Embed Size (px)
Citation preview

Joan AlbanellServicio de Oncología Médica
Implicaciones clínicas de los subtipos intrínsecos de cáncer de mama

The intrinsic breast cancer subtypes
PAM50: intrinsic subtypes and ROR
Studies in Hormone Receptor positive disease
Studies in HER2 positive disease
Studies in Triple Negative disease
Summary

Molecular classification in breast cancer:The intrinsec subtypes
Sorlie, T et al. PNAS, 2001Perou, CM et al. Nature, 2000Perreard, L et al. Breast Cancer Res, 2006

Breast cancer intrinsic subtypes vary in subsets defined by ER and HER2
Prat, A & Perou, CM. Mol Oncol 2011

IHC-based definition of Luminal A is ER+ and/or PR+HER2-Ki67<14%PR>20%
IHC-based definition of Luminal B is ER+ and/or PR+ / HER2- / Ki67<14% / PR<20%orER+ and/or PR+ / HER2- / Ki67>14% or ER+ and/or PR+ / HER2+
IHC-based definition ofLuminal A versus Luminal B tumors
However, these definitions 1) do not fully recapitulate the intrinsic subtypes and 2) are technically challenging (i.e. precise scoring
of Ki-67 and PgR), and thus the Pathology Community needs to establish scoring standards and provide controls
Prat et al. J Clin Oncol 2013
Survival analyses within IHC-LumA tumors

The intrinsic breast cancer subtypes
PAM50: intrinsic subtypes and ROR
Studies in Hormone Receptor positive disease
Studies in HER2 positive disease
Studies in Triple Negative disease
Summary

Extract RNA from FFPE tumor sample
Run RNA & CodeSet on nCounter Analysis System
Intrinsic Subtype
Risk of Relapse (ROR)
RESEARCH
DIAGNOSTICS
FDA 510(k)
Prosigna test (PAM50)
Adapted from Aleix Prat

1. The qRT-PCR assay consists of 50 genes
2. The subtype classification accuracy of the 50 genes by qRT-PCR versus 2000 genes by microarray was 93%
3. The assay works using RNA from FFPE materials or fresh frozen tissues.
PAM50 Using nCounter Classifies Breast CancerInto Intrinsic Subtypes
Parker J Clin Oncol 2009

PAM50 Generates a Risk Of Relapse (ROR) Score Specific to Each Patient
• ROR is based on the similarity of the gene expression profile to intrinsic subtypes, proliferation score (i.e. mean expression prolif-related genes), nodes and tumor size.
• ROR ranges from 0 through 100 (ROR) indicating the probability of distant recurrence in a “training cohort” of patients with tumors representing all subtypes and patients that did not receive any adjuvant systemic therapy.
Patient expression
profile Lum
B
Lum
A
Basa
l-like
HER2
-enr
iched
PAM50 centroids
ROR = aRLumA+
bRLumB+
cRHer2e+
dRBasal+
eP+
fT
Pearson’s correlation to centroids
Proliferation scoreTumor size
Parker et al. JCO 2009; Nielsen et al. CCR 2010


The intrinsic breast cancer subtypes
PAM50: intrinsic subtypes and ROR
Studies in Hormone Receptor positive disease
Studies in HER2 positive disease
Studies in Triple Negative disease
Summary

ATAC studyPostmenopausal
women with invasive BC (N=9366)
Tam alone (N=3116)
Arimidex alone (N=3125)
Tam + Arimidex (N = 3125)
TransATAC study (N=1125 blocks)
ABCSG-8 studyPost-menopausal women with HR+
BC (N=3714)
Tamoxifen(N=1849)
Anastrozole (N=1865)
ABCSG-8 study (N = 1478 blocks)
Tam2-years 3 years
PAM50 (PROSIGNA®) Validation Studies
Primary Objective: Validate published observations that Prosigna/ROR Score provides additional prognostic information over and above standard clinical variables for DRFS at 10 yrs- Primary Analysis: All patients- Secondary Analysis: Node-
negative, node-positive, and HER2-negative patients
Secondary Objective: Validate observations that Luminal A and Luminal B patients have statistically significantly different DRFS at 10 yrs1

Findings From the Combined Analysis of >2400 Patient Samples
DRFS by Risk-Group for Node-negative Patients
DRFS by Risk-Group for Node-positive Patients (1-3 positive nodes)
1.0
0.9
0.8
0.7
0.6
1.0
0.9
0.8
0.7
0.60 2 4 6 810
Follow-Up Time (yrs)
Perc
ent W
ithou
t Dist
ance
Rec
urre
nce
Low-riskIntermediate-riskHigh-risk
0 2 4 68 10 Follow-Up Time (yrs)
Perc
ent W
ithou
t Dist
ance
Rec
urre
nce
Low-riskIntermediate-riskHigh-risk
1.0
0.9
0.8
0.7
0.6
1.0
0.9
0.8
0.7
0.6
Risk Group N (%) EventsThrough 10 Yrs
% Without Recurrence at 10 yrs [95% CI]
Low 875 (49%) 31 96%.2 [94.7% - 97.3%]
Intermediate
551 (31%) 53 89.2% [86.%1 - 91.7%]
High 360 (20%) 73 77.7% [72.8% - 81.95%]
Total 1,786 (100%)
157
Risk Group N (%) EventsThrough 10 yrs
% Without Recurrence at 10 yrs [95% CI]
Low 24 (4%) 2 91.7% [70.6% - 97.8%]
Intermediate
211 (36%) 18 90.4% [85.2% - 93.9%]
High 355 (60%) 87 71.8% [66.3% - 76.6%]
Total 590 (100%)
107
Prosigna Low Risk patients
remain Low Risk over
10yrs
Source: Dowsett M, Sestak I, Lopez-Knowles E, et al. Comparison of PAM50 risk of recurrence score with Oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine therapy. J Clin Oncol. 2013;31(22):2783-2790: Gnant M, Filipits M, Greil R, et al; Austrian Breast and Colorectal Cancer Study Group. Predicting distant recurrence in receptor-positive breast cancer patients with limited clinicopathological risk: using the PAM50 Risk of Recurrence score in 1478 postmenopausal patients of the ABCSG-8 trial treated with adjuvant endocrine therapy alone. Ann Oncol. 2014;25(2):339-345.

Knowledge of Luminal Status May Improve Disease Management
DRFS by Risk-Group for Node-Negative Patients
Risk Group N (%)
EventsThrough 10
yrs
% Without Recurrence at 10
yrs [95% CI]
Luminal A
1254 62 94.6% [93.1% – 95.8%]
Luminal B
460 75 81.9% [77.7% – 85.3%]
Total 1,714 137
Risk Group N (%)
EventsThrough 10
yrs
% Without Recurrence at 10
yrs [95% CI]
Luminal A
375 41 87.6% [83.5% – 90.8%]
Luminal B
186 52 68.3% [60.4% – 75.0%]
Total 561 93
DRFS by Risk-Group for Node-Positive Patients
(1-3 Positive Nodes)
Source: Dowsett M, Sestak I, Lopez-Knowles E, et al. Comparison of PAM50 risk of recurrence score with Oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine therapy. J Clin Oncol. 2013;31(22):2783-2790: Gnant M, Filipits M, Greil R, et al; Austrian Breast and Colorectal Cancer Study Group. Predicting distant recurrence in receptor-positive breast cancer patients with limited clinicopathological risk: using the PAM50 Risk of Recurrence score in 1478 postmenopausal patients of the ABCSG-8 trial treated with adjuvant endocrine therapy alone. Ann Oncol. 2014;25(2):339-345.

JCO 2013
• Discordance between ROR and RS groups of 43% at the
individual level

Prospective study of the impact of the Prosigna® assay on adjuvant clinical decision-making in an unselected population of women with ER+, HER2-negative, node-negative breast cancer: a GEICAM study

JNCI 2013
• TransATAC study• OncotypeDX RS, PAM50 ROR and IHC4 (Ki67, PgR, ER, HER2 status)

Ivana Sestak
Jack Cuzick, Mitch Dowsett, Martin Filipits, Peter Dubsky, J. Wayne Cowens, Sean Ferree, Carl Schaper, Christian Fesl, Michael Gnant
Centre for Cancer Prevention, Wolfson Institute of Prevention Medicine, Queen Mary University, London, UK Academic Department of Biochemistry, Royal Marsden Hospital, London, UK
Austrian Breast and Colorectal Cancer Study Group, Vienna, AustriaDepartment of Surgery and Comprehensive Cancer Centre, Medical University of Vienna, Vienna, Austria
NanoString Technologies, Seattle, WA, USAMyRAQA, Redwood Shores, CA, USA
San Antonio Breast Cancer – Cancer Therapy and Research Center at UT Health Science Center – December 10-14, 2013
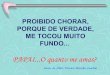
Prediction of late distant recurrence after 5 years of
endocrine treatment: A combined analysis of 2137 patients from the ABCSG-8
and transATAC studies using the PAM50 Risk of Recurrence (ROR) score

Luminal A vs Luminal BHR (95% CI) P-value
Luminal A (N=1530 (71.6%)) - -
Luminal B (N=542 (25.4%)) 2.89 (2.07- 4.02) <0.0001
San Antonio Breast Cancer – Cancer Therapy and Research Center at UT Health Science Center – December 10-14, 2013
Sestak et al. SABCS 2013 and JCO 2014
05
10
15
5 6 7 8 9 10
Follow-up time [years]
Luminal B
Luminal A
Dis
tan
t re
curr
en
ce (
%)
4.1%
12.9%
05
10
15

San Antonio Breast Cancer – Cancer Therapy and Research Center at UT Health Science Center – December 10-14, 2013
Risk groups – ROR score (N=2137)HR (95% CI)
Low (N=1183 (55.4%)) -
Intermediate (N=538 (25.2%)) 3.26 (2.07-5.13)
High (N=416 (19.5%)) 6.90 (4.54-10.47)
2.4%
16.6%
8.3%
05
1015
20
5 6 7 8 9 10Follow-up time [years]
LowIntermediateHigh
Dis
tant
rec
urre
nce
(%)
05
1015
20
Sestak et al. SABCS 2013

The intrinsic breast cancer subtypes
PAM50: intrinsic subtypes and ROR
Studies in Hormone Receptor positive disease
Studies in HER2 positive disease
Studies in Triple Negative disease
Summary

The HER2-enriched subtype is associated wit higher responses and improved survival outcomes in
HER2+ breast cancer in the NOAH study
• Chemotherapy: AT x 3 T x 4 CMF x 3
• 156 (46.7%) pre-treatment samples were PAM50 profiled.
HER2+ HER2+/HR-
Prat et al. Clin Cancer Res 2014Note: interaction test between HER2E subtype and treatment was not statistically significant.
pCR Odds Ratio P-value
HER2+/HER2-E
No-trastuzumab (n=29) 27.6%
Trastuzumab (n=34) 52.9%
HER2+/nonHER2-E
No-trastuzumab (n=22) 18.2%
Trastuzumab (n=29) 34.5%
HER2+/HR-/HER2-E
No-trastuzumab (n=28) 25.0%
Trastuzumab (n=27) 63.0%
HER2+/HR-/nonHER2-E
No-trastuzumab (n=9) 11.1%
Trastuzumab (n=16) 31.3%
0.002
2.4 0.582
Subtype
5.1 0.009
2.1 0.352
8.7
RESPONSE


The intrinsic breast cancer subtypes
PAM50: intrinsic subtypes and ROR
Studies in Hormone Receptor positive disease
Studies in HER2 positive disease
Studies in Triple Negative disease
Summary

Prat et al. BJC 2014



Summary
• The PAM50 assay provides better intrinsic subtype molecular (Luminal A and B, HER2-enriched and Basal-like) classification than current pathology-based surrogate definitions.
• PAM50 ROR provides robust prognostic information in ER+/HER2- early breast cancer and influenced systemic treatment recommendations in a prospective clinical impact study.
• PAM50 ROR and classification of luminal A vs B tumors may also help to estimate the risk of late recurrences (> 5 years) in ER+ disease.
• HER2+ disease includes all the intrinsic subtypes (i.e. not just Luminal B and HER2-enriched). HER2+enriched tumors appear to benefit the most from anti-HER2 treatments in combination with chemotherapy in the neoadjuvant setting. The role of HER2+ subtyping may vary by disease burden (neoadjuvant, micrometastasis, overt metastasis) and type of regimen.
• Within TNBC, distinguishing Basal-like vs. Other subtypes predicted benefit from chemotherapy and docetaxel vs. carboplatin benefit.