-
8/3/2019 Jacobus ECG Tips
1/19
ECGPrimer
ChristianJacobus,MD
RossUniversity
IntroductiontoClinicalMedicine
WhenIdictateECGsforapatientsmedicalrecord,Iusethefollowingformat:rate,rhythm,axis,
intervals,hypertrophy,ischemia.Forexample,Therateis60,therhythmissinus,axisisminus45
degrees,intervalsarenormal,thereisnoevidenceofhypertrophy,andnosignsofischemia.Sothat's
theorderinwhichI'mgoingtogooverthesetoday.
RateTherearetwoeasywaystofigureouttheheartratebylookingattheECG.
1)
StandardECGsrecordfor10secondssoaneasywaytocalculatetherateistocountthenumberofQRScomplexesononepageandmultiplybysixtogetthenumberinonefullminute.
(#QRScomplexesononepage)*(6)=BPM
2)
The300rule:countthenumberofbigboxesbetweentwoadjacentQRScomplexesanddivide300bythatnumber.Soonebigboxbetweencomplexeswillmeanaheartrateof300;twobig
boxeswouldbe150;threeis100;four
is75;fiveis60;sixis50.Thisismost
easilydonebyfindingonecomplexthat
fallsrightontoadarkerlineand
countingthenumberofbigboxesto
thenextQRScomplex.Ifthenext
complexfallsbetweenthelinesthen
youcanestimatebasedontheline
beforeandafter.Forexample,ifIfind
anR
wave
that
falls
right
on
adark
line,
andthenextRwavefallsbetweenfour
andfivebigboxeslater,thenIknowthe
rateisbetween75and60.Ifitscloser
tofourbigboxesthenImightestimate
70,closertofivebigboxesImightestimate65.
(300)/(#bigboxesbetween2adjacentQRScomplexes) =BPM
RhythmFirst,
some
basics.
The
Pwave
is
atrial
depolarization;
the
QRS
complex
is
ventricular
depolarization;theTwaveisventricularrepolarization(atrialrepolarizationoccursatthesametimeas
ventriculardepolarizationandsoislostintheQRScomplex).Whentheventriclesdepolarizenormally,
currentmovesthroughtheHisPurkinjesystem,specializedcellsthatconductelectricalchargequickly,
likeelectricalwiringfortheheart.Becausetheypropagatethatwaveofdepolarizationquickly,and
becausetimeequalshorizontaldistanceonECG,anormalQRScomplexisnarrow.
Incontrast,slowdepolarizationcausesawidenedQRScomplexbecausetimeisonthexaxisof
anECG,asstatedabove.Forinstance,whendepolarizationstartsintheventricularmyocardiumand
-
8/3/2019 Jacobus ECG Tips
2/19
spreadsfrommyocytetomyocyteitisnotusingtheHisPurkinjesystemandsodischargepropagates
moreslowly.TheothercauseforawidenedQRSisablockintheHisPurkinjesystem,delaying
depolarizationandwideningthecomplex.
SinusrhythmisaregularrhythmwithaPwaveoccurringbeforeeveryQRScomplex.TheseareheartbeatsthatoriginateintheSAnode.
JunctionalrhythmisanimpulsethatbeginsintheAVnoderatherthantheSAnode.IftheSA
nodeisdiseasedorischemicitwillnotfunctionproperly,causingtheAVnodetohavetotakeover
pacemakingduties.TheAVnodehasanintrinsicratethatisslowerthantheSAnode:4060bpm(vs.
theSAnodewhichis60100).ThesecomplexesdontusuallyhaveaPwavebecausethechargestarts
intheAVnodeandgoesdowntotheventricles.Atthesametime,thecurrentdoesgobackuptothe
atria,butbecausethisoccursatthesametimeastheventriculardepolarization,thePwaveislostinthe
QRScomplex.Ifthecurrentgetstotheatriaslightlybeforetheventricles,youmayseeinverted
(becausethewaveofdepolarizationisgoingup,ratherthandown)Pwavesimmediatelybeforethe
QRS.SoontheECGyoullseeslow,regular,narrowQRScomplexeswithnoPwavesbeforethemorinvertedPwaves.
Anidioventricularrhythmoriginatesinthemyocardiumoftheventriclesthemselves.Incases
wheretheSAnodeandtheAVnodearebothdiseasedorischemicandnotgeneratingimpulses,the
ventricularmyocyteshavetotakeover.Theirintrinsicrateis2040bpm.Becausethechargesarenot
travelingthroughtheHisPurkinjesystemthesecomplexeswillusuallybewideandbizarrelookingandtheratewillbeslow.
Atrialfibrillation:inthisrhythmtheatriahaveuncoordinatedelectricalactivity,kindoflike
they'rehavingaseizure.TheAVnodeisgettingbombardedwithelectricalsignalsbecauseofallthis
electricalactivity.WhentheAVnoderesetsfromthepreviousfiring,itisreadytofireagainandwilllet
thenextchargeitreceivesthrough,whichisthenconducteddowntotheventricles.Becausethecharge
goesthroughtheAVnode,therestofthechargeisconductednormally,propagatingdowntheHis
Purkinjesystem.AsaresulttheQRScomplexesarenarrow(i.e.normal).EverytimetheAVnoderesets
itwaitsforthenextcurrent,whichstartsthecycleoveragain.Becausetheelectricalactivityintheatria
-
8/3/2019 Jacobus ECG Tips
3/19
isuncoordinatedandunpredictablethenextchargecouldoccurinonemillisecondor1000.Thus,the
frequencywithwhichachargeissentdowntotheventriclestoactuallygenerateaheartbeatis
irregular.Sowhatyouseeisawavybaseline,causedbythefibrillatingatria,andirregular,narrowQRScomplexes.
SVT:thisisaprettynondescriptivename.SVTstandsforsupraventriculartachycardia,whichjust
meansanytachycardia(rategreaterthan100)causedbydischargesabovetheventricles.Soanything
fastand
coming
from
above
the
ventricles
would
qualify:
sinus
tachycardia,rapidafib,etc.Whatweusuallymeanwhenwe
saySVTisactuallyAVNRT:AVnodalreentrytachycardia.The
ideaisthatyouhaveapathwayinoraroundtheAVnode,
which,inadditiontoconductingthechargedownthelengthof
theventricles,alsoloopsbackuptowardstheAVnode.So
whentheAVnodefiresmostofthechargecontinuesdownto
theventriclesandmakethemfirenormally,butsomecharge
willridethatloopingpathwaybackaround.IftheAVnodeis
readytofireagainthatchargewillsetitoffearlierthanusual
andyougetafastercycle:theAVnodefires,thechargeloops
aroundandmakesitfireagain.Thiscanresultinheartratesof
over200.
So
think
about
what
we'd
see
on
ECG.
Pwaves?
ProbablynotsincethechargeiscomingfromtheAVnodeso
thisislikeajunctionalrhythm.SincethechargestartsintheAV
nodeitdepolarizestheventriclesthenormalwaybutitdepolarizestheatriagoingup.Soyoumightsee
aninvertedPwaverightbeforetheQRS(closerthanusual),youmightseenoPwaves(becauseitislost
intheQRScomplex),oryoumightseealittlePwaveaftertheQRS.TheQRSwillbenarrow(normal)
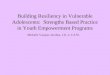
sincedepolarizationisoccurringdowntheHisPurkinjesystem.ClassicallythiswillbeaveryfastratewithnarrowQRScomplexesandnoPwaves.IntheexamplebelowthesmallwavesbetweentheQRScomplexesareTwaves,notPwaves.
-
8/3/2019 Jacobus ECG Tips
4/19
Ventriculartachycardia:thisoccurswhenanirritatedareaofmyocardiumsomewhereinthe
ventriclesstartstofireonitsown,withoutwaitingforachargefromtheHisPurkinjesystem.Irritation
canbecausedbyischemia,electrolyteimbalance,trauma,orotherreasons.Themyocardiumstarts
firingandjustkeepsgoing.Becausethecurrentstartsintheventricularmyocardium,thechargeisgoing
tospreadmyocytetomyocyteratherthandowntheHisPurkinjesystem.SoonECGyou'llseewideQRScomplexesoccurringataveryfastrate.IthinkthatitoftenlookslikeabunchofMcDonaldssignsinarow.
Ventricularfibrillation:thisisuncoordinatedelectricalactivityintheventricles,justlikea
seizure.Thereisnocoordinatedelectricalactivityatalland,hence,nocontraction.OnECGthisjust
lookslikeawavyline.
Asystole:thisisnothing,noelectricalactivityatall.OnECGthislookslikeasimplestraightline.
AxisMeanelectricalaxis(MEA)isprobablythemostdifficultpartofECGinterpretationtoteach.SoIll
giveyoumyquickanddirtymethodaswellasmymoreformalway.
-
8/3/2019 Jacobus ECG Tips
5/19
Quick
handisg
aVF.Poin
positivet
pointing
Ifp
If
If
anddirty:lo
ingtorepre
tyourthumb
anyourleft
own.
bothofyour
ositive,then
yourleftthu
yourrightth
okatleadIa
entleadI.a
sinthedirec
thumbwillb
thumbsare
you'reliketh
mbisupand
umbisupan
ndaVFonth
Fisontheri
tionoftheQ
epointingup
up,meaning
eFonz(Aaaa
yourrightth
dyourlefto
eECG.LeadI
ghtsideoft
RScomplexi
,ifleadaVF
thattheQRS
y!),twothu
umbisdow
eisdownth
isontheleft
epagesoyo
neachlead,
isnegativeth
complexesi
bsupandt
thenyouha
enyouhave
sideofthep
urrighthand
orexamplei
enyourrigh
leadIanda
eaxisisnor
vealeftaxis
arightaxis
agesoyourl
willreprese
fleadIismo
thumbwill
VFaremainl
al.
deviation.
eviation.
eft
nt
stly
e
-
8/3/2019 Jacobus ECG Tips
6/19
Ifu
The
1
2
S
bothofyour
nusual.
oreindept
) Weonlyu) AnECGledepolariza
depolariza
depolariza
thisismyp
thumbsare
version.We
sethelimbl
dislikeane
tioncoming
tiongoinga
tiongoingp
referredmet
downtheny
needtolay
adstocalcul
yeball,itsee
towardsmeI
ayfromme
rpendicular
hod.
uhaveane
ownacoupl
atethemea
electricity.I
'lldeflectth
I'lldeflectth
omeI'lldefl
tremeright
eofassump
electricala
fIamanele
ECGtracing
eECGtracin
ecteithereq
axisdeviatio
ionsfirst.
is(I,II,III,aV
trodeandI
up;ifIseea
down;ifIse
uallyupand
nwhichisve
R,aVL,aVF).
eeawaveof
waveof
eawaveof
downornot
ry
atall.
-
8/3/2019 Jacobus ECG Tips
7/19
1)
Findthelimbleadthatisthemostisoelectric(i.e.netdepolarizationzero)2)
Weknowfromnumbertwoabovethatthismeansthatthewaveofdepolarizationis
travelingperpendiculartothelead,right?
3)
Sofromlookingatthediagrambelow(amodificationofEinthovenstriangle)wecanseethatifweknowtheaxisisperpendiculartoaleadthenwehavetwochoices,itcanbe
perpendicularcomingfromtherightoftheleadandgoingtotheleftofthelead,orthe
otherwayaround.Forexample,lookingatthediagrambelow,iftheaxisisperpendicularto
leadIIthenithastobeeither
30or+150.Sowhichisit?Well,let'slookatthe
perpendicularlead.IftheQRScomplexesaremorepositiveinthatleadthentheaxisis
goingtowardthatlead;iftheyremorenegativethentheaxisisgoingawayfromthatlead.
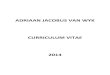
4) Usethisaxisdrawingtohelp:
Examples:
SothemostisoelectricleadhereisaVL.
-
8/3/2019 Jacobus ECG Tips
8/19
Sinceweknow,then,thatthemeanelectricalaxismustbegoingperpendiculartoaVL,then(bylookingatourleadsinthediagramabove)itmustbeeither+60or
120.
Todeterminewhichofthoseitis,welookattheleadthatisperpendiculartoaVL,whichisleadII.IftheQRScomplexispositiveinIIthenitmeansthatcurrentiscomingtowardsitandtheaxis
mustbe+60.IftheQRScomplexisnegative,thenchargemustbemovingawayfromitandthe
axiswouldbe 120.
TheQRSinleadIIispositive,sotheaxisisabout60,whichisnormal,whichconfirmsourthumbsupmethod.
Anotherexample:
ThemostisoelectricleadhereisaVR.aVFisprettyclose,butitseemstomelikeaVRismoreequallyupanddown.
SotheaxismustbeperpendiculartoaVRwhichwouldbe,whenlookingattheaxisdiagramabove,+120or
60.SowegototheleadperpendiculartoaVRtodecidewhichwaytheaxisis
going,towards+120or 60.
TheleadperpendiculartoaVRisleadIII.LeadIIIislocatedat+120.Soifthecomplexispositivethenchargeismovingtowardstheleadandtheaxisis120;ifthecomplexisnegative,then
chargeismovingawayfromtheleadandtheaxisis 60.
ThecomplexinleadIIIisnegative,sothatmeansthatthemeanelectricalaxisis
60.Thisisaleftaxisdeviation,andjiveswithourthumbsupmethod.
Onemoreexample:
-
8/3/2019 Jacobus ECG Tips
9/19
ThemostisoelectricleadhereisleadII.Soweknowthatthechargeismovingperpendiculartoitwhichwouldbe+150or
30.
TofindoutwhichoneitiswelookattheleadthatisperpendiculartoleadIIwhichisaVL.WeknowthataVLislocatedat
30soifthecomplexinaVLispositivethenchargeismoving
towardsaVLandtheaxisis
30;ifthecomplexisnegativethenchargeismovingawayfromit
andtheaxisis+150.
TheQRScomplexinaVLisnegative,meaningthattheaxisis+150.Thisisarightaxisdeviationandalsocorrespondstoourthumbsupmethod.
Soafterdoingthatwecanseewhythethumbsupmethodworks.IfleadIandaVLarepositive
thentheaxismustbesomewhereinthequadrantbetweenzeroand90sincethat'stheonlyareathat
willmake
both
leads
positive.
Onastandard12leadECG,theperpendicularleadsarearrangedlikeso:
-
8/3/2019 Jacobus ECG Tips
10/19
Ii
Intervals
T
aretheP
QTinterv
though:a
occurring
stretchof
onewave
between
intervali
Qwavet
A
thatitto
istheent
thebaseli
thesame
P
fromthe
littlebox
ThePRin
longPRin
theendo
Rememb
depolariz
sperpendic
hemainECG
interval,th
al.Aquickw
segmentis
betweentw
ECGtracing
.SotheSTs
theSwavea
the
area
fro
theendoft
lsonotefro
kmeyearst
ireportiono
ne,ratherth
appliesfort
Rinterval:th
beginningof
sor
0.12
to
tervalprimar
tervalusuall
RSinterval:t
fthelastwa
rwhatwes
estheheart
lartoaVF;II
intervalswe
QRSinterva
rdondefini
stretchofE
waves,ani
thatincludes
gmentisthe
dthePwav
mthe
beginn
heTwave.
thisdiagra
ofigureout:
theQRSco
anjustthefi
eQandSw
isameasure
thePwavet
.20seconds.
ilyrepresent
indicatesso
hisisameas
e.Itreprese
idearlier:n
uickly.Soth
isperpendic
measure
l,andthe
ions,
Gtracing
tervalisa
atleast
area
e;theQT
ingof
the
something
theRwave
plexabove
stupslope;
ves.
ofthetime
thebeginni
We
will
loo
thedelayt
mekindofd
urementfro
ntsthetimei
rmalconduc
eQRSshould
lartoaVL;II
ngoftheQR
at
abnorma
attheelectr
iseaseatthe
thebeginni
ttakesforth
tiontravelst
benarrow,
Iisperpendi
complex.A
litiesof
the
P
icalsignalun
AVnode.
ngofthefirs
eventricles
hroughthe
rlessthant
ulartoaVR.
normalPRin
Rinterval
in
dergoesatth
twaveofth
ocompletel
isPurkinjes
hreelittlebo
tervalis3to
fewminute
eAVnode.S
QRScomple
depolarize.
stemandth
xes,0.12sec
5
s.oa
xto
us
nds.
-
8/3/2019 Jacobus ECG Tips
11/19
AwiderQRScomplexusuallymeansslowconductionintheventricleseither1)becausetheimpulse
startedintheventriclesandisspreadingmyocytetomyocyteratherthanusingtheHisPurkinjesystem
or2)becauseofadefectorablockinoneofthebundlebranchesoftheHisPurkinjesystem.Moreon
thoseinafewminutes.
QTinterval:theQTintervalismeasuredfromthebeginningoftheQRScomplextotheendof
theTwave.Itisameasureofthetimefromthebeginningofdepolarizationtotheendofrepolarization
butsincedepolarizationissoshortitismainlyameasureofthetimetorepolarizetheventricles.The
QTintervalwillchange,though,dependingontheheartrate.Aheartbeatingfastneedsashort
repolarizationtimewhileonebeatingslowlycantakelonger.SoweapplyacorrectiontotheQTinterval
toaccountfortheheartrate.ItiscalledtheQTc(QTcorrected).TheformulaisQTdividedbythesquare
rootoftheRRinterval:
AnormalQTcislessthan0.44seconds(11littleboxes).Ausefulquickanddirtymethodfor
checkingtheQTcistodrawalineverticallyupfromtheendoftheTwave.Nowdrawalinebetweenthe
topoftheRwavebeforeandthetopoftheRwaveafter.IftheendoftheTwaveislessthanhalfthe
wayto
the
next
R
then
it's
likely
in
the
normal
range.
Long
QT
syndrome
can
be
congenital
or
acquired
andisdangerousbecauseitcanleadtoTorsadesdePointe.
Example:
Inthisexample,theendoftheTwavefallslessthanhalfwaybetweenthe2Rwaves,andsois
mostlikelynormal.
Anotherexample:
Inthisexample,theendoftheTwavefallsmorethanhalfofthedistancetothenextRwave
andsoisprolonged.
-
8/3/2019 Jacobus ECG Tips
12/19
PRintervalabnormalities/AVBlocks:aswesaidbefore,alongPRintervalusuallymeanssome
sortofpathologyattheAVnodesincethePRintervalmainlymeasurestimebetweenatrial
depolarizationandventriculardepolarization,thetimewhenthechargeisbeingdelayedbytheAV
node.Solet'stalkaboutafewblocks,therearefourthatyouneedtoknow.
Firstdegree:thisissimplyalongerthanusualdelayattheAVnode,manifestedbyafixedPRintervalthatislongerthan0.20seconds.Itisbenignanddoesn'tneedanyimmediatetreatment.
SeconddegreetypeI:thisisaPRintervalthatgetslongerwitheachbeatuntiliteventuallyblocksthedepolarizationcompletelyleadingtoadroppedQRScomplex.It'salsoknownasMobitzIorWenckebach.(Ifyouhaven'talreadyseenitIhighlyrecommendwatchingDiagnosis
WenckebachonYouTube.)Thisisalsoabenignrhythmandneedsnourgentintervention.
SeconddegreetypeII:thisisaPRintervalthatisnormalandunchangingwiththeexceptionthatoccasionallythePwaveswilloccurwithoutaQRS
i.e.theAVnodeblockstransmissionofanimpulsefromtheatriatotheventriclescompletely.Thisisconsideredamalignantblock
duetoitstendencytodeteriorateintoathirddegreeheartblock.
8littleboxes=0.32sec
Normal Long Longer DroppedQRS
Dropped
QRS Dropped
QRS
-
8/3/2019 Jacobus ECG Tips
13/19
Tb
t
t
r
is
t
r
Asho
ofanacc
intervalis
withoutg
QRSi
timeitta
impulset
Purkinjes
hirddegree(
etweenthea
avesbutno
eventricles,
eventricles
gularPwav
noconnecti
reateningbl
arkedbelow
gardforan
rtPRinterva
ssorypathw
shorterbec
oingthrough
ntervalabno
esforthev
hatstartsin
ystem,or2)
completehe
triaandthe
eofthoseat
itappearsa
needtotake
esandregul
nbetweent
ockandman
,youcansee
rmalorder.
l,inconjuncti
aybetweent
usethedep
thedelayat
malities/Bun
ntriclestofu
heventricles
animpulset
rtblock):thi
entricles.Th
rialdepolari
iftheSAan
overpacem
rQRScomp
hematall.T
datesurgent
thattheyse
onwithade
heatriaand
larizationca
theAVnode
dleBranchB
llydepolariz
andhastos
atstartsnor
siswhereth
eatriaconti
ationsareg
AVnodesh
kingdutiest
exesbutocc
eQRScomp
intervention
emtomarch
ltawave(cir
theventricle
ngostraight
.
locks:aswe
.Thiscanbe
preadmyocy
mallybutth
ereisacom
uetobeata
ttingconduc
avestopped
hemselves.S
urringatco
lexescanbe
,usuallyapa
throughthe
ledingreen
s,suchasin
fromtheatr
saidearlier,t
delayedfor
tetomyocyt
nhitsacon
leteelectric
susualprodu
teddownto
orkingcom
owhatyous
pletelydiff
narroworwi
cemaker.Th
QRScomple
below),impli
olffParkins
iadowninto
heQRSinter
oneoftwor
e,whichissl
uctionblock
ldisconnecti
cingregular
theventricle
pletelyandt
eonthestri
rentrates.T
de.Thisisal
Pwavesar
eswithouta
estheprese
onWhite.Th
theventricle
alrepresent
asons:1)an
werthanth
intheHis
on
P
s.To
us
pis
here
ife
ny
ce
ePR
s
sthe
His
-
8/3/2019 Jacobus ECG Tips
14/19
Purkinjes
leftandri
Asyo
blocking
depolariz
158ofDa
blockwill
complex
yourima
aQRSco
V6which
LBBB:
RBBB
Hypertro
V
hypertro
counting
LVH:
bediagno
1) Tb
2) T
ysteminthe
ghtbundleb
umayreme
feitherone
ation.Therei
vis,QuickanhaveaQRS
oftenwithb
ination)in
plexgreate
isonthelef
:
hy
entricularhy
hyaswell.D
boxes.
herearethr
sedasLVH.
heSwavein
igboxes).
heRwavein
ventricles.T
ranchblocks.
ber,thebu
ofthesebra
sagooddes
dAccurate1urationgre
unnyears:a
1whichiso
rthan0.12s
sideofthec
pertrophyis
iagnosingLV
emainform
V1(blue)plu
aVL(red)isg
etwomain
dleofHissp
cheswillcau
riptionofwLeadECGInterthanthr
QRScomple
therightsi
econdsand
hest.
oingtobeo
HandRVHis
ulastoknow
stheRwave
reaterthan
conductionb
litsintotwo
seawideQ
ythecharac
terpretation.
elittleboxe
thathastw
eoftheche
positiveQR
urmainfocu
reallyjusta
forLVH;ifa
inV5orV6(
requalto11
lockswewill
undlebranc
Scomplexd
teristicECG
Forourpur
s(0.12seco
opositivede
st.Aleftbun
complex(a
sbutwewill
atterofre
ECGmeets
green)isgre
mm
discussinth
hes,theleft
uetoadelay
indingsoccu
osesaright
ds)andapo
flections,an
dlebranchbl
lsooftenwit
touchbriefly
emberingfo
anyoneoft
terthanore
eventriclesa
ndright.A
incomplete
ronpages1
undlebranc
sitiveQRS
RandanR,
ockwillalso
bunnyears
onatrial
rmulasand
esecriteriai
qualto35m
re
2to
h
use
have
)in
tcan
m(7okolow Criteria:
-
8/3/2019 Jacobus ECG Tips
15/19
3) TheRwaveinV5orV6(purple)isgreaterthanorequalto27mm.
Ifyounotice,allofthesecriteriahaveincommonthatyouarelookingforabigpositivedeflection
ontheleft(aVLandV5andV6)andabignegativedeflectionintherightleads(V1).
RVH:sameidea,youonlyneedtomeetoneofthecriteriabelow,buttheformulasare:
21mm
25mm
22mm
37mm
-
8/3/2019 Jacobus ECG Tips
16/19
1. R2. t
Again,he
deflectio
Lefta
1) ad
s
b
2) Aaa
r
n
Right
leadII.So
waveinV1(
eRwavein
reweareloo
inthelefts
trialhypertr
notchedor
istentionor
condpeaki
ottomleftof
hichishand
largenegati
triumdepola
triumdepola
sultingina
egativedefl
atrialhypert
inrightatria
purple)isgre
1plustheS
kingforabi
idedleads(V
phy:therea
shapedPw
ypertrophy
thedepolari
thebodywh
becausethe
eportionof
rizesthe
cha
rizes,becaus
egativedefl
ctioninthe
rophy:theri
lhypertroph
aterthanth
waveinV6i
positivedefl
).
retwomain
aveinleadII
ndsothefir
zationofthe
ichiswherel
leadIIPwa
thePwavei
gemoves
to
etheleftatri
ction.Soift
waveofle
htatriumde
therewillb
SwaveinV
greatertha
ectioninthe
riteriatolo
.Theleftatri
stpeakisthe
leftatrium.
eadIIislook
veslookslik
V1.V1ison
ardsthe
le
umismorep
eleftatriu
dV1.
polarizesdo
etallPwave
orequalto
rightsidedl
kforinleft
aldepolariza
depolarizati
heyarebot
ingfrom.Thi
anM.
theanterior
dgiving
apo
osterior,the
ishypertro
nandtoth
sinleadII,
11mm.
eads(V1)an
trialhypertr
tionisdelaye
onoftherigh
positivewh
sfindingisca
chestsowh
sitivedeflect
chargemov
hiedyou'llg
left,almost
iggerthan2.
abignegati
phy:
ddueto
tatrium,the
enseenfrom
lledPmitralntheright
ion.When
t
sposteriorly
talarge
directlytow
4mm.
ve
the
eleft
rds
-
8/3/2019 Jacobus ECG Tips
17/19
IschemiaT
1) Tr
r
c
p
2)t
herearethre
waveinversi
hythisoccur
polarization
polarization
angescanr
ersistforwe
waves:Qw
eyare:
a. widerb. greate
fromt
emainECGs
ons:Ihaveb
s,butitdoes
ofcardiacm
reversesand
presentcurr
kstomonth
ves(theiniti
than0.04se
rthanonet
hesamecom
ignstolook
eenunablet
.Ischemiah
ocytes.Inm
theTwave,
entorrecen
sbeforenor
alnegatived
onds(onelit
irdofthehe
plex.
orwhencon
findasatisf
scomplexe
yocardialisc
normallyup
ischemia.U
alizing.
eflectionof
tlebox)or
ightoftheR
cernedabou
actoryelectr
fectsonthe
emiaorinfa
ightinalllea
ually,inthe
QRScomple
wave
ischemiaor
ophysiologic
depolarizatio
rctionthedir
dsexceptaV
caseofanin
x)areconsid
infarction:
lexplanatio
nand
ectionof
R,inverts.Th
arction,the
eredpatholo
for
ese
will
gicif
-
8/3/2019 Jacobus ECG Tips
18/19
T
e
g
in
n
t
3) Sina
c
d
S
d
e
S
s
heydevelop
lectricity.So
ovingtowar
tanegative
farction.Th
oothersigns
ansmuralin
segmentch
farctionhav
cuteinfarctio
yocardiumc
lledthecu
epressions.F
elevations
epressions.
levations.Th
elevations
vereSTelev
becauseani
henanelec
sitbutthe
deflection.T
yusuallyper
ofischemia
arction.Not
anges:aswe
asignifican
nthechange
reatesanele
rentofinjur
orreasonsto
overtheaffe
eepinmind,
ideaisthat
illseetheo
ationsinII,II
farctingori
trodeisover
ppositeven
hepresence
sistforther
(Twaveinve
thepresen
mentionedi
effect
on
th
inpotential
ctrochemical
.Thesecur
odetailedfo
ctedregion
though,the
thataleadt
pposite:STd
I,andaVF,w
farctedarea
anareaofin
riclehasaw
oftheQwav
stofthepat
rsionorSTs
eofQwave
nthesection
eway
apiec
betweenthe
gradientan
entsarema
rinclusionh
ndasubend
STdepressio
at'slooking
epression.In
ithreciprocal
ofmyocardi
farctionther
aveofdepol
esindicates
ient'slife.So
gmentcha
inIII,aVF,V
onTwavei
of
myocardi
ischemicm
chargeflow
ifestedasS
re,afullthi
ocardialinfa
scanbe"re
intheopposi
theexample
STdepressi
mdoesnot
eisnowave
rizationmo
fullthickne
thepresenc
ges)indicat
1,V2,andV3
versions,isc
umcan
hand
ocardiuman
sbetweenth
segmentel
knessinfarc
rctionwillg
ciprocalchan
tedirectionf
belownote
nsinV1V
conduct
ofdepolariza
ingaway,so
sortransmu
ofQwaves
sanold
below.
hemiaand
lecharge.
In
dhealthy
oseareas.T
vationsor
tionwillgen
nerateST
ges"ofST
romthelead
hepresence
.
tion
you
ral
with
an
isis
rate
with
of
-
8/3/2019 Jacobus ECG Tips
19/19