of care that is fragmented and in some instances of variable quality. Many also complain about the fractured nature of their care experience between not only different providers of health and social care, but also different parts of the same organisation not knowing what each other is doing. Calderdale’s utilisation of emergency care illustrates a greater reliance on acute settings (hospital) to meet patient need when compared with other CCGs across England – see chart from Atlas of Variation that ranks Calderdale’s rate of non-elective admission in the 5th (upper) quintile nationally.
Based on the growing body of evidence that suggests a large proportion of emergency activity can be influenced by effective collaboration across the health and social care system, reviewing the variation in the rate of activity between populations highlights the scale of the opportunity we face in Calderdale to:
1. Increase the effectiveness of how we design integrated services that provide care closer to home and reduce reliance on unplanned episodic treatment in hospital
2. Maximise the value we obtain from the investment we make in commissioned service that enable to people to manage their own health to maintain their independence
3. Ensure patients receive integrated and high quality care emergency care and can access these services when they need it
18 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
3.3 Responding to the needs of the local community We know that local people want to see services improved, whilst we know some things work well there are a number of areas which require improvement. Feedback from our recent engagement activity has told us that we need to improve access to our services and ensure people receive more services in a community setting. Current services are not responding fully to this request and we need to ensure we can develop future services with this in mind. In addition the public want agencies to work together, including how information is shared and providing information once. Investment in staff training and new technology is part of the public response to seeing improvements. Supported self-care is also a major focus for the public including how we develop information and systems to support people to be able to do this. 3.4 Finance The initial impact of the national reduction in levels of funding for public sector services manifested itself as a £20bn cost reduction challenge, dubbed the ‘Nicholson Challenge’, for the whole NHS to be achieved by 2014/15, as well as a significant reduction in local authority central funding equivalent to ~25% over 3 years. The latest economic projections suggest that the government spending review scheduled for 2015 will result in the NHS and local authority needing to deliver savings at a similar, if not higher level than those previously achieved. This will represent a significant funding pressure.
In July 2013 NHS England published “The NHS belongs to the people: a call to action” which sets out the challenges facing the NHS, including more people living longer with more complex conditions, increasing costs whilst funding remains flat and rising expectation of the quality of care. The document says clearly that the NHS must change to meet these demands and make the most of new medicines and technology and that it will not contemplate reducing or charging for core services.
“A call to action” forecasts that continuing with the current model of care will lead to a funding gap of around £30bn between 2013/14 and 2020/21. These savings are in addition to the £20bn savings already set out in the existing cost reduction challenge.
19 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
As a Calderdale system, the scale of the NHS system pressures identified in “A call to action” is significant. The Calderdale system needs to realise an approximate funding efficiency requirement of £80m between 2014/15 and 2018/19 across Calderdale CCG and providers.
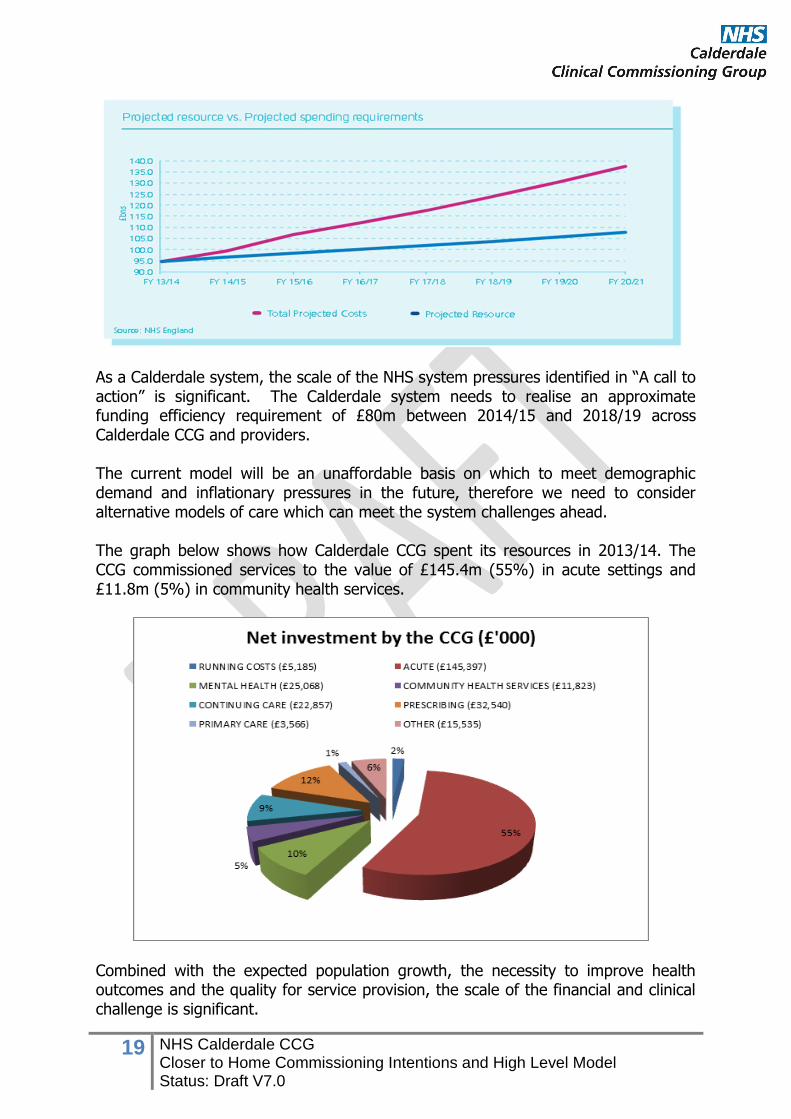
The current model will be an unaffordable basis on which to meet demographic demand and inflationary pressures in the future, therefore we need to consider alternative models of care which can meet the system challenges ahead. The graph below shows how Calderdale CCG spent its resources in 2013/14. The CCG commissioned services to the value of £145.4m (55%) in acute settings and £11.8m (5%) in community health services.
Combined with the expected population growth, the necessity to improve health outcomes and the quality for service provision, the scale of the financial and clinical challenge is significant.
20 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
3.5 Quality of Care The lessons from the Francis Report, Winterbourne View Hospital Review and the Berwick Report, are that quality is as much about our behaviours and attitudes to patients as human beings, as it is about the transactions we need to make to ensure services improve. We are working to deliver all external standards. Current pressure areas include: Providing good quality care is dependent on the quality of the available workforce
Current workforce challenges experienced both at national and local level highlight a need for providers and commissioners to work differently to meet care standards
Requirements from the Royal College of Physicians for early involvement of senior medical professionals in the assessment and management of acutely ill individuals and specialist services for children and young people’s compliance with national standards.
A critical part of meeting the professional standards and driving up quality are the consideration of professional dependencies. This is a set of services or functions which, when co-located or co-delivered, improve quality. The programme has considered the degree to which co-location and co-delivery are essential, desirable or preferable to agree the list of dependencies to be considered when designing future health and care services. 3.6 Workforce The NHS has a large and highly valued workforce but there are increasing shortages of skills in essential areas. The service has too often been configured around what can be offered. Our challenge is to drive reconfiguration of staff to meet emerging patient needs. This is supported by a recent Kings Fund report which identifies that today's workforce is facing a number of challenges. Training and development focuses on episodic care, but the greatest demand on services comes from older people who require integrated, long-term health and social care. There is a mismatch between the location of the current workforce and where care is needed, and both the NHS and social care sector require multi-skilled staff to work across boundaries. (Kings Fund, July 2013) The Workforce Assurance Group that brings together the seven organisations across Calderdale and Greater Huddersfield has developed a workforce model to capture baseline workforce information in relation to numbers and skills for all partners. The group will now undertake a SWOT analysis which will describe the impact of each organisation’s Strategic Plans on the current workforce. This will help to identify what the key gaps and workforce challenges are for the Calderdale health and social care system over the next few years.
21 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
3.7 Social Capital Providing a sense of what is meant by social capital is difficult and no one single definition can satisfy everyone. However for the sake of simplicity we can think of social capital as the links, shared values and understandings in society that enable individuals and groups to trust each other and so work together (OECD). Calderdale is made up of both urban and rural districts with a number of distinct communities, towns and networks where social capital can be found such as neighbourhoods, churches, schools, community centres, civic associations, sports clubs or even the local pub. These networks provide a platform to add value or have the potential to add to the social capital across the district through multiple channels such as: • Bonds - links to people based on a sense of common identity (“people like
us”) – such as family, close friends and people who share our culture or ethnicity
• Membership - links that stretch beyond a shared sense of identity, for example to clubs, societies or social groups
• Networks - links to people or groups from different social groups e.g. colleagues, associates
The pattern and intensity of these networks can vary. However the shift of services and the resources currently required to support episodic unplanned hospital admissions will need to harness the existing social capital that the district has to offer to support the shift required to provide and more importantly sustain the provision of care and support closer to home. 3.8 Summary of Case for Change Responding to the system drivers outlined above will require commissioners to develop new models of delivery. Radical changes to the commissioning and provision of services are needed that will:
meet the needs of the ageing population and the increasing number of people with long-term conditions
respond to what people have already told us they want from future services. sustain the quality of services patients experience
commission services that maximise value for money integrate services with social care and other agencies to reduce the reliance
on unplanned episodes of care in hospital
empower citizens to manage their own health enable patients to access the advice, care and treatment they need closer to
home
maximise the use of current infrastructure to deliver care closer to home
22 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
4.0 What are our ambitions for the future? Calderdale Closer to Home Model The suggested vision for Calderdale and integrating services closer to home is: The people of Calderdale will live healthy and independent lives secure in the knowledge that, if they need them, services will be there to keep them safe, supported and cared for.
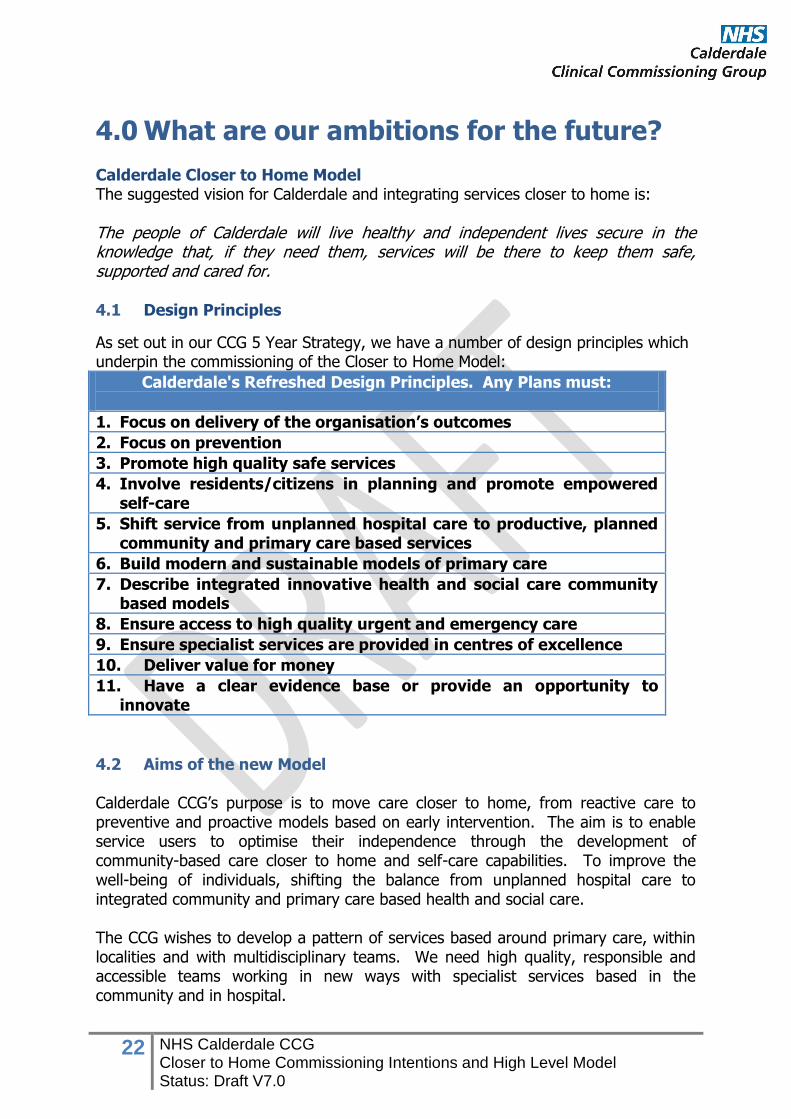
4.1 Design Principles
As set out in our CCG 5 Year Strategy, we have a number of design principles which underpin the commissioning of the Closer to Home Model:
Calderdale's Refreshed Design Principles. Any Plans must:
1. Focus on delivery of the organisation’s outcomes
2. Focus on prevention
3. Promote high quality safe services
4. Involve residents/citizens in planning and promote empowered self-care
5. Shift service from unplanned hospital care to productive, planned community and primary care based services
6. Build modern and sustainable models of primary care
7. Describe integrated innovative health and social care community based models
8. Ensure access to high quality urgent and emergency care
9. Ensure specialist services are provided in centres of excellence
10. Deliver value for money
11. Have a clear evidence base or provide an opportunity to innovate
4.2 Aims of the new Model
Calderdale CCG’s purpose is to move care closer to home, from reactive care to preventive and proactive models based on early intervention. The aim is to enable service users to optimise their independence through the development of community-based care closer to home and self-care capabilities. To improve the well-being of individuals, shifting the balance from unplanned hospital care to integrated community and primary care based health and social care. The CCG wishes to develop a pattern of services based around primary care, within localities and with multidisciplinary teams. We need high quality, responsible and accessible teams working in new ways with specialist services based in the community and in hospital.
23 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
The high level model for Closer to Home has been developed using local evidence and key outcomes from the engagement events undertaken across Calderdale over the past three years and clinical consensus that is informing us about the impact community services can have and what is needed to improve their effectiveness. The model responds to what local clinicians have told us. Our aim is for the model to be designed by putting our patients at the heart of everything we do and focusing on improving the things that really matter.
Underlying key aims of the proposed service model are to: Keep well, Stay Healthy
Detect problems early & prevent deterioration Keep out of hospital and Long Term Care Manage admission and discharge The six generic functions described in the model have been broken down into the following areas:
Information and Advice – self-care, self-management, primary prevention Early Intervention Services – promoting independence
Multi-Disciplinary Working Intermediate Tier/Urgent Response Specialist Support (In/Out Reach) Supported Discharge
A description of the six generic functions will be clearly defined in the service specification developed for Closer to Home. An early indication of the development for this is set out in section 4.3.2. Further development of how the six functions will be provided in Calderdale will be defined once the numbers and geography of the locality teams has been determined.
In addition to the case studies provided in Appendix A, an example has been provided below to explain how this model could work in the future: Example – A patient living in Sowerby Bridge with a long term condition would receive access to the dedicated multi-disciplinary team (MDT). This team will consist of a range of skilled and trained professional and clinical staff e.g. therapists, psychiatric nurses, social workers, voluntary workers, community matrons etc. The MDT will offer integrated physical health, mental health and social care support dependent on the patient’s needs. Support and care would be available from the appropriately skilled members of the MDT, this could involve one or more members of the team at any one time. The MDT will support patients to manage their health and care needs where appropriate, either, at home, in their local community or within their locality e.g. Upper Valley. The MDT will support patients to self-manage and self-care by
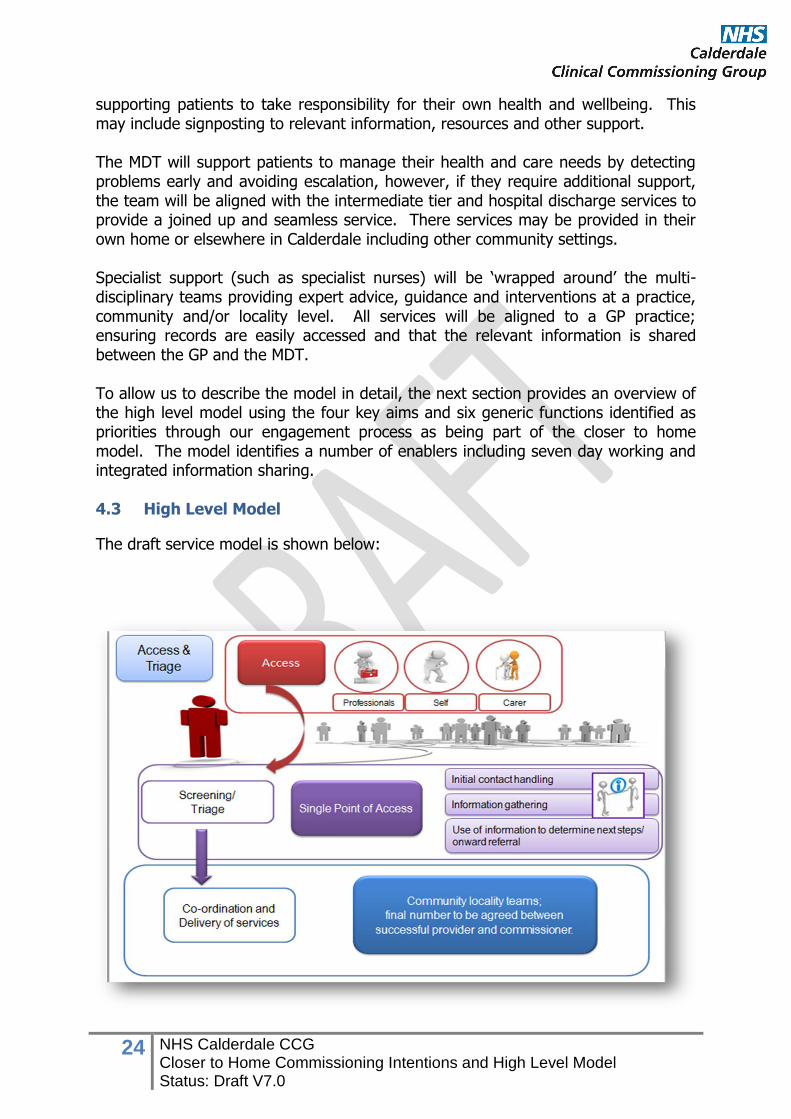
24 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
supporting patients to take responsibility for their own health and wellbeing. This may include signposting to relevant information, resources and other support. The MDT will support patients to manage their health and care needs by detecting problems early and avoiding escalation, however, if they require additional support, the team will be aligned with the intermediate tier and hospital discharge services to provide a joined up and seamless service. There services may be provided in their own home or elsewhere in Calderdale including other community settings. Specialist support (such as specialist nurses) will be ‘wrapped around’ the multi-disciplinary teams providing expert advice, guidance and interventions at a practice, community and/or locality level. All services will be aligned to a GP practice; ensuring records are easily accessed and that the relevant information is shared between the GP and the MDT. To allow us to describe the model in detail, the next section provides an overview of the high level model using the four key aims and six generic functions identified as priorities through our engagement process as being part of the closer to home model. The model identifies a number of enablers including seven day working and integrated information sharing. 4.3 High Level Model
The draft service model is shown below:
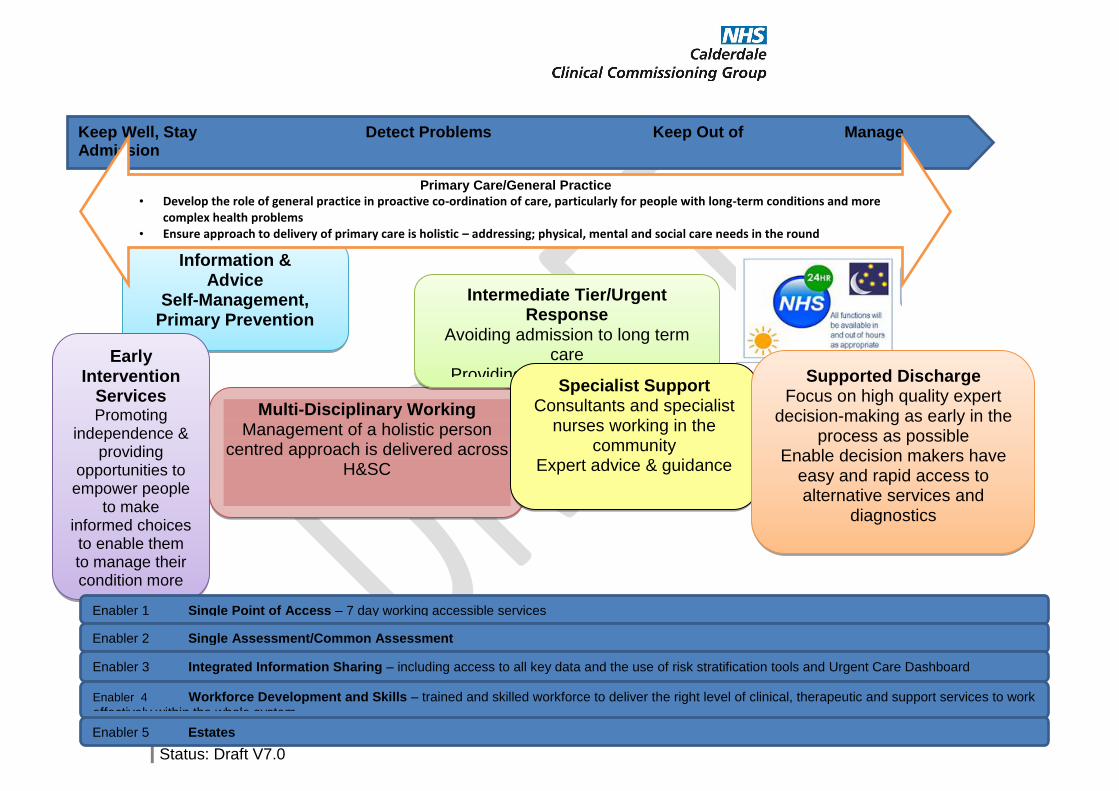
25 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Keep Well, Stay Detect Problems Keep Out of Manage Admission Healthy Early & Prevent Deterioration Hospital and Long Term Care & Discharge
Information & Advice
Self-Management, Primary Prevention
Early Intervention
Services Promoting
independence & providing
opportunities to empower people
to make informed choices to enable them to manage their condition more
effectively
Multi-Disciplinary Working Management of a holistic person
centred approach is delivered across H&SC
Intermediate Tier/Urgent Response
Avoiding admission to long term care
Providing urgent/crisis support
Enabler 1 Single Point of Access – 7 day working accessible services
Enabler 2 Single Assessment/Common Assessment
Enabler 3 Integrated Information Sharing – including access to all key data and the use of risk stratification tools and Urgent Care Dashboard
Enabler 4 Workforce Development and Skills – trained and skilled workforce to deliver the right level of clinical, therapeutic and support services to work effectively within the whole system
Primary Care/General Practice
• Develop the role of general practice in proactive co-ordination of care, particularly for people with long-term conditions and more complex health problems
• Ensure approach to delivery of primary care is holistic – addressing; physical, mental and social care needs in the round
Specialist Support Consultants and specialist
nurses working in the community
Expert advice & guidance
Supported Discharge Focus on high quality expert
decision-making as early in the process as possible
Enable decision makers have easy and rapid access to alternative services and
diagnostics
Enabler 5 Estates
26 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
4.3.1 Access and triage
This function sets out a Single Point of Access (SPA) and triage process, building and evolving the current SPA model developed within the redesign of the Integrated Intermediate Tier in 2011, following a 12 week consultation process with the public. This model also takes into account the findings from our recent engagement activity, which is cited in section 2.5.
The aim of this service is to improve access to community services, for example providing an integrated service at the outset with joint health and social care triage, extending opening times and providing availability out of hours.
The detail on how the SPA will work will be developed further through the specification. The specification is being developed through a multi-agency steering group and will involve representation from the public identified through our local Voluntary Sector and community networks.
Use of a single shared patient record will be critical to the delivery of an integrated care system, so patients and their carers only need to give information once.
4.3.2 Functions of the new model
Information and Advice, Self-Management and Primary Prevention
Practical information and support, focused on empowerment.
Local and national support networks integrated with other levels in model.
Care that is personalised with the support of specialist staff; patients being
able to access the right services at the right time
Provide support to encourage and empower individuals to be healthy and self-
care by providing access to information, advice and support with regards to
diet, exercise, support groups/networks and contacts for on-going support
Ensuring patients and carers are involved in the development of care plans
and informed of what to expect for the future.
Involvement of wider networks such as carers and families and considering
their needs
‘Self-Care’ to support those who are well to ensure prevention – well-being
courses for the community, particularly for young people
Care navigators and co-ordinators to support individuals
Other areas to be considered:
Fully integrated model with Social Service and Public Health
Fully integrated model with the Third Sector
27 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Early Intervention Services Promoting independence and providing opportunities to empower people to make
informed choices to enable them to manage their condition/s more effectively Proactive Early Intervention using risk stratification tools to identify the most
vulnerable individuals with long term conditions
Management within locality teams
Other areas to be considered:
Fully integrated model with Social Service and Public Health
Fully integrated model with the Third Sector
Multi- Disciplinary Team Working
Providing comprehensive assessment and re-ablement during post-acute care to
determine and reduce long-term care needs
Proactive Early Intervention using risk stratification tools
Wrap MDTs around localities, including mental health, social care, specialist
nursing and community resources
Deliver proactive care management approaches
Support people to manage their health and care needs in their own homes by
exercising self-management, choice and control where possible
Preventing unnecessary escalation by self-care support, through pathways and
strong gatekeeping functions in place to prevent default to admission
Co-ordinate risk and needs assessments and service delivery by ensuring
specialists are involved to design packages of care
Use innovations in IT to help record, deliver and share service information
electronically through a single shared record to help with service delivery
Other areas to be considered:
Fully integrated model with Social Services
Fully integrated model with the Third Sector
Criteria to include:
Co-morbidities
Working age adults with long term conditions/complex needs
Conditions relating to ageing
Age 75+ is a guide but not restricting criteria
28 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Intermediate Tier/Urgent Response Avoiding admission to long term care
Deliver rapid assessment by the most appropriate member of the MDT for urgent
health needs or breakdown of care, usually in the person’s home or care home.
Provide IV antibiotics and other ‘step up’ facilities to prevent a patient going into
hospital inappropriately
Provide crisis/urgent response 24/7 through access to a suitably trained clinician
To deliver home based care for those identified as most vulnerable.
Re-ablement to reduce dependence on high intensity, long term home support
Therapeutic interventions to facilitate timely or early discharge from acute
hospital
Meet the needs of people with mental health needs (mild cognitive impairment
and functional mental health) whose primary presenting need is of a physical
nature
Work with the existing Quest for Quality in Care Home and End of Life Care
(EOLC) models
Assess for aids and adaptations in the home
Consultants and specialist nurses to work in the community providing expert
advice and guidance to support care at home, working closely with GPs but not
always requiring referral by them
Manage the intermediate care beds
7 day working
Use innovations in IT to help record, deliver and share service information
electronically to help with service delivery
Other areas to be considered:
Fully integrated model with Social Services
Fully integrated model with the Third Sector
Explore options for integrated support workers to provide appropriate
interventions
Specialist Support Specialist expert advice and guidance will be available in a timely way to support decision making and care planning for patients with complex and or deteriorating conditions Support care at home and hospital avoidance
Service wrapped around an MDT model
Provide advice, up skilling and support to primary care
Provide outreach to care homes
Accessible through a wider range of care providers and not restricted by
requiring GP referral
29 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Supported Discharge Avoid unnecessary hospital admissions by providing timely care for patients in
their own homes/choice of care
Work into ED & MAU, create in-reach services to support discharge planning
(building on the frailty model)
Focus on high quality expert decision-making as early in the process as possible
(particularly for elderly patients)
Consultants and specialist nurses to work in the community providing expert
advice and guidance to avoid hospital admission
Planning for discharge by localities, to enable timely or early discharge
Decision makers have easy and rapid access to alternative services and
diagnostics
Use innovations in IT to help record, deliver and share service information
electronically through a single shared record to help with service delivery
Other areas to be considered include: Quest for Quality in Care Homes and End of Life Care pilots
Minor injury and illness units
Home from Hospital
Out of hours?
Potential for integrated support workers to provide appropriate interventions.
Criteria to include:
Patient at risk of unnecessary hospital admission or readmission To deliver the care closer to home integrated model of care we need to:
Develop the role of general practice in proactive co-ordination of care, particularly for people with long-term conditions and more complex health problems
Ensure approach to delivery of primary care is holistic – addressing; physical, mental and social care needs in the round
Promote self-management and primary prevention, proactive early intervention services
Establish a single point of access and single assessment process and documentation
Wrap multi-disciplinary teams around localities for people of all ages with complex needs, including social care, mental health, learning disabilities etc.
Build on existing integrated models of care across the whole system with the patient at the centre to proactively manage LTC’s, the elderly and end of life care closer to home
Develop clearly understood pathways ensuring care is provided closer to home and not delivered in a hospital setting where unnecessary
Provide rapid response to urgent needs to avoid unnecessary hospital emergency care
30 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Ensure co-ordinated early supported discharge is in place to manage discharge into planned, supportive community care
Use innovations in IT to help record, deliver and share service information electronically through a single shared record to help with service delivery.
4.4 Case Studies
We have produced two case studies to help explain the current and future model which can be seen in Appendix A. Both case studies have been tested at the Clinical Commissioning Leads Development forum, Practice Leads meeting and with the CCG Governing Body. Further development of case studies are in production and are being developed through our engagement team who will develop some Calderdale patient stories for us to use in the future as outlined in section 6.1.2.
4.5 Services in Scope
An integrated financial envelope has been produced to categorise the services within the scope for the Closer to Home Programme, these include community, primary care, social care, third sector and voluntary sector services across all age groups. This work will provide the CCG with clarity and assurance of the right services and the financial envelope to deliver the Closer to Home Programme. The work is in the development stage and will continue to be reviewed and revised over the next few weeks.
4.6 Quality Outcomes A draft Quality Outcome Framework has been produced focusing on the outcomes identified in the 5-year Strategic Plan and from all the engagement activity informing us of ‘what the public have told us they want’. There are eight new outcomes identified, these are:
1. Reduced preventable deaths; 2. Reduced health inequalities; 3. Improved quality of life of patients with a long-term condition or illness 4. Improved patient experience and perception – both within and outside
hospital care 5. People are helped to maximise their independence and recover from illness
and injury 6. Ensure the services we commission are safe 7. Reduce reliance on unplanned hospital based care 8. Empowered citizens and resilient communities
31 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
In developing the high level Quality Outcomes within this document, we have refreshed the CCG outcomes originally published in our prospectus in 2012/13. The table in Appendix B shows the consistency between the CCG outcomes, those of our system and the NHS England Planning for Patients outcomes. Continuous improvement will be evidenced through key performance indicators, action plans, progress monitoring and improvements / outcomes achieved reported at regular intervals. The draft high level Quality outcomes can be seen in Appendix B 4.7 Quality and Safety Standards All providers of Health Care will:
Have ways to ensure that high quality care is delivered
Publicise how well they are doing against a set of standards
Learn from reported incidents, complaints and peer review
The Quality and Safety standards are:
All commissioners of health care will expect high quality services and will
investigate unexpected variations in care and will support providers to be
open, honest and learn from mistakes.
All commissioners and providers of health care will work together to identify
people whose circumstances make them vulnerable, and as far as possible,
protect them from avoidable harm.
All commissioners and providers will learn from the experiences of people
who use services
All members of the health care workforce will have the right skills and
experience to deliver high quality care.
All health care providers will promote health and wellbeing.
All health care providers will support self-care and independence.
5.0 How will we assess the impact of any service change proposals?
5.1. Impact on Quality for service users
We have defined the high level Quality Outcomes we expect the service change proposals to deliver. We have set the high level quality and safety standards we will expect from providers. Work is now underway to clearly define the set of impact measures, key performance indicators and monitoring arrangements for the proposals.
32 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
We will consider the impact on quality for services users from a number of perspectives including, clinical effectiveness, patient safety and patient experience.
5.2. Equality Impact Assessment
As a public body the CCG has to consider if it has met its public sector equality duty and demonstrated due regard to the three aims of the general duty, in the exercise of its functions; · Eliminate discrimination, harassment and victimisation · Advance equality of opportunity · Foster good relations To demonstrate this, the CCG has undertaken an equality impact assessment (EQIA) on this programme. The initial draft to accompany the development of the programme will be considered at the Calderdale Quality Committee and will be developed further as the model evolves and particularly as the specification for service is developed. The EQIA considers if the plans would have an impact on people with protected characteristics and if so would this impact be positive or negative and whether any impacts could be potentially unlawful and what mitigating actions need to be taken to ensure the plan meets the general duty. The assessment is supported by local engagement activity and data on the Calderdale community. The protected characteristics are; age, disability, gender reassignment, pregnancy and maternity, race (this includes ethnic or national origins, colour or nationality), religion or belief (this includes lack of belief), sex, sexual orientation and marriage or civil partnership (employment only). 5.3. Outline economic modelling of the case We have jointly commissioned a piece of work with Greater Huddersfield CCG to produce a financial case for change. In the first instance we will produce a business case for the plans for changes to Community Services in Calderdale and Greater Huddersfield that takes account of planned reductions in Emergency Admissions and proposed changes to how services will be delivered. At the same time we will produce a robust probabilistic economic model to identify the areas which are most critical to transition from Hospital to Community. This will determine the sensitivity of the transition to changes in underlying assumptions (e.g. questions like, “How critical is making the expected savings in any particular service?” or “What is the probability of failing to make the expected savings in this service?”) provide a preliminary analysis of the number of beds potentially saved, split by service and identify where we should focus our efforts in completing a Full Business Case.
33 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
We will then utilise the Business Case for changes to Community Services and the Economic Modelling to produce a financial case for change that demonstrates the economic and financial sustainability of the proposed changes, both during transition and post transition.
6. Engagement Plan
6.1. Engagement with the public, patients and service users
6.1.1. Our strategic approach to engagement
0ur approach to public engagement and consultation is to ensure that we use a variety of different mechanisms, methods and approaches to engage with people. Our ‘Patient and Public Engagement and Experience Strategy’ which sets out our plans for the next three years is also in place to ensure that we adopt a whole system approach to supporting this work. Our strategy enables us to meet our responsibilities under the Health and Social Care Act 2012:
putting patients at the heart of everything we do
focusing on improving those things that really matter to our patients empowering and liberating clinicians to innovate, with the freedom to focus
on improving healthcare services and,
The recommendations of the Francis Report. Our strategy shows that we are committed to ensuring that we actively engage with patients, the public and other key stakeholders to ensure that the commissioning, design, development, delivery and monitoring of healthcare in Calderdale meets the needs of our population. By listening to patients, and learning from their experience of health care we can understand what really matters to people
6.1.2. Our approach to delivering engagement for closer to home
As the model is developed we will have an accompanying engagement plan which sets out our approach to further engaging on the closer to home service specification. This plan will set out how we intend to further engage public, patients and carers and continue to use emerging insights from our most recent engagement activity over the next few months. The plan will include:
Presenting further insight to the Closer to Home steering group from our most recent engagement activity which was on Calderdale CCG commissioning intentions and the providers SOC.
Setting up a network of service users who can work with the Care Closer to Home steering Group to further inform the development of the specification.
34 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
The development of arrange of case studies which provide a local focus to the current experience of services that can be used to test the model.
Engaging with the public on the model to further understand if we have considered everything we need to or if there is anything else we should consider.
Engaging with clinicians to further develop the model and to further understand if we have considered everything we need to or if there is anything else we should consider.
6.2. Alignment with partners strategic plans
Through the development of the Closer to Home Programme we will ensure alignment with the following areas:
Better Care Fund
Joint Commissioning with CMBC on Children and Young People’s work
Strategic priorities of Calderdale’s Health and Wellbeing Board
Plans for Specialist Commissioning
Plans developed by the West Yorkshire 10 CCGs
7.0 Appendices Appendix A: Case Studies Appendix B: Quality Outcomes
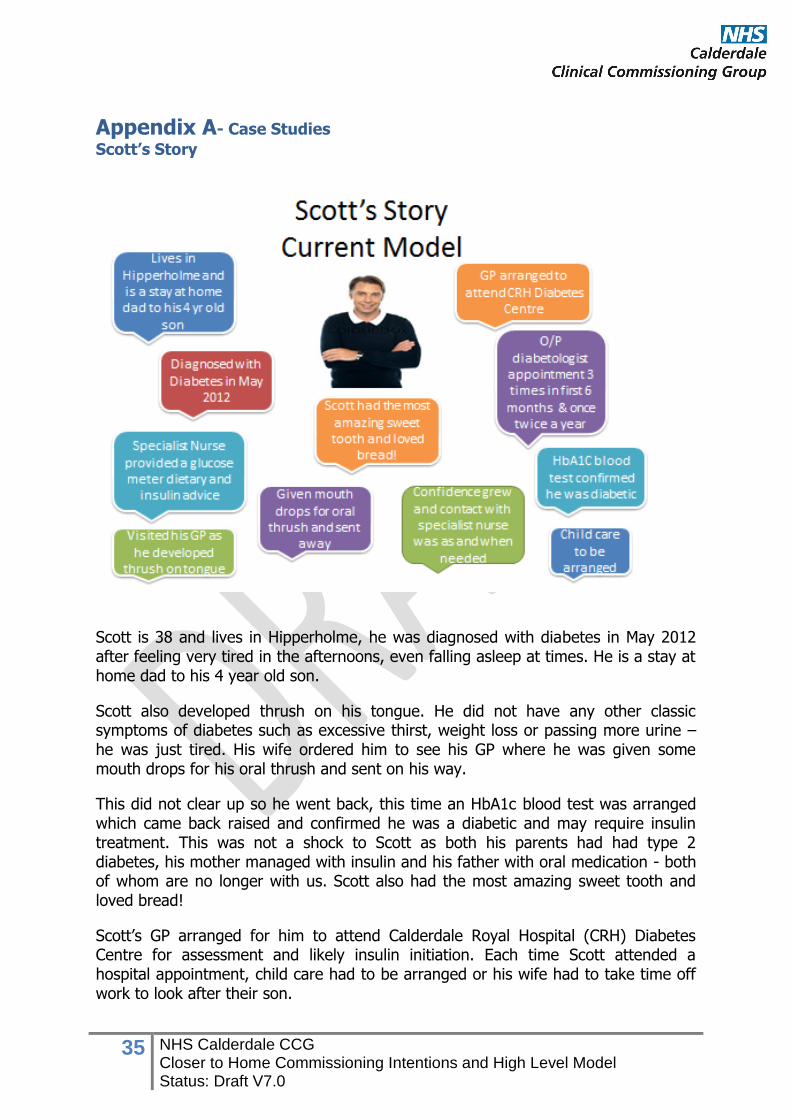
35 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Appendix A- Case Studies
Scott’s Story
Scott is 38 and lives in Hipperholme, he was diagnosed with diabetes in May 2012 after feeling very tired in the afternoons, even falling asleep at times. He is a stay at home dad to his 4 year old son.
Scott also developed thrush on his tongue. He did not have any other classic symptoms of diabetes such as excessive thirst, weight loss or passing more urine – he was just tired. His wife ordered him to see his GP where he was given some mouth drops for his oral thrush and sent on his way.
This did not clear up so he went back, this time an HbA1c blood test was arranged which came back raised and confirmed he was a diabetic and may require insulin treatment. This was not a shock to Scott as both his parents had had type 2 diabetes, his mother managed with insulin and his father with oral medication - both of whom are no longer with us. Scott also had the most amazing sweet tooth and loved bread!
Scott’s GP arranged for him to attend Calderdale Royal Hospital (CRH) Diabetes Centre for assessment and likely insulin initiation. Each time Scott attended a hospital appointment, child care had to be arranged or his wife had to take time off work to look after their son.
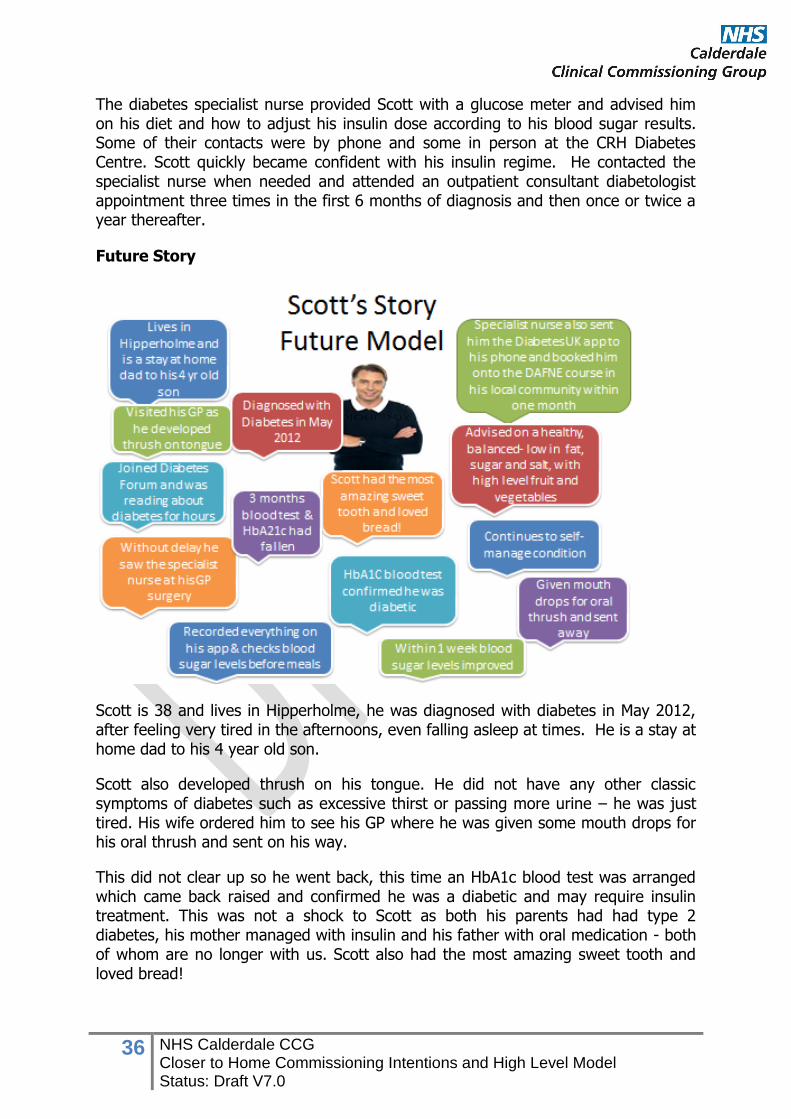
36 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
The diabetes specialist nurse provided Scott with a glucose meter and advised him on his diet and how to adjust his insulin dose according to his blood sugar results. Some of their contacts were by phone and some in person at the CRH Diabetes Centre. Scott quickly became confident with his insulin regime. He contacted the specialist nurse when needed and attended an outpatient consultant diabetologist appointment three times in the first 6 months of diagnosis and then once or twice a year thereafter.
Future Story
Scott is 38 and lives in Hipperholme, he was diagnosed with diabetes in May 2012, after feeling very tired in the afternoons, even falling asleep at times. He is a stay at home dad to his 4 year old son.
Scott also developed thrush on his tongue. He did not have any other classic symptoms of diabetes such as excessive thirst or passing more urine – he was just tired. His wife ordered him to see his GP where he was given some mouth drops for his oral thrush and sent on his way.
This did not clear up so he went back, this time an HbA1c blood test was arranged which came back raised and confirmed he was a diabetic and may require insulin treatment. This was not a shock to Scott as both his parents had had type 2 diabetes, his mother managed with insulin and his father with oral medication - both of whom are no longer with us. Scott also had the most amazing sweet tooth and loved bread!
37 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Without delay Scott saw the specialist nurse at the GP surgery who sent him the Diabetes UK app directly to his phone and booked Scott onto the DAFNE course in a local community centre within one month. Scott joined the Diabetes Forum and was reading about diabetes for hours. The decision was made that he would follow a healthy, balanced diet - low in fat, sugar and salt and containing a high level of fresh fruit and vegetables, and he was given a glucose monitor, which very quickly became his best friend.
Scott initially recorded everything he ate on his phone app for counting nutritional info. Scott doesn’t note what he eats now unless it’s new food. He also checks his blood sugar levels before and after every meal.
Within 1 week his blood sugar levels were much improved and with the supervision of his specialist nurses he was adjusting the dose of his insulin according to what he ate, using the information he learnt on the DAFNE course.
Just over 3 months later Scott visited the specialist nurse at his GP surgery for another set of blood tests and his HbA1c had fallen to 41 mmol/mol. The nurse was delighted with Scott’s excellent results in such a short time
Scott continues to self-manage his condition and is confident with his insulin regime. Scott is a regular contributor to the patient question forum on the Diabetes UK website and has established a diabetes patient support group at his practice to support local people with diabetes.
In summary Scott never has to go to hospital or see a consultant. His GP is still senior coordinating clinician but most of the work is done by supportive community staff.
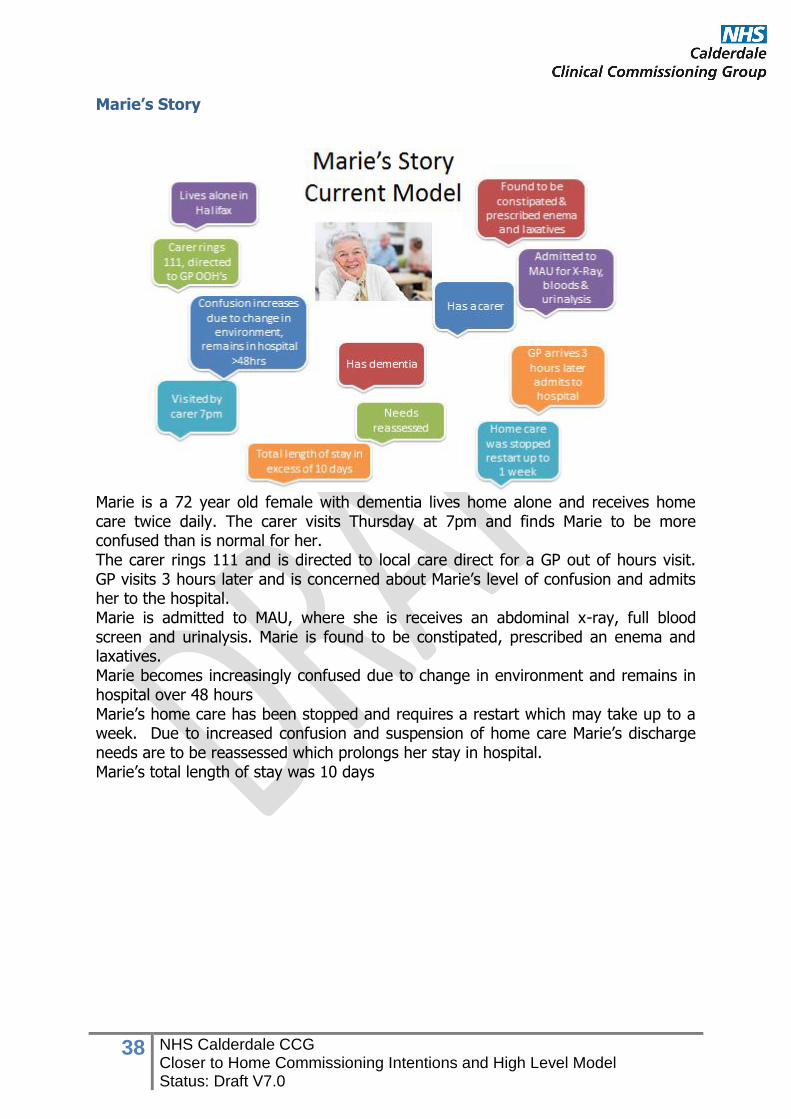
38 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Marie’s Story
Marie is a 72 year old female with dementia lives home alone and receives home care twice daily. The carer visits Thursday at 7pm and finds Marie to be more confused than is normal for her. The carer rings 111 and is directed to local care direct for a GP out of hours visit. GP visits 3 hours later and is concerned about Marie’s level of confusion and admits her to the hospital. Marie is admitted to MAU, where she is receives an abdominal x-ray, full blood screen and urinalysis. Marie is found to be constipated, prescribed an enema and laxatives. Marie becomes increasingly confused due to change in environment and remains in hospital over 48 hours Marie’s home care has been stopped and requires a restart which may take up to a week. Due to increased confusion and suspension of home care Marie’s discharge needs are to be reassessed which prolongs her stay in hospital. Marie’s total length of stay was 10 days
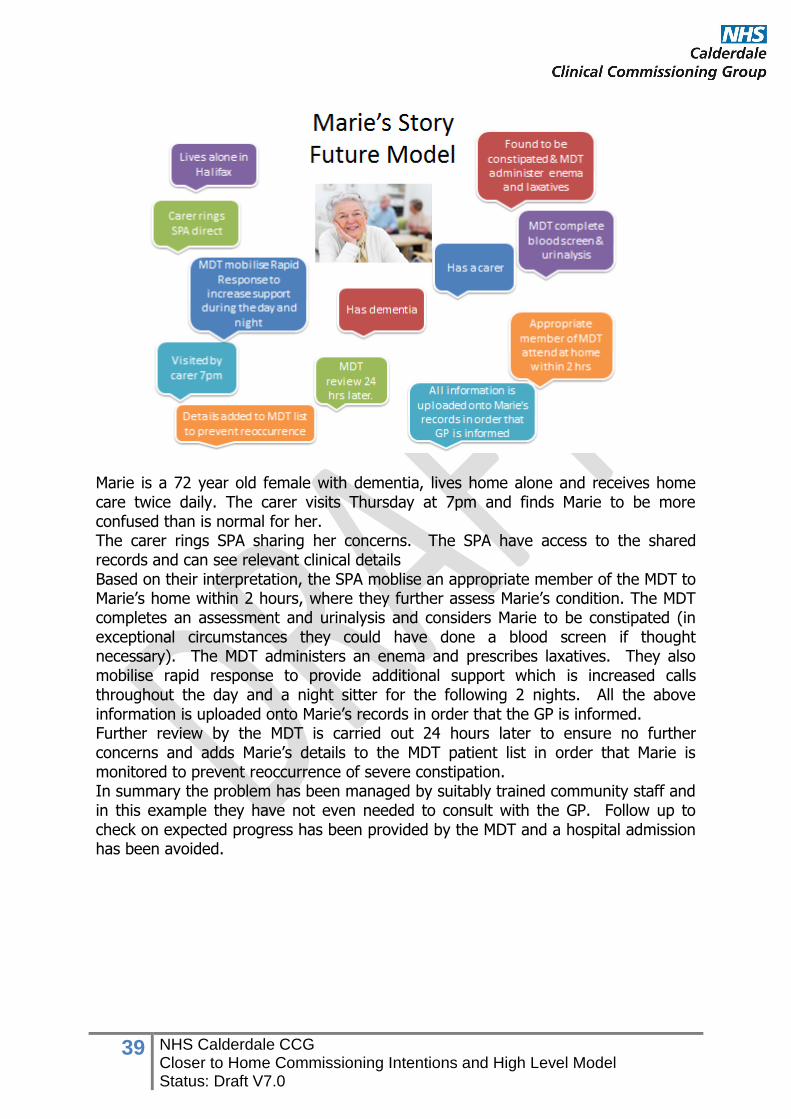
39 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Marie is a 72 year old female with dementia, lives home alone and receives home care twice daily. The carer visits Thursday at 7pm and finds Marie to be more confused than is normal for her. The carer rings SPA sharing her concerns. The SPA have access to the shared records and can see relevant clinical details Based on their interpretation, the SPA moblise an appropriate member of the MDT to Marie’s home within 2 hours, where they further assess Marie’s condition. The MDT completes an assessment and urinalysis and considers Marie to be constipated (in exceptional circumstances they could have done a blood screen if thought necessary). The MDT administers an enema and prescribes laxatives. They also mobilise rapid response to provide additional support which is increased calls throughout the day and a night sitter for the following 2 nights. All the above information is uploaded onto Marie’s records in order that the GP is informed. Further review by the MDT is carried out 24 hours later to ensure no further concerns and adds Marie’s details to the MDT patient list in order that Marie is monitored to prevent reoccurrence of severe constipation. In summary the problem has been managed by suitably trained community staff and in this example they have not even needed to consult with the GP. Follow up to check on expected progress has been provided by the MDT and a hospital admission has been avoided.
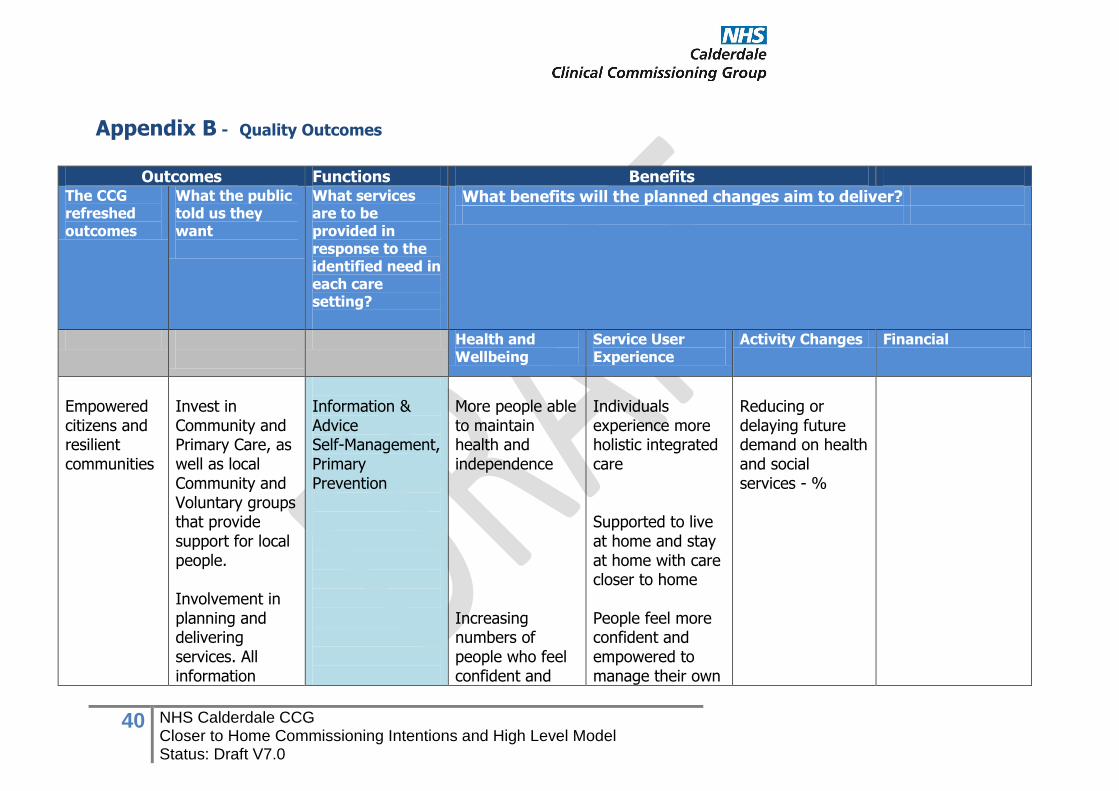
40 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Appendix B - Quality Outcomes
Outcomes Functions Benefits
The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
Empowered citizens and resilient communities
Invest in Community and Primary Care, as well as local Community and Voluntary groups that provide support for local people. Involvement in planning and delivering services. All information
Information & Advice Self-Management, Primary Prevention
More people able to maintain health and independence Increasing numbers of people who feel confident and
Individuals experience more holistic integrated care Supported to live at home and stay at home with care closer to home People feel more confident and empowered to manage their own
Reducing or delaying future demand on health and social services - %
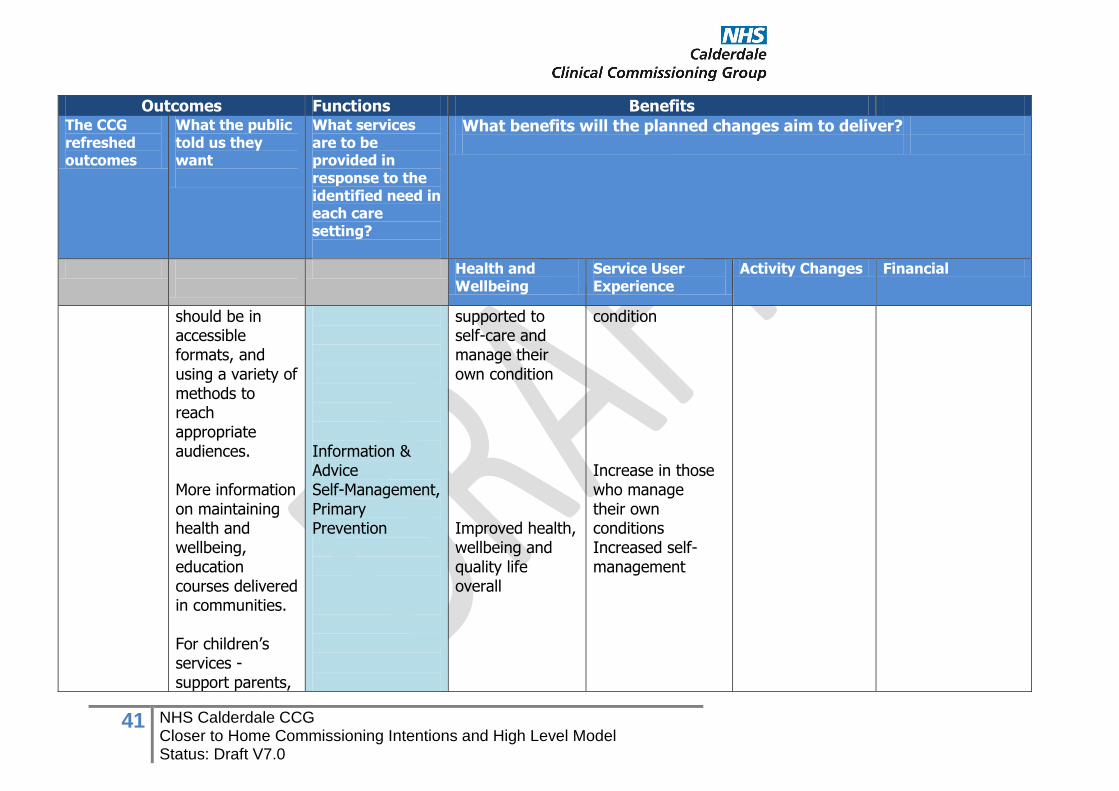
41 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Outcomes Functions Benefits The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
should be in accessible formats, and using a variety of methods to reach appropriate audiences. More information on maintaining health and wellbeing, education courses delivered in communities. For children’s services - support parents,
Information & Advice Self-Management, Primary Prevention
supported to self-care and manage their own condition Improved health, wellbeing and quality life overall
condition Increase in those who manage their own conditions Increased self-management
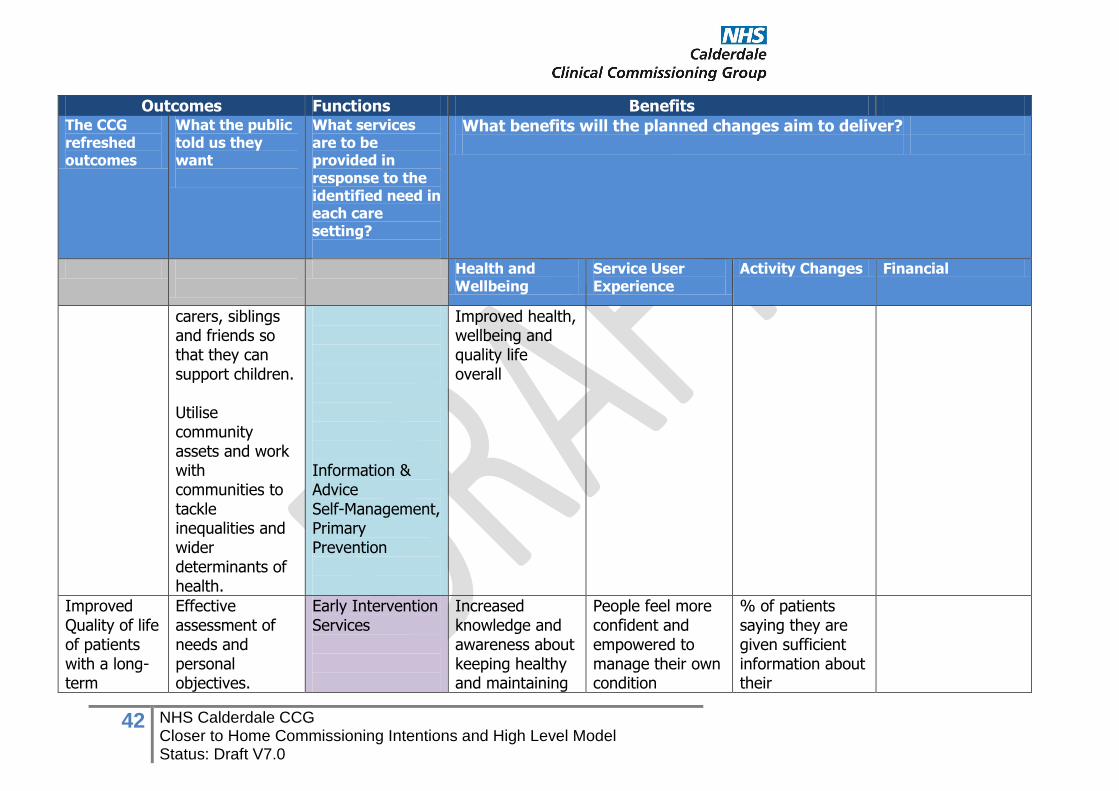
42 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Outcomes Functions Benefits The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
carers, siblings and friends so that they can support children. Utilise community assets and work with communities to tackle inequalities and wider determinants of health.
Information & Advice Self-Management, Primary Prevention
Improved health, wellbeing and quality life overall
Improved Quality of life of patients with a long-term
Effective assessment of needs and personal objectives.
Early Intervention Services
Increased knowledge and awareness about keeping healthy and maintaining
People feel more confident and empowered to manage their own condition
% of patients saying they are given sufficient information about their
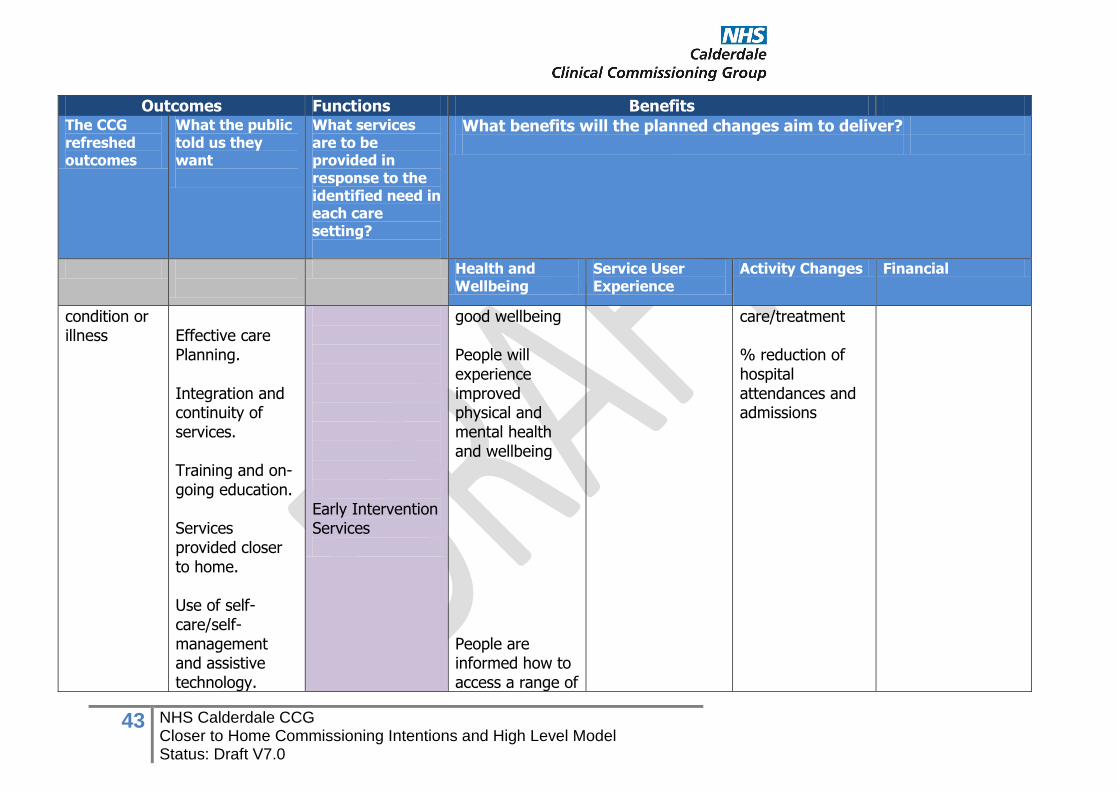
43 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Outcomes Functions Benefits The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
condition or illness
Effective care Planning. Integration and continuity of services. Training and on-going education. Services provided closer to home. Use of self-care/self-management and assistive technology.
Early Intervention Services
good wellbeing People will experience improved physical and mental health and wellbeing People are informed how to access a range of
care/treatment % reduction of hospital attendances and admissions
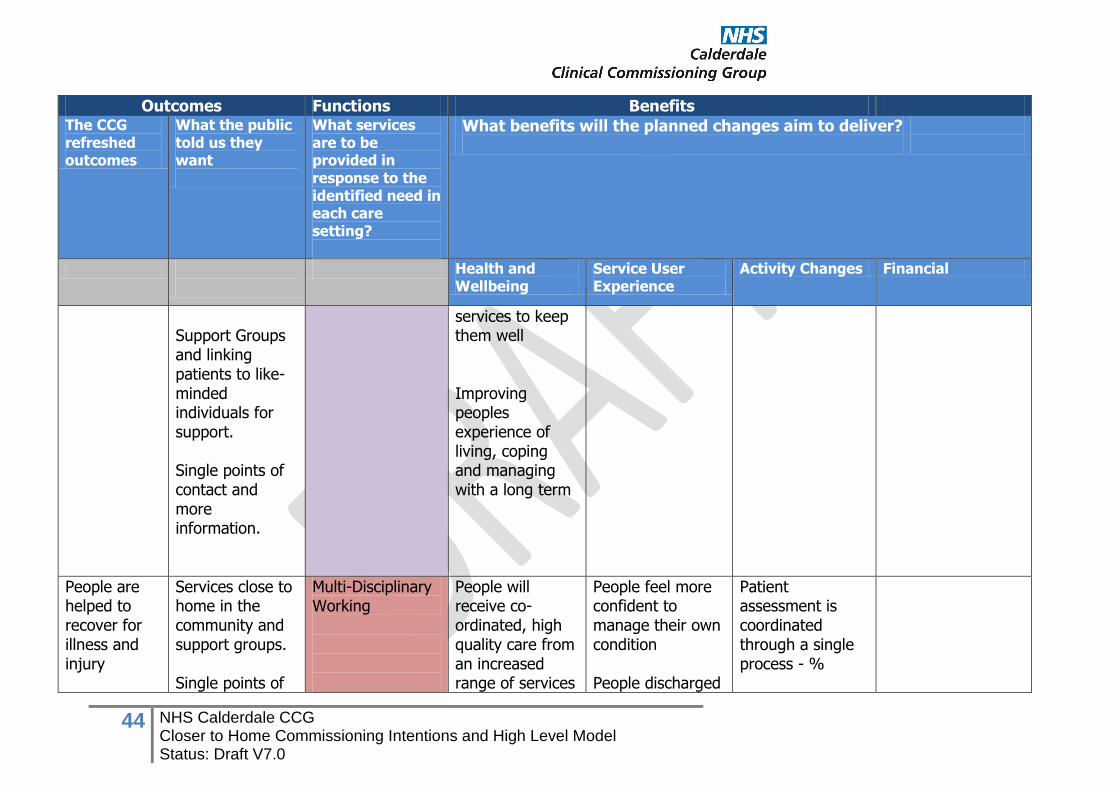
44 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Outcomes Functions Benefits The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
Support Groups and linking patients to like-minded individuals for support. Single points of contact and more information.
services to keep them well Improving peoples experience of living, coping and managing with a long term
People are helped to recover for illness and injury
Services close to home in the community and support groups. Single points of
Multi-Disciplinary Working
People will receive co-ordinated, high quality care from an increased range of services
People feel more confident to manage their own condition People discharged
Patient assessment is coordinated through a single process - %
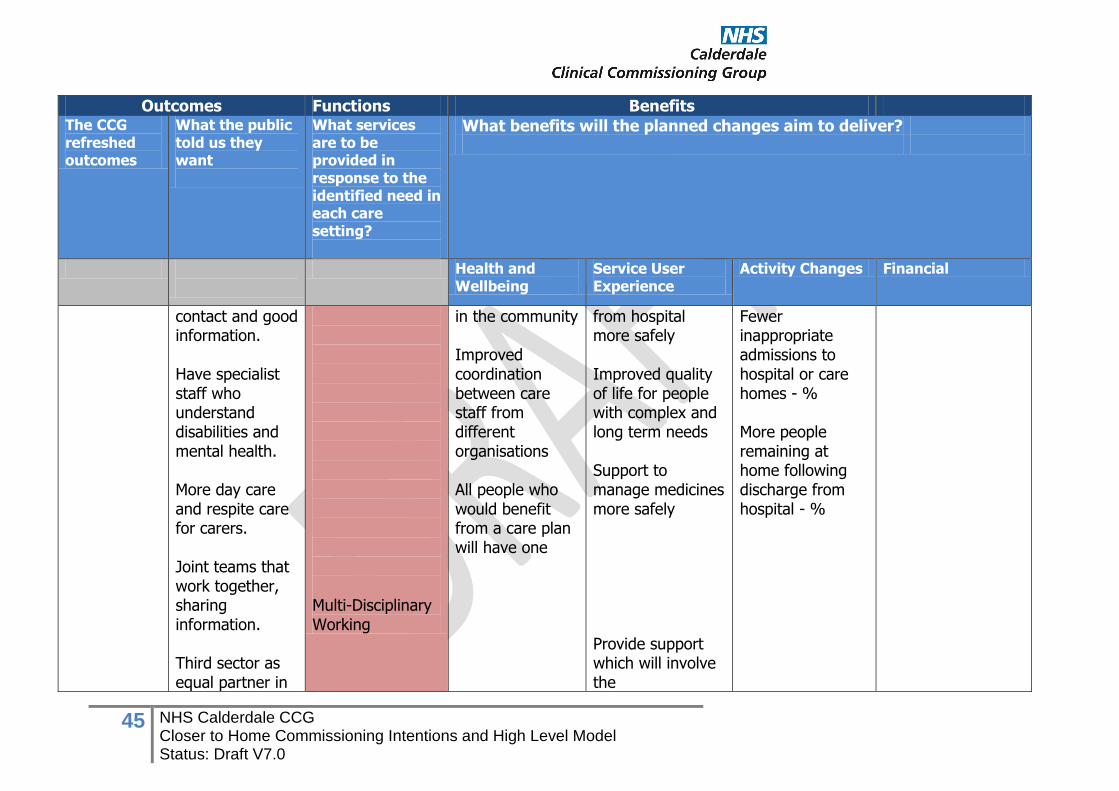
45 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Outcomes Functions Benefits The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
contact and good information. Have specialist staff who understand disabilities and mental health. More day care and respite care for carers. Joint teams that work together, sharing information. Third sector as equal partner in
Multi-Disciplinary Working
in the community Improved coordination between care staff from different organisations All people who would benefit from a care plan will have one
from hospital more safely Improved quality of life for people with complex and long term needs Support to manage medicines more safely Provide support which will involve the
Fewer inappropriate admissions to hospital or care homes - % More people remaining at home following discharge from hospital - %
46 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Outcomes Functions Benefits The CCG refreshed outcomes
What the public told us they want
What services are to be provided in response to the identified need in each care setting?
What benefits will the planned changes aim to deliver?
Health and Wellbeing
Service User Experience
Activity Changes Financial
delivering support.
person’s/family’s natural circle of support and maximize the use of the community assets
1 NHS Calderdale CCG Closer to Home Commissioning Intentions and High Level Model Status: Draft V7.0
Title Calderdale Health and Social Care Service Change Proposal
Owner Closer to Home Programme Board
Purpose of Document To describe the commissioning Intentions and High Level Model for the Closer to Home Programme
Status DRAFT
Version Number 7.0
Document Reference Number N/A
Date 5th August 2014
Author(s) DG, RR, LK, TS, LB, JT, AB, LS
Circulated to Calderdale CCG Governing Body
Date of Approval by 13th August 2014
Version Control
Version Number
Revision Date Changes Made By Summary of Changes Circulation Date
1.0 27 June 2014 Laura Kennedy Created and shared with Programme Board
27 June 2014
2.0 Various Further sections added
3.0 18 July 2014 Laura Kennedy Section 2.5, 2.6 drafted 18 July 2014
4.0 29 July 2014 Laura Kennedy Section 4.0, 6.0 drafted 31 July 2014
4.1 31 July 2014 Laura Kennedy Appendix B added
5.0 1 August 2014 Laura Kennedy Amendments following Closer to Home PB
1 Aug 2014
6.0 4 August 2014 Laura Kennedy Amendments following comments from Programme Board members
4 Aug 2014
7.0 5 August 2014 Laura Kennedy Amendments made following Calderdale SMT
5 Aug 2014
Distribution/Approval list
Formal Reviewers Role and Review Responsibility Signature
Sign-off Reviewer Role and Review Responsibility Signature
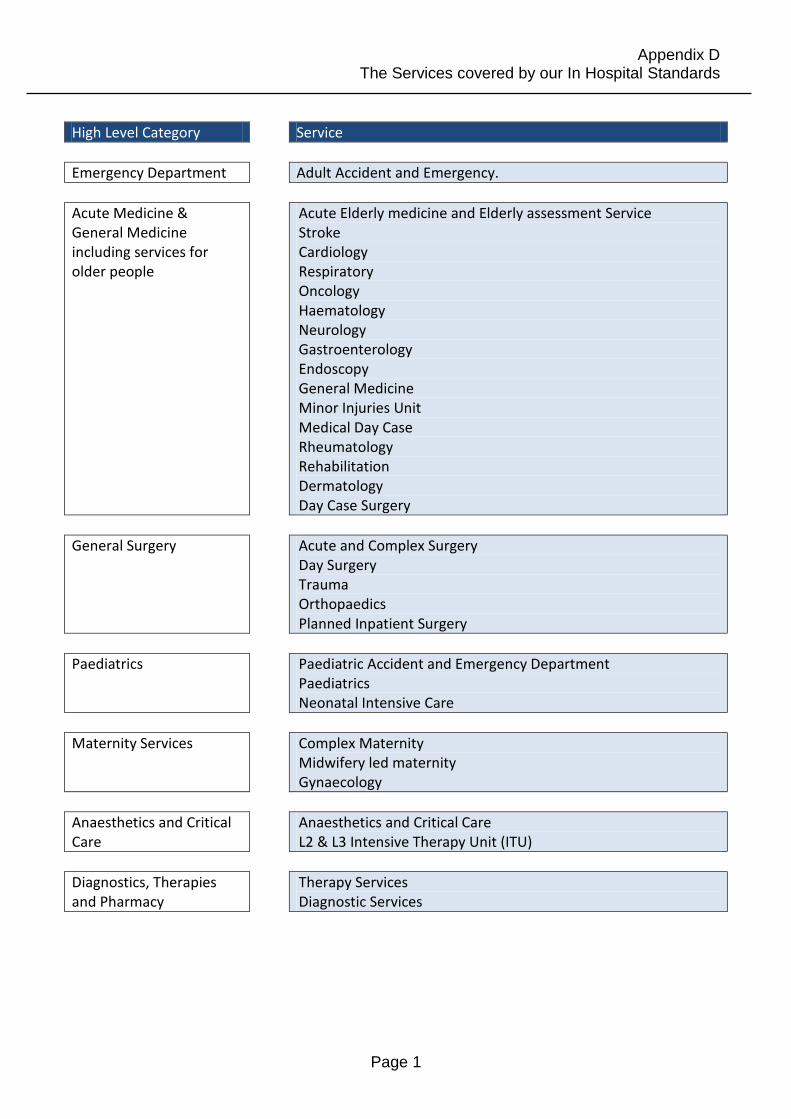
Appendix D The Services covered by our In Hospital Standards
Page 1
High Level Category Service
Emergency Department Adult Accident and Emergency.
Acute Medicine & General Medicine including services for older people
Acute Elderly medicine and Elderly assessment Service Stroke Cardiology Respiratory Oncology Haematology Neurology Gastroenterology Endoscopy General Medicine Minor Injuries Unit Medical Day Case Rheumatology Rehabilitation Dermatology Day Case Surgery
General Surgery Acute and Complex Surgery Day Surgery Trauma Orthopaedics Planned Inpatient Surgery
Paediatrics Paediatric Accident and Emergency Department Paediatrics Neonatal Intensive Care
Maternity Services Complex Maternity Midwifery led maternity Gynaecology
Anaesthetics and Critical Care
Anaesthetics and Critical Care L2 & L3 Intensive Therapy Unit (ITU)
Diagnostics, Therapies and Pharmacy
Therapy Services Diagnostic Services
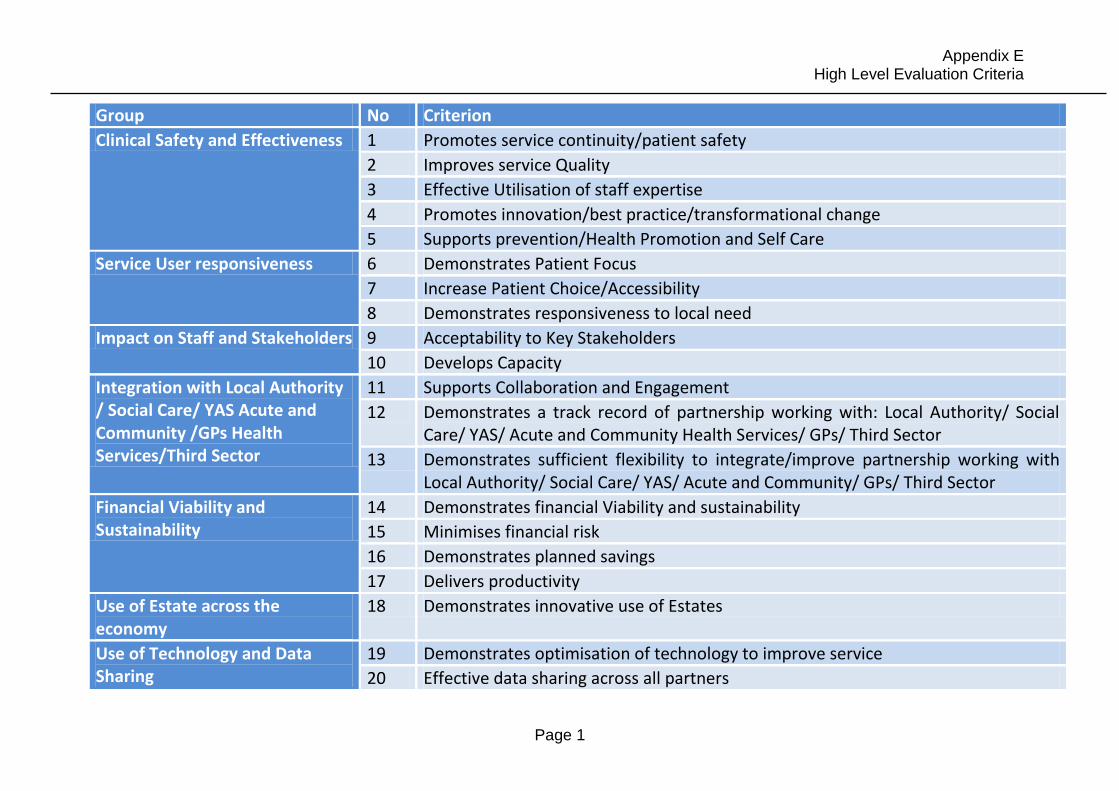
Appendix E High Level Evaluation Criteria
Page 1
Group No Criterion
Clinical Safety and Effectiveness 1 Promotes service continuity/patient safety
2 Improves service Quality
3 Effective Utilisation of staff expertise
4 Promotes innovation/best practice/transformational change
5 Supports prevention/Health Promotion and Self Care
Service User responsiveness 6 Demonstrates Patient Focus
7 Increase Patient Choice/Accessibility
8 Demonstrates responsiveness to local need
Impact on Staff and Stakeholders 9 Acceptability to Key Stakeholders
10 Develops Capacity
Integration with Local Authority / Social Care/ YAS Acute and Community /GPs Health Services/Third Sector
11 Supports Collaboration and Engagement
12 Demonstrates a track record of partnership working with: Local Authority/ Social Care/ YAS/ Acute and Community Health Services/ GPs/ Third Sector
13 Demonstrates sufficient flexibility to integrate/improve partnership working with Local Authority/ Social Care/ YAS/ Acute and Community/ GPs/ Third Sector
Financial Viability and Sustainability
14 Demonstrates financial Viability and sustainability
15 Minimises financial risk
16 Demonstrates planned savings
17 Delivers productivity
Use of Estate across the economy
18 Demonstrates innovative use of Estates
Use of Technology and Data Sharing
19 Demonstrates optimisation of technology to improve service
20 Effective data sharing across all partners





























