Embed Size (px)
Citation preview

J Clin Pathol 1994;47:269-271
Atypical progression of multiple myeloma withextensive extramedullary disease
S N Jowitt, A Jacobs, P A Batman, D A Sapherson
AbstractMultiple myeloma is a neoplastic dis-order caused by the proliferation of atransformed B lymphoid progenitor cellthat gives rise to a clone ofimmunoglobu-lin-secreting cells. Other plasma celltumours include solitary plasmacytomaof bone (SPB) and extramedullary plas-macytomas (EMP). Despite an apparentcommon origin there exist pathologicaland clinical differences between theseneoplasms and the association betweenthem is not completely understood. Acase of IgG multiple myeloma that pre-sented with typical clinical and labora-tory features, including a bone marrowinfiltrated by well differentiated plasmacells, is reported. The tumour had anunusual evolution, with the developmentof extensive extramedullary disease whilemaintaining mature histological features.
(7 Clin Pathol 1994;47:269-271)
Department ofHaematology,Bradford RoyalInfirmary, Bradford,West Yorkshire, BD96RJS N JowittA JacobsDepartment ofHistopathologyP A BatmanDepartment ofRadiologyD A SaphersonCorrespondence to:Dr D A SaphersonAccepted for publication7 September 1993
Case reportA 67 year old man of Indian descent pre-sented with a three month history of low backpain. Physical examination was unremarkable.Plain films of the lumbar spine revealed a lyticlesion in the vertebral body of L3 associatedwith end plate collapse; lateral views showedan abnormal soft tissue mass anterior to thesame vertebral body. A skeletal survey identi-fied multiple lucent areas in the skull vault butno additional lytic lesions were seen else-where. The diagnosis of multiple myelomawas confirmed by the following investigations:electrophoresis revealed an IgGX paraprotein(quantitated at 50 gil) in the serum and free X
light chains in the urine; a bone marrow aspi-rate contained 27% myeloma cells in the formof well differentiated plasma cells.
After receiving local radiotherapy to thelumbar spine the patient was given melphalan(10 mg/day for seven days) and prednisolone(40 mg/day for seven days), repeated atmonthly intervals. The plateau phase wasreached after 12 courses of the aforemen-tioned chemotherapy (paraprotein concentra-tion 3 g/l) and treatment was discontinued.Two months later the patient presented
with central abdominal discomfort. Physicalexamination yielded normal results. Anabdominal ultrasound scan showed an hypoe-choic mass measuring 6 cm in diameter andsituated anteriorly to the lumbar spine; nor-mal kidneys and pancreas were identified.
Plain films confirmed that this was the
same soft tissue mass identified at presenta-tion and implied the mass represented soft tis-sue extension of myeloma. After four weeks ofclinical observation the abdominal mass hadbecome palpable and the serum paraproteinhad risen to 13 g/l. The patient was againgiven melphalan (10 mg/day for five days) andprednisolone (40 mg/day for five days) andlocal radiotherapy to the abdominal mass.The mass became impalpable and after fourfurther courses of chemotherapy the serumparaprotein had fallen to 4 g/l.
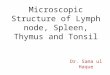
Six weeks after completion of the fifthcourse of melphalan and prednisolone thepatient re-presented with abdominal pain anda mass was palpable in the right hand side ofthe abdomen. Investigations of note were asfollows: haemoglobin concentration 88 g/l;white cell count 1-9 x 109/1 (differential ofneutrophils 1-3 x 109/l, lymphocytes 0*4 x109/l, monocytes 0-2 x 109/l); platelet count of71 x 109/1; paraprotein concentration 15 g/l;bone marrow aspirate was diluted with bloodbut a trephine biopsy specimen revealed ahypocellular marrow with reduced normalhaemopoiesis and foci of plasma cells.Circulating plasma cells were not detected atany stage. An abdominal ultrasound scandetected a mass in the right para-aortic regionand another anterior to the splenic vein; theright kidney also appeared to have been com-pletely replaced by abnormal tumour tissue.An ultrasound guided biopsy specimen of theright renal mass was obtained, the histology ofwhich showed sheets of plasma cells withareas of necrosis with no renal tissue identi-fied. A computed tomogram of the abdomenwas performed and relevant abnormalities areshown in fig 1.The serum paraprotein rose to a concentra-
tion of 19 g/l over the course of one week andthe patient's general condition began toworsen. Haemopoietic recovery was delayedand the patient was given methylprednisolone(1.5 g/day for five days). He developedsymptoms and signs of pulmonary sepsisand was given broad spectrum antibiotics.Unfortunately, he continued to deteriorateand died 10 days later. Two days earlier hisserum paraprotein had measured 31 g/l.
Post mortem examination confirmed thepresence of bronchopneumonia together withevidence of disseminated tumour of the rightkidney, pancreas, porta hepatis, serosa of thetransverse colon, pelvic and left perirenal fat,left-sided ribs, and left parietal pleura.
Histological examination showed amonomorphic diffuse infiltrate of plasma-cytoid cells with little supporting stroma
269
on March 12, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.47.3.269 on 1 March 1994. D
ownloaded from

2owitt, Jacobs, Batman, Sapherson
Figure 1 Computedtomogram ofabdomen andpelvis after intravenouscontrast.(A) At level Ll is anextensive retroperitonealmass replacing thepancreas and invading theright kidney. There arefurther masses anterior andposterior to the left kidney.(B) At the level of therenal hila are severalmasses in the base of themesentery and almost noopacification of the rightkidney, implying loss offunction due to invasion.(C) At level L4 is anecrotic mesenteric massand also several peritonealdeposits (arrows). (D)Several soft tissue masses(arrows) around thesigmoid colon in the pelvis.
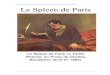
(fig 2A). The neoplastic cells showed typicalplasma cell features with an eccentric nucleusand perinuclear hof. Immunoperoxidase stain-ing showed k light chain restriction (fig 2B).
DiscussionWe have described a case of multiplemyeloma which, after an initial response tochemotherapy, progressed in an atypicalmanner, with the development of multipleextramedullary plasma cell tumours affectingthe right kidney, pancreas, porta hepatisserosa of the transverse colon, pelvic and leftperi-renal fat, left-sided ribs and left parietalpleura.
Multiple myeloma generally presents dueto the result of dissemination of malignantplasma cells throughout the bone marrow andthe effects of the excessive amount of mono-clonal protein they produce. The primaryfocus of the tumour is not usually evident. Itis not uncommon to see the effects of extra-osseous extension of intramedullary tumournodules as a result of erosion of the cortex andsubsequent spread beyond the periosteum,although soft tissue involvement itself isunusual except in the rare IgD multiplemyeloma.I In the case we have described therewas radiological evidence of spread from theL3 vertebral body, but no clinical evidence ofany other soft tissue disease at presentation.Relapse from a plateau phase in multiplemyeloma is most often manifest by impair-ment of bone marrow function together withthe reappearance and gradual increase in theconcentration of the paraprotein. In someinstances locally aggressive tumours develop.These tend to arise in pre-existing bonylesions rather than in soft tissue sites.
Although microscopic disease of the spleen,liver, or lymph nodes is found in up to 70% ofcases at post mortem examination the pres-ence of gross extramedullary tumour forma-tion at other locations is less common andrarely involves more than a single site.' Thepattern of spread shown in our case is veryunusual for multiple myeloma. In an extensiveliterature search we have been able to findonly one report of multiple myeloma withcomparable features. Foucar described twocases of multiple myeloma that developedprominent extramedullary disease at multiplesites one and four years after initial diagnosis.3However, one was of an IgD subtype andboth cases had anaplastic features and seemedto represent a variant of multiple myelomawhich resulted from a transformation of welldifferentiated myeloma cells to poorly differ-entiated immunoblastic-like cells. In contrast,the multiple extramedullary tumours in ourcase were all composed of cells with featuresof plasmacytoid differentiation.The association between the different cate-
gories of plasma cell tumours has been thesubject of much debate." Solitary myelomaof bone (SMB) usually presents as a locallypainful lesion with no evidence of widespreaddissemination of plasma cells in the bone mar-row, although in 10-20% of cases monoclonalprotein is detected.5 However, there is a highrate of conversion to multiple myeloma fol-lowing successful treatment of the primarylesion.6 Yentis proposed that all cases of SPBrepresented early multiple myeloma.7 Thestrong similarity between multiple myelomaand the disseminated stage of SPB was alsonoted in an extensive review by Wiltshaw,who supported the hypothesis that SPBrepresented the same pathological process as
270
on March 12, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.47.3.269 on 1 March 1994. D
ownloaded from

Atypical progression of multiple myeloma with extensive extramedullary disease
Figure 2 (A) Low power view of tissue obtainedfrom ight kidney at post mortemexamination showing diffuse infiltration by tumour cells (haematoxylin and eosin).(B) High power view ofsame tissue as in (A). The tumour cells show plasmacytoidfeatures and A light chain restriction (immunoperoxidase stain).
multiple myeloma.5 Although our casedemonstrated radiological evidence of extra-osseous spread from the vertebrae at presenta-tion, the clinical history was short and we feelit is unlikely that the patient's disease hadevolved from an SPB at that site.The evolution of our patient's disease was
unusual in that the pattern of spread followingrelapse from the plateau phase was similar tothat seen in some cases of extramedullaryplasmacytoma (EMP) in which relapse isoften associated with the event of spread. Thedevelopment of successive, multiple asynchro-nous EMP at different localisations has alsobeen described.8 However, in her reviewWiltshaw considered that the behaviour ofEMP reflected a malignant process distinctlydifferent from multiple myeloma or SPB.5
At presentation our case demonstratedfeatures that satisfied the generally acceptedcriteria to establish a diagnosis of multiplemyeloma of IgG subtype. However, webelieve the atypical clinical course disclosedfeatures not hitherto reported in IgG multiplemyeloma and underscores the complexity ofthe plasma cell dyscrasias.
We thank Dr K M Hunt for allowing us to report this case.
1 Jancelwicz Z, Takatsuki D, Sugai S, Pruzanski W: IgDmyeloma. Review of 133 cases. Arch Intern Med 1975;135:87-93.
2 Hayes DW, Bennett WA, Heck FJ. Extramedullary lesionsin multiple myeloma. Review of literature and patho-logical studies. Arch Pathol 1952;53:262-72.
3 Foucar K, Raber M, Foucar E, Barlogie B, Sandler CM,Alexanian R Anaplastic myeloma with massiveextramedullary involvement. Cancer 1983;51:166-74.
4 Knowling MA, Harwood AR, Bergsagel DE. Comparisonof extramedullary plasmacytomas with solitary and mul-tiple plasma cell tumours of bone. J Clin Oncol 1983;1:255-62.
5 Wiltshaw E. The natural history of extramedullary plasma-cytoma and its relation to solitary myeloma of bone andmyelomatosis. Medicine 1976;55:217-38.
6 Corwin J, Lindberg RD. Solitary plasmacytoma of bonevs. extramedullary plasmacytoma and their relationshipto multiple myeloma. Cancer 1979;43:1007-13.
7 Yentis I. The so-called solitary plasmacytoma of bone. JFac Radiol 1957;8:132-44.
8 Bauduer F, Tanguy A, Mandard AM: Plasmacytoma withasynchronous metastasis. Immunological and ultrastruc-tural contribution. Arch Anat Cytol Pathol 1992;40:23-7.
271
on March 12, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.47.3.269 on 1 March 1994. D
ownloaded from