Embed Size (px)
Citation preview

J Clin Pathol 1992;45:1023-1026
Intramammary lymph nodes
IH Jadusingh
AbstractAims: To determine the prevalence andpathology ofintramammary lymph nodesin breast specimens.Methods: AUl breast specimens examinedby a single pathologist over 70 months in alarge teaching hospital were studied retro-spectively. AUl the surgical pathologyreports were reviewed. Relevant glassslides from cases in which intramammarylymph nodes were identified were also re-examined.Results: Breast specimens (n = 682) wereexamined. Seven lymph nodes were foundin five patients. The specimens comprised533 biopsy specimens, 29 segmental resec-tions, 22 reduction mammoplasties, 77modified radical mastectomies and 20gynecomastia mastectomies. No clinicallyrelevant microscopical abnormalitieswere found in four lymph nodes and slightsinus histiocytosis was seen in two nodes.One node contained metastatic adeno-carcinoma and benign glandular epithe-lial inclusions.Conclusion: Although rare, intramam-mary lymph nodes may be detected bycareful gross examination ofbreast speci-mens even in the absence of clinical iden-tification. They can occur in any quadrantof the breast and can display a varietyof pathological conditions. Pathologistsshould be alert to the existence and poten-tial importance of these lymph nodes.
(7 Clin Pathol 1992;45:1023-1026)
The occurrence of lymph nodes in the breasthas not been extensively reported, even inanatomy textbooks. There is also a dearth of asingle source of information on the patho-logical importance of these lymph nodes.
Department ofLaboratory MedicineCalgary GeneralHospital, Calgary,Alberta, CanadaIH JadusinghCorrespondence to:Dr IH Jadusingh,Department of LaboratoryMedicine, Calgary GeneralHospital-BVC, 841 CenterAvenue East, Calgary,Alberta T2E OA1, Canada.
Accepted for publication3 June 1992
MethodsThe reports on all specimens of the breast inwhich the author performed a gross examina-tion were reviewed over 70 months.The hospital in which the cases were col-
lected is a fairly large, university affiliated,teaching hospital with close to 1000 beds. Thespecimens were received mainly from generalsurgeons, with a smaller number from plasticsurgeons, and the rare case from a generalpractitioner. Most patients had had surgerybecause of a clinically detected condition, but a
smaller number were from patients in whom an
abnormality had been detected by mammo-graphy.As a component of the gross pathological
examination, specimen mammography wasperformed on all cases in the following cate-gories: (a) lesions detected by screening; (b)biopsy specimens taken after a preoperativemammographic needle localisation; (c) mam-moplasty specimens in women aged over 30years; (d) biopsy specimens measuring morethan 3 0 cm in greatest dimensions, in whichthere was no grossly visible abnormality.
Gross examination was done in a routinemanner with inspection of the external aspectsand subsequent examination of thick slices(3-4 mm) of the entire specimen. Specialclearance techniques by fat dissolution werenot done. Whenever possible, the examinationwas done in conjunction with a review of themammographic films. Selected sections weretaken either for frozen sections, using a cryo-stat, or paraffin wax embedded sections. Thesewere stained with haematoxylin and eosin andan occasional case was stained with specialstains such as elastic van Gieson or periodicacid Schiff.
If the patient had more than one proceduredone at the same time, the case was categorisedby the larger specimen. A biopsy leading toimmediate mastectomy was counted as a mas-tectomy specimen. Tylectomies were classifiedas biopsies. Patients with multiple procedureswere counted as a single case.To evaluate the specimen size and type of
operation, the entire group was divided intobiopsy, segmental mastectomy, reductionmammoplasty, modified radical mastectomyand mastectomy done for gynaecomastiaspecimens.
ResultsA total of 681 cases were examined grossly.These comprised: 533 biopsy specimens, 29segmental resections, 22 reduction mammo-plasty specimens, 77 modified radical mastec-tomy and 20 gynaecomastia mastectomyspecimens. The male:female ratio was about1:29. The female patients ranged in age from14 to 92 years with a mean of44 years. Routinemicroscopical examination of paraffin waxembedded sections was done on all the casesand frozen section evaluation was done on 272cases. Microscopical examination did notreveal any lymph nodes that were not alreadyidentified by gross evaluation.Intramammary lymph nodes were found in
specimens from five patients. Surgery was
1023
on February 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.1023 on 1 Novem
ber 1992. Dow
nloaded from

1adusingh
done because of a clinically palpable mass thatwas suspicious of malignancy in three patientsand because of abnormal mammographic find-ings in two. None of the nodes had beenpalpated on clinical examination. Threepatients had a modified radical mastectomy,one a segmental mastectomy, and the other abiopsy (tylectomy). Of the three modifiedradical mastectomies, two were done for infil-trating duct carcinoma and the other, on theyoungest patient, was for a stromal sarcoma.
All the patients in whom intramammarylymph nodes were found were female. Theirages were 17, 43, 45, 51 and 75 years. Theyoungest (stromal sarcoma) and oldest (infil-trating duct carcinoma) each had two lymphnodes and a single node was found in each of
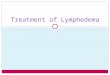
Figure I Preoperative fine wire localisation mammogram (nodule previously detected bya screening mammogram). Note smal lymph node partially obscured by the tip of thewire.
Analysis of specimens
IntramammaryBreast specimens lymph nodes
Biopsy specimens 533 1Segmental resections 29 1Reduction mammoplasties 22Modified radical mastectomies 77 5Gynaecomastia mastectomies 20Total 681 7 (5 patients)
the other three. Thus a total of seven lymphnodes was found in the five patients (table).The nodes were detected by pathologicalexamination in all except the 51 year oldpatient in whom the node presented as aclinically undetectable mass noted on a mam-mogram (fig 1). Specimen mammography,which was performed on selected cases, asdetailed previously, confirmed the presence ofthe single node that was detected by screeningmammography, but no additional nodes wereidentified.On gross examination the lymph nodes
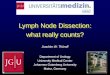
ranged in size from slightly less than 05 cm to1 0 cm in maximum diameter. All were pink,round, or slightly oval, solid, firm and welldemarcated from the surrounding breast par-enchyma. Their appearance somewhat resem-bled small fibroadenomas. All the nodes werelocated in the dorsal (posterior) third of thebreast (fig 2). Three were in the upper outer(lateral) quadrant, two in the lower outer(lateral) quadrant, and two in the lower inner(medial) quadrant.Microscopic examination of the lymph
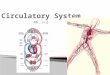
nodes revealed no clinically important abnor-malities in four nodes and slight sinus histiocy-tosis in two. One node showed the interestingfinding of a metastatic adenocarcinoma andareas interpreted to be benign glandular epi-thelial inclusions (figs 3 and 4). The metastasiswas apparently from an infiltrating duct carci-noma in a different area of the same breast.
DiscussionBy definition, intramammary lymph nodes aresurrounded by breast tissue and should bedistinguished from low axillary lymph nodes.1 2The fact that lymph nodes can be found in thebreast is probably not generally appreciatedand some standard textbooks of anatomy34and surgical pathology5 make no mention ofthem. The same deficiency occurs even in anarticle devoted exclusively to the anatomy andembryology of the breast.6 One popular bookon the pathology of the breast does notmention the structures,7 but a more recentpublication contains a short paragraph on thetopic.8 Haagenson describes "adventitious"and "pre-pectoral" nodes in his book ondiseases of the breast. His subsequent discus-sion on their locations suggests that the nodeshe is describing are not true intramammarylymph nodes.9 In contrast to this cursorycoverage, published findings on radiology,particularly the publications of Egan haveclearly defined these nodes. ' 2 The nodes were
1024
on February 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.1023 on 1 Novem
ber 1992. Dow
nloaded from

Intramammary lymph nodes
.1-1
..: ......
Figure 2 Close up view of a lymph node in the dorsal aspect of a modified radicalmastectomy specimen (grasped by forceps, at the tip of the arrow).
ws~_ee _.ix.t 9 i \ x t
Figure 3 Intramammary lymph node with benign glandular inclusions (arrow) andmetastatic adenocarcinoma (arrow heads). Inset: periphery of node with patent;ubcapsular sinus (haematoxvlin and eosin).N._~
4.q~
_^k . .^. t i.,,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-
44b
.. .Js
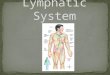
Figure 4 High power magnification offigure 3, showing benign glandular inclusions andmetastatic carcinoma (inset) (haematxylin and eosin).
detected by radiographical examination of5-0 mm thickness slices of "intact breast speci-mens". Surprisingly, pathological treatises inwhich the entire breast was examined do notmention these nodes, but it is difficult to tell ifthey were truly absent or if they were simplynot mentioned.'0-12The prevalence is difficult to assess. Egan's
showed the surprisingly high figure of 28% (45of 158 breasts). Five cases of normal intra-mammary lymph nodes were detected in 1030sonograms of palpable or mammographicallydetected breast masses by Gordon and Gilks. 13
Eighteen patients with 19 lymph nodes pre-sented with breast lumps over a six year periodat the Charing Cross Hospital.'4 In 108excisional biopsy specimens of occult breastmasses which were subjected to guided pre-operative needle localisations, six normal intra-mammary lymph nodes were detected at theMassachusetts General Hospital.'" Three caseswith metastatic carcinoma to intramammarylymph nodes occurring in 16 000 mammo-grams were reported from the MassachusettsGeneral Hospital.'6 A total of seven nodes infive patients were found in the present study of681 cases (see results section for case break-down). An estimate of the prevalence ofintramammary lymph nodes is difficultbecause of the variation in the methods ofanalysis in the aforementioned papers.The reported sizes vary from 0 3 cm to
3-0 cm in diameter. Most seem to be about1-0 cm in diameter. In most instances only asingle node is identified with a propensity to belocated in the upper outer quadrant, but asmany as nine have been reported involving allquadrants of the breast.2
Most intramammary lymph nodes are prob-ably detected by mammography and most willbe normal. This paper represents one of thefew reports in which the nodes were detectedon the basis of gross pathological examinationduring routine surgical pathology in contrast todetection in more careful studies using speci-men mammography of the entire breast.Pathological nodes may or may not be palpa-ble. Pathological conditions that have beenreported include metastatic carcinoma with aprimary in the ipsilateral breast, 2 carcinomasimulating medullary carcinoma without evi-dence of cancer in the mastectomy specimen orelsewhere,'6 fibrosis, lymphoid hyperplasia,sinus histiocytosis, melanin pigmentation(which may or may not be associated withother features of dermatopathic lymphadenop-athy)'7 fatty infiltration, a capsular naevus,'4tuberculosis,18 non-Hodgkin's malignant lym-phoma'9 20 and gold deposition simulatingmicrocalcifications on mammography in apatient who had received chrysotherapy forrheumatoid arthritis about 17 years earlier.2'Intramammary lymph nodes can be affected
by any disease that can involve lymph nodes inother areas of the body. Doubtless, becausetheir existence is difficult to detect, publica-tions on topics such as malignant lymphomasof the breast and medullary carcinoma donot, with rare exceptions,20 discuss thesenodes.22.28Although previous publications suggest that
1025
on February 11, 2021 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.45.11.1023 on 1 Novem
ber 1992. Dow
nloaded from

16adusingh
these structures have been largely ignored bypathologists, they will probably receive increas-ing attention as mammography for breastcancer screening becomes more widely used. Itis hoped that this publication will increaseawareness and prompt further studies on thepathological importance of intramammarylymph nodes.
Financial assistance was provided by the Calgary GeneralHospital.
I thank my secretary, Helen Mason, for her invaluableassistance in preparing the manuscript and Dr F Alexander,director, Department of Laboratory Medicine for funding.
1 McSweeney MB, Egan RL. Prognosis of breast cancerrelated to intramammary lymph nodes. Recent Res CancerRes 1984;90:166-72.
2 Egan RL, McSweeney MB. Intramammary lymph nodes.Cancer 1983;51: 1838-42.
3 Williams PL, Warwick R, Dyson M, Bannister LH, eds.Gray's Anatomy. Edinburgh: Churchill Livingstone,1989.
4 Basmajian JV. Grant's Method of Anatomy. Baltimore: Wil-liams & Wilkins, 1980.
5 Rosai J. Ackerman's Surgical Pathology. St Louis, Missouri,CV Mosby Company, 1989.
6 Morehead JR. Anatomy and embryology of the breast. ClinObstet Gynaecol 1982;25:353-7.
7 Azzopardi JG, Ahmed A, Millis RR. Major problems inpathology. Philadelphia: WB Saunders Company Ltd,1979.
8 Page DL, Anderson TJ, eds. Diagnostic histopathology of thebreast. Edinburgh: Churchill Livingstone, 1987.
9 Haagensen CD. Diseases of the breast. Philadelphia: WBSaunders Company, 1986.
10 Jensen HM. On the origin and progression ofhuman breastcancer. Obstet Gynecol 1986;154:1280-4.
11 Wellings SR, Jensen HM, Marcum RG. An atlas of subgross
pathology of the human breast with special reference topossible precancerous lesions. JNCI 1975;55:231-73.
12 Gallager HS, Martin JE. Early phases in the development ofbreast cancer. Cancer 1969;24: 1170-8.
13 Gordon PB, Gilks B. Sonographic appearance of normalintramammary lymph nodes. Y Ultrasound Med1988;7:545-48.
14 Dawson PM, Shousha S, Burn JI. Lymph nodes presentingas breast lumps. Br J Surg 1987;74:1 167-8.
15 Meyer JE, Kopans DB, Lawrence WD. Normal intra-mammary lymph nodes presenting as occult breastmasses. Breast 1982;8:30-2.
16 Lindfors KK, Kopans DB, McCarthy KA, Koerner FC,Meyer JE. Breast cancer metastasis to intramammarylymph nodes. Am J Rheum 1986;146:133-6.
17 Kopans DB, Mayer JE, Murphy GF. Benign lymph nodesassociated with dermatitis presenting as breast masses.Radiology 1980;137:15-9.
18 Arnaout AH, Shousha S, Metaxas N, Husain OAN.Intramammary tuberculous lymphadenitis. Histopathology1990;17:91-3.
19 Caimi F, Menozzi C, Freschi M. Localizzazione linfonodaleintramammaria di linfoma malign non-Hodgkin (Non-Hodgkin's malignant lymphoma in intramammarylymphnodal location). Radiol Med 1989;78:266-8.
20 Meis JM, Butler JJ, Osborne BM. Hodgkin's diseaseinvolving the breast and chest wall. Cancer1986;57: 1859-65.
21 Carter TR. Intramammary lymph node gold depositssimulating microcalcifications on mammogram. HumPathol 1988;19:992-4.
22 Jenstrom P, Sether JM. Primary lymphosarcoma of themammary gland. _AMA 1967;201:503-6.
23 Schouten JT, Weese JL, Carbone PP. Lymphoma of thebreast. Ann Surg 1981;194;749-53.
24 Telesinghe PU, Anthony PP. Primary lymphoma of breast.Histopathology 1985;9:297-307.
25 Wiseman C, Liao KT. Primary lymphoma of the breast.Cancer 1972;29:1705-12.
26 Jaffe ES. Surgical pathology of the lymph nodes and relatedorgans. Major Prob Pathol 1985;16:298-9.
27 Ridolfi RL, Rosen PP, PortAP, Kinne D, MikeV, Medullarycarcinoma of the breast. Cancer 1977;40:1365-85.
28 Mambo NC, Burke JS, Butler JJ. Primary malignantlymphomas of the breast. Cancer 1977;39:2033-40.
1026 on F
ebruary 11, 2021 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.45.11.1023 on 1 N
ovember 1992. D
ownloaded from