Embed Size (px)
Citation preview

JANUARY 2020 - CODING 2020 Critical Care Coding: How to Get Physicans and Coders Singing from the Same Sheet of Music
DESCRIPTION Providing critical care services often means one thing to coders and another to seasoned clinicians. The speaker will Analyze the documentation and coding requirements woven into a nuanced discussion of common critical-care presentations.
OBJECTIVES • Providing critical care services often means one thing to coders and another to seasoned
clinicians. The speaker will Analyze the documentation and coding requirements woven into a nuanced discussion of common critical-care presentations.
• Review multiple specific critical care clinical presentations and dispel common misperceptions regarding who qualifes for critical care
• Discuss critical care coding issues including: bundled services, time requirements, and CPR • Identify documentation and coding requirements to appropriately report critical care services
1/30/2020, 9:00 AM - 10:00 AM, 2020 Critical Care Coding: How to Get Physicans and Coders Singing from the Same Sheet of Music
FACULTY Rebecca B. Parker, MD, FACEP
DISCLOSURE (+) No significant financial relationships to disclose

Critical CareRebecca Parker, MD, FACEP
Chief Medical Affairs Officer, Envision Physician Services
Past President, ACEP

Objectives
� Identify documentation and coding requirements to appropriately report critical care services
� Discuss critical care coding issues including: bundled services, time requirements, and CPR
� Review and dispel common misperceptions regarding specific critical care clinical presentations


Critical Care Definition

CPT & CMS Definition
An illness or injury that acutely impairs one or more vital organ systems such that there is a high
probability of imminent or life threatening deterioration in the patient’s condition.

CPT & CMS Definition
Critical care services are a physician’s (or other qualified health care professional’s*) direct
delivery of medical care for the critically ill or injured patient.
It involves decision making of high complexity to assess, manipulate and support vital organ system failure and/or to prevent further life threatening
deterioration of the patient’s condition.

CPT & CMS Definition
� Examples of vital organ systems include, but not limited to:ü CNS failureü Circulatory failureü Shockü Renal, hepatic, metabolic, and/or respiratory failure

CMS Adds
“…the failure to initiate these interventions on an urgent basis would likely result in sudden,
clinically significant or life threatening deterioration of the patient’s condition.”
It must be medically necessary and reasonable.

Provider Education: KISS
To meet CC requirements, answer YES to all 3 questions:
1. Is at least one vital organ system acutely impaired?
2. Is there a high probability of imminent, life-threatening deterioration?
3. Did you intervene to prevent further deterioration of the patient’s condition?
**In addition to YES, the physician request and time requirement greater than 30 minutes must be met.

“Butt Out of Seat” cases*
*Dr. Jay Edelberg

Critical Care vs 99285

CPT Definition:99285
� Emergency department visit for the evaluation and management of a patient, which requires these 3 key components within the constraints imposed by the urgency of the patient's clinical condition and/or mental status:
A comprehensive history;A comprehensive examination; andMedical decision making of high complexity
� Usually, the presenting problem(s) are of high severity and pose an immediate significant threat to life or physiologic function.

CPT Appendix C: 99285 Examples� Emergency department visit for a patient with a complicated overdose requiring
aggressive management to prevent side effects from the ingested materials.
� Emergency department visit for a patient exhibiting active, upper gastrointestinal bleeding.
� Emergency department visit for a previously healthy young adult patient who is injured in an automobile accident and is brought to the emergency department immobilized and has symptoms compatible with intra-abdominal injuries or multiple extremity injuries.
� Emergency department visit for a patient with an acute onset of chest pain compatible with symptoms of cardiac ischemia and/or pulmonary embolus.
� Emergency department visit for a patient who presents with a sudden onset of "the worst headache of her life," and complains of a stiff neck, nausea, and inability to concentrate.
� Emergency department visit for a patient with a new onset of a cerebral vascular accident.
� Emergency department visit for acute febrile illness in an adult, associated with shortness of breath and an altered level of alertness.

CPT Appendix C: 99291 Examples� First hour of critical care of a 65-year-old male with septic shock
following relief of ureteral obstruction caused by a stone.
� First hour of critical care of a 15-year-old with acute respiratory failure from asthma.
� First hour of critical care of a 45-year-old who sustained a liver laceration, cerebral hematoma, flailed chest, and pulmonary contusion after being struck by an automobile.
� First hour of critical care of a 65-year-old female who, following a hysterectomy, suffered a cardiac arrest associated with a pulmonary embolus.
� First hour of critical care of a 6-month-old with hypovolemic shock secondary to diarrhea and dehydration.
� First hour of critical care of a 3-year-old with respiratory failure secondary to pneumocystis carinii pneumonia

99285 vs 99291
� Considerable overlap between 99285 and 99291 CPT descriptors99285 examples tend to suggest a high risk presentation � MVA compatible with intra-abdominal/extremity
injuries
� 99291 examples consistent with high risk presentation PLUS positive finding or dx� Septic shock� Auto ped with liver lac, pulmonary contusion� CMS: need to intervene to prevent deterioration

Critical Care Practice Management ConsiderationsGetting physician leadership buy in.

Critical Care – the Missed Code
� Total (all payer) rate� about 3-6% of E/M codes depending on type of ED
� 2018 CMS Medicare acuity data (formerly BESS)� National: 7.8%� CO: 8.9%� TX: 8.9%� MT: 4.7%� CA-S: 12.1%; DC: 9.7%� PR: 0.6%; VI: 0.02%
� Must be audit defensible� Documentation and policy

Critical Care Value
� 99285� 2019 WRVU: 3.80� 2019 MFS: $176.23
� 99291� 2019 WRVU: 4.50 � 2019 MFS: $226.32
� Missed CC = about $50 lost revenue� 60k/yr ED goes from 2 to 4% CC� Revenue increases by over $60,000/yr� Must still be compliant and defensible!!!

Physicians Must Lead - CahabaPart B Critical Care CPT 99291 Widespread Prepayment Targeted Review Results
Posted July 19, 2013 in Part B Medical Review (MR) Part B has recently completed the widespread prepayment widespread targeted review of CPT 99291, Critical Care, Evaluation and Management of the Critically Ill or Injured Patient: First 30-74 Minutes. Claims which met the edit parameters were randomly selected across the provider community. The error rates for this review were 80% for Alabama, 92% for Georgia, and 70% for Tennessee. Based on the outcomes of this review the prepayment widespread targeted review will be continued. Review of the claims submitted indicated that the documentation did not support critical care services were provided as submitted on the claim by the billing of 99291.

Cahaba
Medical record reviews indicated the following:
Critical care time was not documented; the reviewer could not determine the amount of time the physician and/or hospital staff spent with patients.
CPT 99291 was billed with less than 30-74 minutes documented;Examples:
Total critical care time of 15 minutes was documented in the record
Patient had arrived on full life support and was pronounced dead soon after arrival
Documentation did not support that the physician and/or hospital staff were engaged in active face to face critical care of a critically ill or critically injured patient.

CC justification: The Physician Opinion(and documentation)
“God heals, and the physician takes the
fee.”Benjamin Franklin

Critical Care TimeNuts and bolts

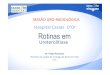
Critical Care Time
Total Duration of Critical Care
Appropriate CPT Codes
Less than 30 minutes Appropriate 99281-99285
30-74 minutes 99291 X 1
75-104 minutes 99291 X 1 and 99292 X 1
105-134 minutes 99291 X 1 and 99292 X 2
135-164 minutes 99291 X 1 and 99292 X 3
165-194 minutes 99291 X 1 and 99292 X 4
194 minutes or longer 99291 & 99292 as above illustration

Critical Care Time
� Time based code� Must meet 30 minutes and document specific number of
minutes
� CC time defined as� At the bedside� On the unit and immediately available to patient� Full attention: cannot provide services to any other
patient during that period of time� May be aggregated – doesn’t need to be continuous

Critical Care Time
� CC time defined as (cont):� Reviewing test results or imaging studies� Discussing patient’s care with other medical staff� Documenting in the record� Time spent with other decision makers when patient is
unable to make decisions� Time to perform procedures such as gastric intubation,
temporary transcutaneous pacing, ventilator management, peripheral vascular access

The following services are included in critical care time, not reported separately:
� Interpretation of cardiac output (93561, 93562)� Chest x-rays, professional component (71045, 71046)� Blood gases, information stored on computers (e.g.
ECGs, blood pressures, hematologic data)� Gastric intubation (43752, 91105)� Pulse oximetry (94760, 94761, 94762)� Temporary transcutaneous pacing (92953)� Ventilator management (94002-94004, 94660, 94662)� Vascular access procedures (36000, 36410, 36415,
36591, 36600)

Critical Care Conundrums

CC Time Conundrums
Presence of physician or APP
� CMS and CPT agree:� MLN Matters Number: MM5993 Revised: Time spent off
the unit or floor where the critically ill/injured patient is located (i.e., telephone calls, whether taken at home, in the office, or elsewhere in the hospital) may not be reported as critical care time because the physician is not immediately available to the patient. This time is regarded as pre- and post service work bundled in evaluation and management services.

Controversy case:EMS ST Elevation MI
� EMS calls with 72-year-old male patient en route with chest pain. 10-minute ETA.
� Pre arrival ECG sent and shows ST elevation MI.
� Cath lab team activated pre arrival.
� After 25 minutes patient leaves department to cath lab.
� Does patient meet 30-minute threshold for critical care?

CC Time Conundrums
Team activation
� CMS: Concurrent critical care services provided by each physician must be medically necessary and not provided during the same instance of time.
� CPT: Only one physician/provider may report services for a given hour of critical care, even if more than one physician/provider has rendered critical care to the patient (CPT Assistant July ’06).

Controversy case:Level 1 Trauma Activation
� 22-year-old female in high velocity MVA, ejected from the vehicle.
� Obvious femur fracture, confused and combative with major contusions to head and face.
� Level 1 trauma team ready on arrival.
� After 60 minutes in ED trauma bay and after intubation goes to ICU.
� Who bills for critical care?

CC Time Conundrums
� Time spent speaking with family members or surrogate decision-makers counts if (MLN Matters Number: MM5993):� The patient is unable or incompetent to participate in
giving history and/or making treatment decisions; � Obtaining a history, reviewing the patient’s condition or
prognosis or discussing treatment or limitation(s) of treatment
� “provided the conversation bears directly on the management of the patient”
� A summary in the medical record that supports this medical necessity.
� CPT policy is consistent with CMS

Controversy case:Elderly end of life care
� 90-year-old female history of lung cancer on chemotherapy with fever, cough, pneumonia, sepsis.
� Patient oriented, competent, requests hospice and does not want antibiotics or fluids. Just wants to go home.
� As you are arranging, etc 50 year old son, the POA, pulls you aside and wants to discuss his mother’s status, wishes and wants to discuss hospice.
� Can you count your conversation with son towards critical care time?

CC Time Conundrums: Past Midnight� Scenario 1: How would you code a patient who presents to the
ED at 2335 Day 1, with CC services beginning at that time and performed continuously until 0015 on Day 2, with no more CC services performed on Day 2?
Answer: Critical care 99291 can be reported for Day 1.
� Scenario 2: How would you code a patient who presents to the ED at 2335 Day 1, with CC services beginning at that time and performed continuously until 0015 on Day 2, at which time continuous CC services are interrupted; CC services are reinitiated at 0130 Day 2, with an additional 65 minutes provided on Day 2 following the re-initiation?
Answer: Critical care 99291 can be reported for Day 1, and a second 99291 reported for Day 2.

CC Conundrum: can CC and9928X be Reported Together? � Patient presents with chest pain and has a 99285
service provided. While waiting for a bed he has an episode of hypotension and run of ventricular tachycardia. 99291 critical care criteria met.� CPT: May report 9928x plus 99291 by same
physician on same calendar day� CMS: CMS Transmittal 1548 specifically states:
Hospital emergency department services are not payable for the same calendar date as critical care services when provided by the same physician to the same patient.

Critical Care & Procedures

CC Time: Procedures
� Time spent performing unbundled procedures is not considered as counting toward CC time
� Unbundled procedures are separately billed
� Examples� Wound repair� Intubation� Chest tubes� Central lines� CPR

CC Time Documentation: Procedures
� Recommended that the physician note that separately billed procedure time was not included in CC time� “the time involved in the performance of separately
reportable procedures was not counted toward critical care time” or
� “exclusive of separately billed procedures” � To avoid reduction of time by payers

CPR & CC Time: CPT Assistant July 2012
Question: May a physician report CPT code 92950 for chestcompressions performed by another member of the clinical teamwhen the physician manages the cardiopulmonary resuscitation?
Answer: Yes. If the physician manages the cardiopulmonaryresuscitation (and is present face to face), then the physicianmay report code 92950, Cardiopulmonary resuscitation (eg, incardiac arrest). It is not required that the physician performs theactual chest compressions and/or mouth to-mouth resuscitationor bagging in order to report code 92950. It is also appropriatefor a physician to report code 92950 with codes 99291 and99292 (for the critical care services) when cardiopulmonaryresuscitation and critical care services are performed on thesame day by the same physician. Both services should be clearlydocumented in the medical record.

Controversy case:Critical Care and CPR
� You are called to room 3 for a chest pain patient your PA saw for sudden unresponsiveness.
� Initial ECG was normal and cardiac work up started. Watchful RN in room said patient said “my chest pain is back” and became unresponsive.
� Team there, ACLS started, you intubate (took 5 minutes), round of meds given and pulse returns after 10 minutes.
� Repeat ECG shows STEMI and alert called. Your entrance into room until he leaves, 60 minutes.
� Can you bill critical care 99291? 92950?

NPPs (Non-Physician Providers)

CC Time: NPPs
� Non-physician practitioners (NPP)� May report 99291/92 using NPP NPI if CC is within state
and hospital scope of practice� CMS: Shared service between physician and NPP may not
be reported as sum of individual times.� Must report based on either NPP or physician time

CPT 2013
� Editorial change to clarify usage by NPPs
� Critical care is the direct delivery by a physician(s) or other qualified health care professional of medical care for a critically ill or critically injured patient

NPP Limitations
� CC services of NPP varies based on: � Hospital bylaws� State scope of practice laws� Non-CMS individual payer policy

Teaching Physicians

Critical Care Time: Teaching Physicians
� Time that does not count� Teaching time at the bedside� Resident time alone at the bedside
� CMS: “The medical review criteria are the same for the teaching physician as for all physicians…”
� Documentation� TP note may tie into resident note but must support all
CC criteria and time is only TP time

Critical Care and Teaching Physicians
CMS: The teaching physician medical recorddocumentation must provide substantive information including:
(1) the time the teaching physician spent providing critical care,
(2) that the patient was critically ill duringthe time the teaching physician saw the patient,
(3) what made the patient critically ill, and
(4) the nature of the treatment and management provided by the teaching physician.

Critical Care and Teaching Physicians
CMS example of acceptable documentation:
“Patient developed hypotension and hypoxia; I spent 45 minutes while the patient was in this condition, providing fluids, pressor drugs, and oxygen. I reviewed the resident’s documentation and I agree with the resident’s assessment and plan of care.”

Critical Care & Pediatrics

Pediatrics – Critical Care
� Critical care same (99291, 99292)� Other critical codes inpatient only & per day
� Neonatal Critical Care (99468-99469)� Pediatric Critical Care (99471-99472, 99475-99476)
� Interfacility transport of critically ill or injured 24 months or under, � Face-to-face, 99466 first 30-74 minutes, 99467 next 30� Supervision by control physician, 99485 first 30 minutes,
99486 next 30� Available for EP doing peds transport (e.g. flight)

Pediatrics – Critical CareThe Clues are Different!� Typical cases
� Fever/sepsis� Respiratory distress (status asthmaticus,
bronchitoitis/RSV, pneumonia, etc)� SVT/congenital heart disease� Status epilepticus/complex febrile seizure� Abuse
� History heavily depend on non-patient sources

Pediatrics – Critical CareThe Clues are Different!� Physical exam
� General; alert and playful, cries on exam consoles normally� Severity: lethargic, not interactive, afraid of parent/adult
� Cardiovascular; tachycardic � Severity: perfusion clues such as delayed capillary refill,
mottled, altered mental status� Respiratory
� Severity: nasal flaring, retractions, abdominal pushing, grunting� Skin; capillary refill, pink
� Severity: delayed refill, gray/ashen, yellow/icteric, unexplained bruising
� Neuro; non focal, normal for developmental age, walks normally to parent� Severity: focal findings, intermittent seizure activity

Pediatrics – Critical CareThe Clues are Different!
� Evaluation and interventions may be limited, but support severity of illness:� IV/IO� High flow oxygen, end
tidal CO2, bipap, intubation
� IV fluid boluses, antibiotics, drips
� XR, glucose check, basic labs-pending
� Transfer early

Critical Care DocumentationWhen is it Critical Care?Tricks of the Trade

Critical Care Documentation
� Accurate time statement always required� Exact number of minutes, 30 or more� Exclusive of separately billed procedures� Document 99285 elements or acuity caveat if any
potential to be down-coded to 99284-285
� ED Course must establish medical necessity� Should support high complexity MDM� Include diagnostic and therapeutic interventions
performed and/or considered even if no positive response
� Serial assessments

When is it Critical Care
� Is it CC?� Disposition may help as far as suggesting
that CC should be considered:� ICU admit� Direct to OR� Death in the ED
� Disposition suggesting likely not CC:� Floor or tele admit� Discharged home

When is it Critical Care
� Documentation suggesting may not be CC � “NAD”� Normal VS� “Resting comfortably”� Minimally documented and/or benign ED
Course that does not support medical necessity
� Psychiatric cases� Maybe: High risk presentation with
subsequent r/o of critical illness/injury

When is it Critical Care
� May not be CC� Urgent call and arrival of specialist is not CC unless
substantial portion of workup and initiation of treatment by EP
� Abnormal lab values alone do not support CC unless MDM reflects high complexity MDM and initiation of life-saving assessment/treatment or prevention of serious deterioration
� Consider Medical Necessity statement if above scenarios justify CC

Critical Care Documentation“Medical Necessity” statement:
� “Organ system(s) at risk is…”� Differential diagnosis � “What and why” as far as diagnostic and/or therapeutic
interventions undertaken by YOU� Critical lab, imaging EKG findings documented and
significance addressed� ED Course reflects frequent re-assessments and decision-
making� Likelihood of life-threatening deterioration

Critical Care � Risk management/compliance approach.
Consider reviewing: � CC >2 hours � Questionable medical necessity� High (and low) frequency providers � Importance of “Medical Necessity” note
in questionable cases� Number of minutes and exclusion
statement

Critical Care ExamplesTop 3 Scenarios

Examples
� Stroke syndromes� Consider CC
� Abnormal vital signs requiring treatment� Any airway issues� Stroke Alerts� Start/consider TPA � Rapid assessment and transfer for definitive treatment at a
stroke center� Example dx: intraventricular hemorrhage, intracranial
hemorrhage (ICH), subarachnoid hemorrhage (SAH), non-ischemic and ischemic stroke
� Probably not CC� Stable patient with completed stroke

Examples
� Dyspnea� Consider CC
� Bi-PAP/CPAP� High flow oxygen, continuous nebs and ICU admit � Altered mental status� Impending respiratory failure documented � Intubation performed or considered� CHF (usually with pulmonary edema or severe dyspnea) with
nitro drip, lasix/bumex, Bi-PAP/CPAP� Status asthmaticus (hour long NEB, frequent NEB, steroids,
magnesium SO4, ketamine, Bi-Pap/CPAP, frequent assessment)� Probably not CC
� 2-4 nebs or continuous nebs plus steroids and clear� Dispo home

Examples
� Psych� Consider CC
� Delirium or organic cause identified plus ICU admit � Overdose requiring intervention and admission
� Probably not CC� Overdose cleared in the emergency department for
psychiatric assessment� Intoxicated awaiting sobering� Agitation/pure psych� Suicide assessment

In closing…We’re almost there!

Provider Education: KISS
To meet CC requirements, answer YES to all 3 questions:
1. Is at least one vital organ system acutely impaired?
2. Is there a high probability of imminent, life-threatening deterioration?
3. Did you intervene to prevent further deterioration of the patient’s condition?
**In addition to YES, the physician request and time requirement greater than 30 minutes must be met

Critical Care Documentation
� Accurate time statement always required� Exact number of minutes, 30 or more� Exclusive of separately billed procedures� Document 99285 elements or acuity caveat if any
potential to be down-coded to 99284-285
� ED Course must establish medical necessity� Should support high complexity MDM� Include diagnostic and therapeutic interventions
performed and/or considered even if no positive response
� Serial assessments

Still unsure?
� Ask yourself two questions:1. Was patient admitted (based on medical necessity) to
ICU or immediate dispo to OR?� If yes: strongly consider CC� If no: is it really CC?� If no (and you think it is CC): consider a Medical
Necessity note2. Will the patient die or deteriorate (soon) if you don’t
do something (quickly)?� If yes: document CC time� If no: is it really CC? � If no (and you think it is CC) : consider a
Medical Necessity note

Critical Care ExamplesAppendix - Complete

Critical Care Examples
� Chest pain� Consider CC
� EKG compatible with ischemia� Enzyme changes� Arrhythmias requiring treatment� Hypotension� Pain requiring ongoing IV NTG� Use of IV, heparin, lytics� Immediate dispo to cath lab or ICU � Example Dx: acute MI/STEMI, non-ST elevation MI, unstable
angina� Probably not CC
� EKG normal and given ASA per protocol� Repeat EKG, enzymes normal� SL or topical NTG only � Dispo home

Examples
� Arrhythmias� Consider CC
� If symptomatic (eg syncope, altered mental status/neuro signs, chest pain, dyspnea; not simply palpitations) or significant co-morbidities such as ingestion
� Treated with electricity, IV drips or multiple doses/drugs� Example dx: afib/aflutter with RVR, afib with WPW, Vtach,
PSVT� Probably not CC
� PAT converted in field� Post spontaneous conversion in stable patient� Asymptomatic AF with single bolus of diltiazem

Examples
� Hypertension – new ICD-10 codes!� Consider CC
� Hypertensive emergency & crisis� Both end organ damage, crisis rapidly rising� End organ(s) affected
� Brain� Heart� Kidney
� Treatment ongoing and typically ICU admit� Probably not CC
� Hypertensive urgency� Incidental finding unrelated to main problem� May get PO or IV Rx but usually discharged or floor
admit

Examples
� Syncope� Consider CC
� Syncope plus a significant co-morbidity. For example:� Arrhythmias such as new onset AF� Lower or UGI bleed � Significant hypovolemia� Altered mental status or seizure� Pulmonary embolism� Dispo: typically admit ICU
� Probably not CC� “Weak and dizzy”� No significant co-morbidity� Simple faint

Examples
� Seizures� Consider CC
� Status epilepticus� Complex febrile seizure (peds)� Context of trauma, OD or ingestions� ETOH or drug withdrawal (delirium tremors)
� Probably not CC� Recurrent with noncompliant or sub-therapeutic meds

Examples
� Stroke syndromes� Consider CC
� Abnormal vital signs requiring treatment� Any airway issues� Stroke Alerts� Start/consider TPA � Rapid assessment and transfer for definitive treatment at a
stroke center� Example dx: intraventricular hemorrhage, intracranial
hemorrhage (ICH), subarachnoid hemorrhage (SAH), non-ischemic and ischemic stroke
� Probably not CC� Stable patient with completed stroke

Examples
� Dyspnea� Consider CC
� Bi-PAP/CPAP� High flow oxygen, continuous nebs and ICU admit � Altered mental status� Impending respiratory failure documented � Intubation performed or considered� CHF (usually with pulmonary edema or severe dyspnea) with
nitro drip, lasix/bumex, Bi-PAP/CPAP� Status asthmaticus (hour long NEB, frequent NEB, steroids,
magnesium SO4, ketamine, Bi-Pap/CPAP, frequent assessment)� Probably not CC
� 2-4 nebs or continuous nebs plus steroids and clear� Dispo home

Examples
� Abdominal pain� Consider CC
� Immediate dispo to OR (eg AAA, perforated viscus)� Hemodynamic instability (low blood pressure, elevated HR,
fever)� Peritonitis� ICU admit (bowel ischemia, sepsis)
� Probably not CC� Appy/diverticulitis: routine and admitted to floor � Perforated appy or diverticulitis admitted to floor

Examples
� Trauma� Consider CC
� Hemodynamic instability/abnormal VS� Possible cord injury� Unresponsive/altered mental status� Penetrating trauma (gun shot, stabbing)� Procedures such as chest tube, intubation, central line� Dispo to OR or transfer to Trauma Center
� Probably not CC� Mechanism alone in alert patient w/o complaints� Isolated extremity injuries w/o neurovascular compromise

Examples
� Ingestions� Consider CC
� High lethality agent requiring intervention or close monitoring� Seizures, coma, arrhythmias, hypotension� Active co-management with poison control
� Probably not CC� Benign overdose with watchful waiting
� Severe allergic reactions� Consider CC
� Stridor, wheezing. hypotension� IV epi or pressors
� Probably not CC� Epipen in field and/or IV steroids and clears

Examples
� Metabolic� Consider CC
� Most admitted DKA and/or other metabolic acidosis admitted to ICU
� Hyperosmolar states (e.g. coma)� Example dx: non-anion gap/anion gap metabolic acidosis,
diabetic ketoacidosis, non-ketotic hyperosmolar coma, hyperthyroidism/thyroid storm, myxedema coma
� Probably not CC� Mild DKA treated on floor or in ED and DC’d

Examples
� Fluid and electrolyte abnormalities� Consider CC
� Abnormal EKG � Symptomatic (e.g. confusion, muscle weakness)� Requires IV replacement treatment� Documentation of a critical value
� Comment and/or treatment� Emergent dialysis required� Acute renal failure� Example dx: hyperkalemia, hypercalcemia

Examples
� Sepsis� Consider CC
� Sepsis bundle management� Sepsis alert� Lactate levels and repeat levels� 30 ml/kg IV fluid boluses early� Antibiotics early� Common procedures: central line, US for hydration status� ICU admit
� Immunocompromised patient� Transplants/cancer patients
� Most infectious disease admits to ICU� Pneumonia, encephalitis, meningitis, endocarditis

Examples
� Pediatric� Consider CC
� Any shock-like state (blood pressure last VS affected)� Altered mental status� Typical cases
� Respiratory distress� Dehydration� Fever/sepsis� Abuse� Status epilepticus/complex febrile seizure� SVT/congenital heart disease
� Evaluation and intervention may be limited� IV/IO, intubation, transfer� IV fluids, antibiotics� XR, basic labs-pending

Examples
� Psych� Consider CC
� Delirium or organic cause identified plus ICU admit � Overdose requiring intervention and admission
� Probably not CC� Overdose cleared in the emergency department for
psychiatric assessment� Intoxicated awaiting sobering� Agitation/pure psych� Suicide assessment

Examples
� Environmental� Consider CC
� Hypothermia: with aggressive re-warming� Lightening strike� CO with signs/symptoms requiring treatment,
especially hyperbaric chamber