Embed Size (px)
Citation preview

Volume 2 • Issue 4 • 1000142J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Ansari and Khan, J Community Med Health Educ 2012, 2:4 DOI: 10.4172/2161-0711.1000142
Research Article Open Access
An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year ExperienceM. Athar Ansari* and Z. Khan
Department of Community Medicine, J.N. Medical College, Aligarh Muslim University, Aligarh, India
AbstractBackground: Eating establishments provide food on a large scale and are important from the point of view
of epidemiology of food borne diseases in the community. They have been identified as an important source for contamination of food and food borne disease outbreaks. Eating at these places significantly increases the risk of diarrhea among consumers.
Objectives: The present study was carried out with the following objectives:
(1) To find out the socio-demographic characteristics of food handlers working in eating establishments.
(2) To assess the impact of health education intervention on hygienic status of food handlers.
Methods: The present longitudinal study was carried out by interview method during academic session from 2008-2009 to 2010-11 (3 Years) among 701 food handlers including cooks, helpers and waiters/ bearers employed by 18 kitchens establishments. IEC material and power point presentation was used for imparting health education. Data was collected, tabulated and analyzed statistically using appropriate tests of significance.
Results: Majority of food handlers (36.8%) belonged to age group of 18-30 years followed by 31 to 40 years (30.8%). There were 95.6% male workers and only 4.4% female worker, employed mainly in girl’s hostel. Majority of workers were illiterate (41.1%). Apron and caps were not used by most of them (84.5%) but the dresses were clean. Hands and nails were clean in large number of participants (69.9%). 59.8% workers were not addicted to any type of tobacco. On an arbitrary scale of hygiene, general conditions were satisfactory in 63.7% food handlers. Overall hygiene status of the food handlers improved during the three years (2009 to 2011).
Conclusion: There was marked improvement among food handler’s knowledge, attitude and practice towards personal hygiene. Certain steps should be taken to improve the status of food hygiene in food service establishments like banning smoking and the use of all tobacco products during food handling. Strict periodical examination for early identification of morbid conditions should be carried out.
*Corresponding author: Dr. M. Athar Ansari, Associate Professor, Department of Community Medicine, J.N. Medical College, Aligarh Muslim University, Aligarh, India-202002, Tel: +91-9897267621, E-mail: [email protected]
Received March 07, 2012; Accepted April 21, 2012; Published April 23, 2012
Citation: Ansari MA, Khan Z (2012) An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year Experience. J Community Med Health Educ 2:142. doi:10.4172/2161-0711.1000142
Copyright: © 2012 Ansari MA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords: Food handler; Hygienic status; Kitchen establishments;Tobacco addiction
IntroductionFood is an important basic necessity, its procurement, preparation
and consumption is vital for the sustenance of life. However, diseases spread through food are common and persistent problems results in appreciable morbidity and occasionally in death [1]. Eating establishments provide food on a large scale and are important from the point of view of epidemiology of food borne diseases in the community. They have been identified as an important source for contamination of food and food borne disease outbreaks. Eating at these places significantly increases the risk of diarrhea among consumers [2].
The explosive nature of gastrointestinal diseases generates the public reaction and attention of health authorities. These diseases are the major public health problems in developing countries including India, resulting in high mortality. Diarrheal diseases kill an estimated 1.9 million people annually in the world. Even in developed countries, an esti mated one-third of the population is affected by microbiological food borne diseases each year [3].
Numerous control strategies are in place but person-to-person disease transmission has not ceased. Food handlers play an important role in ensuring food safety throughout the chain of production, processing, storage and preparation.
To prevent the episodes of these diseases, food should be prepared hygienically using safe food handling practices. Cooked food should be stored in cold storage to prevent growth of the microorganisms. Food sanitation should be followed in the kitchen like adequate work space,
light and ventilation. There should be washing facilities and garbage disposal system.
Food handlers should observe high standards of personal hygiene in the handling, preparation and cooking of food. They should avoid the direct handling of ready to serve food items with bare hands. They should practice hand washing with soap and water especially after toilet. Food handlers should be screened periodically for the presence of apparent or inapparent infection responsible for food poisoning [3]. Those suffering from infected wounds, boils, diarrhea, dysentery, throat infection should be excluded from food handling. Health education given to the food handlers is the most cost effective measure to prevent episodes of diarrheal diseases in the community.
Keeping in mind the above facts, the present study was carried out with the following objectives:
1. To find out the socio-demographic characteristics of foodhandlers working in eating establishments.
Jour
nal o
f Com
munity Medicine & Health Education
ISSN: 2161-0711
Community Medicine & Health Education

Volume 2 • Issue 4 • 1000142J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Ansari MA, Khan Z (2012) An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year Experience. J Community Med Health Educ 2:142. doi:10.4172/2161-0711.1000142
Page 2 of 5
2. To assess the impact of health education intervention on hygienic status of food handlers.
Materials and MethodsThe district of Aligarh, (in the state of Uttar Pradesh) is situated
126 Kilometers south east of Delhi. As of 2011 India Census, Aligarh district had a population of 3,622,727 with a sex ratio of 951 females per 1000 males and literacy rate of 74.3%.
Aligarh is synonymous with the Muslim University that is spread across much of the city’s civil lines area. Aligarh Muslim University is a residential academic institution of international repute and draws students from all corners of the world, especially Africa, West Asia and South East Asia.
There are 16 halls and 2 schools of residence and each comprises 4 to 8 hostels. In each hall, there is a kitchen where breakfast, lunch and dinner are served. All students are supposed to get the food in the dining halls. Cooks and helpers work in shifts by rotation in the kitchen and bearers are employed to serve the food to the students in the dining room. Sometimes students take food outside the hall making them vulnerable to food borne diseases as food safety measures are not taken adequately in roadside dhabas (eating outlets).
An epidemic of gastroenteritis was reported in one of the hall in January, 2008 where large numbers of students were prescribed medicines in Out Patients Department (OPD) and few students were admitted In Patients Department (IPD) within a short period (Figure 1).
Following the epidemic, a high level Expert Committee on Health and Hygiene was constituted by the university authorities with the objectives:
1. To define the magnitude of epidemic in terms of time, place and person.
2. To determine the particular conditions and factors responsible for the occurrence of the epidemic.
3. Identify source of infection and mode of transmission in order to determine measures necessary to control the epidemic.
4. To make recommendations to prevent recurrence in future.
The committee visited the halls/schools of residence for physical inspection of the kitchen, water supply and waste disposal of the hall. We also carried out health checkups of the dining hall staff and assessed the bacteriological quality of water samples. The University Health Service was also visited to confirm the diagnosis of the disease and to confirm the existence of an epidemic.
Later on it was emphasized that survey and monitoring of kitchen establishments and health and hygiene appraisal of cooks, helpers and bearers should be continued periodically throughout the year. Therefore, this longitudinal study was carried out from February, 2009 to January, 2011. A team of health personnel, medico-social workers, lab technicians and medical interns visited all halls of residence on prior informed dates. In-charges of all halls were requested to make sure that all the workers should remain present on the day of visit along with senior students. They were given health education regarding prevention of epidemics of food born diseases and importance of personal hygiene and environmental sanitation. Information, education and communication (IEC) material used were poster and pamphlets in Urdu and Hindi and demonstrations by the team members like proper and correct method of hand washing. A power
point presentation was also shown to the workers showing hazards of smoking and importance of personal hygiene.
Each study subject was interviewed face to face at his/her workplace with the help of a pretested, semi-structured schedule after obtaining their informed consent. Those who were absent or did not want to be part of the study were not included in the study. Data were collected from all the study subjects by only two interviewers in order to reduce interobserver bias. Information collected, included socio-demographic and professional characteristics such as age, gender, religion, native place, literacy status, nature of job, duration in the profession, substance use, clothing and hygiene status etc. An arbitrary scale was developed for the assessment of hygiene status of kitchen staff (Annexure-I). A score of 6 and above was taken as good, 3 to 5 as satisfactory and status was poor if the score was less than 3 in
Source: Data from University Health Service, AMU, Aligarh, February 05, 2008
0
10
20
30
40
50
60
06.01
.08
07.01
.08
08.01
.08
09.01
.08
10.01
.08
11.01
.08
12.01
.08
13.01
.08
14.01
.08
15.01
.08
21.01
.08
22.01
.08
23.01
.08
24.01
.08
25.01
.08
26.01
.08
27.01
.08
28.01
.08
29.01
.08
30.01
.08
31.01
.08
OPDIPD
Figure 1: Epidemic of gastro-enteritis.
12.9
24.6
13.7
48.8
10 13.6 12.3
64.1
8.5 9.3 12
70.2
0
10
20
30
40
50
60
70
80
Smoker and Tobacco Chewer
Smoker only Tobacco Chewer only Non Smoker and Non Tobacco Chewer
2009 2010 2011
%
Figure 2: Pattern of tobacco addiction from 2009-2011.
2.7
63.7
33.6
9.1
41.4
49.5
3.7
35.1
62.2
0
10
20
30
40
50
60
70
Poor Satisfactory Good
2009
2010
2011
%%
Figure 3: Change in the hygiene status from 2009-2011.

Volume 2 • Issue 4 • 1000142J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Ansari MA, Khan Z (2012) An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year Experience. J Community Med Health Educ 2:142. doi:10.4172/2161-0711.1000142
Page 3 of 5
these workers. Quality of data was assessed and shortcomings were rectified.
Ethical clearance
Ethical clearance was obtained from the Institutional Ethical Committee of J.N. Medical College, Aligarh Muslim University, Aligarh and the objectives of the study were explained to the study participants to get their informed verbal consent.
ResultsTable-1 shows the distribution of study population by age.
Out of 701 employees, majority of the subjects (36.8%) were in the age group of 18-30 years followed by 31-40 years (30.8%) and 41-50 years (21.3%) age groups. It can be also seen in Table-1, most of the subjects were males 670 (95.6%) and females comprised
only 31 (4.4%) of the study population. 41.1% of subjects were illiterate. 145 (20.7%) were having literacy status up to primary level followed by middle school (15.7%) and up to 10th standard (11.1%). Mostly the employees in the age group of 21-30 years were literate and older people were comparatively less literate or illiterate. As far as clothing is concerned, out of 701 employees interviewed, 592 (84.5%) did not wear apron and caps but their dresses were clean. 43 employees (6.3%) wore dirty clothes while clean aprons and caps were seen in 66 (9.4%) workers. We found that cleanliness of the clothes improved significantly from 1.2% in 2009 to 13.8% in 2011(X2 = 29.0, d.f.=01, p < 0.001) (Table-2).
In Table-2, it can also be seen that large number of the food handlers (69.9%) had clean and trimmed nails, 23.1% subjects were having moderately dirty nails, while 7.0% workers had black and dirty nails. There was gradual improvement in nail hygiene as percentage of
S. No. Age Group (Years) 2009 2010 2011 TotalNo. % No. % No. % No. %
1. 18-30 87 34.0 82 37.3 89 39.6 258 36.82. 31-40 89 34.8 62 28.2 65 28.9 216 30.83. 41-50 50 19.5 50 22.7 49 21.8 149 21.34. 51-60 30 11.7 26 11.8 22 9.8 78 11.1
Sex1. Male 248 96.9 203 92.3 219 97.3 670 95.62. Female 08 3.1 17 7.7 06 2.7 31 4.4
Education1. Illiterate 115 44.9 94 42.7 79 35.1 288 41.12. Just Literate 31 12.1 12 5.4 23 10.2 66 9.43. Primary 71 27.7 45 20.5 29 12.9 145 20.74. Middle 12 4.7 47 21.4 51 22.7 110 15.75. High School 25 9.8 20 9.1 33 14.7 78 11.16. Above H.S. 02 0.8 02 0.9 10 4.4 14 2.0Total 256 36.5 220 31.4 225 32.1 701 100.0
Table 1: Demographic profile of study population.
Table 2: Distribution of study population according to clothing and condition of nails.
S. No. Clothing 2009 2010 2011 TotalNo. % No. % No. % No. %
1. Dirty 11 4.3 38 17.3 17 7.6 66 9.42. No Apron and Caps but Clean Dress 242 94.5 173 78.6 177 76.9 592 84.53. Clean Apron and Caps 03 1.2 09 4.1 31 13.8 43 6.3
(X2 = 29.0, d.f.=1, p < 0.001)Condition of Nails
1. Black and Dirty 22 8.6 16 7.2 11 4.9 49 7.02. Moderately Dirty 74 28.9 43 19.5 45 20.0 162 23.13. Clean and Trimmed 160 62.5 161 73.2 169 75.1 490 69.9
(X2 = 8.8, d.f.=1, p < 0.01)Total 256 36.5 220 31.4 225 32.1 701 100.0
(X2 = 42.1, d.f.=1, p < 0.001)
Table 3: Distribution according to addiction.
S. No. Condition of Nails 2009 2010 2011 TotalNo. % No. % No. % No. %
1. Smoker and Tobacco Chewer 33 12.9 22 10.0 19 8.5 74 10.52. Smoker only 63 24.6 30 13.6 21 9.3 114 16.33. Tobacco Chewer only 40 13.7 27 12.3 27 12.0 94 13.44. Non Smoker and Non Tobacco
Chewer120 48.8 141 64.1 158 70.2 419 59.8
5. Alcoholism 00 0.0 00 0.0 00 0.0 00 0.0Total 256 36.5 220 31.4 225 32.1 701 100.0

Volume 2 • Issue 4 • 1000142J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Ansari MA, Khan Z (2012) An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year Experience. J Community Med Health Educ 2:142. doi:10.4172/2161-0711.1000142
Page 4 of 5
clean and trimmed nails improved significantly from 62.5% (2009) to 75.1% (2011) (X2 = 8.8, d.f.=1, p < 0.01). Percentage of black and dirty nails in food handlers had gone down from 8.6% (2009) to 4.9% (2011).
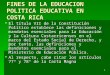
Out of 701 workers, 419 (59.8%) were non smoker and non tobacco chewer. 114 (16.3%) workers were smokers only. Only tobacco was chewed by 94 (13.4%) food handlers and remaining 74 (10.5%) were smoker and tobacco pan chewers. None of the worker was found to be addicted to alcohol. It was also observed that there was an impact of health education imparted to these food handlers as percentage of non smoker and non tobacco chewer improved from 48.8% (2009) to 70.2% (2011) and percentage of smoker and tobacco chewer declined from 12.9% (2009) to 8.5% (2011). Sharp decline in smoking habit of food handlers was noticed as percentage of smokers declined from 24.6% (2009) to 9.3% (2011) (Table-3, Figure 2).
In Table 4, Figure 3 general hygienic status of food handlers has been shown. It was based on total score achieved by each worker. In majority of food handlers it was good (47.8%) followed by satisfactory (47.5%) and hygienic status was found to be poor only in 33 employees (4.7%). There was marked improvement in the hygienic status of food handlers as good hygienic status had gone up from 33.6% (2009) to 62.2% (2011).
DiscussionIn the present study, most of the workers were males and belonged
to age group of less than 30 years and similar observations were made in a study conducted in Bijapur city where most of the respondents were also below 30 years [4,5]. In another study conducted in Gondar Town, Northwest Ethiopia, large majority (72.4%) of the food-handlers was young adults aged 20-40 years [6].
Most of the workers were males as mainly hostels were inhabited by male students and even in girls hostels, food handlers were mostly male because at a time, food for 700-900 girls were prepared at a time and it was difficult for the females to cook food for such a large numbers of students. Females were working mostly on compassionate ground where husband died. Similar observations were made in a study carried out in Delhi where only 2.6% of the study subjects were females [7].
Majority of subjects were literate but proportion of illiterate persons was also very high. Most of the illiterate food handlers were in the older age groups where there was no minimum education criterion at the time of the appointment nearly 30 to 40 years back. Mostly the young employees were literate. Similar observations were also made in Bijapur where majority of them were literate but proportion of literate workers was high as compared to present study and it could be due to the fact that they were employed in good hotels governed by the hotel associations [4]. However slight differences were reported by other researchers in their studies [8,9]. Now it has become mandatory to have minimum of 10th standard literacy level for a worker to be employed in public (government) sector.
As far as clothing is concerned, most of the employees did not wear
apron and caps but their dresses were clean. Proportion of workers with clean apron and caps was low however cleanliness of the clothes improved significantly from 2007 to 2009 and this could be attributed to the health education sessions carried out frequently in their working places. Some of them could not get the information about visit of the team otherwise they would come in clean clothes. Some of the workers might have clean clothes on the day of visit to escape criticism. All efforts should be made to ensure that workers should wear clean clothes as hands and clothes can spread harmful bacteria or viruses to food [10].
Majority of workers were non smoker and non tobacco chewer. However, sizeable numbers of food handlers were taking it in both forms. It was also observed that there was impact of health education imparted to these food handlers as percentage of non smoker and non tobacco chewer improved from 2009 to 2011 and percentage of smoker and tobacco chewer declined from 2009 to 2011. Sharp decline in smoking habit of food handlers was noticed over the three years. Those chewing tobacco were likely to affect food sanitation because of indiscriminate spitting or dribbling of secretion while talking, serving etc. Slightly higher figures were obtained in a study conducted in Amritsar where 53.7% were smokers, 11.2% tobacco chewer and 10.7% as betel chewer [11].
In the present study none of the workers was found addicted to alcohol while in the above mentioned study [11], alcoholism was high (23.4%) and it was attributed to the fact that our study was conducted in the Muslim majority population and in Islam, alcoholism is absolutely prohibited. No liquor shop, both country made and English is situated in and around campus within a radius of 5 Kilometer. If any worker is found having alcohol, he will not be allowed to work in the kitchen establishment. He may be transferred to other places as tube well operator or gate keeper. Since it is highly condemnable in our society, he may conceal that fact to escape the criticism or humiliation and subsequent transfer and it could be another reason for nil reporting of alcoholism in the present study.
Findings of this preliminary study may help in planning regular health education intervention programs for food handlers in order to have improvement in knowledge, attitude and practice towards food-borne diseases and food safety. It is recommended that education and training in good-hygiene practices should be provided to all food-handling personnel. Furthermore, if they are healthy, it will in turn reduce morbidity and mortality of food-borne diseases among themselves as well as population served by them. Education, training and the development of food safety certification examinations are key components in the process of ensuring that food handlers are proficient and knowledgeable about food safety and sanitation principles.
Based on the findings of the present study, it is further recommended that certain steps should be taken and enforced strictly to improve the status of food hygiene in food service establishments. These include banning smoking and the use of all tobacco products during food
(X2= 39.4, d.f.=1, p <0.001)
Table 4: Distribution of study population according to hygiene status.
S. No. Condition 2009 2010 2011 TotalNo. % No. % No. % No. %
1. Poor 07 2.7 20 9.1 06 3.7 33 4.72. Satisfactory 163 63.7 91 41.4 79 35.1 333 47.53. Good 86 33.6 109 49.5 140 62.2 335 47.8Total 256 36.5 220 31.4 225 32.1 701 100.0

Volume 2 • Issue 4 • 1000142J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Ansari MA, Khan Z (2012) An Evaluation of Health Education Intervention on Hygienic Status of Food Handlers in Aligarh - A Three Year Experience. J Community Med Health Educ 2:142. doi:10.4172/2161-0711.1000142
Page 5 of 5
handling, strict monitoring by the managers for proper hand washing, early identification of morbid conditions and urgent referral to health care facility, exclusion from food handling on a temporary basis during illness and pre-placement and regular in-service medical examinations including immunization against organisms causing enteric fevers and tetanus.
One limitation of the study was that, all the food-handlers could not be included in the study; otherwise results could have been more précised. However, findings of this study can be taken as base line information on the problem which may be carried out by other researchers who are interested in this domain.
References
1. The World Health Report (1998) Life in the 21st century-A vision for all. World Health Organization. Geneva.
2. Tjoa WS, DuPont HL, Sullivan P, Pickering LK, Holguin AH, et al. (1977) Location of food consumption and travelers’ diarrhea. Am J Epidemiol 106: 61-66.
3. Hedberg CW, MacDonald KL, Osterholm MT (1994) Changing epidemiology of food-borne disease: a Minnesota Perspective. Clin Infect Dis 18: :671-680; quiz 681-682.
4. Udgiri RS, Masali KA (2007) A study on the health status of food handlers employed in food establishments in Bijapur city. Indian J Community Med 32: 131-132.
5. Udgiri R, Yadavnnavar MC (2006) Knowledge and food hygiene practices among food handlers employed in food establishment of Bijapur City. Indian J Public Health 50: 240-241.
6. Andargie G, Kassu A, Moges F, Tiruneh M, Huruy K (2008) Prevalence of bacteria and intestinal parasites among food-handlers in Gondar Town, northwest Ethiopia. J Health Popul Nutr 26: 451-455.
7. Malhotra R, Lal P, Prakash SK, Daga MK, Kishore J (2007) Profile of food handlers working in food service establishments located within the premises of a medical college in Delhi, India. Public Health 121: 455-461.
8. Rathore AS, Sonker ML (1993) An evaluation of the health status of food handlers and sanitary status of the messes of a training establishment in Karnataka, Indian J Community Med 18: 21-25.
9. Chitnis UKB, Ganguli SK, Taneja RN, Ganguly SS (1986) An evaluation of the health status of workers of eating establishments in Pune cantonment. Medical Journal Armed Force India 42: 39-42.
10. Schuurkamp GJ, Bulungol PK, Kereu RK (1990) The monitoring of food handlers in Papua New Guinea. P N G Med J 33: 99-106.
11. Mohan V, Mohan U, Dass L, Lal M (2001) An evaluation of health status of food handlers of eating establishments in various educational and health institutions in Amritsar city. Indian J Community Med 26: 80-85.