Embed Size (px)
Citation preview
ORIGINAL RESEARCH
Japanese Expert Panel Meeting on the Managementof Prostate Cancer with Bone Metastases
Shunji Takahashi . Seigo Kinuya . Norio Nonomura . Nobuo Shinohara . Kazuhiro Suzuki . Hiroyoshi Suzuki .
Katsumasa Nakamura . Takefumi Satoh . Ukihide Tateishi . Toshiyuki Yoneda . Hiroyuki Horikoshi .
Tsukasa Igawa . Takao Kamai . Mitsuru Koizumi . Takeo Kosaka . Nobuaki Matsubara . Hideaki Miyake .
Atsushi Mizokami . Takashi Mizowaki . Naoki Nakamura . Masahiro Nozawa . Takeo Takahashi .
Hiroji Uemura . Motohide Uemura . Akira Yokomizo . Mana Yoshimura . Yoshiyuki Kakehi
Received: September 11, 2018 / Published online: December 11, 2018� The Author(s) 2018
ABSTRACT
Introduction: The incidence of prostate cancerin Japan continues to increase, necessitating thecontinued development of effective therapiesand strategies. Recent advances in treatmentshave improved the prognosis of metastatic dis-ease and highlighted the importance of treatingbone metastases to reduce the incidence ofskeletal complications and improve patients’quality of life. With the increasing number oftreatment options that have become available,including bone-targeted therapy with the alpha
emitter radium-223 dichloride (Ra-223), Japa-nese clinicians are faced with making difficultdecisions on the choice of optimal treatmentstrategy. In such situations, guidance based onexpert opinions can be beneficial.Methods: A panel meeting of 27 Japaneseexperts in the management of prostate cancerwas held to share opinions and to establishconsensus recommendations on key clinicalquestions. Panelists were asked to vote on morethan 40 questions pertinent to prostate cancer,and the answers helped guide a comprehensivediscussion.Results: The panel reached a consensus on keytopics related to the optimal treatment strategyfor Ra-223 therapy, namely, that patients withsymptomatic, metastatic castration-resistantprostate cancer (CRPC) would benefit mostfrom the use of this agent and that this treat-ment therapy should be provided beforechemotherapy. Other topics that achieved
Enhanced digital features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.7306703.
Electronic supplementary material The onlineversion of this article (https://doi.org/10.1007/s40487-018-0088-0) contains supplementary material, which isavailable to authorized users.
S. Takahashi (&) � M. KoizumiThe Cancer Institute Hospital of the JapaneseFoundation for Cancer Research, Koto-ku, Tokyo,Japane-mail: [email protected]
S. Kinuya � A. MizokamiKanazawa University, Kanazawa, Ishikawa, Japan
N. Nonomura � M. UemuraOsaka University, Yamadaoka, Suita, Osaka, Japan
N. ShinoharaHokkaido University, Sapporo, Hokkaido, Japan
K. SuzukiGunma University, Maebashi, Gunma, Japan
H. SuzukiToho University Sakura Medical Center, Sakura,Chiba, Japan
K. Nakamura � H. MiyakeHamamatsu University School of Medicine,Hamamatsu, Shizuoka, Japan
T. SatohKitasato University School of Medicine, Sagamihara,Kanagawa, Japan
Oncol Ther (2018) 6:157–171
https://doi.org/10.1007/s40487-018-0088-0

consensus included: monitoring for osteoporo-sis and providing treatment if necessary duringandrogen deprivation therapy; performingmagnetic resonance imaging in the presence ofdiscrepancies in bone scintigram and computedtomography scans; monitoring alkaline phos-phatase during CRPC treatment; using osteo-clast-targeting in patients with CRPC with bonemetastases; and using osteoclast-targeted agentscombined with Ra-223.Conclusion: These consensus recommenda-tions and the updated information whichbecame available subsequent to the panelmeeting included here provide useful informa-tion for clinicians to aid in designing optimaltreatment strategies for their patients.Funding: Bayer Yakuhin Ltd.
Keywords: Bone metastasis; Castration-resistant; Japanese; Prostate cancer;Therapeutic consensus
INTRODUCTION
The incidence of prostate cancer is increasingamong Japanese males, with an estimated86,100 new cases diagnosed by the National
Cancer Center Japan in 2017 [1]. For patientswith metastatic disease, recent advances intreatment strategies have improved their prog-nosis and disease management. As the mostfrequent metastatic site of prostate cancer isbone, it is important to treat bone metastases inorder to reduce the incidence of skeletal com-plications and improve patients’ quality of life.
In Japan, various therapeutic options arenow available for the treatment of metastaticprostate cancer. As a result, clinicians are oftenfaced with the daunting challenge of deter-mining the optimal management strategy foran individual patient, including diagnosis andmonitoring. To facilitate the decision-makingprocess regarding the optimal treatment for apatient who has castration-resistant prostatecancer (CRPC) with bone metastases, a thor-ough review of the recent advances in basic andclinical research, which have resulted in theintroduction of drugs with novel modalities, isrequired .
For decades, prostate cancer was treated pri-marily with androgen deprivation therapy(ADT). Docetaxel (DOC) was introduced at thebeginning of the twenty-first century and hasproven to be effective in the treatment of CRPC.In 2014, enzalutamide (ENZ) and abiraterone(ABI) were introduced in Japan as treatments forCRPC, as was cabazitaxel, after trials reported
T. SatohSato Takefumi Zenritsusen Clinic, Machida, Tokyo,Japan
U. TateishiTokyo Medical and Dental University, Bunkyo-ku,Tokyo, Japan
T. YonedaOsaka University Graduate School of Dentistry,Suita, Osaka, Japan
T. YonedaIndiana University, Bloomington, IN, USA
H. HorikoshiGunma Prefectural Cancer Center, Ohta, Gunma,Japan
T. IgawaKurume University, Fukuoka, Fukuoka, Japan
T. KamaiDokkyo Medical University, Shimotsuga-gun,Tochigi, Japan
T. KosakaKeio University, 35 Shinanomachi, Shinjuku-ku,Tokyo, Japan
N. Matsubara � N. NakamuraNational Cancer Center Hospital East, Kashiwa,Chiba, Japan
T. MizowakiKyoto University, Sakyo, Kyoto, Japan
M. NozawaFaculty of Medicine, Kindai University, Osaka-Sayama, Osaka, Japan
T. TakahashiSaitama Medical University, Kawagoe, Saitama,Japan
H. UemuraYokohama City University Medical Center,Yokohama, Kanagawa, Japan
A. YokomizoHarasanshin Hospital, Fukuoka, Fukuoka, Japan
158 Oncol Ther (2018) 6:157–171

improvements in survival following treatmentwith DOC. Bone-targeted therapy with thealpha emitter radium-223 dichloride (Ra-223)was approved in Japan in June 2016. Ra-223 isthe first agent found to improve both overallsurvival (OS) and time to symptomatic skeletalevents, as shown in the ALSYMPCA trial [2, 3];however, optimal patient selection and theoptimal timing to initiate therapy have yet to bedetermined. Given the currently limited real-world experience with Ra-223, expert opinions,rather than clinical guidelines offering evi-dence-based recommendations, would be help-ful for such decision-making in daily clinicalpractice.
We therefore organized a Japanese expertpanel meeting for the management of prostatecancer with bone metastases, a forum at whichexperts could share their experiences and reachconsensus on the key clinical questions relatedto the management of prostate cancer withbone metastases. The main focus of this meet-ing was to determine the optimal incorporationof Ra-223 into CRPC therapeutic regimens, butpanelists also discussed other important andcontroversial topics in the areas of imaging andmonitoring of prostate cancer.
METHODS
Held on September 3, 2016, in Tokyo, Japan,the consensus panel included 27 experts from avariety of specialties involved in the manage-ment of prostate cancer (Table 1). Of the panelparticipants, 96% were actively working atinstitutions that met facility requirements forthe use of Ra-223, although 60% did not haveany personal experience with Ra-223 treatmentin clinical practice (except in clinical trials) atthe time of meeting. Steering committee
members were selected from the leadership ofsocieties associated to the field and nominatedby the participating panelists with no influencefrom the sponsor/funding agency.
Since the goal of the panel meeting was toaddress practical clinical needs, identifying real-world clinical questions was essential. The for-mat of this meeting broadly followed that of theSt Gallen Advanced Prostate Cancer ConsensusConference (APCCC) 2015 [4], and the simpli-fied method of the Delphi process was usedthroughout [5]. Before the meeting, members ofthe steering committee discussed and agreedupon the goal of the meeting. They identifiedclinical questions that would address issuespertinent to the management and monitoringof patients with CRPC with bone metastases.panelists were selected for their relevant exper-tise and were asked to submit examples ofclinically relevant questions that are commonlyraised during their daily practice. Starting withthe list of clinical questions in the currentJapanese Urological Association Guidelines,panelists deleted questions that were not clini-cally relevant to the topic on hand and addedothers they expected to be asked. The questionsgathered using this process were categorizedand prioritized by the steering committee, andthe final version of the list was presented at theconsensus panel meeting.
During the forum, all of the questions werepresented to the panel in a multiple-choiceformat. panelists were polled anonymouslyusing an electronic voting system. Those whowere unable to vote for a best choice for anyreason could choose ‘abstain’ as an option (seeElectronic Supplementary Material [ESM]Table S1 for details). Each question was votedon only once, and there was no option to re-vote. After voting, the panel discussed theresults and shared opinions.
The data presented in this consensus docu-ment are based on the voting results and relateddiscussions and, therefore, do not report onresearch conducted on human subjects. Thisarticle does not contain any studies withhuman participants or animals performed byany of the authors. All panelists have reviewedand approved this manuscript.
A. YokomizoKyushu University, Fukuoka, Fukuoka, Japan
M. YoshimuraTokyo Medical University, Shinjuku-ku, Tokyo,Japan
Y. KakehiKagawa University, Kita-gun, Kagawa, Japan
Oncol Ther (2018) 6:157–171 159

Table 1 Panel members
Role Name Specialty Affiliations
Meeting Chair
SC Member
Takahashi, Shunjia Medical Oncology The Cancer Institute Hospital of the
Japanese Foundation for Cancer Research
Meeting Chair
SC Member
Kinuya, Seigo Nuclear Medicine Kanazawa University
Meeting Chair
SC Member
Nonomura, Norio Urology Osaka University
Meeting Chair
SC Member
Shinohara, Nobuo Urology Hokkaido University
Meeting Chair
SC Member
Suzuki, Kazuhiro Urology Gunma University
Meeting Chair
SC Member
Suzuki, Hiroyoshi Urology Toho University Sakura Medical Center
Meeting Chair
SC Chair
Kakehi, Yoshiyuki Urology Kagawa University
Plenary Speaker Nakamura, Katsumasa Radiation Oncology Hamamatsu University School of Medicine
Plenary Speaker Satoh, Takefumi Urology Kitasato University School of Medicine
Plenary Speaker Tateishi, Ukihide Nuclear Medicine Tokyo Medical and Dental University
Plenary Speaker Yoneda, Toshiyuki Basic Science Research Indiana Universityb
Panelist Horikoshi, Hiroyuki Radiation Diagnostic Gunma Prefectural Cancer Center
Panelist Igawa, Tsukasa Urology Kurume University
Panelist Kamai, Takao Urology Dokkyo Medical University
Panelist Koizumi, Mitsuru Nuclear Medicine The Cancer Institute Hospital of the
Japanese Foundation for Cancer Research
Panelist Kosaka, Takeo Urology Keio University
Panelist Matsubara, Nobuaki Medical Oncology National Cancer Center Hospital East
Panelist Miyake, Hideaki Urology Hamamatsu University School of Medicine
Panelist Mizokami, Atsushi Urology Kanazawa University
Panelist Mizowaki, Takashi Radiation Oncology Kyoto University
Panelist Nakamura, Naoki Radiation Oncology National Cancer Center Hospital East
Panelist Nozawa, Masahiro Urology Kindai University
Panelist Takahashi, Takeo Radiation Oncology Saitama Medical University
Panelist Uemura, Hiroji Urology Yokohama City University Medical Center
Panelist Uemura, Motohide Urology Osaka University
160 Oncol Ther (2018) 6:157–171

RESULTS
The voting results on the questions are dis-cussed in detail in the following sub-sections,with the complete dataset shown in the ESMTable S1 and ESM Figs. S1–S30. The total num-ber of voters for each question included thosewho chose to abstain; however, the numbersvary between questions because some panelistsdid not vote on all questions.
Management of Castration-SensitiveProstate Cancer
First we queried the panelists about their prac-tices in the management of castration-sensitiveprostate cancer (CSPC) and the assessment andtreatment of bone disease in CSPC.
Combined Androgen Blockade as Primary ADTAt the time of this consensus meeting theJapanese Urological Association Guidelines rec-ommended combined androgen blockade(CAB) as the primary ADT (PADT) in patientswith M1 prostate cancer [6], and 73% (19/26) ofthe panel members agreed with that recom-mendation. In contrast, half of the panel at theAPCCC 2015 did not recommend CAB astreatment [7].
Treatment Strategy for Patientswith OligometastasesAccording to a recent multi-institutional anal-ysis, stereotactic body radiotherapy (SBRT) is
associated with a prolonged progression-freesurvival (PFS) in patients with oligometastaticprostate cancer recurrence who are treatment-naive [8]. Azzam et al. also reported that prog-nosis was better for men with recurrent prostatecancer treated with SBRT if they had B 4metastases [9]. Regarding the treatment strat-egy for patients with oligometastases (B 3[bone, lymph node]) at initial diagnosis, 38% ofthe panelists recommended drug treatmentalone, 15% recommended ‘radical therapy’ inaddition to drug treatment, and 27% recom-mended radiation to metastases in addition todrug treatment. Radical therapy may be anoption for oligometastases, but it should onlybe taken after careful evaluation to preventoverlooking micro-metastases.
Osteoclast-Targeting Agents for CSPCThe panel members felt that regular osteo-porosis diagnosis is important; however, as tothe timing of initiation of bone-targeted thera-pies, the opinions of the panel members weredivided. For patients with CSPC with bonemetastases, 27% prescribe osteoclast-targetingagents (zoledronic acid or denosumab) to themajority of patients, while 34% prescribe theseagents to a minority of selected patients due totheir concern for adverse events, especiallyosteonecrosis of the jaw (Fig. 1). It should benoted that steoclast-targeting agents were notshown to improve patient prognosis in severalrandomized trial results available in 2016, suchas the STAMPEDE trial [10] and a meta-analysis[11].
Table 1 continued
Role Name Specialty Affiliations
Panelist Yokomizo, Akira Urology Kyushu Universityb
Panelist Yoshimura, Mana Nuclear Medicine Tokyo Medical University
SC Steering Committeea First/corresponding authorb Affiliation at the time of meeting
Oncol Ther (2018) 6:157–171 161

Initial Diagnosis of Bone MetastasesA meta-analysis of studies comparing fluoro-2-deoxy-D-glucose positron emission tomography(PET), computed tomography (CT), magneticresonance imaging (MRI), and bone scintigra-phy for the diagnosis of bone metastases foundthat PET and MRI were comparable and thatboth were more accurate than CT and bonescintigraphy for the diagnosis of bone metas-tases [12]. On these questions, there was con-sensus within our panel, with 73% agreeing thatbone scintigraphy alone is not sufficient for theinitial diagnosis of bone metastases. There wasalso clear consensus, with the panel unani-mously (100%) agreeing that an MRI should beperformed to confirm a diagnosis of metastaseswhen there are discrepancies between the CTscan and bone scintigraphy.
Management of Patients with CRPC
The panel members were queried on theirpractices in treating patients with CRPC withdifferent types of disease progression.
The Reason for Stopping or ChangingTreatment for CRPCThere was strong consensus (91%) that at leasttwo of three criteria (prostate-specific antigen[PSA] progression, radiographic progression,and symptomatic progression) should be metbefore treatment was changed.
Osteoclast-Targeted Agent for CRPCThe panel was almost equally divided on thequestion of whether a change of drug oradministration schedule is necessary if CRPC isdiagnosed in a patient currently being treatedwith an osteoclast-targeting agent for CSPCwith bone metastases. In contrast, for a patientwho has not received such an agent, 83% rec-ommended that an osteoclast-targeting agentbe prescribed after the diagnosis of CRPC. Thepanel felt that the combined therapy would bean appropriate option, as suggested by the posthoc analysis from the COU-AA-302 study [13].Further trials are necessary to confirm theeffectiveness of this treatment strategy andoptimal patient selection.
Fig. 1 Do you prescribe osteoclast-targeting agents (zoledronic acid or denosumab) in patients with CSPC with bonemetastases? [CQ6]
162 Oncol Ther (2018) 6:157–171
Treatment Strategies on Each ProgressionStatusThe panel members discussed treatment strate-gies for CRPC patients with multiple bonemetastases but no visceral metastases (withgood performance status [PS]).
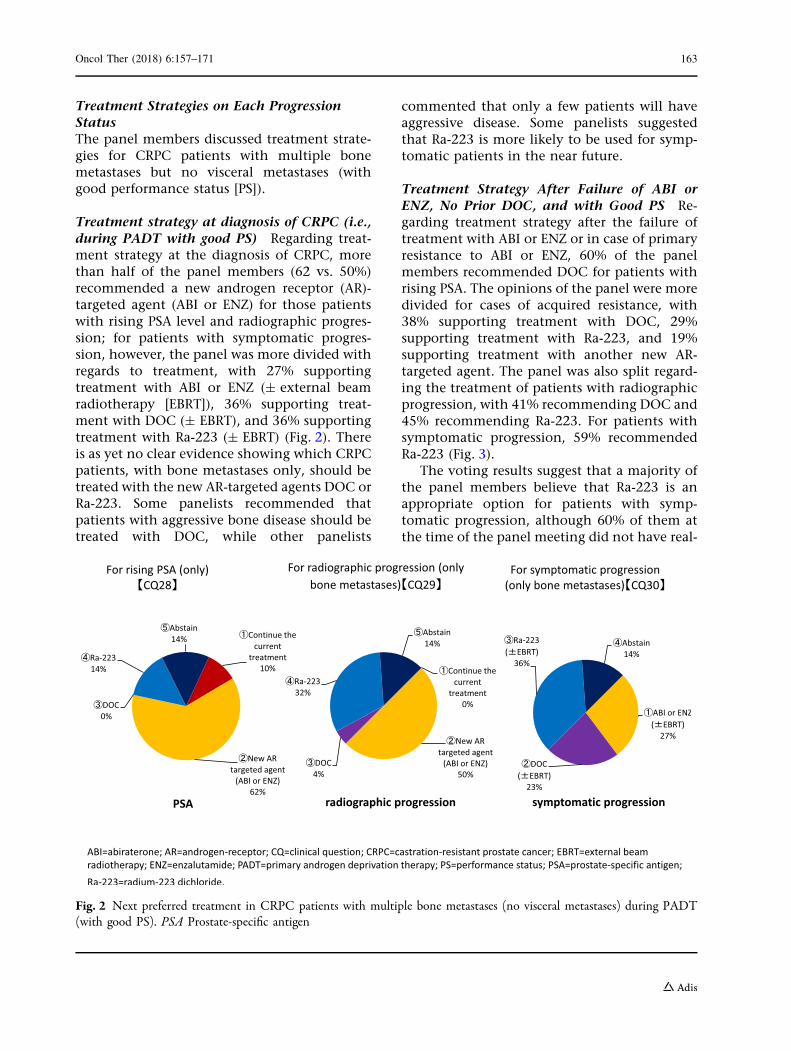
Treatment strategy at diagnosis of CRPC (i.e.,during PADT with good PS) Regarding treat-ment strategy at the diagnosis of CRPC, morethan half of the panel members (62 vs. 50%)recommended a new androgen receptor (AR)-targeted agent (ABI or ENZ) for those patientswith rising PSA level and radiographic progres-sion; for patients with symptomatic progres-sion, however, the panel was more divided withregards to treatment, with 27% supportingtreatment with ABI or ENZ (± external beamradiotherapy [EBRT]), 36% supporting treat-ment with DOC (± EBRT), and 36% supportingtreatment with Ra-223 (± EBRT) (Fig. 2). Thereis as yet no clear evidence showing which CRPCpatients, with bone metastases only, should betreated with the new AR-targeted agents DOC orRa-223. Some panelists recommended thatpatients with aggressive bone disease should betreated with DOC, while other panelists
commented that only a few patients will haveaggressive disease. Some panelists suggestedthat Ra-223 is more likely to be used for symp-tomatic patients in the near future.
Treatment Strategy After Failure of ABI orENZ, No Prior DOC, and with Good PS Re-garding treatment strategy after the failure oftreatment with ABI or ENZ or in case of primaryresistance to ABI or ENZ, 60% of the panelmembers recommended DOC for patients withrising PSA. The opinions of the panel were moredivided for cases of acquired resistance, with38% supporting treatment with DOC, 29%supporting treatment with Ra-223, and 19%supporting treatment with another new AR-targeted agent. The panel was also split regard-ing the treatment of patients with radiographicprogression, with 41% recommending DOC and45% recommending Ra-223. For patients withsymptomatic progression, 59% recommendedRa-223 (Fig. 3).
The voting results suggest that a majority ofthe panel members believe that Ra-223 is anappropriate option for patients with symp-tomatic progression, although 60% of them atthe time of the panel meeting did not have real-
Fig. 2 Next preferred treatment in CRPC patients with multiple bone metastases (no visceral metastases) during PADT(with good PS). PSA Prostate-specific antigen
Oncol Ther (2018) 6:157–171 163

world experience with the agent. When thepanel members were asked whether they wouldwant to prescribe Ra-223, in addition to newAR-targeted agents, if it were reimbursable, 67%voted ‘Yes, in the majority of patients’ and 14%voted ‘Yes, in a minority of selected patients.’Further studies are necessary to develop evi-dence for reimbursement decisions.
Treatment Strategy After DOCRegarding the next treatment option forpatients who have received DOC for 10 cyclesand whose PSA is stable and bone metastases onimaging indicate stable disease, 33% of thepanel recommended discontinuation of DOC,while 22% recommended continuation of DOCand 22% recommended switching to Ra-223(Fig. 4).
The panel members discussed whether theuse of Ra-223 in this setting should be recom-mended or not. The voting results varied
depending on the patient’s status, with 50, 76,and 81% of the panel members recommendingthe use of Ra-223 in patients with a rising PSAonly, with radiographic progression, and withsymptomatic progression, respectively (Fig. 5).
Treatment Strategy with Ra-223The panel members discussed the optimal tim-ing of Ra-223 treatment. There was consensusthat its use before chemotherapy was the morereasonable option rather than treatment afterchemotherapy. The rationale for this recom-mendation is that a course of Ra-223 therapyrequires a 6-month interval, and the time atwhich subsequent chemotherapy can be initi-ated requires careful evaluation.
Ra-223 is associated with hematologicaladverse events. As a result, the panel recom-mended performing regular blood tests at leastevery 2–4 weeks.
Fig. 3 Preferred next treatment in CRPC patients with multiple bone metastases (no visceral metastases) during treatmentwith new AR-targeted agent (ENZ/ABI), with no prior exposure to DOC and with good PS
164 Oncol Ther (2018) 6:157–171

Fig. 5 The use of Ra-223 in CRPC patients with multiple bone metastases (no visceral metastases) during DOC (withgood PS)
Fig. 4 What is the next treatment option for CRPC patients with multiple bone metastases (no visceral metastasis) whohave received DOC for 10 cycles and whose PSA is stable and bone metastases on imaging indicate stable disease? [CQ35]
Oncol Ther (2018) 6:157–171 165

Managing Bone Metastases in Patientswith CRPC
The panel members addressed many questionson their experiences and preferences formanaging and treating bone metastases inpatients with CRPC.
Monitoring Bone MetastasesRegarding treatment monitoring of patientswith CRPC with bone metastases, 52% of thepanel members recommended bone scintigra-phy on a regular basis. The Prostate CancerWorking Group 3 (PCWG3) recommended amonitoring frequency of 8–9 weeks for the first24 weeks, then every 12 weeks for bone scans aswell as CT/MRI [14].
As to monitoring during treatment with Ra-223, the panel strongly (91%) recommendedmonitoring with CT scans to detect lymph nodeand/or visceral metastases. Altogether, 83% ofthe panel members also recommended regularmonitoring of alkaline phosphatase (ALP) dur-ing treatment of CRPC with bone metastases.
Definition of Progression of Bone MetastasesTo evaluate metastatic bone progression, thePCWG2 outlined the 2 ? 2 rule that recom-mends using two additional scans to confirmthe appearance of at least two new lesionscompared to an initial post-treatment scan. Thismethod was maintained in PCWG3 and furtherextended to define the progression from non-metastatic to metastatic CRPC [15]. The rule isintended to distinguish bone scan ‘flare’ fromactual disease progression. However, imple-mentation of this rule in real-world practicedoes appear to be haphazard, with fewer thanhalf of panelists adopting this recommendationfor assessing progression of bone metastases byimaging. Discussion showed that the PCWG3recommendation was generally consideredapplicable for the clinical trial setting.
The panel reached a consensus (77%) that atleast two of three criteria (PSA progression,radiographic progression, and symptomaticprogression) should be used as the definition ofprogression.
Quantification of Bone MetastasesThe bone scan index (BSI), which is obtainedusing a computer-aided bone scan evaluationsystem, is anticipated to become an objectiveand quantitative clinical tool for evaluatingbone metastases in prostate cancer [16]. Mostpanelists did not use BSI in clinical practice, andBSI was thought by some panelists to be pre-mature for use in practice.
Re-Biopsy/Biopsy in CRPCIn 2014, a European Expert Consensus Panelemphasized the importance of biopsy to furtherunderstand the heterogeneity of prostate cancerand to move treatment planning toward adecision-making that was more individualizedto the needs of the patient [17].
Conversely, in this forum, when asked if a re-biopsy of the primary tumor for patients whoare diagnosed as CRPC is necessary, 77% of thepanel voted ‘No.’ As to biopsy of the metastaticsite, 64% voted ‘No.’ Most panelists consideredre-biopsy of CRPC to have little significance fortherapeutic decision-making and more signifi-cance for research.
Response to Bone PainThe panel discussed the best treatment optionfor bone pain and recommended EBRT forpatients who develop isolated pelvic bone painand Ra-223 for patients who develop multipleor diffused bone pain at the pelvis and spine.Ra-223 following EBRT would be an appropriateoption as well.
DISCUSSION
The main objective of this meeting was to shareopinions among experts and to provide guide-lines that would facilitate clinicians to success-fully incorporate Ra-223 into CRPC treatment.At the time of the meeting, 60% of the panelmembers had no experience with Ra-223 treat-ment in actual practice and the optimal treat-ment strategy with Ra-223 had not yet beenestablished. However, there was consensus for anumber of key areas, including appropriatepatient selection and optimal timing of treat-ment with Ra-233, for which the consensus was
166 Oncol Ther (2018) 6:157–171

that patients with symptomatic metastaticCRPC and Ra-223 before chemotherapy,respectively, would benefit the most patients.
For patients with CSPC, CAB therapy wasrecommended by most panelists, although bycontrast half of the panelists in the APCCC 2015were opposed to CAB. CAB has more efficacythan luteinizing hormone-releasing hormone(LHRH) agonists alone and can prevent flarephenomenon, but following the introduction ofLHRH antagonists and new AR-targeted drugs inclinical practice, the significance of CAB as atreatment option is being re-considered.
New findings have been reported since themeeting and these should be taken into accountwhen a treatment for metastatic CSPC is beingconsidered. According to a systematic reviewand meta-analysis, DOC at the beginning ofADT therapy for metastatic CSPC resulted insignificantly longer OS and PFS than that seenwith ADT therapy alone [11]. At the time of themeeting in September 2016, this benefit had notbeen confirmed; 62% of the panel wanted to useDOC with ADT in patients with CSPC with bonemetastases, and 23% used this regimen in theirpractice. The panel stressed that DOC with ADTshould be used only in appropriate patients andthat careful patient selection is crucial. Accord-ing to the randomized CHAARTED trial [18], theregimen was most effective in patients withhigher volume disease; however, those patientswith high-volume disease may have a higher riskof chemotherapy intolerance, and the definitionof ‘high tumor volume’ has not been estab-lished. Therefore, it was also stressed by thepanelists that other factors, including Gleasonscore, response to ADT, and patient character-istics, should be taken into consideration, andthat new biomarkers must be explored.
The publication of the results of two impor-tant studies have resulted in changes in thetreatment recommendations for metastaticCSPC since this consensus forum was held. TheLATITUDE study showed that the addition ofABI and prednisone to ADT therapy to treatnewly diagnosed, high-risk metastatic CSPCimproved OS when compared to ADT therapyalone [19]. The STAMPEDE trial showed similarresults, with improved OS and higher rates offailure free survival seen with the addition of
ABI and prednisone to ADT therapeutic regimenin a more heterogeneous patient populationthat included those with locally advanced ormetastatic CSPC [20]. As a result of these stud-ies, the addition of ABI and prednisone to ADTeither before or after chemotherapy has beenapproved in Japan, as well as the USA and othercountries, for high-risk CSPC [21].
Most panelists recommended that patientsbe monitored for osteoporosis and that treat-ment be provided if necessary during ADT. Allpanelists recommended using MRI when thereare discrepancies between bone scintigram andCT findings. Almost all panelists recommendedmonitoring ALP during CRPC treatment.
Osteoclast-targeting agents were recom-mended for CRPC with bone metastases, andosteoclast-targeted agents can be used in com-bination with Ra-223. Most panelists recom-mended Ra-223 for patients with bonemetastases only and with radiographic orsymptomatic progression.
For other clinical questions, consensusbetween panelists was harder to determine andrequires results from ongoing and future clinicalstudies and progress on regulatory issues. Thepanel was divided on the treatment strategy forpatients with oligometastases, with half recom-mending drug treatment and others recom-mending additional therapies, including radicaltherapy and radiation. The diagnosis ofoligometastases is important, and the signifi-cance of MRI or PET must be considered. Therewere different opinions on the definition of‘castration,’ with regards to the thresholdtestosterone levels of\ 50 ng/dL (conventional)or\20 ng/dL. In the COU-AA-02 study of ABIacetate, prognosis was different between thresh-old testosterone levels of[20 and B 20 ng/dL,but in practice almost all patients have\20 ng/dL testosterone with an LHRH agonist.
Regarding the evaluation of progression,fewer than half of the panelists recommendedthe use of PCWG3 or BSI criteria for monitoring.Many panelists thought that the PCWG3 crite-ria seem difficult and that the BSI criteria are toopreliminary for use in clinical practice. Thetiming for changing treatment by scintigramextension of disease (EOD) grading was dividedbetween EOD 1–2, 2–3, and 3–4 and is probably
Oncol Ther (2018) 6:157–171 167

dependent on which treatment is considered:Ra-223, DOC, or a new AR-targeting treatment.
The treatment choice by panelists forpatients with CRPC with bone metastases varieddepending on whether the disease status wasPSA-only, radiographic progression, or symp-tomatic progression. It was recommended thatbone metastases with PSA-only progression betreated with a new AR-targeted agent and thatsymptomatic bone metastases be treated withRa-223. The combination therapy of ABI and Ra-223 was studied in a phase 3 randomized dou-ble-blind setting (ERA 223; NCT02043678) forCRPC patients with bone metastases, but due tothe observation of an increased risk of fracturesand death in the combination arm, the trial wasunblinded in December 2017 before the sched-uled end of the study. Analysis of these studydata is currently being performed [22, 23].
The discussions and opinions of 27 Japaneseexperts on the treatment of prostate cancer arereported here. However, there are limitations tothese data. First, these data represent the votingresults of the meeting, and the treatmentselections were not determined from the actualprescribing records. Due the progress of thistherapeutic area, the participants may currentlyhave different opinions.
This report is based on a consensus meetingheld in 2016, and subsequent trial results andevidence influencing current therapeutic stan-dards are not reflected in all of the votingresults. However, it is important for physiciansto know how our understanding of the optimaluse of therapy has evolved to what is seen todayby knowing the consensus formed at eachmilestone of development. Being familiar withthese developmental steps is useful to improv-ing our understanding of the rationale behindstandard therapies and reinforces the educationneeded by physicians who must provide opti-mal treatments in this therapeutic area that hasan increasing complexity of choices.
CONCLUSIONS
The panel was in consensus that the optimaltiming of Ra-223 treatment is before chemother-apy rather after chemotherapy because a course of
Ra-223 therapy requires a 6-month interval, andthe time to which subsequent chemotherapyadministration can be initiated requires carefulevaluation. Data from this meeting inform thedevelopment of future discussions or contribu-tions to the development of new guidelines.
ACKNOWLEDGEMENTS
Funding. This study and the article process-ing charges were funded by Bayer Yakuhin Ltd.,Tokyo, Japan.
Medical Writing and Other Editorial Assis-tance. The authors acknowledge medical writ-ing support by Masami Kajiura and Aya Tokaji,MDS-CMG Inc., Tokyo, Japan, with fundingfrom Bayer Yakuhin Ltd., Tokyo, Japan. Theirservices encompassed preparation of the firstdraft, preparing tables and figures, and incor-porating authors’ revisions, all under the direc-tion of the authors. Bayer Yakuhin had theopportunity to review the manuscript as afunding sponsor, but did not have the authorityto influence the content.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole and have given theirapproval for this version to be published.
Author Contributions. ST: conceptualiza-tion; methodology; steering committee mem-ber; drafting of clinical questions; original draftpreparation. SK, NN, NS, KS, and HS: conceptu-alization; methodology; steering committeemember; drafting of clinical questions. YK:supervision of the project; conceptualization;methodology; chairperson of the steering com-mittee; drafting of clinical questions. All authorswere present at the consensus meeting and votedon the clinical questions; they were all involvedin the development and approved the finalmanuscript. The authors of this manuscript didnot receive any honorarium for their writing andinvolvement in the developing of this
168 Oncol Ther (2018) 6:157–171

manuscript. Funding for the expert panel meet-ing was provided by Bayer Yakuhin, at which thespeakers for the meeting received a speakers’ fee.
Disclosures. Shunji Takahashi reportedreceiving lecture fees from Eisai and Daiichi-Sankyo and research grants from AstraZeneca,Daiichi-Sankyo, Chugai Pharmaceutical, Novar-tis Pharma, Bayer, and Parexel International, andreceiving meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Norio Nonomura receivedconsulting and meeting fees from Bayer. NobuoShinohara received research grants from Astellasand Ono Yakuhin and honoraria from GSK,Novartis, Pfizer, and Bayer, and also reportsreceiving meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Kazuhiro Suzuki reportedconsulting and meeting expenses from Bayer,research grants from Astellas, Takeda, and Dai-ichi-Sankyo, and honoraria for speaking andeducational writing from Astellas, Takeda, Dai-ichi-Sankyo, AstraZeneca, Janssen, Nihon-kayaku, Bayer, and Fuji Film; he also reportedreceiving meeting and medical writing fincancialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Hiroyoshi Suzuki reportedreceiving honoraria and/or research grants fromAstellas, Takeda, AstraZeneca, Bayer, Chugai,Novartis Pharma, Janssen Pharma, NihonKayaku, and Daiichi-Sankyo, and received anhonorarium from Nihon Medi-Physics for serv-ing as a medical specialist; he also reportsreceiving meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Takefumi Satoh currently hasanother position in Sato Takefumi ZenritsusenClinic, and reported receiving meeting andmedical writing financial support for thismanuscript from Bayer Yakuhin Ltd., Tokyo,Japan. Toshiyuki Yoneda reported receiving aconsultant fee from Daiichi-Sankyo and receiv-ing meeting and medical writing financial sup-port for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Takao Kamai reportedreceiving honoraria from Astellas and Sanofi, andreceiving meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Takashi Mizowaki reported
receiving a grant from Eisai, speaker fees fromAstellas, Philips Electronics Japan, Takeda, Hita-chi, Valiant Medical Systems, Brain Labo, Medi-con, Electa, Asuka Pharma, Daiichi-Sankyo, andBayer, and to receiving meeting expenses fromMDS; he also reported receiving meeting andmedical writing financial support for thismanuscript from Bayer Yakuhin Ltd., Tokyo,Japan. Nobuaki Matsubara reported receivingspeaking honoraria from Astellas, Astra Zeneca,Bayer, Eisai, Janssen, MSD, Novartis, Ono, Phizer,and Sanofi and to have received research fundingfrom Novartis, Ono, and Sanofi; he has alsoreceived meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Hiroji Uemura reportedreceiving consultation fees from Bayer and toreceiving meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan. Akira Yokomizo reportedreceiving speaking honoraria from Astellas,Takeda, Daiichi-Sankyo, Novartis Pharma,AstraZeneca, and Janssen and also to receivingmeeting and medical writing financial supportfor this manuscript from Bayer Yakuhin Ltd.,Tokyo, Japan. Mana Yoshimura reproted receiv-ing research funding from Nihon Medi-Physicsand also to have received meeting and medicalwriting financial support for this manuscriptfrom Bayer Yakuhin Ltd., Tokyo, Japan. SeigoKinuya, Nobuo Shinohara, Katsumasa Naka-mura, Ukihide Tateishi, Hiroyuki Horikoshi,Tsukasa Igawa, Mitsuru Koizumi, Takeo Kosaka,Hideaki Miyake, Atsushi Mizokami, TakashiMizowaki, Naoki Nakamura, Masahiro Nozawa,Takeo Takahashi, Motohide Uemura, and Yosh-iyuki Kakehi have each reported that they havereceived meeting and medical writing financialsupport for this manuscript from Bayer YakuhinLtd., Tokyo, Japan.
Compliance with Ethics Guidelines. Thisarticle does not contain any studies withhuman participants or animals performed byany of the authors.
Data Availability. All data generated oranalyzed during this study are included in thispublished article as supplementary informationfiles.
Oncol Ther (2018) 6:157–171 169

Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any non-commercial use, distribution, and reproductionin any medium, provided you give appropriatecredit to the original author(s) and the source,provide a link to the Creative Commons license,and indicate if changes were made.
REFERENCES
1. National Cancer Center (Japan), Cancer Registra-tion and Statistics 2017. http://ganjoho.jp/reg_stat/statistics/stat/short_pred.html. Accessed 26 Mar2017.
2. Parker C, Nilsson S, Heinrich D, et al. Alpha emitterradium-223 and survival in metastatic prostatecancer. N Engl J Med. 2013;369(3):213–23. https://doi.org/10.1056/NEJMoa1213755.
3. Sartor O, Coleman R, Nilsson S, et al. Effect ofradium-223 dichloride on symptomatic skeletalevents in patients with castration-resistant prostatecancer and bone metastases: results from a phase 3,double-blind, randomised trial. Lancet Oncol.2014;15(7):738–46. https://doi.org/10.1016/S1470-2045(14)70183-4.
4. Gillessen S, Omlin A, Attard G, et al. Managementof patients with advanced prostate cancer: recom-mendations of the St Gallen Advanced ProstateCancer Consensus Conference (APCCC) 2015. AnnOncol. 2015;26(8):1589–604. https://doi.org/10.1093/annonc/mdv257.
5. Hsu C-C, Sandford BA. The Delphi technique:making sense of consensus. Pract Assess Res Eval.2007;12(10):1–8.
6. Japanese Urological Association. Clinical guidelinefor prostate cancer 2012. Bunkyo-ku, Tokyo: Kane-hara-Shuppan; 2012. (in Japanese).
7. Thomas C, Bogemann M, Konig F, et al. AdvancedProstate Cancer Consensus Conference (APCCC)2015 in St. Gallen: Critical review of the recom-mendations on diagnosis and therapy of metastaticprostate cancer by a German expert panel. UrologeA. 2016;55(6):772–82. https://doi.org/10.1007/s00120-016-0030-8 (in German).
8. Ost P, Jereczek-Fossa BA, As NV, et al. Progression-free survival following stereotactic body
radiotherapy for oligometastatic prostate cancertreatment-naive recurrence: a multi-institutionalanalysis. Eur Urol. 2016;69(1):9–12. https://doi.org/10.1016/j.eururo.2015.07.004.
9. Azzam G, Lanciano R, Arrigo S, et al. SBRT: anopportunity to improve quality of life for oligome-tastatic prostate cancer. Front Oncol. 2015;5:101.https://doi.org/10.3389/fonc.2015.00101.
10. James ND, Sydes MR, Clarke NW, et al. Addition ofdocetaxel, zoledronic acid, or both to first-linelong-term hormone therapy in prostate cancer(STAMPEDE): survival results from an adaptive,multiarm, multistage, platform randomised con-trolled trial. Lancet. 2016;387(10024):1163–77.https://doi.org/10.1016/S0140-6736(15)01037-5.
11. Vale CL, Burdett S, Rydzewska LH, et al. Addition ofdocetaxel or bisphosphonates to standard of care inmen with localised or metastatic, hormone-sensi-tive prostate cancer: a systematic review and meta-analyses of aggregate data. Lancet Oncol.2016;17(2):243–56. https://doi.org/10.1016/S1470-2045(15)00489-1.
12. Yang HL, Liu T, Wang XM, Xu Y, Deng SM. Diag-nosis of bone metastases: a meta-analysis compar-ing 18FDG PET, CT, MRI and bone scintigraphy. EurRadiol. 2011;21(12):2604–17. https://doi.org/10.1007/s00330-011-2221-4.
13. Scher HI, Morris MJ, Stadler WM, et al. Trial designand objectives for castration-resistant prostate can-cer: updated recommendations from the ProstateCancer Clinical Trials Working Group 3. J ClinOncol. 2016;34(12):1402–18. https://doi.org/10.1200/JCO.2015.64.2702.
14. ASCO Annual Meeting, The Prostate Cancer Work-ing Group 3 (PCWG3) consensus for trials in castra-tion-resistant prostate cancer (CRPC). http://meetinglibrary.asco.org/content/149791-156. Accessed30 Mar 2017.
15. Uemura K, Miyoshi Y, Kawahara T, et al. Prognosticvalue of a computer-aided diagnosis systeminvolving bone scans among men treated withdocetaxel for metastatic castration-resistant pros-tate cancer. BMC Cancer. 2016;16:109. https://doi.org/10.1186/s12885-016-2160-1.
16. Fitzpatrick JM, Bellmunt J, Fizazi K, et al. Optimalmanagement of metastatic castration-resistantprostate cancer: highlights from a European ExpertConsensus Panel. Eur J Cancer.2014;50(9):1617–27. https://doi.org/10.1016/j.ejca.2014.03.010.
17. Saad F, Shore N, Van Poppel H, et al. Impact ofbone-targeted therapies in chemotherapy-naıvemetastatic castration-resistant prostate cancer
170 Oncol Ther (2018) 6:157–171

patients treated with abiraterone acetate: post hocanalysis of study COU-AA-302. Eur Urol.2015;68(4):570–7. https://doi.org/10.1016/j.eururo.2015.04.032.
18. Sweeney CJ, Chen YH, Carducci M, et al. Chemo-hormonal therapy in metastatic hormone-sensitiveprostate cancer. N Engl J Med. 2015;373(8):737–46.https://doi.org/10.1056/NEJMoa1503747.
19. Fizazi K, Tran N, Fein L, LATITUDE Investigators,et al. Abiraterone plus prednisone in metastatic,castration-sensitive prostate cancer. N Engl J Med.2017;377(4):352–60. https://doi.org/10.1056/NEJMoa1704174.
20. James ND, de Bono JS, Spears MR, STAMPEDEInvestigators, et al. Abiraterone for prostate cancernot previously treated with hormone therapy.
N Engl J Med. 2017;377(4):338–51. https://doi.org/10.1056/NEJMoa1702900.
21. Janssen Biotech, Inc. Zytiga(r) (Abiraterone acetate).Janssen Biotech, Inc. Horsham, PA. 2018. http://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/ZYTIGA-pi.pdf. Accessed 21 Nov 2018.
22. Parker C, Heidenreich A, Nilsson S, Shore N. Cur-rent approaches to incorporation of radium-223 inclinical practice. Prostate Cancer Prostatic Dis.2018;21(1):37–47. https://doi.org/10.1038/s41391-017-0020-y.
23. Sartor O, de Bono JS. Metastatic prostate cancer.N Engl J Med. 2018;378(7):645–57. https://doi.org/10.1056/nejmra1701695.
Oncol Ther (2018) 6:157–171 171

![Research Paper Nuclear receptor ERRα contributes to ... · the management of CRPC . In fact, xenograft [5, 6] models of CRPC and CRPC tissues show increased expressions of multiple](https://img.pdfslide.net/doc/110x75/5ed997291b54311e7967d8e3/research-paper-nuclear-receptor-err-contributes-to-the-management-of-crpc.jpg)