-
7/28/2019 j.1532-849X.1998.tb00185.x
1/7
Palato ram Assessment of MaxillaryCompH te DenturesDauid W
.FarlT, DDS,John D.Jones, DDS,2 and RobertJ . CroninDDS, S3
Phonetics, esthetics, function, and comfort form the foundation
of a successful dentalprosthesis.A revi ew of the mechanics of
speech as well as common speech prob lems encounteredwith a
removabl e maxillary prosthesis are presented. The use of a palato
gram o aid the clinician inthe assessment and resolution of speech
problems associated with a maxillary denture isdemonstrated.
J Prosthod 1998;7:84-90.Copyright0 1998by The American Collegeof
Prosthodontists.INDEXWORDS: palate, speech, phonetics
HONETICS,ESTEIETICS, functional efficiency,P nd comfort are key
elements of successhl com-plete denture treatment. All too often. a
thoroughevaluation of phonetics is neglccted as more empha-sis is
placed on the other three components. Optimalphonetics following
denture placement is dependenton the establishment of
physiologically accurate vcrti-cal dimension of occlusion, occlusal
plane, p d a t dcontour, and positioning of the anterior
teeth.b7
BackgroundIt has been stated that the primary functional
pho-netic role of a complete denture is to facilitate thestream of
air as it passes through the oral cavity.eSpeech sounds are noises
created by a combination oflaryngeal tone and airflow. Rothman
lists the follow-ing essential mechanisms of speech
production2:
Initintor-the motor speech area of the brain.Motor-the lungs and
associated musculature.Vibrator-expired air from the lungs cause
vibra-tions in the vocal cords yielding pitch and
tone.Resonatow-oral, nasal, and phaqiigeal catiticsintensify and
enrich the sound.
From the UniniDersitp f Texar Health Scierut Center at San
Antonio,GraduateProsfhodontirResiknt.2hsociatePmfasor.3AssociateProf.or,
Directorofportdoctoral Prosthodontics.Accepted March 12,
1998.Presented ar a table clinic at the I.996Annual SesrionofThe
Ammia n
CoUqea/Pro&?dontists,Kuruar Ci@; O .Correspondence to:
Rob&.]. Cronin, ODs, CniaersiQof Texas Health
Science Cmtrt at San Antonio, Ilefiartment vf Graduate
Pmsthodontics,7703FZyd CurlDT. San14nlonio.TX 8284-7912
DepartmentofProsthoduritics, Sun Antonio, TX.
Copyright 0 998ly The Amorkan
Collegeu/Prosthodontirts105~-g4rx/98/0702-00~4~~.OIO
5. Enwciators-the lips, tongue, soft palate, hardpalate, and
teeth add distinctncss and articulationto the speech sounds.The
tongue plays a major role in the formation ofspecch. The tongue
changes position and shape for
pronunciation of cach of the vowcls, with little or nocontact w
i t h other tissues. The tonLgucalso acts asthe principal
articulator of the consonants as itcontacts specific areas of the
teeth, alveolar ridge,and hard palate. For this reason, the
corisonantsounds are of greatest intcrcst to the
prosthodontist.Several classifications of speech sounds are
presentedin Table I .
This review will focus on those sounds formed byphonetic contact
betwccn the hard palate and thetongue that can be assessed with a
clinical palato-gram technique. These are known as
the@alatolinpalconfonants and consist of the S, T, D, N,
andLsounds. Tanaka studied the relationship betweenpalatal contour
and speech intelligibility. He notedthat in a sagittal section, the
natural anterior palateexhibits a rcvcrse curve. This contour is
crucial forpronunciation of the S and SH sounds. In acomparison
betcvccn the palatal contours of dentatepatients and acrylic resin
maxillary dentures, Tanakafound this prominence either deficient or
completelylacking in the majority of maxillary complete
den-tures.gAn alveolopalatal prominence should also be prc-sent
beginning at the premolar teeth and shouldbecome thicker as it
progresses distally to thc molars.This contour allows the tongue to
seal the posteriorpalatal denture surface and direct a flow of
airanteriorly. Many dentures feature a concavity on thepalatal
surface ust below the gingival margin insteadof this posterior
palatal prominence. Phonetic alter-ations occur when an airstrcam
escapes over one or
84 Journal ofPosthodonticr, Vol7,No 2 (June), 1998:pp 84-90
-
7/28/2019 j.1532-849X.1998.tb00185.x
2/7
June 1998, Volume 7 Nurnbn 2 85
Table 1. Classiticatioiis ofSpeech SoundsVuicelersSpcech S o u n
d (meuted by air u h e )
PlosivesAffricatives
Air is forced by the tongue through a narrow apertiire and s ,
sh , th , fis associated with ~ c t i o n&x@losioe release
ofair p, t , kA combination of the fiction and ex t i h i~ t e
lcnients ch
Voice Speech Sounds (created by laryngeallyproduced
noise)VowelsVoiccd ConsonantsClassification 4ccording to Anatomic
Sound Formation
Formed from continuour oocul cord oibrutiom; tongue and lipA
combinarioiiof air-producedsounds and laryngeal tone
a, e, i, o, ub, d, g, j, I, m, n, q, r, v,w, x , xpositions
impart structural overtones
PalatolingualTongue and hard palate The tonguc is positioned
just behind t h e maxillary incisorteeth with the sides of the
tongue in contact wi th themaxillary posterior teeth an d alveolar
ridgespalatesoft palatemandibiilar incisal edgesmaxillary incisor
teeth
s
Tongue and hard palate The tongue is placed firmly against the
anterior hard 1 d, n, 1Tongue and soft palate T h c posteriordorsal
tongue is raised to occlude wi th t h e
The tip ofThe tongue is placcd between the maxillary andFormed
by the lower lip contacting 1 h e iricisal cdges of the
k,g, ngthf,v
Linpoden a1LabiodentalBilabial These sounds are formcd between
the lips b, p, 171
both sides of the tongue when the tongue t ip is incontact wi th
the an terior denture palatc or when thetongue t ip cannot compress
the ai rs t ream betweenthe tongue and palatal dentu rc surface.
Allen s tatcdthat the most widely used procedure to improvcdenture
phonet ics is thc random thinning of theentire maxillary liiigual
surface to create m ore spacefor the tongue.1 Such arbitrary
removal of acrylicresin fiom the palatal surfacc ignores the
criticalimportance of correct palatal contours in the propcrformat
ion of sounds.
A patient receiving a new maxi llary dcn ture m aynoticc subtle
changes in the palatal contours. Suchchanges can be manifestcd as
phonet ic al terat ions ofthe pa latolingual conson ants,
especially the S sound.Typical alterations ar e a whistling Sor a
shift to anSh sound.? Th e S sound is Cornled by a s t ream ofair
escaping from th e m edial groovc of the tonguebehind the alveolus.
Th e s ides of the tongue a re incontact wi th th e m axil lary
posterior teeth and palatalden ture base.* The t ip of the ton
-
7/28/2019 j.1532-849X.1998.tb00185.x
3/7
86 Palatogram Rrsessrncnl Farlgy, ones, and Cronzn
Table 2. Common Palatolingual h ee c h ProblemsPossible Cuuw
Iliupnostic Procedure
~
Treatment1. Whistle on s soundsMedian tongue groove too deepAir
escape space in denture base tooMaxillary teeth set too far
labialInsufficient denture basc material on
lingual of maxillary anterio r teethPosterior leeth set too far
lingual
cramping the tongue spaceDenture base material tooprominent
causing median ,qoove to deepen
deepPalatogram assessmentAdd wax to anterior palate to
restoreAdd a wax incisive papilla (1 to 3-mm
Replace wax with acrylic resin ifwhistle is correctednormal
palatal s c u n ~height X 3 to 4-mm diameter )
Palatogram assessmentAdd wax to thicken cente r of palateRelieve
posterior denture baseAdd wax to anterior palate
~ ~ ~ ~ ~2. s sounds like shMedian tongue groove too shallow
Palatogram assessment Relieve anterior palatal denture base
and ai r escapes at lateral borders oftongucanterior teeth
Excessive denture base lingual toAnterior teeth set too far
lingualAir escaping at la teral tongue borders
due to insuficient denture basceminence lingual to posterior tee
th(stigmatismus lateralis)
Palatogram assessmentBuild up linLpal issue roll adjacent to
Replace wax with acrylic dentureresin
posterior tee th in wax
Note. Adapted h n l KuehkerWA Denture Problems: Causes,
Diagnostic Procedures, and Clinical Treatment.n W . Gagging
Problemsand Speech Problems. Quint Int
1984;12:1231-1238.Quintessence PublishingG o, Inc Copyright
holder.
certain sounds are pronounccd. T he palatogram isuseful at the
wax try-in appointment to assess properlingual contact with the
record base. It can also beused as a guide for the assessment of
phoneticalterations after placement of a maxillary prosthesis.
A palatogram assessment or denture palatal con-tours can be
beneficial when used with implant-supported maxillary dentures.
Deviation from idealpalatal contours are often encountered with
maxil-lary implant-supported dentures. This can bc causedby implant
an pl at io n problems, diminished restor-ative space, and bulky
attachment mechanisms. Thepalatogram can be an extremely useful
technique,alloming the clinician to determine the phoneticimpact of
the implant-affected contours.
Another indication for use of the palatogramtechnique is in the
cvaluation of maxillary dentureplaccment in the sensory- or
muscularly impairedpatient. An analysis of the space of Donder
inpatients suffering from a loss of motor function canbe simplified
by the use of a palatogram. A carefulevaluation of speech patterns
and food bolus manage-ment in the orally disabled or geriatric
patient mayinclude palatal contour assessment. The usc of
thepalatogram grcatly aids the communication between
the prosthodontist and the speech pathologist or
oralphysiotherapist in evaluating the problematic pa-ticnt.
Clinical TechniquesTo demonstratc the use of a palatogram, a
patientsmaxillary denture was duplicatcd. Two differentmaxillary
dentures were fabricated with modifiedpalatal contours representing
an undercontouredand a n overcontoured palate. The patients
denturewas uscd to represent a well-contoured palate. T h epatient
was then instructed to pronouncc certainpalatolingual sounds with
each of the three maxillaryprostheses, and the contacting surfaces
were re-corded.
According to the protocol set forth by Allen, allconsonants used
in making the palatograms werecombincd with thc vowel 0.hc 0ound
wasfound to be the only vowel that consistently had nopalatal
contact when pronounced. Because pronuncia-tion of the consonant
sounds alone involves two ormore sounds, and therefore two or more
tonguepositions, this prevented unwanted additional
palatalcontacts. For example, when pronouncing the T
-
7/28/2019 j.1532-849X.1998.tb00185.x
4/7
June 1998, Volume 7.Numbt-,2 87
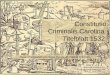
Figure 1. Complete denture sprayed with grecn Occludcmarker.
sound, the vowel sound ee is also made. Having thepatient say ~
o c o register the Tound creates amore accurate reproduction of the
desircd contactareas.
Palatograms were made using green Occludeaerosol (Pascal
Company, Inc, Bellewe, WA) as amarking media. All ingredients in
the Occlude prod-uct are listed as safe for ingestion. The green
Oc-clude material provided a distinctive contrast against
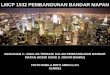
Figure3. Snormal-contoured palate. In a more anatomi-cally
correct dcnture palate, some of the marking materialhas been wipcd
away from the palatal surface by thetongue, in addition to wetting
t h e wrfa~:e.This is indicativeof an increase in contact
prcssure.the pink denture base and did not transfer to thepatients
tongue or intraoral tissues. The polishedpalatal and alveolar areas
of the dentures werccarefully sprayed with the Occlude marking
media.The patient was asked to repeat only the desiredsound two
consecutive times. The denture was thenpromptly removed and
assessed for contact. Ex-
Figure 2. S unciercontoured palate. Light ctintaci isseen
adjacent to the posterior teeth as the tongue has wetthe surface of
the marking material.
Figure 4. S overcontoured palate. Tissue contact hasincreased
further as indicated by the extent ofwetting bothanteriorly and
into the palatal vault area.
-
7/28/2019 j.1532-849X.1998.tb00185.x
5/7
88 Palatogram .4~te1\rnpnt a Far&, Jiints, and Cronzn
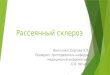
Figure 5 . T undcrcontoured palate. Light contact be-tween the
tongue and the acrylic resin palate is seen bothadjacent to the
posterior t eeth and in the antcrior palatearea.
~i~~~~ . y L,rrc:ontoured alate. H~~~ (:ontact in theanterior
palatal regiDn is indica ted by an irlcrease in thramount
,,fwetting o)rllle sprayed denture base.
amples of palatograms for the S and T soundsare demonstrated in
Figs 1 through 7. These photo-graphs reveal progressively
increasing contact withthe palate when comparing the undercontoured
den-
Figure6. Tnormal-contoured palate. A broader area ofcontact is
seen in the anterior palatal area when comparedwith the
undercontoured palatal surface. Also, some niark-ing material ha s
been wiped away from the palatal surfacesadjaccnt to thc posterior
teeth.
ture base with the normal and overcontoured palatesfor all
sounds tested. This is indicated both byincreased wetting of the
marking material by thetongue and the removal of the niarking
material incertain areas caused hy greater contact
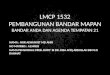
pressures.Additional line drawings are shown to
demonstraterepi-cscntativc palatograms for the T and Ssounds (Figs
8 and 9). Each individual will produce asimilar palatogram for a
given sound, but there willbe unique characteristics for that
particular pcrsoii.This is because individuals have anatomic
variationsin the shape and size ofthe tongue, palatal vault,
andarch form.
If it is dctermincd that some areas of palatalcontour are
deficient, an assessment as to the extentof deficiency can be made.
The palatal and alveolarareas of the maxillary denture a re lightly
coated withan alginate adhesive. i\ mix of alginate is thenprepared
usingvery cold water to retard the set ofthematcrial. A thin wash
of alginate is uniformly spreadover the palatal area of the denture
and smoothedwith a wet, gloved finger. The denture is quicklyplaced
into the patients mouth and the patient isallowed to speak using
various sound stimulus sen-tences. Table 3 lists various sound
stimulus sentencesuseful for this purpose.9 After the alginate has
set, aperiodontal probe can be inserted through thc algi-nate to
the acrylic denture base as seen in Fig 10.The
-
7/28/2019 j.1532-849X.1998.tb00185.x
6/7
June 1998, Volume 7,Number 2 89
Figure 8. Palatogram representative of the S sound. Figure 9.
Palatogram representative of the T, D,N, 3, nd Ch sounds.depth of
the alginate can serve as a guidc for accuratepalatal contouring.
To prevent excessive thickness ofthe alginate, the phonetic
displacement of the mate-rial should commence immediately after
insertion ofthe denture.
Conclusions1. Palatograms are helpful in the evaluation of
pho-
netics of th e complcte denture patient.2. Thc grecn marking
spray Occlude is a safe,
effective, and highly visible marking media for apalatogram.3.
The u se of alginate as a palatal disclosing media isu s e f d when
detcrrnining th e extent or a spacialdcficicncy.
Figure 10. Demonstration of measuring a palatogrammade with
irreversible hydrocolloid.Table 3. Sound Stimulus Sentences
Sound Sentencech Chuck is watching Butch.j Jane enjoyed th e
fudge.sh She is warhing the dkh.zh hlearurc the garage.
Sue is mining one piece.z Zelma is b i q .I Tom waded a bite.n
Ned won man y prixes.d Did W y ead?1 L ee will allow it.
Note. From Tanaka H . Speech Patterns of Edentulous Patientsand
Morphologyof the Palate in Relation to Phonetics.J ProsthetDent 1
973;29:16-28.
ReferencesI . Terrell 14 Fundamentals important to good complete
den-2. Rothman R Phonetic considerations in de nture prosthesis.J3.
Martone i v.. BlackJV: An approach to prosthodontics through
speech science: Part V.Speech science research ofprosthodon-tic
significance.J Prosthet De nt 1962;12:629-636
1.Palmer ,JM Analysis of speech in prosthodontic practice.
JProsthet Dent 1974:31:605-614
5. Palmer J M: tructural changes f n r speech improvement
incomplete upper denture fabrication. J Prosthet Dent
1979141:507-510
tin e construction.J Prosthet Dent 1958;8:710-753Prosthet Dent
1961:11:214-223
-
7/28/2019 j.1532-849X.1998.tb00185.x
7/7
90 Palatogram ilssessnzent Fa r ly , ones, and Cronin
6. Weir FS: Relating tooth positions in full dentures to the
oralvestibulc to obtain axu rac y of speech, esthetics, and ana
tomicI;rnction.JAm De nt Assoc 1932;19:1706-1712
7. Zarb GA: Rouchers Prosthodon tic Treatm ent for
EdentulousPatients. St. Louis, M O , C.V.Mosby (20, 1990
8. LandsJS: Practical Full Den ture Prosthesis. London,
DentalItems of Interest Publishing Co, 19.549. Tanaka H: Speech
patterns of edentulous paticnts and m or-
phology of the p alate in relation to phonetics.J Prosthet
Dent197329: 16-28
10. M e n L K Improved phonetics in denture construction.
JProsthet Dent 1958;8:753-63
1 . Sears VH: Principles and Techniques for Complete
DentureConstruction. St.Louis. MO,CVMosby Co , 1949
12. Slaughter MD: Speech correction in full denture
prosthesis.De nta l Digest 1945;51:242-246
13. Kuebker F$A Den ture Problems: Cau ses, Diagtgnostic
Proce-dures, and Clinical Treatm ent. IIm.Gagg ing problems
andSpeech Problems. Quint Int 1984;15:1231-1238