Embed Size (px)
Citation preview

I&yperthyroidism to young men andgrounds of genetic hazard done.
J Nuci Med 17: 826-835, 1976
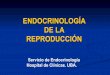
Conflicting views are expressed in the literatureand in various endocrinology textbooks on the absorbed dose of radiation that the ovaries or testesreceive during radioiodine treatment for thyrotoxicosis and on the correct clinical advice to give youngpersons regarding such treatment. There is a 100-
fold divergence among published estimates of ovarian exposure to 131! radiation (Table 1 ) . For thesereasons, we decided (A) to recalculate the gonadalradiation dose from radioiodine; (B) to comparethis radiation dosage with that from common roentgenographic procedures; and (C) to attempt an assessment of the genetic hazard that such radiation
doses involve. While there are other hazards associated with all ionizing radiation, only the geneticeffects will be considered here. Specific problemsrelated to radioiodine therapy have been reviewedby Greig (21 ) and by Becker and Hurley (22).
Gonadal radiation dose estimates in the literature.Table 1 compares published estimates of the ovarian radiation dose from 131! The higher estimatesusually result from the use of assumptions that originated as a basis for health physics rules for the protection of radiation workers and the general public.Such results are valid for their stated purpose, butthey lose meaning when extrapolated to patients
being treated for hyperthyroidism, because in this
disease the iodine metabolism and excretion patternsdo not correspond to the basic assumptions. Moreover, the destructiveness of the therapeutic radiationstill further distorts the patient's iodine metabolism,which invalidates even the dose estimates extrapolated from diagnostic quantities of radioiodine.
At least one ovarian dose estimate, that given byTrunnell et al. (13), appears to involve a decimalpoint error in the calculation. A recalculation, usingtheir data (13) and method (23), leads to a revisedestimate of 0.48 rad/mCi.
MODELOF IODINEKINETICS
The absorbed radiation dose received by the gonads is not uniquely determined by the amount ofradioactivity administered. It depends on the concentration of radioiodine as a function of time not onlyin the gonads themselves, but also in the other tissuesfrom which y radiation can reach the gonads.
The metabolism of iodine is complicated, involving not only uptake of iodide and secretion of iodi
Received July 22, 1975; revision accepted April 23, 1976.For reprints contact: James Robertson,Dept. of Labora
tory Medicine, Mayo Clinic, Rochester, MN 55901.
826 JOURNAL OF NUCLEAR MEDICINE
jIUU/INSTRUMENTATION AND PHYSICS
Gonadal Radiation Dose and Its Genetic Significance
in Radlolodine Therapy of Hyperthyroldism
James S. Robertson and Colum A. Gorman
Mayo Clinic and Mayo Foundation, Rochester, Minnesota
Published estimates of radiation dose to the gonads from 1317 therapy ofGraves' disease vary widely, largely because of differences in assumptionsregarding the details of iodine kinetics. The cakutations described in thispaper show that hyperthyroid patients treated with 10 mCi of 1317 willusually receive a total radiation dose to the ovaries or testes of less than3 rad. Several common roentgenographic diagnostic procedures may involve a greater radiation dose and a greater genetic hazard than does theusual 1317treatment for hyperthyroidism. It is important to minimize totdexposure to radiation, but it seems unreasonable to deny@ treatment for
nonpregnant young women on the
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
Dose(rad/mCi)MethodfCommentReference0.05CT
INSTRUMENTATION AND PHYSICS
nated hormones by the thyroid, but also absorptionfrom the intestinal tract, excretion by the kidneys,and secretion by the gastric and salivary glands. Thekinetic aspects of the physiology of the thyroid glandand the metabolism of iodine and the thyroid hormone have recently been reviewed in detail (24).
Even among tissues that are not actively involvedin iodine metabolism, the iodine concentration ata given time is not uniform ( 13,25—27). Nevertheless, in euthyroid and hyperthyroid patients the kinetics of iodine distribution are so strongly dominated by three rate-determining processes (renal
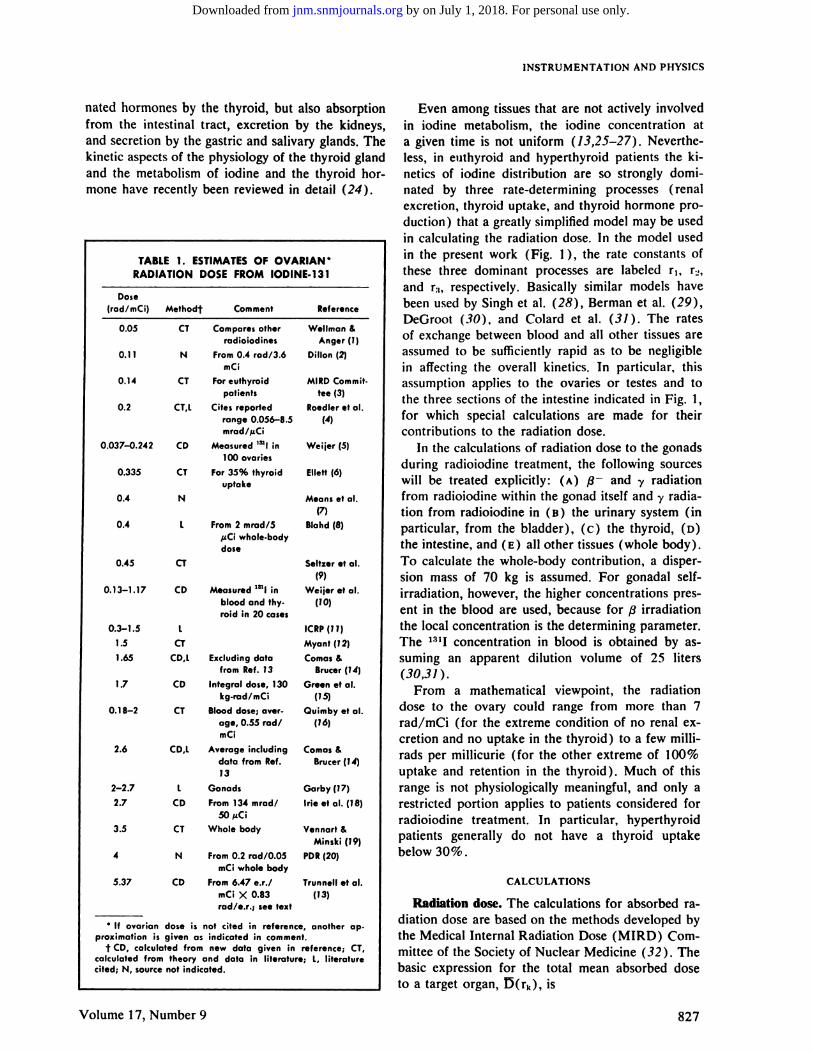
excretion,thyroiduptake,andthyroidhormoneproduction) that a greatly simplified model may be usedin calculating the radiation dose. In the model usedin the present work (Fig. I ), the rate constants ofthese three dominant processes are labeled r1, r@,and r:t, respectively. Basically similar models havebeen used by Singh et al. (28), Berman et al. (29),
DeGroot (30), and Colard et al. (31). The ratesof exchange between blood and all other tissues areassumed to be sufficiently rapid as to be negligiblein affecting the overall kinetics. In particular, thisassumption applies to the ovaries or testes and tothe three sections of the intestine indicated in Fig. I,for which special calculations are made for theircontributions to the radiation dose.
In the calculations of radiation dose to the gonadsduring radioiodine treatment, the following sourceswill be treated explicitly: (A) /@ and @yradiationfrom radioiodine within the gonad itself and y radiation from radioiodine in (B) the urinary system (inparticular, from the bladder), (c) the thyroid, (D)the intestine, and (E) all other tissues (whole body).To calculate the whole-body contribution, a dispersion mass of 70 kg is assumed. For gonadal selfirradiation, however, the higher concentrations present in the blood are used, because for@ irradiation
the local concentration is the determining parameter.The ‘@‘Iconcentration in blood is obtained by assuming an apparent dilution volume of 25 liters(30,31).
From a mathematical viewpoint, the radiationdose to the ovary could range from more than 7
rad/mCi (for the extreme condition of no renal excretion and no uptake in the thyroid) to a few millirads per millicurie (for the other extreme of I 00%uptake and retention in the thyroid) . Much of thisrange is not physiologically meaningful, and only arestricted portion applies to patients considered forradioiodine treatment. In particular, hyperthyroidpatients generally do not have a thyroid uptakebelow 30%.
CALCULATIONS
Radiation dose. The calculations for absorbed radiation dose are based on the methods developed bythe Medical Internal Radiation Dose (MIRD) Cornmittee of the Society of Nuclear Medicine (32 ) . Thebasic expression for the total mean absorbed doseto a target organ, l5(rk), is
TABLE 1. ESTIMATESOF OVARIAN *RADIATION DOSE FROM IODINE-131
Compares otherradioiodines
0.11 N From 0.4 rad/3.6mCi
0.14 CT For euthyroidpatients
0.2 CT,L Citesreportedrange 0.056—8.5mrad/j@Ci
0.037—0.242 CD Measured‘@‘lin100ovaries
0.335 CT For 35% thyroiduptake
0.4 N
0.4 L From 2 mrad/5@iCiwhole-bodydose
CT
0.13—1.17 CD Measured “Iinblood and thy.roidin20 cases
0.3—1.5
1.51.65
0.45
CTCD,L Excludingdata
from Ref. 73
17 CD Integral dose, 130kg-rod/mCi
0.18—2 CT Blood dose; average, 0.55 rad/mCi
2.6 CD,L Average includingdata from Ref.73
2—2.7 L Gonads2.7 CD From134 mrad/
[email protected] CT Whole body
4 N From0.2 rad/0.05mCi whole body
5.37 CD From6.47 e.r./mCi X 0.83rad/e.r.; see text
Wellman &Anger (1)
Dillon (2)
MIRD Committee (3)
Roedler et al.
(4)
Weijer (5)
Ellett(6)
Means et al.(7)
Blahd (8)
Seltzer et al(9)
Weijer etal.
(10)
ICRP(11)Myant (72)
Comas&Brucer (74)
Green et al.(75)
Quimby et al.
(76)
Comas&Brucer (74)
Garby (17)
Inc et al. (18)
Vennart &Minski (79)
PDR (20)
Trunnell et al.
(13)
* If ovarian dose is not cited in reference, another ap
proximation is given as indicated in comment.t CD,calculatedfromnewdatagivenin reference;CT,
calculated from theory and data in literature; L, literaturecited; N, source not indicated.
Volume 17, Number 9 827
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
Source organs Ovariesj Testesj
ROBERTSON AND GORMAN
MODEL FOR IODINE METABOLISM
15(rk) =h
17(rk) = @A11(0,@o)‘h mk
where i@(rk) is the total mean dose to the target organ rk (rads) ; @(rkE—r),)is the dose to rk from sourceorgan r1, (rads) ; A,,(0, oc ) is the cumulated activityin source organ r1, from t = 0 to t =@ (PCi-hr);mk is the mass of the target organ rk (gm) ; @Iis themean energy emitted per nuclear transformation for
i-type radiations (gm-rad/,@Ci-hr) ; 4I(rk@—r),)is theabsorbed fraction of energy for the target organ rkfor i-type radiations emitted in source region r31.
Values for @ifor ‘@‘Iare available in MJRD Pam
H Extrathyroidal Hlod ide
FIG.1. Modelof iodinemetabolismas simplifIed for use in dose calculations.Extrathyroidal thyroid hormone is considered to be uniformly distributed through.out body.
phiet No. 10 (33) . The@ for nonpenetrating radiations from ‘@‘Iis 0.4165 gm-rad/@Ci-hr. Since valuesfor the mean dose per unit cumulated activity, S,have been tabulated (36) , many of the tedious stepsin the dose calculation can be eliminated:
S(rk*-r),) = mk
where S(rk*—rI,) is the mean dose to rk per unitcumulated activity in source organ r11.Thus, we have
15(rk) = @A31(0,oc)S(rkE—r),).h
When S values are used to calculate the dose, certainspecific assumptions are implied, namely, the massesof target and source organs as specified in Ref. 36,a uniform distribution of activity in the source organ,a bladder containing 200 ml of urine, and the nucleardata.
Table 2 gives the “S―values ( in rad/@Ci-hr) forovaries and testes irradiated from 1311. For thesources shown, note that the “5―values for the ovaries are larger than those for the testes. However, theemphasis here will be on ovarian irradiation.
Cumulated activity (A). Values for A for ‘@‘Iarenot yet available in the MIRD pamphlets and mustbe developed independently. To represent radioiodine distribution in the body, we use three compartments (whole body, thyroid, and urinary bladder)during the first 24 hr, and four compartments (theoriginal three plus extrathyroid radioiodinated thyroid hormone) from then on. The other compartments indicated in Fig. 1 are given special attention.
TABLE 2. “5―FACTORS FOR 131I RADIATIONDOSE (rad/@@Ci-hr)TO GONADS
FROM VARIOUS ORGANS*
Bladder contentsStomach contentsSmall intestine plus contentsUpper large intestine contentsLower large intestine contentsOvariesTestesThyroid
Total body
1.9E—05 1.4E—051.4E—06 1.3E—072.7E—05 13.4E—05 1.2E—065.OE—05 5.7E—063.9E—02 —
— 1.3E—024.1E—08 7.2E—091.1E—05 1.OE—05
.AbstractedfromSnyderetal.(36).t In thistable,thenotationsareabbreviatedforms,e.g.,
1.OE—06represents 1.0 X 10@°.
828 JOURNAL OF NUCLEAR MEDICINE
H— ExtrathyroidalThyroid Hormone
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
and r,=0.0018/hr)RadiationA/A,XL000doseSource
organ (@Ci-hr/j@Ci)(rad/mCi.hr)(rad/mCi)
INSTRUMENTATIONANDPHYSICS
tion is assumed not to exceed that in the blood(5,13,25—27).
The values of the rate constants r1, r2, and r3 (Fig.1 ) depend on the patient's physiologic status. Keating et al. (37) reported that the average renal excretion rate of iodide for euthyroid and hyperthyroidpatients was r1 = 7.2 % /hr, and their “collectionrate―(chiefly thyroid uptake, but more broadly defined to include all nonrenal processes removingiodide from the blood) was r2 = 3.9% /hr for normal subjects and 21 .7% /hr for hyperthyroid patients(37) . The values chosen for r3 will be discussedunder the section on “Results.―For predictive purposes, it would be convenient to relate the iodideexcretion rate to the glomerular filtration rate, butthe relationship is not simple and for a given patienta direct measurement of the radioiodide excretionrate is more reliable.
Computations. A prototype calculation is outlined
in Table 3, using data representative of a hyperthyroid patient treated with 1311. The values of A/A0were obtained by numerical evaluation of the equations given in the Appendix and the special calculations described in the foregoing section. The “S―values from Table 2 are multiplied by 1,000 to convert from rad/@@Ci-hr to rad/mCi-hr. The bladderdose was calculated by assuming voiding at 4, 10,16, and 24 hr and at 12-hr intervals from 1 to 53days (when 99% decay of 1311is reached). For the
a-@ @;
b:@.@
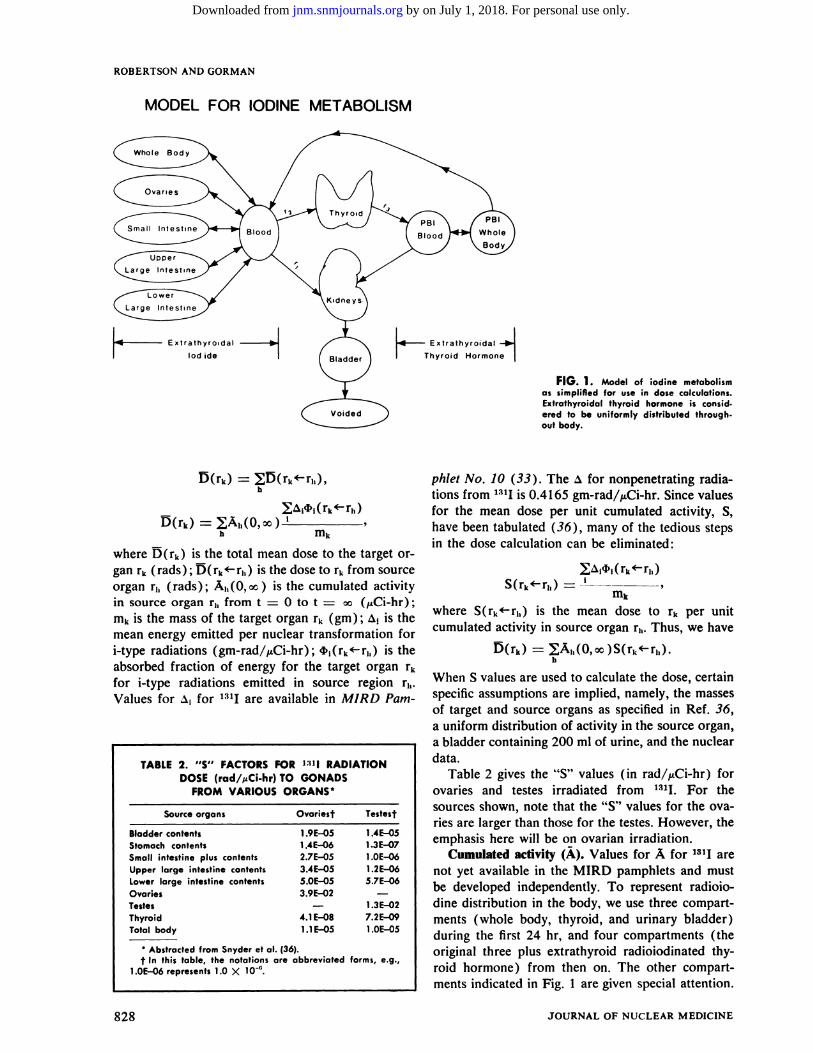
FIG.2. Radioactivityexcretedinurine.Curveiscumulativeexcreted activity, expressed as percentage of administered activity,without correction for radioactive decay. Activity present in bladderis indicated by shaded areas, and voided portion is representedby unshaded areas. Because of decay, voided activity decreasesexponentially, as indicated by slanted tops of unshaded areas,except as additions to it are made when bladder is emptied.Curve was computed by assuming thyroid uptake of 75% of ad
ministered dose. Radiation dose to ovary from bladder is propor.tional to shaded areas, subject to corrections for changes in geom.etry as bladder size changes.
The kinetics of radioiodine is described by a system of differential equations, and integration of theseexpressions gives the desired values of A for eachcompartment. This method accounts for the totalactivity administered A0. That is, at any time t thesum of the activities in the various tissues and urineequals A@e@t. (For the present purposes, fecal excretion is included in urinary excretion. ) An outlineof the derivations is given in the Appendix.
Special calculations are needed for the urinarybladder in order to take the effects of voiding intoaccount. This has been studied experimentally byInc et al. (18) and by Comas and Brucer (14). Themethod we have used is illustrated in Fig. 2. In thisexample it is arbitrarily assumed that the bladderis emptied at 4, 10, 16, and 24 hr. Only the urinethat enters the bladder during the 4—10-hr intervalis used in calculating the dose to the ovary for thesecond period, and so on. The shaded areas in Fig. 2indicate the portion of the integrated activity due to131! in the bladder.
Special calculations were also used for the radiation doses to the ovaries from activity in the intestinaltract and from ovarian self-irradiation, because theseinvolve “S―factors greater than that for the wholebody (Table 2) . The activity in each section of theintestine is assumed to be proportional to its weight.In the calculation of the contribution to the radiationdose from the whole body, the activity assigned tothe intestine is subtracted.
For ovarian self-irradiation, the genetically effec
tive $ dose is assumed to equal the average ovarian $ dose (5) and the ovarian activity concentra
Hours
TABLE 3. PROTOTYPECALCULATION OFRADIATION DOSE TO OVARIES FROM 1@1I(X = 0.003588/hr; ri 0.072/hr; r2 0.217/hr;
ThyroidBladder
OvariesSmall intestineUpper large
intestineLower large
intestineWhole body
(remaining)
TotalVoided
Total
142.61.9920.00220.0964
0.0000410.019
39
0.027
0.00580.03780.08640.0026
0.0396 0.034 0.0013
0.0269 0.050 0.0013
6.297
151.06127.67
278.73
0.011 0.0693'
0.2045
. This result overestimates the whole.body contribution tothe ovarian dose because of partial duplication of the selfirradiation component (38). Also, the “S'factor for wholebody has not been corrected for the deletion of the intestinal component.
Volume 17, Number 9 829
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
: :; ‘@inal'@adioi:dideuptakeinthyroid(%)
ROBERTSON -ANDGORMAN
0.7
0.6 [1@I-radiotiondosetoovariesfrommajorsources
r2@r@Tr/(ITr)
r3:0.18 %/h
@O.5
@ 0.4
.@
.@02
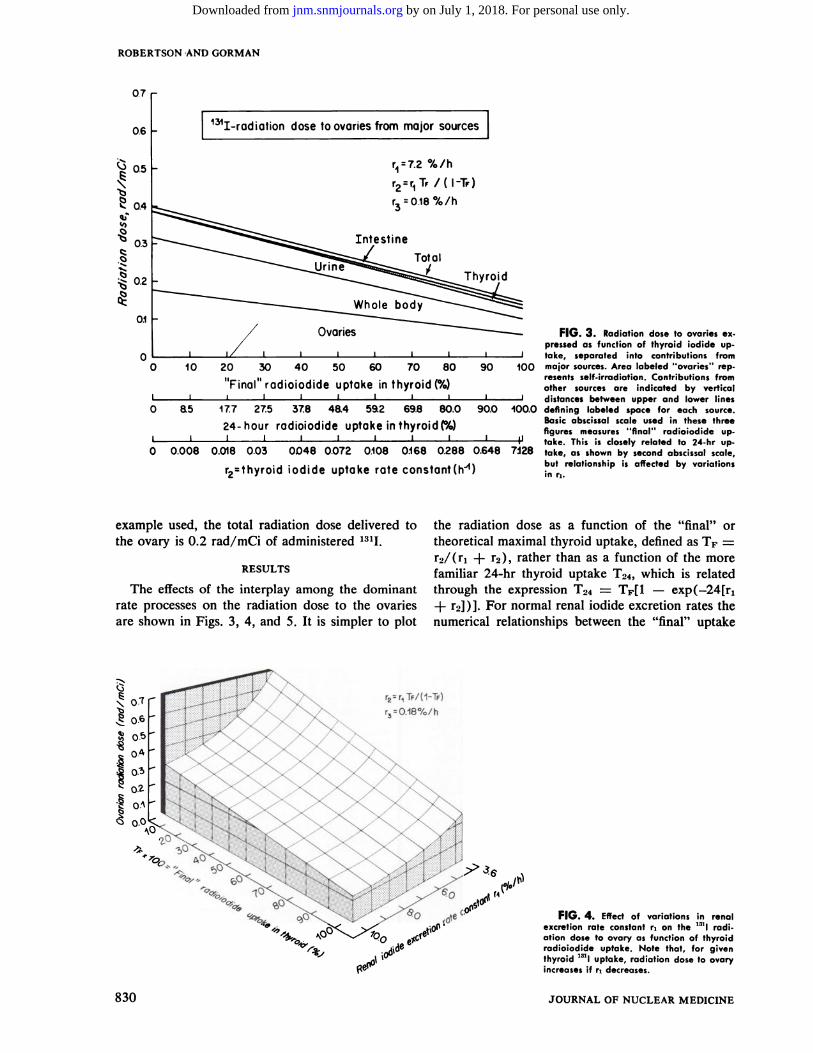
0.1FIG.3. Radiationdosetoovariescx
pressed as function of thyroid iodide up.take, separated into contributions from
90 100 major sources.Area labeled ‘ovaries―rep.resents self-irradiation. Contributions fromother sources are indicated by vertical@ I distancesbetweenupperandlowerlines
90.0 100.0 defining labeled space for each source.Basic abscissal scale used in these threefigures measures ‘final―radioiodide up
1 p take. This is closely related to 24-hr up
0.648 7i28 take,as shownby secondabscissalscale,but relationship is affected by variationsin ri.
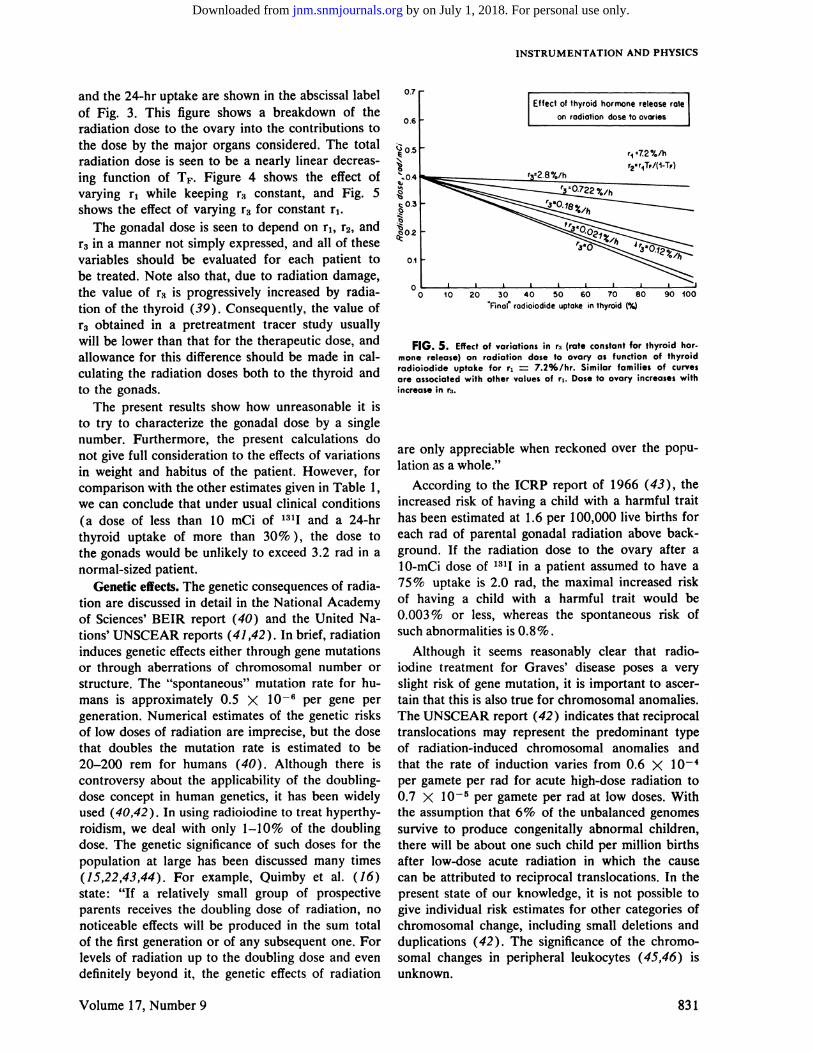
FIG.4. Effectof variationsin renalexcretion rate constant r, on the “Iradiation dose to ovary as function of thyroidradioiodide uptake. Note that, for giventhyroid 1311uptake, radiation dose to ovaryincreases if ri decreases.
0
1.7 27.5 3.8 48.4 592 69.8 80.0
@4-hour radioiodide uptake in thyroid (%)
0 0.008 0.018 0.03 0048 0.072 0.108 0@68 0288
r2thyroid iodide uptake rate constant(h@)
example used, the total radiation dose delivered tothe ovary is 0.2 rad/rnCi of administered 131!.
RESULTS
The effects of the interplay among the dominantrate processes on the radiation dose to the ovariesare shown in Figs. 3, 4, and 5. It is simpler to plot
the radiation dose as a function of the “final―ortheoretical maximal thyroid uptake, defined as TF =r2/(r1 + r2) , rather than as a function of the morefamiliar 24-hr thyroid uptake T24, which is relatedthrough the expression T24 = TF[1 — exp(—24[r1+ r2])}. For normal renal iodide excretion rates thenumerical relationships between the “final―uptake
@0.6
I
r2 r1TF/(1—TF)
r30.18%/h
4#yoo@@
-“:1,-:,‘@o%.
830 JOURNAL OF NUCLEAR MEDICINE
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
[@fect of thyroidhormone release
I onradiationdosetoovaries
ri ‘72%/hr2.r1T,/(1—T,)
INSTRUMENTATION AND PHYSICS
and the 24-hr uptake are shown in the abscissal labelof Fig. 3. This figure shows a breakdown of theradiation dose to the ovary into the contributions tothe dose by the major organs considered. The totalradiation dose is seen to be a nearly linear decreasing function of TF. Figure 4 shows the effect ofvarying r1 while keeping r3 constant, and Fig. 5shows the effect of varying r3 for constant r1.
The gonadal dose is seen to depend on r1, r2, andr3 in a manner not simply expressed, and all of thesevariables should be evaluated for each patient tobe treated. Note also that, due to radiation damage,the value of r3 is progressively increased by radiation of the thyroid (39). Consequently, the value of
r3 obtained in a pretreatment tracer study usuallywill be lower than that for the therapeutic dose, andallowance for this difference should be made in calculating the radiation doses both to the thyroid andto the gonads.
The present results show how unreasonable it isto try to characterize the gonadal dose by a singlenumber. Furthermore, the present calculations donot give full consideration to the effects of variationsin weight and habitus of the patient. However, forcomparison with the other estimates given in Table I,we can conclude that under usual clinical conditions(a dose of less than 10 mCi of 131! and a 24-hrthyroid uptake of more than 30% ), the dose tothe gonads would be unlikely to exceed 3.2 rad in anormal-sized patient.
Genetic effects. The genetic consequences of radiation are discussed in detail in the National Academyof Sciences' BEIR report (40) and the United Nations' UNSCEAR reports (41,42). In brief, radiationinduces genetic effects either through gene mutationsor through aberrations of chromosomal number orstructure. The “spontaneous―mutation rate for humans is approximately 0.5 X 106 per gene pergeneration. Numerical estimates of the genetic risksof low doses of radiation are imprecise, but the dosethat doubles the mutation rate is estimated to be20—200rem for humans (40). Although there iscontroversy about the applicability of the doublingdose concept in human genetics, it has been widelyused (40,42) . In using radioiodine to treat hyperthy
roidism, we deal with only 1—10% of the doublingdose. The genetic significance of such doses for thepopulation at large has been discussed many times(15,22,43,44) . For example, Quimby et al. (16)state: “Ifa relatively small group of prospectiveparents receives the doubling dose of radiation, nonoticeable effects will be produced in the sum totalof the first generation or of any subsequent one. Forlevels of radiation up to the doubling dose and evendefinitely beyond it, the genetic effects of radiation
0.7
0.6
0.1
0
‘Finalrodiolodide uptake in thyroid (%)
FIG.5. Effectofvariationsinr3(roteconstantforthyroidhormone release) on radiation dose to ovary as function of thyroidradiolodide uptake for ri 7.2%/hr. Similar families of curvesare associated with other values of [email protected] to ovary increases withincreasein r@.
are only appreciable when reckoned over the population as a whole.―
According to the ICRP report of 1966 (43), theincreased risk of having a child with a harmful traithas been estimated at 1.6 per 100,000 live births foreach rad of parental gonadal radiation above background. If the radiation dose to the ovary after aI 0-mCi dose of 131! in a patient assumed to have a75 % uptake is 2.0 rad, the maximal increased riskof having a child with a harmful trait would be0.003% or less, whereasthe spontaneousrisk ofsuch abnormalities is 0.8%.
Although it seems reasonably clear that radioiodine treatment for Graves' disease poses a veryslight risk of gene mutation, it is important to ascertam that this is also true for chromosomal anomalies.The UNSCEAR report (42) indicates that reciprocaltranslocations may represent the predominant typeof radiation-induced chromosomal anomalies andthat the rate of induction varies from 0.6 X 10@per gamete per rad for acute high-dose radiation to0.7 X 10—sper gamete per rad at low doses. Withthe assumption that 6% of the unbalanced genomessurvive to produce congenitally abnormal children,there will be about one such child per million birthsafter low-dose acute radiation in which the causecan be attributed to reciprocal translocations. In thepresent state of our knowledge, it is not possible togive individual risk estimates for other categories ofchromosomal change, including small deletions andduplications (42) . The significance of the chromosomal changes in peripheral leukocytes (45,46) isunknown.
Volume 17, Number 9 831
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from

Males Females
Procedures Median Range of means Median Range of means
ROBERTSON AND GORMAN
ment. The two principal paths of removal of iodide fromthis compartment are indicated by r,, the fractional rate ofexcretion by the kidneys into urine, and r,, the fractionalrate of uptake by the thyroid. A 24-hr delay in the secretion of radioactive thyroid hormone is assumed, after whichthe loss of radioiodine from the thyroid is indicated by r:.This rate constant includes both the fractional rate of secretion of protein-bound iodine and any loss of free iodide fromthethyroid.
The distribution of protein-bound iodine is known to dificr from that of iodide (57,58), but this difference is neglected on the grounds that its effect on the gonadal doseis minor. The two iodine compartments are treated as beingseparate but coextensive, so that the two values of A(0,t)/A@for a given organ are additive.
Degradation of the thyroid hormone introduces a feedback into the iodide compartment. The mathematical complications introduced by this lead to equations that, althoughreadily handled by analog or digital computers. are toounwieldy for analytic solutions. For the present purposesit is assumed that the conversion to iodide is relatively rapid,
so that the fractional rate of excretion of the degradedthyroid-hormone iodine may be equated to that of iodide.This simplification leads to solutions that can be evaluatedon a programmable desk calculator, and these equations arederived in the following sections. The symbols used are definedinTable Al.
Equations. With the simplifications discussed, the equations for the rates of change of activity in the four compartments are as follows:
dB/dt=—(X+r,+r2)B=—X,BdT/dt = r,B —(X + r@)T = r2B —XTdP/dt = r:T —(X+ r,)P = r:T —X1PdU/dt = r1(B + P) —XU.
The following solutions for this system of equations describe the fractional activities A(t)/A@ in each of the designatedsites:
B = Boe@2t,
T =@ r2B@ Ee@;t ex2t] + ToeXat,Lr, + r2—r3J
P =@ r2r,B@ Ie_xst___eXtl _ Ie_xIt@ e@8t]
Lri+r2—r,JL r2 J L r1—r,
+ I r,T, ] [e@C3teXltl,Lrs r,
DISCUSSION
In selecting any form of treatment, one alwaystries to assess the alternatives available, the risksincurred, and the benefits to be expected. Surgicaltreatment, even in skilled hands, results in vocal cordparalysis or permanent hypoparathyroidism in about1% of patients (47), and antithyroid drugs are associated with serious unfavorable reactions in 0.1—1%
of patients (48). Radioiodine treatment providesrapid, effective, permanent, and inexpensive control
of thyrotoxic Graves' disease. The disadvantages arethe progressively increasing incidence of hypothyroidism (49), the still unsupported possibility of anincreased incidence of thyroid carcinoma (39,50—56),
and the possible genetic effects.
Table 4 shows the dose to the gonads from variouscommonly used diagnostic procedures. In most patients with Graves' disease treated with radioiodine,
the gonad radiation dose will be in the same rangeas that from a barium enema, an excretory urogram,or a hysterosalpingogram. In our view, the evidencestrongly supports the conclusion that 131! therapy
for Graves' disease poses such a slight genetic hazard
that, solely on the grounds of genetic risk, it is unreasonable to withhold it from young men and nonpregnant young women. Whether any of the otherdrawbacks contraindicate its use is a matter to bedecided for each individual patient.
APPENDIX
Formulas used for integrated activity, A/An, in selectedtissues. Assumptions.The simplifiedmodel of iodine metabolism diagrammed in Fig. 1 is used.
If radioiodine is administered orally, the kinetics of thefirst half hour or so depends on absorption from the gastrointestinal tract, but for simplicity we shall assume intravenous administration. A small correction for oral administration may be applied if desired.
Except for the initial delay in the intestine and a similardelay in the reabsorption of iodide secreted into the intestinal tract, it will be assumed that the exchange rates betweenblood and all nonthyroid organs are sufficiently rapid thatthe nonthyroid iodide may be treated as a single compart
TABLE 4. GONAD DOSE (mrad) PER EXAMINATION WITH COMMON RADIODIAGNOSTIC PROCEDURES*
Barium meal 30
Urography (descending) 430Retrograde urography 580Colon, barium enema 300Upper femur 920Obstetric, abdomen —Hysterosalpingography —
* Abstracted from UNSCEAR report (42), p. 158.
5—23015—2,090
150—2,09095—1,590
230—1,710
340590520870240300
1,270
60—830270—1,160
85—1,390460—175058—680
110-1,600275—2,700
832 JOURNAL OF NUCLEAR MEDICINE
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from

Symbol Explanation Units
Time
INSTRUMENTATION AND PHYSICS
A(24, @).Simplifiedexpressions for these values, assuming thatB0 = 1 and T0 = U0 = P0 = 0, are as follows:
1@(0,co)= x+ r@+ r,'
r r2@ [1(0,24)—@(0,24)]f(0,m) = Lri + r2J
r r2B(24)
r r, 1@@(24,m)=[____] T(24,m),
U(0,m)= @t(0,24)+ @{r,[@(24,m)+ @(24,co)l+ U(24)l,
in which1(0,24)=@ (1 —e24X).x
REFERENCES
1. WELLMAN HN, ANGER RT: Radioiodine dosimetryand the use of radioiodines other than ‘9in thyroid diagnosis. Semin Nod Med 1: 356—378,1971
2. DILLON RS: Handbook of Endocrinology: Diagnosisand Management of Endocrine and Metabolic Disorders.Philadelphia, Lea & Febiger, 1973, p 245
3. MIRD/Dose Estimate Report: Summary of currentradiation dose estimates to humans from @9,121!,19,@13n1 1311, and “I as sodium iodide. I Nuci Med 16: 857—860,
I9754. ROEDLER HD, KAUL A, HINZ 0, et al. : Genetically
significant dose from the use of radiopharmaceuticals. In
Population Dose Evaluation and Standards for Man and HisEnvironment, IAEA-SM-184/3. Vienna, IAEA, 1974, pp377—393
5. WEIJERDL: Beta radiation from radioactive iodine(1―) : Measurementof one hundred human ovaries.J CanAssocRadioll5:153—162,1964
6. ELLETTWH: Calculation of average body and gonadaldose following ‘•@@Iingestion by normal subjects. Royal Postgraduate Medical School, Medical Physics Department. ReportWHE/13.2.67,1969
7. MEANS JH, DE GROOT U, STANBURY JB: The Thyroid and Its Diseases, 3rd ed. New York, McGraw-Hill,1963,pp 232—233
8. BLAHD WH : Nuclear Medicine, 2nd ed. New York,McGraw-Hill, 1971, p 121
9. SELTZER RA, KEREIAKES JG, SAENGER EL: Radiation
exposure from radioisotopes in pediatrics. N Eng! I Med271:84—90,1964
10. WEIJER DL, DUGGAN HE, SCOTT DB: Total bodyradiation and dose to the gonads from the therapeutic useof iodine I 3 1: A survey of 20 cases. I Can Assoc Radiol I I:50—56,1960
11. International Commission on Radiological Protection:Protection of the Patient in Radioni@clide Investigations,Publication I 7. New York, Pergamon, 197 1, p 45
12. MYANT NB: The radiation dose to the body duringtreatment of thyrotoxicosis by 13 1-1. Minerva Nod 8 : 207—210,1964
13. TRUNNELL JB, DUFFY BJ, G0DwIN JT, et al. : Thedistribution of radioactive iodine in human tissues: Necropsy study in nine patients. I Clin Endocrinol Metab 10:1007—1021,1950
14. COMAS F, BRUCER M: Irradiation of the ovaries from
TABLE Al. DEFINITIONS OF SYMBOLS
t
xhr
hr@Radioactive decay constant(X= In 2/physicalhalf-life)
ri Rate constant for urinary iodideexcretion
hr@
r2 Rate constant for thyroid iodide
uptake
hr@
hr@r3 Rate constant for thyroid hormone release
A0
A(t)
lodine-131 administered @Ci
zCi/j@CiFraction of administered activityat time t in designated organor region, with the followingsubstitutions for A:B = whole body (all organs
not otherwise specified)T thyroid (iodide +
hormone)
P = extrathyroid thyroidhormone
U = urineI= totalradioiodine
A(ti,ts) f @:Adt, the integrated frac
tional activity in designatedorgan between times ti and t2
@Ci-hr/@Ci
XI= X + r,x2= x + r,+x3=@ + rs
833Volume 17, Number 9
U = r r1B0@ [e@t e—X2t1Lrl + r2 —r3j
— [ri r @] (B0 + To)[e@t e@C1tJ
—r3J
[r,—r1+r2—r, To][eXtC—X3t1++ r, r3] [ r2B,
Note that the decay factor C@t could be factored out of eachof the above expressions, but the forms shown are convenientfor computer program coding.
Values of A(t,,t,) are obtained by substituting the expressions(CXtI e@@zt5) /X for e@t in the foregoing formulas, with
x = x, x1,x2,or X3astheseexpressionsoccur.Thissubstitution has the effect of integrating the original expressionbetween ti and t2. For A(0,@ ), the e'@ terms are replaced byI /X, which is the integral of e@t for the time interval t = 0tot= m@
A delay in the release of the radioactive thyroid hormone isallowed for by using a simplified set of equations, with r3 = 0for the first 24 hr. The A(24) values so calculated are substitutedfor the A0 values in these formulas for calculation of A(t)and A(24,t), using (t —24) for t.
For calculations of @A(0,@ ), except for the contributionfrom urine in the bladder, the values of A and A for intermediate times are not needed. The considerations involved inobtaining the portion of U attributable to the bladder arediscussed in the main portion of the text. For the other sources,the A(0, m) used in calculating the dose is the sum A(0,24) +
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
ROBERTSON AND GORMAN
the urinary excretion of iodine 13 1. Am I Roenigenol Radium TherNuclMed83: 501—506, 1960
15. GREEN M, FISHER M, MILLER H, et al. : Blood radiation dose after “IItherapy of thyrotoxicosis : Calculationswith reference to leukaemia. Br Med I 2: 210—215,1961
16. QUIMBY EH, FEITELBERG S, GROSS W: RadioactiveNuclides in Medicine and Biology. Philadelphia, Lea &Febiger,1970,pp 132,148—151
17. GARBY L, NOSsNIN B, LöFBEBERG S: Radiation dosesfrom isotopes in medical use. A collection of data basedupon a critical survey of the literature. Stockholm, SwedishNational Institute of Radiation Protection, 1969
18. huE H, TAKESHITA K, MURAKAMI K, et al. : Gonadexposure due to 1-13 1 thyroid function test: Special consideration for 1-131 in urinary bladder. Kyushu I Med Sci12: 83—91,1961
19. VENNART J, MINSKI M : Radiation doses from administered radionuclides. Br I Radio! 35: 372—387,1962
20. Physicians' Desk Reference for Radiology and Nuclear Medicine. Oradell, NJ., Medical Economics Co., 1975,p 82
21. GREIG W: Radioactive iodine therapy for thyrotoxicosis.BrJSurg6O:758—765,1973
22. BECKER DV, HURLEY JR: Complications of radioiodine treatment of hyperthyroidism. Semin Nod Med 1:442—460,1971
23. MARJ.NELLI LD, QUIMBY EH, HINE GJ : Dosage determination with radioactive isotopes. II. Practical considerations in therapy and protection. Am I Roentgenol RadiumTherNuciMed 59:260—281,1948
24. GREER MA, SoLoMoN DH: Handbook of Physiology.Section 7: Endocrinology. Vol. 3. Thyroid. Washington,D.C., American Physiological Society, 1974
25. EVANS TC, HODGES RE, BRADBURY JT: I― contentin ovarial and other tissues at different times after oral administration.I NuclMed 5:733—737,1964
26. MYANT NB, CORBETT BD, HONOUR AJ, Ct al. : Distribution of radioiodide in man. C/in Sci 9: 405—419,1950
27. KURLAND GS, FREEDBERG AS: The distribution of1131 in tissue obtained at necropsy or at surgical operation
in man. I Clin Endocrinol Metab 11: 843—856,195128. SINGH B, SHARMA SM, PATEL MC, et al. : Kinetics
of large therapy doses of 1@@Iin patients with thyroid cancer.INuciMed 15:674—678,1974
29. BERMAN M, HOFF E, BARANDES M, et al. : Iodinekinetics in man: A model. I Cli,z Endocrino! Metab 28:1—14,1968
30. DEGROOT U : Kinetic analysis of iodine metabolism.I C/in Endocrinol Metab 26: 149—173,1966
3/. COLARD JF, VERLY WG, HENRY JA, et al. : Fate ofthe iodine radioisotopes in the human and estimation ofthe radiation exposure. Health Phys I I : 23—35,1965
32. LOEVINGER R, BERMAN M : A Revised Schema forCalculating the Absorbed Dose from Biologically Distributed Radionuclides. MJRD Pa@nphlet No 1, Revised. NewYork, Society of Nuclear Medicine, March 1976
33. DILLMAN LT, VON DER LAGE FC: Radionuclide Decay Schemes and Nuclear Parameters for Use in RadiationDose Estimation. MIRD Pamphlet No 10. New York, Society of Nuclear Medicine, Sept. 1975
34. LEDERER CM, HOLLANDER JM, PERLMAN I: Table
of Isotopes, 6th ed. New York, Wiley, 196735. SNYDER WS, FORD MR. WARNER GG, et al. : Esti
mates of absorbed fractions for monoenergetic photonsources uniformly distributed in various organs of a heterogeneous phantom. I Nucl Med 10: Suppi 3, 5—52,1969
36. SNYDER WS, Foiw MR. WARNER GG, et al. : “5,―Absorbed Dose per Unit Cumulated Activity for SelectedRadionuclides and Organs. MIRD Pamphlet No. 11. NewYork, Society of Nuclear Medicine, Oct. 1975
37. KEATING FR, POWER MH, BERKSON I, et al. : Theurinary excretion of radioiodine in various thyroid states.JClinlnvest26:1138—1151,1947
38. CLOUTIER RJ, WATSON EE, ROHRER RH, et al. : Calculating the radiation dose to an organ. I Nuc! Med 14:53—55,1973
39. DONIACH I: Effects of radiation on thyroid functionand structure. In Handbook of Physiology. Section 7: Endocrinology, Green MA, Solomon DH, eds. Washington,D.C., American Physiological Society, 1974, vol 3, pp 359—375
40. Advisory Committee on the Biological Effects of Ionizing Radiations: The Effects on Populations of Exposureto Low Levels of Ionizing Radiation. Washington, D.C., National Academy of Sciences/National Research Council,1972
41. United Nations Scientific Committee on the Effects ofAtomic Radiation: Report of the General Assembly. 5eventeenth Session, Suppi 16 (A/5216). New York, UnitedNations, 1962, pp 88, 101
42. United Nations Scientific Committee on the Effects ofAtomic Radiation : Ionizing Radiation: Levels and Effects.A Report of the Unite@d Nations Scientific Committee on theEffects of Atomic Radiation to the General Assembly. E. 72,Ix 17. New York, United Nations, 1972
43. InternationaiCommission on Radiological Protection,Committee I: The @valuationof risks from radiation. HealthPhys 12:239—302,1966
44. SOBELSFF1: Estimation of the genetic risk resultingfrom the treatment of women with ‘31iodine.Strahlentherapie138:172—177,1969
45. Bovu E, BUCHANAN WW, LENNOX B: Damage to
chromosomes by therapeutic doses of radioiodine. Lancet 1:977—978,1961
46. NOFAL MM, BEIERWALTESWH : Persistentchromosomal aberrations following radioiodine therapy. J NuciMedS: 840—850, 1964
47. BLACK BM : The present position of thyroidectomy.AdvSurg4: 73—103, 1970
48. WILLIAMS RH : Textbook of Endocrinology, 5th ed.Philadelphia, W. B. Saunders, 1974, p 181
49. DUNN JT, CHAPMANEM: Rising incidence of hypothyroidism after radioactive-iodine therapy in thyrotoxicosis.N EngII Med 271:1037—1042,1964
50. DEGROOT L, PALOYAN E : Thyroid carcinoma andradiation: A Chicago endemic. JAMA 225: 487—491,1973
51. MCDOUGALL IR, KENNEDY JS, THOMSON JA: Thy
roid carcinoma following iodine-131 therapy: Report of acase and review of the literature. I C/in Endocrinol Metab33: 287—292,1971
52. REFETOFF S, HARRISON I, KARANFILSKI BT, Ct al.:
Continuing occurrence of thyroid carcinoma after irradiation to the neck in infancy and childhood. N Engl I Med292:171—175,1975
53. HAYEK A, CHAPMAN EM, CRAWFORD JD: Long-term
results of treatment of thyrotoxicosis in children and adolescents with radioactive iodine. N Engl I Med 283 : 949—953,1970
54. BRAVERMAN LE: Consequences of thyroid radiation
in children. N Engl I Med 292: 204—205, 1975
55. DOBYNS BM, SHELINE GE, WORKMAN JB, et al.:
834 JOURNAL OF NUCLEAR MEDICINE
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
INSTRUMENTATION AND PHYSICS
Malignant and benign neoplasms of the thyroid in patientstreated for hyperthyroidism : A report of the cooperativethyrotoxicosis therapy follow-up study. I C/in Endocrino!Metab 38:976—998,1974
56. SAFA AM, SCHUMACHER OP, RODRIGUEZ-ANTUNEZ A:
Long-term follow-up results in children and adolescentstreated with radioactive iodine (19) for hyperthyroidism.NEnglJMed292: 167—175,1975
57. OPPENHEIMERJH, SURKS MI: Quantitative aspects
of hormone production, distribution, metabolism, and activity. In Handbook of Physiology. Section 7: Endocrinology,Green MA, Solomon DH, eds. Washington, D.C., Amencan Physiological Society, 1974, vol 3, pp 197—214
58. VAN MIDDLESWORThL: Metabolism and excretion ofthyroid hormones. In Handbook of Physiology. Section 7:Endocrinology, Greer MA, Solomon DH, eds. Washington,
D.C., American Physiological Society, 1974, vol 3, pp 215—231
October 25—29,1976 Ambassador Hotel Los Angeles, California
The International Atomic Energy Agency has announced an International Symposium on Medical Radio
nuclide Imaging, to be held on October 25—29,1976, in Los Angeles, California. The program will placeemphasis on recent advances in methods and techniques. Clinical applications will be included in so far asthese reflect improvements in techniques. The symposium will also evaluate the potentialities of medical
radionuclide imaging in relation to those of other imaging disciplines.
To register as an observer for this symposium, please contact:
John H. KaneOffice of Public AffairsU.S.EnergyandResearchDevelopmentAdministrationWashington, D.C. 20545
September 29, 1976 Guy's Hospital London, England
A Symposiumon Radioisotopesin Cardiology,jointlyorganizedbytheBritishInstituteof Radiologyandthe BritishCardiac Society,will be held on Wednesday,September29th, 1976,at the GreenwoodConferenceCentre of Guy's Hospital in London. All interested parties are invited to attend.
Theregistrationfee of £9.50will include lunch,morning coffee, and afternoon tea. Furtherdetails andregistration forms can be obtained from:
The General Secretary
British Institute of Radiology
32 Welbeck Street
London W1M 7PG, United Kingdom
Attendance may be limited and registrations will be accepted in the order they are received.
J
Volume 17, Number 9 835
INTERNATIONALSYMPOSIUM ON MEDICAL RADIONUCLIDE IMAGING
SYMPOSIUM ON RADIOISOTOPES IN CARDIOLOGY
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from
1976;17:826-835.J Nucl Med. James S. Robertson and Colum A. Gorman HyperthyroidismGonadal Radiation Dose and its Genetic Significance in Radioiodine Therapy of
http://jnm.snmjournals.org/content/17/9/826This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1976 SNMMI; all rights reserved.
by on July 1, 2018. For personal use only. jnm.snmjournals.org Downloaded from



![leg.wa.govleg.wa.gov/CodeReviser/WACArchive/Documents/2012/WAC-296-826... · (2/17/09) [Ch. 296-826 WAC—p. 1] Chapter 296-826 Chapter 296-826 WAC ANHYDROUS AMMONIA WAC 296-826-100](https://img.pdfslide.net/doc/110x75/5b2b78217f8b9ae6278b475f/legwa-21709-ch-296-826-wacp-1-chapter-296-826-chapter-296-826-wac.jpg)