Embed Size (px)
Citation preview

UnitedHealthcare respects the expertise of the physicians, health care professionals, and their staff who participate in our network. Our goal is to
support you and your patients in making the most informed decisions regarding the choice of quality and cost-effective care, and to support practice
staff with a simple and predictable administrative experience. The Policy Update Bulletin was developed to share important information regarding
UnitedHealthcare Dental Clinical Policy and Coverage Guideline updates.*
*Where information in this bulletin conflicts with applicable state and/or federal law, UnitedHealthcare follows such applicable federal and/or state law
January 2018
policy update bulletin Dental Clinical Policy & Coverage Guideline Updates

2 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Dental Clinical Policy & Coverage Guideline Updates
Overview
Tips for using the Policy Update Bulletin:
From the table of contents, click the policy title to be
directed to the corresponding policy update summary.
From the policy updates table, click the policy title to view a
complete copy of a new, updated, or revised policy.
Policy Update Classifications
New
New clinical coverage criteria and/or documentation review
requirements have been adopted for a health service (e.g., test, drug,
device or procedure)
Updated
An existing policy has been reviewed and changes have not been made
to the clinical coverage criteria or documentation review requirements;
however, items such as the clinical evidence, FDA information, and/or
list(s) of applicable codes may have been updated
Revised
An existing policy has been reviewed and revisions have been made to
the clinical coverage criteria and/or documentation review requirements
Replaced
An existing policy has been replaced with a new or different policy
Retired
The health service(s) addressed in the policy are no longer being
managed or are considered to be proven/medically necessary and are
therefore not excluded as unproven/not medically necessary services,
unless coverage guidelines or criteria are otherwise documented in
another policy
Note: The absence of a policy does not automatically indicate or imply
coverage. As always, coverage for a health service must be determined
in accordance with the member’s benefit plan and any applicable
federal or state regulatory requirements. Additionally, UnitedHealthcare
reserves the right to review the clinical evidence supporting the safety
and effectiveness of a medical technology prior to rendering a coverage
determination.
This bulletin provides complete details on UnitedHealthcare Dental
Clinical Policy and Coverage Guideline updates. The inclusion of a
dental service (e.g., procedure or technology) in this bulletin
indicates only that UnitedHealthcare has recently adopted a new
policy and/or updated, revised, replaced or retired an existing
policy; it does not imply that UnitedHealthcare provides coverage
for the dental service. In the event of an inconsistency or conflict
between the information provided in this bulletin and the posted
policy, the provisions of the posted policy will prevail. Note that
most benefit plan documents exclude from benefit coverage health
services identified as investigational or unproven/not medically
necessary. Physicians and other health care professionals may not
seek or collect payment from a member for services not covered by
the applicable benefit plan unless first obtaining the member’s
written consent, acknowledging that the service is not covered by
the benefit plan and that they will be billed directly for the service.
A complete library of Dental Clinical Policies & Coverage
Guidelines is available at UHCprovider.com > Menu >
Policies and Protocols > Dental Clinical Policies and
Coverage Guidelines.

3 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Dental Clinical Policy & Coverage Guideline Updates
In This Issue
Take Note Page
ANNUAL CDT CODE UPDATES
Application of Medicaments and Desensitizing Resins – Effective Jan. 1, 2018 .......................................................................................................... 5 Full Mouth Debridement – Effective Jan. 1, 2018 .................................................................................................................................................. 5 General Anesthesia Conscious Sedation Services – Effective Jan. 1, 2018 ................................................................................................................ 5 Implants – Effective Jan. 1, 2018 ....................................................................................................................................................................... 5 Medically Necessary Orthodontic Treatment – Effective Jan. 1, 2018 ....................................................................................................................... 5 Miscellaneous Diagnostic Procedures – Effective Jan. 1, 2018 ................................................................................................................................. 5 National Standardized Dental Claim Utilization Review Criteria – Effective Jan. 1, 2018 ............................................................................................. 5 Non-Surgical Endodontics – Effective Jan. 1, 2018 ................................................................................................................................................ 5 Non-Surgical Extractions – Effective Jan. 1, 2018 ................................................................................................................................................. 5 Oral Surgery: Miscellaneous Surgical Procedures – Effective Jan. 1, 2018 ................................................................................................................ 6 Oral Surgery: Orthodontic Related Procedures – Effective Jan. 1, 2018 ................................................................................................................... 6 Removable Prosthodontics – Effective Jan. 1, 2018 ............................................................................................................................................... 6 Single Tooth Indirect Restorations – Effective Jan. 1, 2018 .................................................................................................................................... 6 Surgical Endodontics – Effective Jan. 1, 2018 ....................................................................................................................................................... 6 Surgical Periodontics: Resective Procedures – Effective Jan. 1, 2018 ....................................................................................................................... 6
Clinical Policy Updates
UPDATED
Genetic Testing for Oral Disease – Effective Jan. 1, 2018 ....................................................................................................................................... 7 Non-Ionizing Diagnostic Procedures – Effective Jan. 1, 2018 .................................................................................................................................. 7
RETIRED
Imaging Services: Cone Beam Computed Tomography – Effective Jan. 1, 2018 ........................................................................................................ 7
Coverage Guideline Updates
UPDATED
Non-Surgical Endodontics – Effective Jan. 1, 2018 ................................................................................................................................................ 8 Provisional Splinting – Effective Jan. 1, 2018 ..................................................................................................................................................... 11 Salivary Testing – Effective Jan. 1, 2018 ........................................................................................................................................................... 12
REVISED
Labial Veneers – Effective Feb. 1, 2018 ............................................................................................................................................................. 12

4 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Dental Clinical Policy & Coverage Guideline Updates
In This Issue
Single Tooth Indirect Restorations – Effective Feb. 1, 2018 .................................................................................................................................. 13

5 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Take Note
ANNUAL CDT CODE UPDATES
Effective Jan. 1, 2018, the following Dental Clinical Policies, Coverage Guidelines, and Utilization Review Guidelines have been modified to reflect the 2018 Current Dental Terminology (CDT) code additions, revisions, and deletions. Refer to the source below for information on the 2018 code updates:
American Dental Association®. Current Dental Terminology: CDT 2018
Policy Title Policy Type Summary of Changes
Application of
Medicaments and Desensitizing Resins
Clinical Policy Revised description for D1354
Full Mouth Debridement
Coverage Guideline
Revised description for D4355
General Anesthesia Conscious Sedation Services
Coverage Guideline
Added D9222 and D9239 Revised description for D9223 and D9243
Implants Coverage Guideline
Added D6096, D6118, and D6119
Medically Necessary Orthodontic
Treatment
Coverage Guideline
Added D8695
Miscellaneous Diagnostic Procedures
Coverage Guideline
Added D0411
National Standardized Dental Claim
Utilization Review
Criteria
Utilization Review Guideline
Added D0411, D5511, D5512, D5611, D5612, D5621, D5622, D6096, D6118, D6119, D7296, D7297, D7979, D8695, D9222, D9239, D9995, and D9996
Removed D5510, D5610, and D5620
Non-Surgical Endodontics
Coverage Guideline
Revised description for D3320, D3330, and D3347
Non-Surgical Extractions
Coverage Guideline
Revised description for D7111

6 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Take Note
ANNUAL CDT CODE UPDATES
Oral Surgery: Miscellaneous Surgical Procedures
Clinical Policy Added D7979 Revised description for D7980
Oral Surgery: Orthodontic Related Procedures
Clinical Policy Added D7296 and D7297
Removable Prosthodontics
Coverage Guideline
Added D5511, D5512, D5611, D5612, D5621, and D5622 Removed D5510, D5610, and D5620
Single Tooth Indirect Restorations
Coverage Guideline
Revised description for D2740
Surgical Endodontics
Clinical Policy Revised description for D3421
Surgical
Periodontics: Resective
Procedures
Clinical Policy Revised description for D4230 and D4231

7 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Clinical Policy Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
UPDATED
Genetic Testing for Oral Disease
Jan. 1, 2018 Updated supporting information to reflect the most current
clinical evidence, FDA information and references; no change to coverage rationale or list of applicable codes
Collection and Preparation of Genetic Sample Material for Laboratory Analysis and Report
Genetic Test for Susceptibility to Diseases – Specimen Analysis
The collection, preparation and testing of genetic samples are indicated for patients who have known human papilloma virus (HPV) infection, or have
other related risk factors, to identify if the strain of HPV known to be related
to oral and oropharyngeal cancers is present.
The clinical utility of genetic testing for susceptibility to periodontal diseases
has not been established. Additionally, there is a lack of objective, high quality clinical evidence to support these tests.
Non-Ionizing Diagnostic Procedures
Jan. 1, 2018 Updated supporting information to reflect the most current clinical evidence and references; no change to coverage rationale or list of applicable codes
There is inadequate evidence demonstrating the efficacy of these devices, limiting their use as a principal diagnostic tool. A non-ionizing diagnostic procedure refers to a device specifically designed to identify, quantify, monitor, and record changes in structure of enamel, dentin and cementum. These devices may be used as an adjunctive tool by the dental provider to
identify high caries risk areas, and create non-invasive treatment plans for
remineralization before caries begins. Visual and radiographic examinations remain the standard diagnostic methods for diagnosing active caries.
Policy Title Effective Date Summary of Changes
RETIRED
Imaging Services:
Cone Beam Computed Tomography
Jan. 1, 2018 Policy retired; the use of cone beam computed tomography (CBCT) for routine dental applications no longer
requires clinical coverage review

8 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
UPDATED
Non-Surgical Endodontics
Jan. 1, 2018
Updated list of applicable CDT codes to reflect annual code
edits; revised description for D3320, D3330, and D3347
Updated supporting information to reflect the most current
references
Vital Pulp Therapy
Direct Pulp Cap
Direct pulp capping is indicated for the following: Tooth has a vital pulp or been diagnosed with reversible pulpitis All caries has been removed Mechanical exposure of a clinically vital and asymptomatic pulp occurs
Bleeding is controlled at the exposure site
Exposure permits the capping material to make direct contact with the vital pulp tissue
Exposure occurs when the tooth is under dental dam isolation Adequate seal of the coronal restoration can be maintained Patient has been fully informed that endodontic treatment may be
indicated in the future
Direct Pulp capping is not indicated for a carious exposure in primary teeth
Indirect Pulp Cap
Indirect pulp capping is indicated for the following:
Tooth has a vital pulp or been diagnosed with reversible pulpitis Tooth has a deep carious lesion that is considered likely to result in pulp
exposure during excavation
No history of subjective pretreatment symptoms Pretreatment radiographs should not show periradicular pathosis
Therapeutic Pulpotomy
Therapeutic pulpotomy is indicated for the following: Exposed vital pulps or irreversible pulpitis of primary teeth Any bleeding was controlled within several minutes As an emergency procedure in permanent teeth until root canal
treatment can be accomplished
As an interim procedure for permanent teeth with immature root formation to allow continued root development
In primary teeth, where there is a reasonable period of retention expected (approximately one year)
Therapeutic pulpotomy is not indicated for the following: Primary teeth with insufficient root structure, internal resorption, furcal
perforation or periradicular pathosis that may jeopardize the permanent successor
As the first stage of complete root canal therapy
9 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
UPDATED
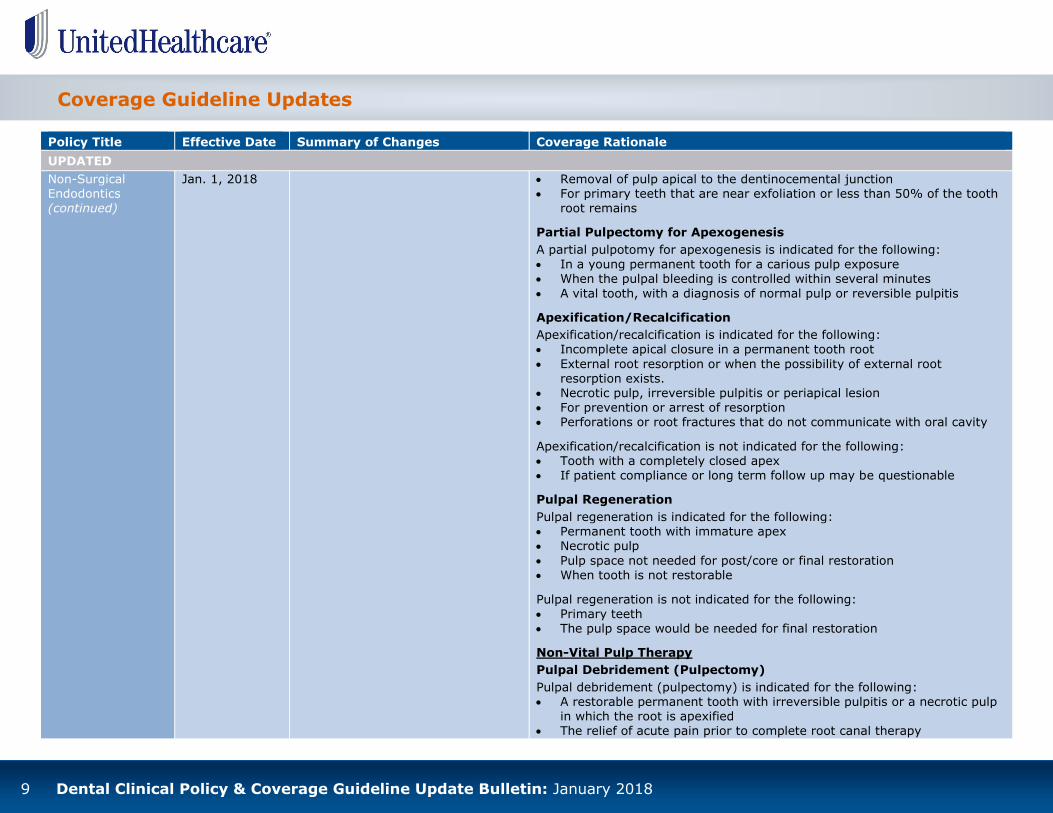
Non-Surgical Endodontics (continued)
Jan. 1, 2018
Removal of pulp apical to the dentinocemental junction For primary teeth that are near exfoliation or less than 50% of the tooth
root remains
Partial Pulpectomy for Apexogenesis
A partial pulpotomy for apexogenesis is indicated for the following:
In a young permanent tooth for a carious pulp exposure When the pulpal bleeding is controlled within several minutes
A vital tooth, with a diagnosis of normal pulp or reversible pulpitis
Apexification/Recalcification
Apexification/recalcification is indicated for the following: Incomplete apical closure in a permanent tooth root
External root resorption or when the possibility of external root resorption exists.
Necrotic pulp, irreversible pulpitis or periapical lesion For prevention or arrest of resorption Perforations or root fractures that do not communicate with oral cavity
Apexification/recalcification is not indicated for the following: Tooth with a completely closed apex If patient compliance or long term follow up may be questionable
Pulpal Regeneration
Pulpal regeneration is indicated for the following: Permanent tooth with immature apex Necrotic pulp
Pulp space not needed for post/core or final restoration When tooth is not restorable
Pulpal regeneration is not indicated for the following:
Primary teeth The pulp space would be needed for final restoration
Non-Vital Pulp Therapy
Pulpal Debridement (Pulpectomy)
Pulpal debridement (pulpectomy) is indicated for the following: A restorable permanent tooth with irreversible pulpitis or a necrotic pulp
in which the root is apexified The relief of acute pain prior to complete root canal therapy

10 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
UPDATED
Non-Surgical Endodontics (continued)
Jan. 1, 2018
A primary tooth, where there is a reasonable period of retention expected (approximately one year)
Pulpal debridement (pulpectomy) is not indicated for the following: Complete root canal therapy of an infected or necrotic tooth Primary teeth that are near exfoliation or less than 50% of the tooth root
remains
Pulpal Therapy (Resorbable Filling) – Primary Teeth
Pulpal therapy for primary teeth is indicated for the following:
A restorable primary tooth with irreversible pulpitis or a necrotic pulp in which the root is apexified
The prognosis for keeping the tooth is up to one year and the tooth root lies in at least 25% bone
Pulpal therapy is not indicated for the following: Primary teeth that are near exfoliation or less than 50% of the tooth root
remains Permanent teeth
Endodontic Therapy
Endodontic therapy is indicated for the following: A restorable mature, completely developed permanent or primary tooth
with irreversible pulpitis, necrotic pulp or frank vital pulpal exposure
Teeth with radiographic periapical pathology Primary teeth without a permanent successor Trauma When needed for prosthetic rehabilitation
Endodontic therapy is not indicated for the following: Teeth with a poor long term prognosis Teeth that are considered non-restorable
Teeth with inadequate bone support or advanced or untreated periodontal disease
Teeth with incompletely formed root apices
Treatment of Root Canal Obstruction; Non-Surgical Access
Treatment of a root canal obstruction is indicated for the following:
When there is an obstruction of the root canal system, (biological, iatrogenic ledges or post removal) and endodontic retreatment is needed
Removal of obstruction is complex and/or requires significant time

11 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
UPDATED
Non-Surgical Endodontics (continued)
Jan. 1, 2018 Treatment of a root canal obstruction is not indicated when there is no obstruction evident.
Incomplete Endodontic Therapy: Inoperable, Unrestorable or Fractured Tooth
Incomplete endodontic therapy is indicated for the following:
During endodontic treatment of a tooth, it becomes apparent that the procedure cannot be successfully completed
The tooth will not be able to be restored, or the tooth fractures, necessitating discontinuation of treatment
Internal Root Repair of Perforation Defects
Internal root repair of perforation defects is indicated for the following:
There is a root perforation caused by pathology such as resorption or decay
A communication between the pulp space and external root surface as a result of internal root resorption.
Internal root repair of perforation defects is not indicated for the following:
Teeth that are considered non-restorable Teeth with inadequate bone support or advanced untreated periodontal
disease
Retreatment of Previous Root Canal Therapy
Retreatment of previous root canal therapy is indicated for the following: Canal fill appears to extend to a point shorter than 2millimeters from the
apex, or extends significantly beyond the apex
Fill appears to be incomplete Tooth is sensitive to pressure and percussion or other subjective
symptoms The existing endodontics is poor
Placement of a post has the potential to compromise the existing obturation or apical seal of the canal system
The canal is accessible and allows for retreatment with a non-surgical procedure
Provisional Splinting
Jan. 1, 2018
Updated supporting information to reflect the most current references; no change to coverage rationale or list of
Provisional Splinting using these codes is indicated for the following: Multiple teeth that have become mobile due to loss of alveolar bone loss
and periodontium During surgical and healing phases of regenerative periodontal therapy
12 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
UPDATED
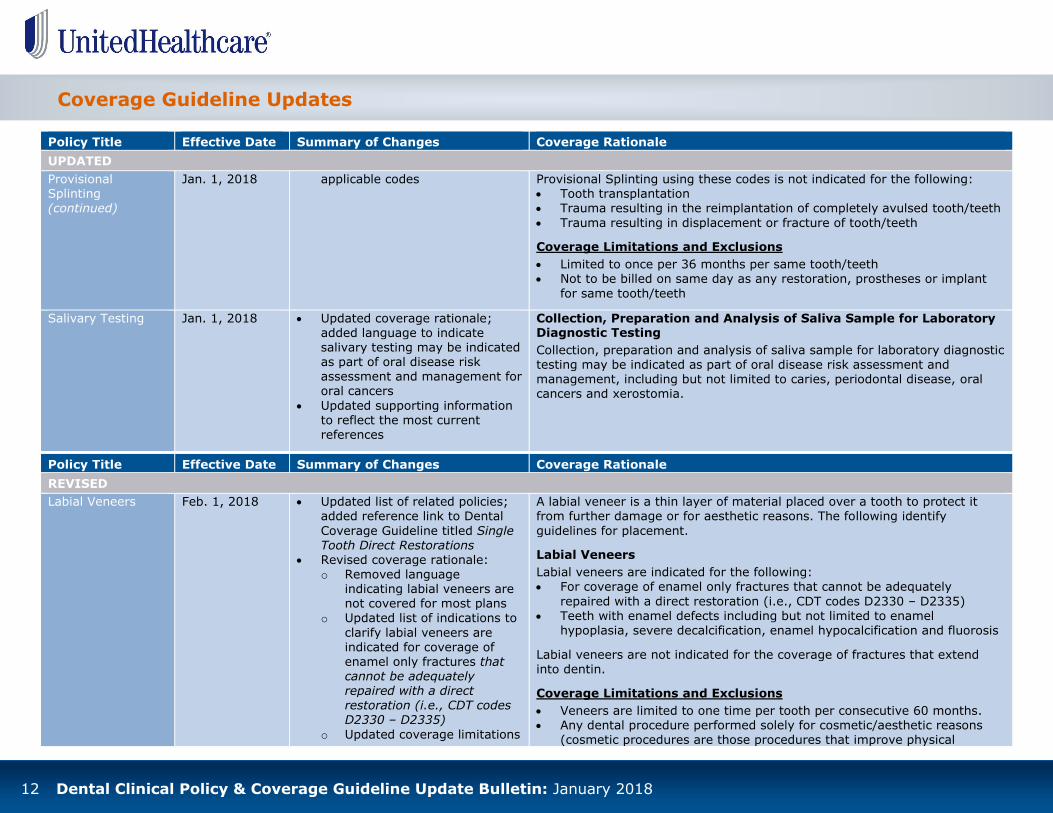
Provisional Splinting (continued)
Jan. 1, 2018 applicable codes
Provisional Splinting using these codes is not indicated for the following: Tooth transplantation Trauma resulting in the reimplantation of completely avulsed tooth/teeth
Trauma resulting in displacement or fracture of tooth/teeth
Coverage Limitations and Exclusions
Limited to once per 36 months per same tooth/teeth Not to be billed on same day as any restoration, prostheses or implant
for same tooth/teeth
Salivary Testing Jan. 1, 2018 Updated coverage rationale; added language to indicate salivary testing may be indicated as part of oral disease risk assessment and management for oral cancers
Updated supporting information to reflect the most current references
Collection, Preparation and Analysis of Saliva Sample for Laboratory Diagnostic Testing
Collection, preparation and analysis of saliva sample for laboratory diagnostic testing may be indicated as part of oral disease risk assessment and management, including but not limited to caries, periodontal disease, oral cancers and xerostomia.
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Labial Veneers
Feb. 1, 2018
Updated list of related policies; added reference link to Dental
Coverage Guideline titled Single Tooth Direct Restorations
Revised coverage rationale: o Removed language
indicating labial veneers are not covered for most plans
o Updated list of indications to
clarify labial veneers are indicated for coverage of enamel only fractures that cannot be adequately repaired with a direct restoration (i.e., CDT codes D2330 – D2335)
o Updated coverage limitations
A labial veneer is a thin layer of material placed over a tooth to protect it from further damage or for aesthetic reasons. The following identify
guidelines for placement.
Labial Veneers
Labial veneers are indicated for the following: For coverage of enamel only fractures that cannot be adequately
repaired with a direct restoration (i.e., CDT codes D2330 – D2335)
Teeth with enamel defects including but not limited to enamel hypoplasia, severe decalcification, enamel hypocalcification and fluorosis
Labial veneers are not indicated for the coverage of fractures that extend into dentin.
Coverage Limitations and Exclusions
Veneers are limited to one time per tooth per consecutive 60 months. Any dental procedure performed solely for cosmetic/aesthetic reasons
(cosmetic procedures are those procedures that improve physical

13 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Labial Veneers (continued)
Feb. 1, 2018 and exclusions; added language to indicate: Veneers are limited to
one time per tooth per consecutive 60 months
Any dental procedure
performed solely for cosmetic/aesthetic reasons (cosmetic procedures are those
procedures that improve physical appearance) is excluded from coverage
appearance) is excluded from coverage.
Single Tooth Indirect Restorations
Feb. 1, 2018
Revised coverage rationale for: Crowns o Updated language to clarify
crowns are indicated for:
Large, >50% of the tooth, defective restoration that can be seen on the radiographic image or intraoral photograph
Documentation/narrative that the failing existing crown can only be resolved with a new crown if not visible on radiographic image or intraoral photograph
Bicuspids and molars: 3 or more surfaces and/or one or more cusps involved
Onlays o Updated language to clarify
onlays are indicated for:
Large, >50% of the tooth, defective
Indications for Coverage
For indirect restorations, the following clinical parameters apply: Five-year longevity should be evident, periodontium must be healthy or
have documentation the member has periodontal disease under control
for a period of at least 6 months, and no evidence of endodontic pathology or potential endodontic issues on the radiographic image.
Crowns
Crowns are indicated for the following: Extensive caries on three or more surfaces or 50% loss of clinical crown Large, >50% of the tooth, defective restoration that can be seen on the
radiographic image or intraoral photograph Fracture of cusps Endodontically treated teeth, unless minimal access opening on anterior
tooth Documentation that a direct restoration is not possible Crown/root ratio must be favorable
Documentation/narrative that the failing existing crown can only be resolved with a new crown if not visible on radiographic image or intraoral photograph
50% bone support with no ligament or root pathology unless patient has undergone periodontal therapy/surgery
Anterior teeth: at least 50% involvement of incisal portion Bicuspids and molars: 3 or more surfaces and/or one or more cusps
involved

14 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
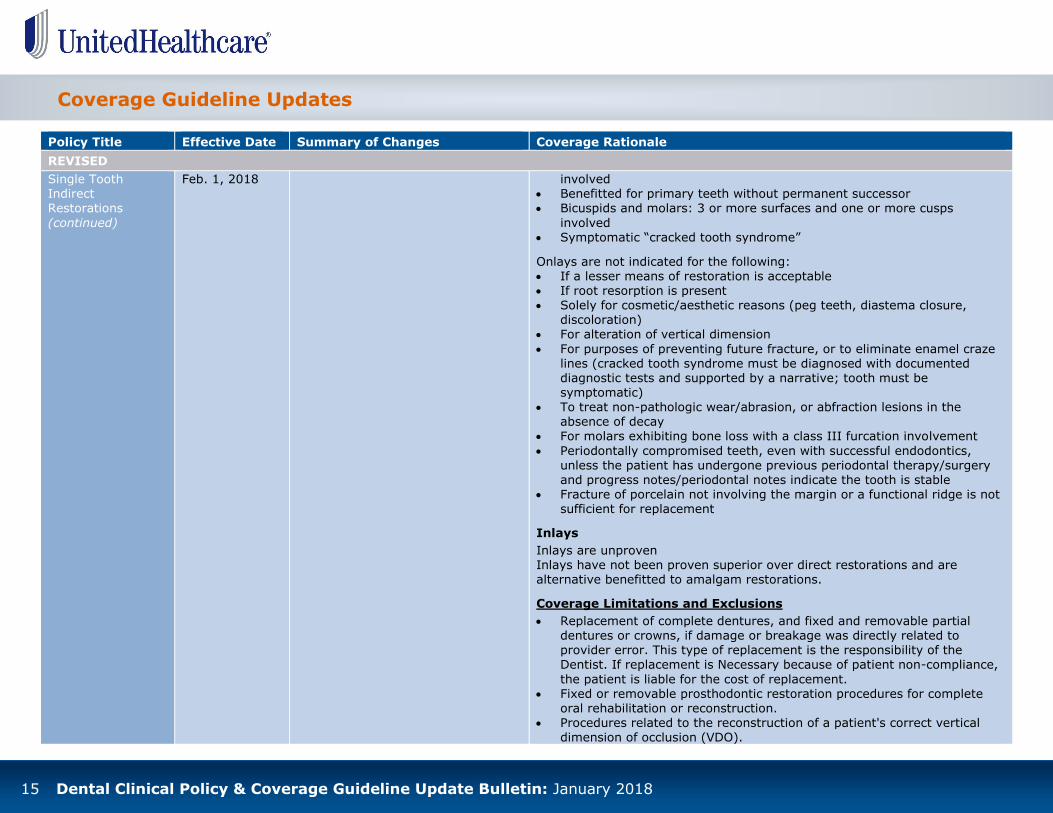
Single Tooth Indirect Restorations
(continued)
Feb. 1, 2018
restoration that can be seen on the radiographic image or intraoral
photograph Documentation/narrative
that the failing existing
onlay can only be resolved with a new onlay if not visible on radiographic image or
intraoral photograph Bicuspids and molars: 3
or more surfaces and/or one or more cusps involved
Symptomatic “cracked tooth syndrome” (not enamel craze lines) Full coverage restoration of a primary tooth without a permanent
successor
Crowns are not indicated for the following: If a lesser means of restoration is acceptable
If root resorption is present Solely for cosmetic/aesthetic reasons (peg teeth, diastema closure,
discoloration) For alteration of vertical dimension For purposes of preventing future fracture, or to eliminate enamel craze
lines (cracked tooth syndrome must be diagnosed with documented
diagnostic tests and supported by a narrative; tooth must be symptomatic)
To treat non-pathologic wear/abrasion, or abfraction lesions in the absence of decay
For molars exhibiting bone loss with a class III furcation involvement Periodontally compromised teeth, even with successful endodontics,
unless the patient has undergone previous periodontal therapy/surgery
and progress notes/periodontal notes indicate the tooth is stable Fracture of porcelain not involving the margin or a functional ridge is not
sufficient for replacement
Onlays
Onlays are indicated for the following: Extensive caries on three or more surfaces or 50% loss of clinical crown Large, >50% of the tooth, defective restoration that can be seen on the
radiographic image or intraoral photograph Fracture of cusps Endodontically treated teeth, unless minimal access opening on anterior
tooth
Documentation that a direct restoration is not possible Crown/root ratio must be favorable Documentation/narrative that the failing existing onlay can only be
resolved with a new onlay if not visible on radiographic image or intraoral photograph
50% bone support with no ligament or root pathology unless patient has
undergone periodontal therapy/surgery Anterior teeth: at least 50% involvement of incisal portion Bicuspids and molars: 3 or more surfaces and/or one or more cusps
15 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Single Tooth Indirect Restorations
(continued)
Feb. 1, 2018
involved Benefitted for primary teeth without permanent successor Bicuspids and molars: 3 or more surfaces and one or more cusps
involved Symptomatic “cracked tooth syndrome”
Onlays are not indicated for the following: If a lesser means of restoration is acceptable If root resorption is present Solely for cosmetic/aesthetic reasons (peg teeth, diastema closure,
discoloration) For alteration of vertical dimension
For purposes of preventing future fracture, or to eliminate enamel craze lines (cracked tooth syndrome must be diagnosed with documented diagnostic tests and supported by a narrative; tooth must be symptomatic)
To treat non-pathologic wear/abrasion, or abfraction lesions in the absence of decay
For molars exhibiting bone loss with a class III furcation involvement
Periodontally compromised teeth, even with successful endodontics, unless the patient has undergone previous periodontal therapy/surgery and progress notes/periodontal notes indicate the tooth is stable
Fracture of porcelain not involving the margin or a functional ridge is not sufficient for replacement
Inlays
Inlays are unproven Inlays have not been proven superior over direct restorations and are alternative benefitted to amalgam restorations.
Coverage Limitations and Exclusions
Replacement of complete dentures, and fixed and removable partial dentures or crowns, if damage or breakage was directly related to provider error. This type of replacement is the responsibility of the Dentist. If replacement is Necessary because of patient non-compliance,
the patient is liable for the cost of replacement. Fixed or removable prosthodontic restoration procedures for complete
oral rehabilitation or reconstruction. Procedures related to the reconstruction of a patient's correct vertical
dimension of occlusion (VDO).

16 Dental Clinical Policy & Coverage Guideline Update Bulletin: January 2018
Coverage Guideline Updates
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Single Tooth Indirect Restorations
(continued)
Feb. 1, 2018 Any Dental Procedure performed solely for cosmetic/aesthetic reasons (cosmetic procedures are those procedures that improve physical appearance).