Embed Size (px)
Citation preview

Jaundice

Aims and DemandsAims and Demands 1. Grasp the concept of jaundice, clinical manifestation 1. Grasp the concept of jaundice, clinical manifestation
and points of inquisitionand points of inquisition 2. Familiar the etiology and mechanism of jaundice2. Familiar the etiology and mechanism of jaundice 3. Realize normal bilirubin metabolism3. Realize normal bilirubin metabolism

DefinitionDefinition:: jaundice,or icterus refers to the yellow appeajaundice,or icterus refers to the yellow appea
rance of the skin,scleral and mucous membranes resulting rance of the skin,scleral and mucous membranes resulting
from an increased bilirubin concentration in the body fluidfrom an increased bilirubin concentration in the body fluid
s. s. Total bilirubin: 1.7-17.1μmol/LTotal bilirubin: 1.7-17.1μmol/L Conjugated bilirubin:0-3.42μmol/lConjugated bilirubin:0-3.42μmol/l ,, Unconjugated bilirubin:1.7-13.68μmol/l.Unconjugated bilirubin:1.7-13.68μmol/l.

Liver
AlbuninHeme
Ferroheme
transferase
Bilirubin
Conjugated bilirubinKidney
Urobilin
Stercobilinogen
Urobilinogen
Intestines
Albumin
Bilirubin
reductase Heme
Globin
Hemoglobin
oxidase
Biliverdin
Marrow
Infantility ErythrocyteFerroheme Enzyme
15%~20%
Bilirubin |Albumin
Erythrocyte80%~85%
UDP UDPGA
Bilirubin glucuronolactone
urobilinogen
Enterohepatic circulation
Y/Z protein
cathepsin
Erythrocyte
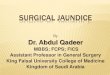
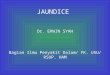
Normal bilirubin
metabolism

Normal bilirubin metabolism

ClassificationClassification
1. Depending on Etiology1. Depending on Etiology Hemolytic JaundiceHemolytic Jaundice Hepatocellular JaundiceHepatocellular Jaundice Cholestatic JaundiceCholestatic Jaundice Congenital jaundiceCongenital jaundice
2. Depending on bilirubin Unconjungated bilirubing
increased jaundice Conjungated bilirubing in
creased jaundice

EtiologyEtiology 1.Congenital hemolytic anemia (1.Congenital hemolytic anemia (thalassemiathalassemia,,hereditary spherocyhereditary spherocy
tosis).tosis). 2.P2.Posteriority acquired hemolytic anemia (autoimmunity hemolyosteriority acquired hemolytic anemia (autoimmunity hemoly
tic anemia, hemolytic disease of newborn,tic anemia, hemolytic disease of newborn, posttransfusion hemolposttransfusion hemol
ytic, Favism)ytic, Favism).. MechanismMechanism A large number of erythrocyte destroyed rapidlyA large number of erythrocyte destroyed rapidly Anemia,hypoxia and toxity of erythocyte metabolism productsAnemia,hypoxia and toxity of erythocyte metabolism products
1.Hemolytic Jaundice

Haemolytic Jaundice mechanis
m

Clinical ManifestationClinical Manifestation Mild jaundice,light lemon,no skin itch.Mild jaundice,light lemon,no skin itch. Acute hemolytis: fever,chill,headache,vomit,backache,anemia, Acute hemolytis: fever,chill,headache,vomit,backache,anemia,
hemoglobinuria( dark sauce or tea), acute renal failure.hemoglobinuria( dark sauce or tea), acute renal failure. Chronic hemolysis:anemia and splenomegaly.Chronic hemolysis:anemia and splenomegaly.

Laboratory ExaminationLaboratory Examination 1.Serum TB↑,UCB↑,CB normal.1.Serum TB↑,UCB↑,CB normal. 2.UCB↑→intestinal CB↑→faecal color deepen.2.UCB↑→intestinal CB↑→faecal color deepen. 3.Intestinal Urobilinogen↑→urinary Urobilinogen↑.3.Intestinal Urobilinogen↑→urinary Urobilinogen↑. 4.Acute hemolytis, occult blood test (+).4.Acute hemolytis, occult blood test (+). 5.Blood test:anemia, reticulocyte↑,erythacyte proliferation↑. 5.Blood test:anemia, reticulocyte↑,erythacyte proliferation↑.

2.Hepatocellular Jaundice2.Hepatocellular Jaundice
EtiologyEtiology Hepatocyte damage.Hepatocyte damage. MechanismMechanism Impair hepatocyte uptakeing,conjugating and excreting biImpair hepatocyte uptakeing,conjugating and excreting bi
lirubin, UCB↑lirubin, UCB↑ CB reflux into blood, serum CB↑→jaundice.CB reflux into blood, serum CB↑→jaundice.

Hepatocellular Jaundice mechani
sm

Clinical ManifestationClinical Manifestation Skin and mucosa:light to deep yellow, mild skin itchSkin and mucosa:light to deep yellow, mild skin itch Tired,loss of appetiteTired,loss of appetite hemorrhagic tendency,ascites,coma.hemorrhagic tendency,ascites,coma. Primary disease manifestationPrimary disease manifestation

Laboratory ExaminationLaboratory Examination
1.1. CB↑, UCB↑CB↑, UCB↑
2.2. Icteric hepatitis:CB↑ ↑ UCB ↑Icteric hepatitis:CB↑ ↑ UCB ↑
3.3. Urine:CB(+),urobilinogen ↑Urine:CB(+),urobilinogen ↑
4.4. Blood test:liver demaged Blood test:liver demaged

3.Cholestatic Jaundice3.Cholestatic Jaundice EtiologyEtiology Obstruction in liver:virus hepatitis,drug caused,drug hepatitis, primary biliary cirrhosiObstruction in liver:virus hepatitis,drug caused,drug hepatitis, primary biliary cirrhosi
s.s. Obstruction of Extrahepatic bile duct:narrow, obstruction,stone, inflammtory,tumor.Obstruction of Extrahepatic bile duct:narrow, obstruction,stone, inflammtory,tumor. MechanismMechanism Obstruction causes small bile duct and bile capillary broken, conjugated bilirubin refluObstruction causes small bile duct and bile capillary broken, conjugated bilirubin reflu
x to blood.x to blood. Failure of hepatocyte excreting CB,bilirubin deposit and bile thrombus formation.Failure of hepatocyte excreting CB,bilirubin deposit and bile thrombus formation.

Cholestatic Jaundice mechanism

Clinical featuresClinical features Skin dark yellow,yellow green.Skin dark yellow,yellow green. Skin itch, bradycardia,dark yellow of urine,facaSkin itch, bradycardia,dark yellow of urine,faca
l light yellow or clay color. l light yellow or clay color. Courvoisier’s sign.Courvoisier’s sign.

Laboratory ExaminationLaboratory Examination Serum CB↑Serum CB↑ Urine bilirubin (+)Urine bilirubin (+) Urobilinogen , stercobilin ↓or absenceUrobilinogen , stercobilin ↓or absence Serum alkaline phosphatase and CholesteSerum alkaline phosphatase and Choleste
rol↑rol↑

Three kinds of jaundice laborotory examination indentifiThree kinds of jaundice laborotory examination indentificationcation
Class Haemolytic Hepatocellular CholestaticClass Haemolytic Hepatocellular Cholestatic
TB increasedTB increased(UCB(UCB) increased increased) increased increased
CB normal increased markedly increased CB normal increased markedly increased
CB/TB CB/TB << 1515 %一%一 2020 % >% > 3030 %一%一 4040 % >% > 5050 %一%一 6060 %% urine bilirubin — urine bilirubin — 十 十十十 十十 urobilinogen increased slight increased decreased or absenceurobilinogen increased slight increased decreased or absence
ALTALT 、、 AST normal markedly increased may increasedAST normal markedly increased may increased
ALP normal increased markedly increased ALP normal increased markedly increased
r-GT normal increased markedly increasedr-GT normal increased markedly increased
PT normal delayed delayedPT normal delayed delayed
Vit K respond no poor goodVit K respond no poor good
Cholesterol normal slight increased or decreased markedly increasedCholesterol normal slight increased or decreased markedly increased
Serum protein normal Alb decreased,Glob increased normalSerum protein normal Alb decreased,Glob increased normal

4.Congenital Nonhemolytic Jaundice 4.Congenital Nonhemolytic Jaundice
Due to the deficiency of the hepatocyte in uptakeiDue to the deficiency of the hepatocyte in uptakei
ng,conjugating and excreting bilirubinng,conjugating and excreting bilirubin UncommonUncommon

1.Gilber syndrome:hepatocyte uptaking UCB abnormal, def1.Gilber syndrome:hepatocyte uptaking UCB abnormal, def
iciency of glucuronyl transferase, →UCB↑ →jaundice (no iciency of glucuronyl transferase, →UCB↑ →jaundice (no
symptom,liver function normal).symptom,liver function normal). 2.Dubin-Johnson’s syndrome:abnormal of Hepatocyte excr2.Dubin-Johnson’s syndrome:abnormal of Hepatocyte excr
eting CB and some anion to bile capillary →CB↑ →jaundiceting CB and some anion to bile capillary →CB↑ →jaundic
e.e. 3.Crigler-Najjar’s syndrome:absence of glucuronyl transfer3.Crigler-Najjar’s syndrome:absence of glucuronyl transfer
ase in hepatocyte, UCB can’t be transfered to CBase in hepatocyte, UCB can’t be transfered to CB ,, serum serum
UCB↑→jaundice,UCB↑↑↑→nuclear jaundic, newborn,poor UCB↑→jaundice,UCB↑↑↑→nuclear jaundic, newborn,poor
prediction.prediction. 4.Rotor’s syndrome:deficiency of Hepatocyte uptaking UC4.Rotor’s syndrome:deficiency of Hepatocyte uptaking UC
B and excreting CB,→bilirubin↑→jaundice.B and excreting CB,→bilirubin↑→jaundice.

Accessory Examination Accessory Examination
1.Ultrosound1.Ultrosound 2.X ray2.X ray 3.ERCP3.ERCP(Endoscopic retrograde cholangiopancreatography) 4.PTC4.PTC(Percutaneous transheptic cholangiography) 5.CT5.CT(Computed tomography)) 6.MRI6.MRI(Magnetic resonance cholangiopancreatography) 7.Radio Nuclide Examination7.Radio Nuclide Examination 8.Liver Biopsy and LC8.Liver Biopsy and LC(Laparoscopy)

Accompanying Symptoms Accompanying Symptoms
1.1. Fever:acute cholangitis,liver abscess, leptospirosis, septicFever:acute cholangitis,liver abscess, leptospirosis, septic
emia, lobar pneumonia.Fever then jaundice:virus hepatitemia, lobar pneumonia.Fever then jaundice:virus hepatit
is,acute hemolysis.is,acute hemolysis.
2.2. Upper abdominal sharp pain:biliary calculi,liver abscess, Upper abdominal sharp pain:biliary calculi,liver abscess,
biliary ascariasis,biliary ascariasis,
Right upper abdom sharp pain,chill, high fever,jaundice, Right upper abdom sharp pain,chill, high fever,jaundice,
Charcot triad sign:acute pyogenic cholangitis,Charcot triad sign:acute pyogenic cholangitis,
Sustained right upper abdominal blur or swell pain:virus Sustained right upper abdominal blur or swell pain:virus
hepatitis,liver abscess,primary carcinoma of liverhepatitis,liver abscess,primary carcinoma of liver

3.3. HepatomegalyHepatomegaly
① ①Mild or moderate,soft or moderate hard,smooth surfMild or moderate,soft or moderate hard,smooth surf
ace:Virus hepatitis,acute infection of biliary tract.obstrace:Virus hepatitis,acute infection of biliary tract.obstr
uction of biliary tractuction of biliary tract
② ②Obvious enlargement, hard, ragged surface:primary Obvious enlargement, hard, ragged surface:primary
or secondary carcinoma of liver.or secondary carcinoma of liver.
③ ③Not obvious enlargement,hard,edge not tidy,nodule Not obvious enlargement,hard,edge not tidy,nodule
on the surface:cirrosis.on the surface:cirrosis.

4.4. Gallbladder enlargement:common bile duct obstructioGallbladder enlargement:common bile duct obstructio
n, n,
pancrease head carcinoma,common bile duct carcinoma,pancrease head carcinoma,common bile duct carcinoma,
carcinoma of ampulla.carcinoma of ampulla.
5.5. Splenomegaly:virus hepatitis,leptospirosis, septicemia, Splenomegaly:virus hepatitis,leptospirosis, septicemia,
Malaria,biliary cirrhosis,hemolytic anemia,lymphoma.Malaria,biliary cirrhosis,hemolytic anemia,lymphoma.
6.6. Acite:serious hepatitis,decompensation of cirrosis, Acite:serious hepatitis,decompensation of cirrosis,
carcinoma of liver.carcinoma of liver.

Interrogatoire Interrogatoire Points Points
1.Assure jaundice1.Assure jaundice 2.Etiology and onset 2.Etiology and onset 3.Accompany syndrome3.Accompany syndrome 4.Time and fluctuation of jaundice4.Time and fluctuation of jaundice 5.Influnce to the overall health5.Influnce to the overall health In one word: make sure the type of jaundice then fiIn one word: make sure the type of jaundice then fi
nd the pathogenynd the pathogeny

Recognise jaundiceRecognise jaundice
PositionPosition:: sclera,skin and sclera,skin and tongue sleevestongue sleeves
Pseudojaundice:Pseudojaundice:eat eat Carotene food(Carotene,pumpkinCarotene food(Carotene,pumpkin, tomat, tomat
o,orange)also can cause skin stained yellow,but bilirubin is o,orange)also can cause skin stained yellow,but bilirubin is
not increased. not increased.
Old people fat Old people fat accumulation at bulbar conjunctivaaccumulation at bulbar conjunctiva ,, yelloyello
w,w,uneven distributionuneven distribution

Jaundice is a common symptom and sign in clinical work,
get to know the mechanism can help us identify different kin
ds of jaundices. hemolytic jaundice is due to the rapidly destr
oyed erythocyte, so the UCB increased. hepatocellular jaundi
ce refers to uptakeing,conjugating and excreting bilirubin, so
both CB and UCB increased. Cholestatic jaundice due to the
obstruction of bile track, so the CB increased and urine biliru
bin positive.
Summary

1.A 13 years old male, chief complaints “Finding skin and
sclera yellow and feeling right upper abdomen swell pain for
1 week”
What are the possible diagnoses and your suggested
examinations.
Question

Reference booksReference books
Cecil mecidine 23Cecil mecidine 23rdrd edition. edition.
Davidson’ principles and practice of medicine.Davidson’ principles and practice of medicine.
Harrison's principles of internal medicine.16Harrison's principles of internal medicine.16thth edition. edition.



![Visceral manifestation Lecturer: QU Hongyan. [Objects] To master the concept of Zang-fu organs To grasp the physiological features of five Zang organs,](https://img.pdfslide.net/doc/110x75/56649e435503460f94b36d96/visceral-manifestation-lecturer-qu-hongyan-objects-to-master-the-concept.jpg)