Embed Size (px)
Citation preview

The Essentials of Preventing Falls in the
Older AdultJessica L. Colburn, MD
Johns Hopkins School of MedicineDivision of Geriatric Medicine & Gerontology
April 15, 2015

Discuss prevalence of falls in older adults
Develop an approach for fall risk screening and post-fall assessment in older adults
Discuss interventions that reduce fall risk in older adults
Objectives

Prevalence Outcomes Risk Factors
◦Common Medical Conditions
◦Changes with Aging
Overview
Screening Evaluation Risk Reduction Community Resources
Take Home Points

Prevalence of Falls

Falls Are A Big Problem

One-third of older adults in the community fall each year
Prevalence One-half of older
adults in long term care fall each year

Falls are the leading cause of traumatic injuries in adults over the age of 65
Increased mortality secondary to falls with each decade of life
Estimated direct medical costs for injuries in older adults due to falls was $32 billion in the year 2013
Prevalence
www.cdc.gov/HomeandRecreationalSafety/Falls/fallcost.html

Fall Outcomes
Kannus et al, Lancet 2005
20% need medical attention
5% fractures
5-10% other serious injuries (lacerations, head injuries, dislocations, bleeding)

Hip fracture◦ Increased risk of dying within the 3-6 months
following a hip fracture◦ Functional impairment – 20-30% of older adults do
not return to baseline function◦ Pain, difficult recovery
Found down – risk of injury due to delay to medical care, can lead to functional impairment
Fear of falling – leads to social withdrawal, admission to long term care facilities
Fall Outcomes
Sterling et al, Journal of Trauma 2001

Risk Factors for Falls

Patients who have fallen in the past year are more likely to fall again
Most consistent predictor of future falls is abnormal gait or balance
Think about conditions that your patient has that contribute to abnormal gait
Risk Factors
Ganz et al, JAMA 2007

Risk Factors for Falls
Falls
External Factors
Medications
Alcohol use
Using an assistive device improperly
Patient (Intrinsic) Factors
Environmental hazards
Medical conditions
Age-related changes
Vision and hearing impairment
Cognitive impairment
Kannus et al, Lancet 2005

Patient Factors
Medical Conditions Age-related changes
Parkinson’s disease Stroke Seizures Dementia Depression Dizziness Orthostatic hypotension Arrhythmia Osteoarthritis Diabetes Peripheral neuropathy
Changes in balance Vision changes Loss of muscle

Cell death in substantia nigra -> reduction in brain dopamine levels
Clinical features:◦ Tremor at rest (pill-rolling) ◦ Cogwheeling rigidity◦ Masked facies◦ Bradykinesia◦ Shuffling gait
Treatment:◦ Symptomatic relief only◦ Dopaminergic agents
Parkinson’s Disease
Image: careplanning.blogspot.com

Early stage – Same fall risk as other community-dwelling older adults
Middle stage - patients may forget that they need an assistive device or have knee pain until they get up and start to walk◦ Lose fine motor skills, forget how to navigate
environment
Late stage– patients forget how to perform motor tasks like walking or even swallowing◦ Muscle wasting, weight loss
Dementia

Change in blood pressure with position changes
Reflex mechanisms needed to counteract gravity are less effective with age◦ Vasoconstriction◦ Elevated heart rate
Comorbid medical conditions Medications – beta blockers,
diuretics, antihypertensives Volume depletion
Orthostatic (Postural) Hypotension
Image: nlm.nih.gov

Very common in older adults Major contributor to gait and balance
problems◦ Joint pain is commonly reported in primary care◦ Balance changes due to joint abnormalities◦ Fear of falling
Pain control: Acetaminophen is safe◦ NSAIDs (ibuprofen, naproxen) are less safe due to
renal and GI effects◦ Opiates increase risk of falls and confusion◦ Physical therapy very useful
Osteoarthritis

Tight control in older adults has been shown to increase severe hypoglycemic events and mortality
Oral hypoglycemics (except for metformin) and insulin are associated with high rates of hospitalization in older adults
Peripheral neuropathy also contributes to falls
Diabetes

External Factors
Antihypertensives Diuretics Digoxin Anticholinergics
Benadryl Ditropan
(incontinence)
Polypharmacy
MEDICATIONS! Antidepressants Sedatives/Pain Meds
Benzodiazepines Opiates
Antipsychotics Dementia agents
(acetylcholinesterase inhibitors)
Dopaminergic agents

External FactorsImproper use of assist devices
Loose rugs Cords Clutter Low lighting Hand rails
Cane Walker Wheelchair/scooter
Environmental hazards

Medications that could increase risk of injury◦ Blood thinners (benefit may outweigh risk but
important to think about)
Improper use of assistive devices◦ Hand-me-down devices
Osteoporosis◦ Increased risk of fracture with a fall
Risk Factors for Injuries

Screening, Evaluation & Fall Risk Reduction

Acute fall?Two or more falls in
the past year?Difficulty with
walking or balance?
Screening for Falls
Adapted from AGS Guideline for Prevention of Falls in Older Persons, 2010
YES
NO
Gait and balance
assessment
Fall in thepast year?
YES
NO
Abnormal?
FALL ASSESSMENT
YES
NOReassess periodically

Obtain relevant medical history, physical exam, cognitive and functional assessment
Determine multifactorial fall risk:◦ History of falls Feet/footwear◦ Medications Environmental hazards◦ Gait, balance, mobility◦ Visual acuity◦ Other neurologic impairments◦ Muscle strength◦ Heart rate and rhythm◦ Orthostatic hypotension
Fall Assessment
Adapted from AGS Guideline for Prevention of Falls in Older Persons, 2010

How did the fall happen? Did the patient have any symptoms? Was there an injury? Patient risk factors for falls (medical
problems, gait imbalance, footwear) Patient risk factors for injury
(anticoagulants, osteoporosis) Where there any environmental hazards? Are there any new or problem medications? Any change in mental status or functioning?
Evaluation - History
Moncada LV. Am Fam Phys 2011

Vital signs (orthostatics) Vision exam Cognitive assessment Other neurologic impairments Muscle strength Heart rate and rhythm Gait and balance assessment
Watch your patient walk!
Evaluation – Physical Exam

Drop in systolic blood pressure of 20 mm Hg with position change (sitting to standing) within 3 minutes
Five minutes of rest before first blood pressure
Drop may be delayed so typically I check immediately with standing and again at 2-3 minutes later
Assess for lightheadedness, but not all patients who are orthostatic get lightheaded
Physical Exam – Orthostatic Hypotension

Snellen chart Pocket card okay
Wearing glasses? Glasses appropriate? Reading vs. distance Bifocals may increase
fall risk
Physical Exam – Visual Acuity

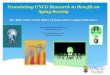
3 word recall + Clock Draw Test
Sensitivity/specificity comparable to using a cutpoint of 25 on the MMSE ◦ Sensitivity 76% (vs 79% MMSE) ◦ Specificity 89% (vs 88% MMSE)
Shorter to administer in practice than the MMSE
Physical Exam - Cognitive Assessment – Mini-Cog
Borson et al, JAGS, 2003Borson et al, Int Jnl Geri Psych, 2011

Physical Exam - Cognitive Assessment – Mini-Cog Mini-Cog
◦ Give the patient 3 words to remember Banana, chair, sunrise
◦ Administer the Clock Drawing Test – “ten past eleven” or “two forty-five” or “eight twenty”
◦ 3 word recall Scoring:
◦ 1 point for each word recalled (0-3 points)◦ Clock draw test = 2 points normal, 0 points
abnormal◦ 0-2 = positive screen (“possibly impaired”)◦ 3-5 = negative screen (“probably normal”)
Borson et al, Int Jnl Geri Psych, 2011

Clock Draw Test Examples

Neurologic exam to assess for causes of falls
Parkinsonian features Muscle strength Sensation Gait/balance
Physical Exam – Neurologic Impairments
Cardiac examination
Evaluation for abnormalities that would affect balance or positioning
Irregular heart rhythm
Bradycardia or tachycardia
Physical Exam – Heart Rate and Rhythm

Timed Up and Go◦ Start with patient seated in a chair◦ Instruct patient to stand, walk 3 meters (10 feet),
turn around, come back, and sit down in the chair◦ Time from when you say go until when patient is
re-seated in the chair◦ Patient may use his or her assistive device
Scoring:◦ >/= 12 seconds associated with increased risk of
falls 87% sensitivity & specificity
Gait & Balance Assessment
Shumway-Cook et al, PT, 2000

Home/Environmental Assessment Assess home
environment for risks for falling◦ Rugs, clutter, cords,
lighting
Consider ways to improve safety in the home environment with assistive devices

Initiate multifactorial intervention to address identified risks:◦ Minimize/adjust medications◦ Recommend appropriate exercise program◦ Treat vision impairment (consider cataracts, bifocals)◦ Manage orthostatic hypotension◦ Manage heart rate and rhythm abnormalities◦ Supplement vitamin D◦ Manage foot/footwear problems◦ Modify the home environment◦ Consider risks for injury (osteoporosis, blood
thinners)◦ Provide education and information
Indication for Intervention?
Adapted from AGS Guideline for Prevention of Falls in Older Persons, 2010

Fall Risk Reduction Check orthostatics (some patients do not report
dizziness)◦ Goal BP based on JNC 8 guidelines is 140 – 150 systolic,
reduce antihypertensives if appropriate◦ Encourage fluid intake
Vision screening ◦ Cautious use of bifocals, can increase fall risk especially with
navigating curbs and steps Home safety evaluation
◦ Medicare no longer reimburses for home safety evaluation unless it is done as part of home physical therapy treatment
◦ Can provide instructions for patient/caregiver to assess home environment

Vitamin D therapy (Grade B evidence) - 800 IU daily for at least 12 months, regardless of serum level
Physical therapy or exercise referral (Grade B evidence)◦ PT for gait & balance training◦ Assessment of appropriate assistive device and
training to use assistive device◦ Many types of exercise will reduce falls – Tai Chi, low
to high intensity, group or in home, many are effective
Multifactorial risk assessment not needed for every patient, tailor interventions to individual needs
Fall Risk Reduction – USPSTF Recommendations
Moyer, Ann Int Med, 2012

Department of Aging –> Resources for Fitness and Fall Prevention/Risk Reduction◦ Baltimore County Department of Aging –>
Maryland Access Point: 410-887-2594◦ Baltimore City Department of Aging -> Maryland
Access Point: 410-396-2273
◦ Senior Centers, exercise programs, fall prevention programs (ie. Stepping On)
◦ Online tools to help patients/caregivers do their own home safety assessments
Community Resources

Falls are a common problem for older adults
Falls are dangerous – increased risk of functional impairment and death
Risk can be modified with screening, assessment, and intervention
You can prevent an older adult from falling!
Take Home Points