Embed Size (px)
Citation preview

Jayashree Ravishankar, MD Jayashree Ravishankar, MD Medical Director, STAR Health Center Medical Director, STAR Health Center
New York/ New Jersey AETC & SUNY Downstate Medical CenterNew York/ New Jersey AETC & SUNY Downstate Medical Center&&
Simona Bratu, MDSimona Bratu, MDSUNY Downstate Medical CenterSUNY Downstate Medical Center
5/12/06 5/12/06
Community Acquired Methicillin Community Acquired Methicillin Resistant Resistant Staphylococcus aureusStaphylococcus aureus
in HIV-Infected Patients: in HIV-Infected Patients: An Emerging PathogenAn Emerging Pathogen

Case: HistoryCase: History
43 yo male w/ no past medical Hx presents 43 yo male w/ no past medical Hx presents with 3 days of scrotal edema, perirectal with 3 days of scrotal edema, perirectal discharge, fever, chillsdischarge, fever, chills
States “one day I had a small pimple on my States “one day I had a small pimple on my penis, the next day the whole area just penis, the next day the whole area just exploded”exploded”
No allergies, no travel HxNo allergies, no travel Hx +Hx unprotected sex w/both men and women+Hx unprotected sex w/both men and women +Hx recent wt loss (about 30 lbs in 4 mo)+Hx recent wt loss (about 30 lbs in 4 mo)

Case: Physical ExaminationCase: Physical Examination On admission febrile to 103°, other vital signs On admission febrile to 103°, other vital signs
normalnormal Gen: thin male, looks younger than stated ageGen: thin male, looks younger than stated age HEENT: PERRLA, oropharynx clearHEENT: PERRLA, oropharynx clear Heart: RRR No M/R/GHeart: RRR No M/R/G Lungs: clear bilaterallyLungs: clear bilaterally Abd: normal sounds, soft, no HSM. Tender R Abd: normal sounds, soft, no HSM. Tender R
inguinal mass, warm, fluctuantinguinal mass, warm, fluctuant GU: extensive scrotal/perirectal abscessGU: extensive scrotal/perirectal abscess

Case: Laboratory Test ResultsCase: Laboratory Test Results
WBC: 28,560, 88% PMNsWBC: 28,560, 88% PMNs Hb/Ht: 12.7/40Hb/Ht: 12.7/40 Platelet: 336Platelet: 336 BUN/Cr: 14/1.0BUN/Cr: 14/1.0


MRSA skin and soft tissue infection, MRSA skin and soft tissue infection, penis and scrotumpenis and scrotum

Case: CulturesCase: Cultures
Perirectal abscess culture x 2: community-Perirectal abscess culture x 2: community-acquired (CA)-MRSAacquired (CA)-MRSA sensitive to clindamycin, gentamicin, rifampin, sensitive to clindamycin, gentamicin, rifampin,
tetracycline, bactrim, vancomycintetracycline, bactrim, vancomycin Scrotal abscess culture: CA-MRSAScrotal abscess culture: CA-MRSA Inguinal aspirate: CA-MRSAInguinal aspirate: CA-MRSA HIV Ab+, CD4=240 cells/mm³HIV Ab+, CD4=240 cells/mm³ All blood cultures negativeAll blood cultures negative

HistoryHistory
Shortly after penicillin was introduced in Shortly after penicillin was introduced in 1940s, PCN-resistant 1940s, PCN-resistant S aureusS aureus emerged emerged
Methicillin was introduced in 1961, Methicillin was introduced in 1961, MRSA was reported 1 yr later MRSA was reported 1 yr later
MRSA now accounts for >50% of MRSA now accounts for >50% of S S aureusaureus isolates from ICUs in the U.S. isolates from ICUs in the U.S.

Emergence of Community- Emergence of Community- Acquired Methicillin Resistant Acquired Methicillin Resistant
Staphylococcus aureusStaphylococcus aureus (CA MRSA) (CA MRSA)
Earliest reports of outbreaks of CA-Earliest reports of outbreaks of CA-MRSA in the aboriginal communities in MRSA in the aboriginal communities in Western Australia.Western Australia.
CA-MRSA reported in 1982 among CA-MRSA reported in 1982 among IVDU in Detroit, Michigan. IVDU in Detroit, Michigan.
MRSA is increasingly acquired in the MRSA is increasingly acquired in the community (rather than in medical community (rather than in medical settings)settings)

What constitutes CA-MRSA?What constitutes CA-MRSA?
1.1. Lack of multidrug resistant phenotypeLack of multidrug resistant phenotype
2.2. Presence of exotoxin virulence factors Presence of exotoxin virulence factors like Panton-Valentine leukocidin like Panton-Valentine leukocidin
3.3. Type IV SCC (staphylococcal Type IV SCC (staphylococcal chromosome cassette) chromosome cassette)
4.4. Molecular distinction from nosocomial Molecular distinction from nosocomial strainsstrains

Phenotype and Molecular Phenotype and Molecular Characteristics of CA-MRSACharacteristics of CA-MRSA
Multiple toxins, including super antigensMultiple toxins, including super antigens Panton-Valentine leukocidin (PVL) is a Panton-Valentine leukocidin (PVL) is a
cytotoxin which causes leukocyte cytotoxin which causes leukocyte destruction destruction
Responsible for necrotic skin lesions and Responsible for necrotic skin lesions and severe necrotizing pneumoniasevere necrotizing pneumonia

Representative Antimicrobial Susceptibilities Representative Antimicrobial Susceptibilities (%) of CA- and Hospital-Acquired (HA)-MRSA(%) of CA- and Hospital-Acquired (HA)-MRSA
ANTIMICROBIAL ANTIMICROBIAL AGENTAGENT
% Susceptible% Susceptible
CACA HAHA
OxacillinOxacillin 00 00
CiproCipro 7979 1616
ClindaClinda 8383 2121
ErythroErythro 4444 99
GentGent 9494 8080
RifampinRifampin 9696 9494
TetracyclineTetracycline 9292 9292
TMP-SMXTMP-SMX 9595 9090
VancomycinVancomycin 100100 100100

Populations at riskPopulations at risk
ChildrenChildren SoldiersSoldiers PrisonersPrisoners Homeless peopleHomeless people IVDUIVDU MSMMSM

Risk Factors for CA-MRSA Risk Factors for CA-MRSA among HIV+ MSMamong HIV+ MSM
Nolan E.Lee :Risk Factors for Community-Associated Methicillin-Resistant Staphylococcus aureus Skin Infections among HIV-Positive Men Who Have Sex with Men. CID 2005;40:1529–34

The Five “C”s of TransmissionThe Five “C”s of Transmission
CrowdingCrowding CleanlinessCleanliness Contaminated surfacesContaminated surfaces ContactContact Compromised skinCompromised skin

Clinical SyndromesClinical Syndromes
Skin and soft tissue infections (SSTI)Skin and soft tissue infections (SSTI) FurunculosisFurunculosis Cutaneous skin abscessesCutaneous skin abscesses Deep seated abscessesDeep seated abscesses
Community acquired pneumoniaCommunity acquired pneumonia BacteremiaBacteremia OsteomyelitisOsteomyelitis

Approach to Suspected Approach to Suspected Staphylococcal InfectionsStaphylococcal Infections
Consider MRSA in suspected Consider MRSA in suspected S.aureusS.aureus infections in the community settinginfections in the community setting
Maintain a low threshold for obtaining Maintain a low threshold for obtaining cultures to document MRSAcultures to document MRSA
Recommend surgical drainage of infections Recommend surgical drainage of infections when feasiblewhen feasible

Adequate drainage of purulent collections Adequate drainage of purulent collections = the cornerstone of therapy= the cornerstone of therapy

Initial Therapeutic DecisionInitial Therapeutic Decision
Assess disease severityAssess disease severity Assess the need for parenteral therapyAssess the need for parenteral therapy Consider local susceptibility patternsConsider local susceptibility patterns

Follow Up on the Results of Follow Up on the Results of Susceptibility Testing!!!Susceptibility Testing!!!
Susceptibility patterns vary from region to Susceptibility patterns vary from region to regionregion

Treatment of Seriously Ill PatientsTreatment of Seriously Ill Patients
with Skin and Soft Tissue Infectionswith Skin and Soft Tissue Infections
Vancomycin is still the preferred antibiotic.Vancomycin is still the preferred antibiotic. In case of intolerance to vancomycin or In case of intolerance to vancomycin or
failure, alternative therapy:failure, alternative therapy: LinezolidLinezolid Quinupristin-dalfopristinQuinupristin-dalfopristin DaptomycinDaptomycin

Treatment of Seriously Ill Treatment of Seriously Ill Patients with PneumoniaPatients with Pneumonia
VancomycinVancomycin Linezolid (alternative therapy if Linezolid (alternative therapy if
intolerance to or failure of vancomycin)intolerance to or failure of vancomycin) Do not use daptomycin for pneumoniaDo not use daptomycin for pneumonia

Treatment of Seriously Ill Treatment of Seriously Ill Patients with BacteremiaPatients with Bacteremia
VancomycinVancomycin Alternative therapy: Alternative therapy:
DaptomycinDaptomycin LinezolidLinezolid Quinupristin-dalfopristinQuinupristin-dalfopristin

Outpatient Therapy for CA-MRSA Skin Outpatient Therapy for CA-MRSA Skin and Soft Tissue Infectionsand Soft Tissue Infections
Limited information on the value of antibiotics in the treatment of SSTIs
Isolates are generally susceptible to the following oral antibiotics: clindamycin, TMP-SMX, tetracyclines, linezolid
The efficacy of adding a second drug such as rifampin is uncertain.
Beware of interaction of rifampin with protease inhibitors

ClindamycinClindamycin
Active against many CA-MRSA strainsActive against many CA-MRSA strains Toxin-inhibiting propertiesToxin-inhibiting properties Concerns: Concerns:
- inducible resistance- inducible resistance
- risk of - risk of Clostridium difficileClostridium difficile colitis colitis

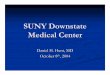
Inducible Clindamycin Resistance Inducible Clindamycin Resistance (MLSBi Phenotype)(MLSBi Phenotype)
MRSA strains that are MRSA strains that are susceptible to clindamycin susceptible to clindamycin but resistant to but resistant to erythromycin erythromycin
Due to the presence of Due to the presence of erythromycin ribosomal erythromycin ribosomal methylase gene (erm)methylase gene (erm)

Positive D-test = MLSBi PhenotypePositive D-test = MLSBi Phenotype
It is called D test as the It is called D test as the shape of the zone of shape of the zone of clearance around clearance around clindamycin is shaped like clindamycin is shaped like a ‘D’ a ‘D’
D-test is recommended on D-test is recommended on all all S.aureusS.aureus isolates isolates reported as resistant to reported as resistant to erythromycin and erythromycin and susceptible to clindamycinsusceptible to clindamycin

Clinical Implications of Inducible Clinical Implications of Inducible Clindamycin ResistanceClindamycin Resistance
MLSBi phenotype precludes the use of MLSBi phenotype precludes the use of clindamycin for severe infectionsclindamycin for severe infections
For uncomplicated infections (cellulitis) For uncomplicated infections (cellulitis) due to MLSBi CA-MRSA the efficacy of due to MLSBi CA-MRSA the efficacy of clindamycin is unclearclindamycin is unclear

Trimethoprim-sulfamethoxazole Trimethoprim-sulfamethoxazole (TMP-SMX, Bactrim, Septra)(TMP-SMX, Bactrim, Septra)
Many CA-MRSA isolates remain Many CA-MRSA isolates remain susceptible to TMP-SMXsusceptible to TMP-SMX
Good oral bioavailabilityGood oral bioavailability Bactericidal against Bactericidal against S aureusS aureus Dose: 10 mg/kg/day (TMP component) Dose: 10 mg/kg/day (TMP component)
in divided doses twice dailyin divided doses twice daily

TMP-SMX LimitationsTMP-SMX Limitations
Side effects: rash and allergic reactions, Side effects: rash and allergic reactions, bone marrow suppression with higher bone marrow suppression with higher doses and prolonged use, electrolyte doses and prolonged use, electrolyte disturbancesdisturbances
Not a good choice for empiric therapy, Not a good choice for empiric therapy, because of frequent resistance in because of frequent resistance in Streptococcus pyogenesStreptococcus pyogenes (group A (group A streptococci)streptococci)

Doxycycline/Minocycline: Caution!!!Doxycycline/Minocycline: Caution!!!
Limited clinical dataLimited clinical data Might be an alternative treatment for Might be an alternative treatment for
patients with SSTIs due to MRSA, in patients with SSTIs due to MRSA, in selected casesselected cases

Preventing Staphylococcal Skin Lesions
Encourage good hygiene; scrupulous hand washing
Discourage sharing of personal items such as towels
Establish appropriate cleaning procedures and schedules for clothes and equipment
Cover wounds Decolonization? Vaccination?

AcknowledgementAcknowledgement
Amy Wecker, MDAmy Wecker, MD Frank Lowy, MDFrank Lowy, MD

The EndThe End