Embed Size (px)
Citation preview

Joan B SorianoFISIB-IdISPa, Hospital Universitari Son Espases
Infradiagnóstico en EPOC: ¿cómo podemos mejorarlo?
I have the following disclosures that relate or not to this presentation: - JBS received pharmaceutical company grants from GSK in 2011 and Chiesi
in 2012 via CIMERA his home institution- JBS participated in speaking activities during the period 2010-2014
sponsored by: -Almirall- AstraZeneca- Boehringer-Ingelheim - Chiesi - Grifols- GSK - Novartis - Pfizer- and Rovi
- JBS is Director of Foreign Affairs (COMRI) of SEPAR
Conflict of interest disclosures of Joan B Soriano
I declare I have no, real or perceived, conflicts of interest that relate to this presentation.

Bilbao, 7 de junio de 2014

1. International Agency for Research on Cancer (IARC), Lyon, France;2. INSERM, Centre for research in Epidemiology and Population Health (CESP), U1018, Environmental epidemiology of cancer Team, F-94807, Villejuif, France;3. Université Paris-Sud, UMRS 1018, F-94807, Villejuif, France;4. Institute for Medical Informatics, Biometry and Epidemiology, University of Duisburg-Essen, Essen, Germany;5. Department of Population Health Research, Cancer Control Alberta, Alberta Health Services, Calgary, Canada6. Department of Clinical Sciences and Community Health, Università degli Studi di Milano, Milan, Italy;7. National Heart & Lung Institute, Respiratory Epidemiology, Occupational Medicine and Public Health, Imperial College London, London, UK;8. The Tisch Cancer Institute and Institute for Translational Epidemiology, Mount Sinai School of Medicine, New York, USA;9. Institut für Epidemiologie, Deutsches Forschungszentrum fur Gesundheit und Umwelt, Neuherberg, Germany;10. National Cancer Institute, Bethesda, USA;11. University of Montreal Hospital Research Center (CRCHUM), Montreal, Canada;12. Bremen Institute for Prevention Research and Social Medicine, Bremen, Germany;13. Russian Cancer Research Centre, Moscow, Russia;14. Roy Castle Lung Cancer Research Programme, Cancer Research Centre, University of Liverpool, Liverpool, UK;15. Samuel Lunenfeld Research Institute, Toronto, Canada;16. Occupational Cancer Research Centre, Cancer Care Ontario, Toronto, Canada;17. The Nofer Institute of Occupational Medicine, Lodz, Poland;18. The M Sklodowska-Curie Cancer Center and Institute of Oncology, Warsaw, Poland;19. National Institute of Environment Health, Budapest, Hungary;20. Regional Authority of Public Health, Banska Bystrica, Slovakia;21. Institute of Public Health, Bucharest, Romania;22. Institute of Hygiene and Epidemiology, 1st Faculty of Medicine, Charles University, Prague, Czech Republic;23. Masaryk Memorial Cancer Institute, Brno, Czech Republic;24. Palacky University, Faculty of Medicine, Olomouc, Czech Republic;25. Institute for Prevention and Occupational Medicine of the German Social Accident Insurance – Institute of the Ruhr-Universität Bochum (IPA), Germany;26. Institute for Risk Assessment Sciences, Utrecht, the Netherlands;27. Occupational Respiratory Epidemiology, School of Population Health, University of Western Australia, Perth, Australia.28. The Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden;
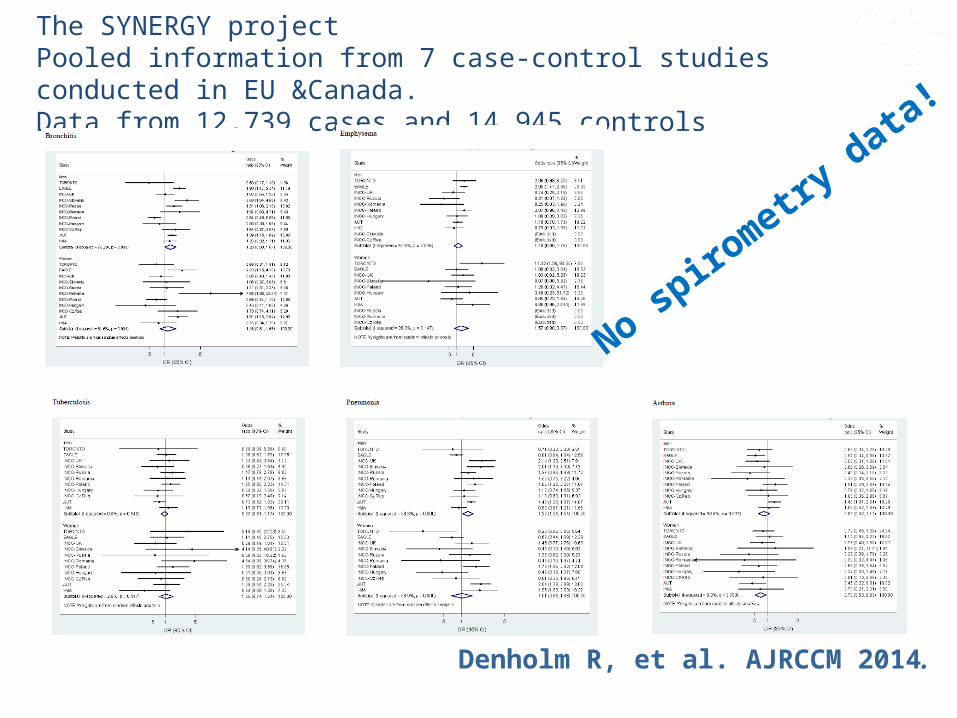
Denholm R, et al. AJRCCM 2014.
Denholm R, et al. AJRCCM 2014.
The SYNERGY projectPooled information from 7 case-control studies conducted in EU &Canada.Data from 12,739 cases and 14,945 controls
No spirometry
data!

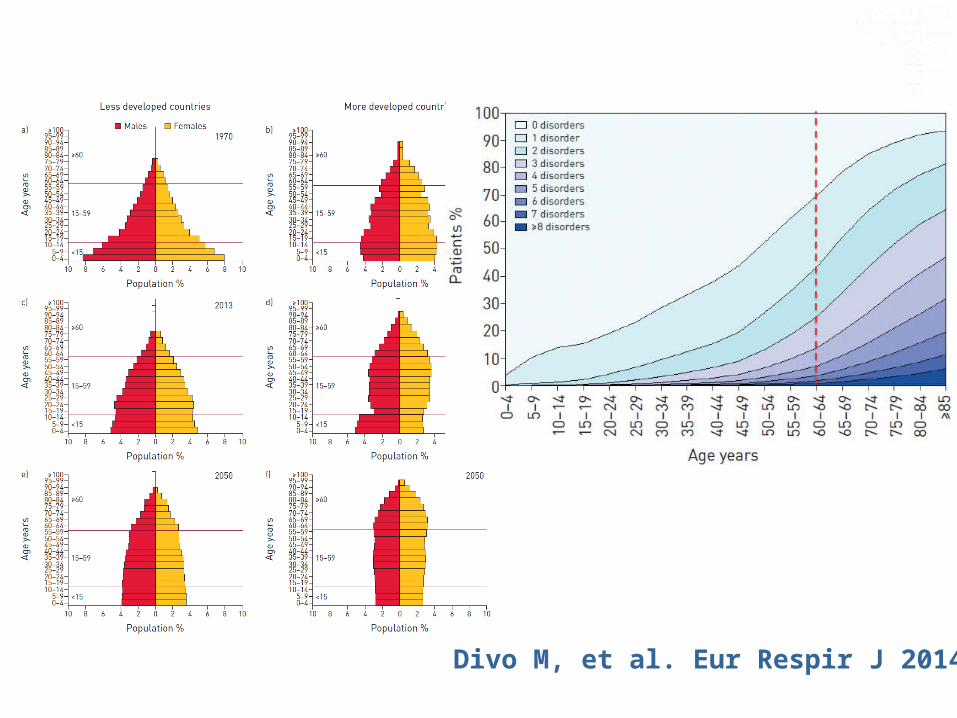
Divo M, et al. Eur Respir J 2014.
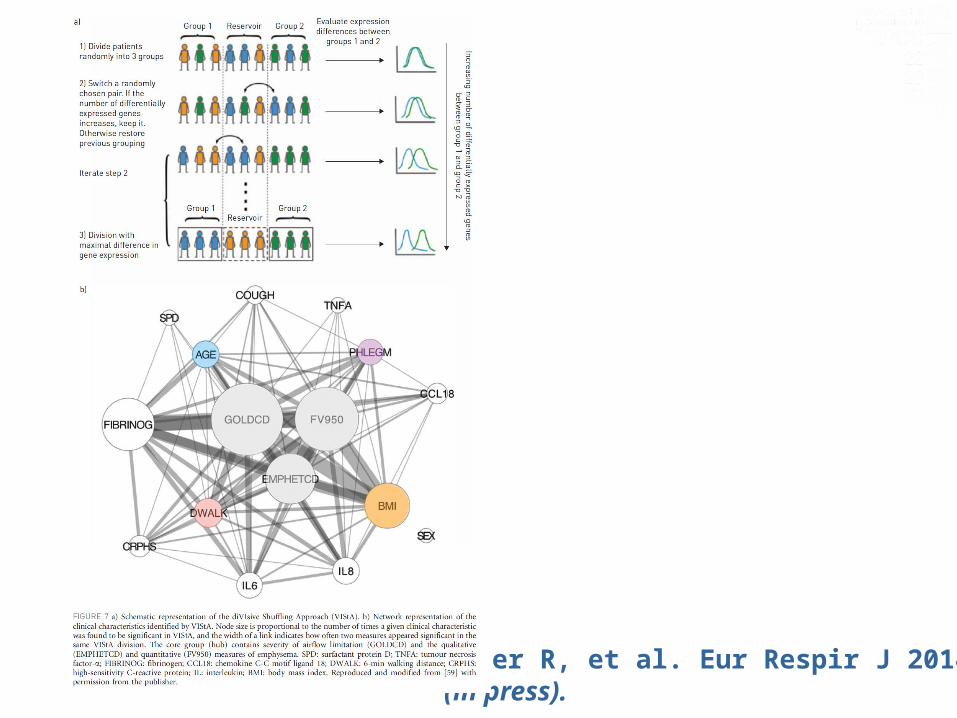
Faner R, et al. Eur Respir J 2014(in press).
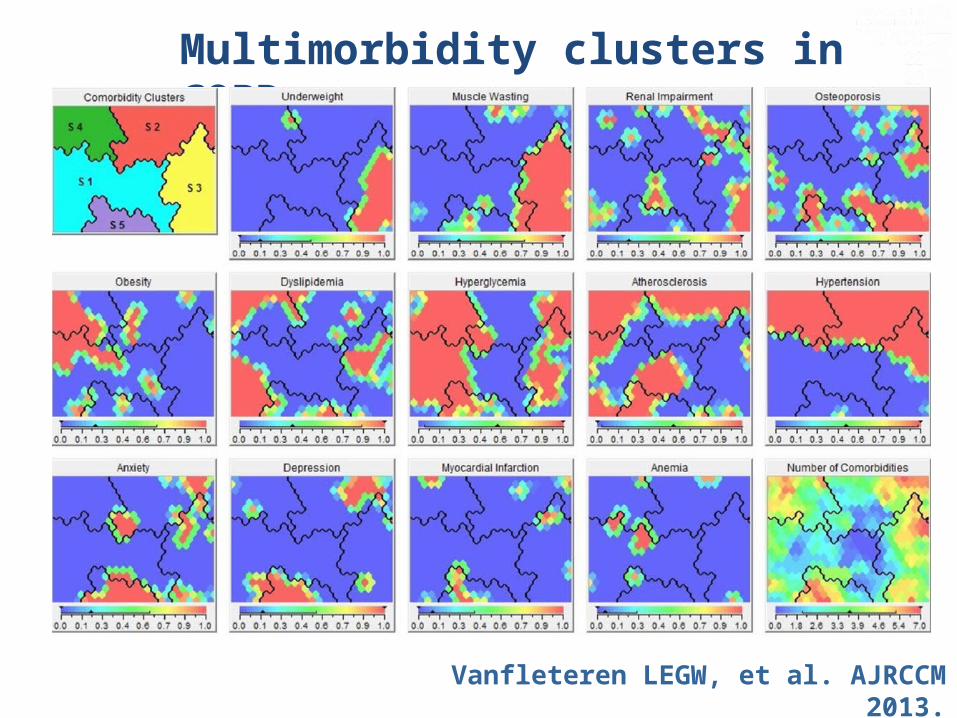
Multimorbidity clusters in COPD
Vanfleteren LEGW, et al. AJRCCM 2013.

Published COPD surveys, per year
105 prevalence estimates
Corresponding to 78 studies in 50 years
Soriano JB, Rodriguez-Roisin R. PATS 2011.
• “… To date, for COPD, such evidence is absent for general population improvements in lung function, reductions in exacerbations, or other disease outcomes and endpoints.”
Soriano JB, Zielinski J, Price D. Lancet 2009.
• “… Ongoing contentious issues in COPD research include definition and staging of the disorder. No consensus exists on how, when, and where spirometry and other methods should be implemented to screen for the disease, if at all..”

The iceberg phenomenon leads to …
the “clinician’s fallacy”
“… an inaccurate view of the nature and causes of a disease results from studying the minority of cases of the disease that are seen in clinical treatment .”
Duncan, D. F. (1988). Epidemiology: Basis for Disease Prevention and Health Promotion. New York: MacMillan.

Rate of underdiagnosis of COPD
Soriano JB, Zielinski J, Price D. Lancet 2009.
P > 0.05
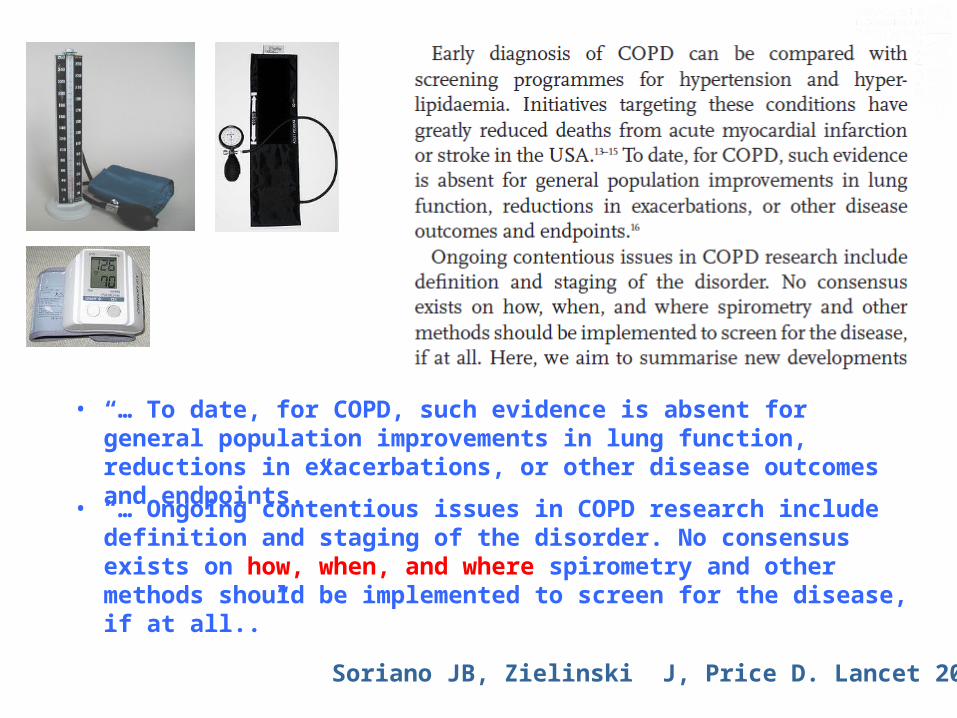
Any Changes/Improvements in COPD Underdiagnosis at the population level?
Govern Balear Govern Balear
Vizcaya8,2%
OVIEDO6,1%
BURGOS10,3%
MADRID9,8%
CACERES4,9%
SEVILLA6,3%
MANLLEU18%
IBERPOC 1997IBERPOC 1997
In Spain 1.228.000 people 40 to 69 years suffered COPD78% were yet undiagnosed
PREVALENCE GLOBAL: 9,1%
40 to 69 years
MALE 14,3%MALE 14,3%(12,8(12,8--15,9) 15,9)
FEMALE 3,9%FEMALE 3,9%(3,09(3,09--4,81)4,81)
Sobradillo-Peña V, et al. Chest 2000;118:981
Govern Balear Govern Balear
Vizcaya8,2%
OVIEDO16,9%
BURGOS6,2%
MADRID13,7% and 8,3%
SEVILLA8,1%
BARCELONA14,8%
EPIEPI--SCAN 2007SCAN 2007 PREVALENCE GLOBAL: 10,2%
40 to 80 years
MALE 15,1%MALE 15,1%(13,5(13,5--16,8) 16,8)
FEMALE 5,7%FEMALE 5,7%(4,7(4,7--6,7)6,7)
Miravitlles M, et al. Thorax 2009 (in press).
CORDOBA12,4%
HUESCA11,0%
REQUENA9,9%
VIC9,0%
VIGO8,2%
78% in 1997 (IBERPOC) to 73% in 2007 (EPI-SCAN)

The Finnish Action Programme:
Pietinalho A, et al. Respir Med 2007.
Kinnula VL, et al. Prim Care Respir J 2011.
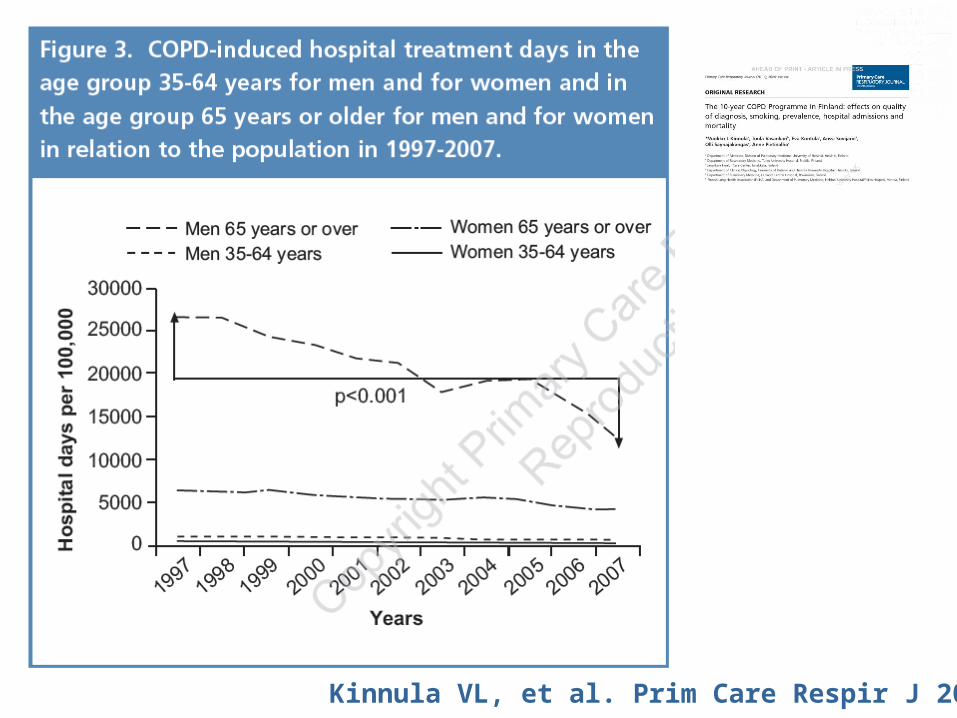
• Taxa d'hospitalitzacions per MPOC va baixar un 39.7%
• Els costos totals d'hospitalització per MPOC van baixar un 88%
• Es va reduïr el tabaquisme …
Kinnula VL, et al. Prim Care Respir J 2011.
Bize R, et al. Cochrane Database Syst Rev 2012.
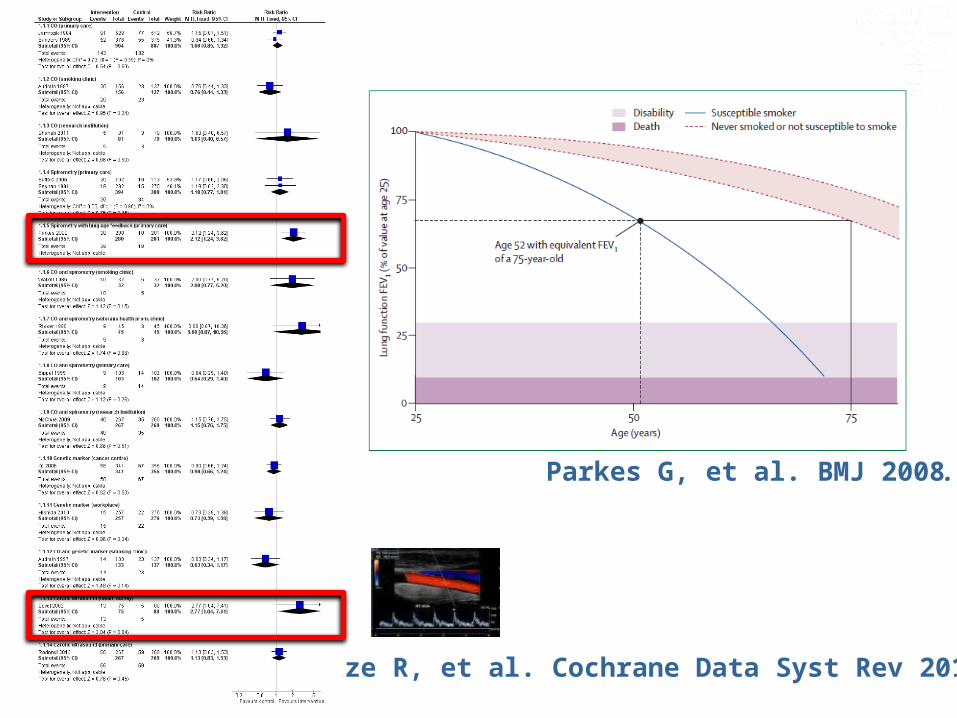
Bize R, et al. Cochrane Data Syst Rev 2012.
Parkes G, et al. BMJ 2008.
Examples in other medical fields: • Mamography and breast
cancer
• PSA and prostate cancer
• CT scan lung cancer
Why is COPD different?
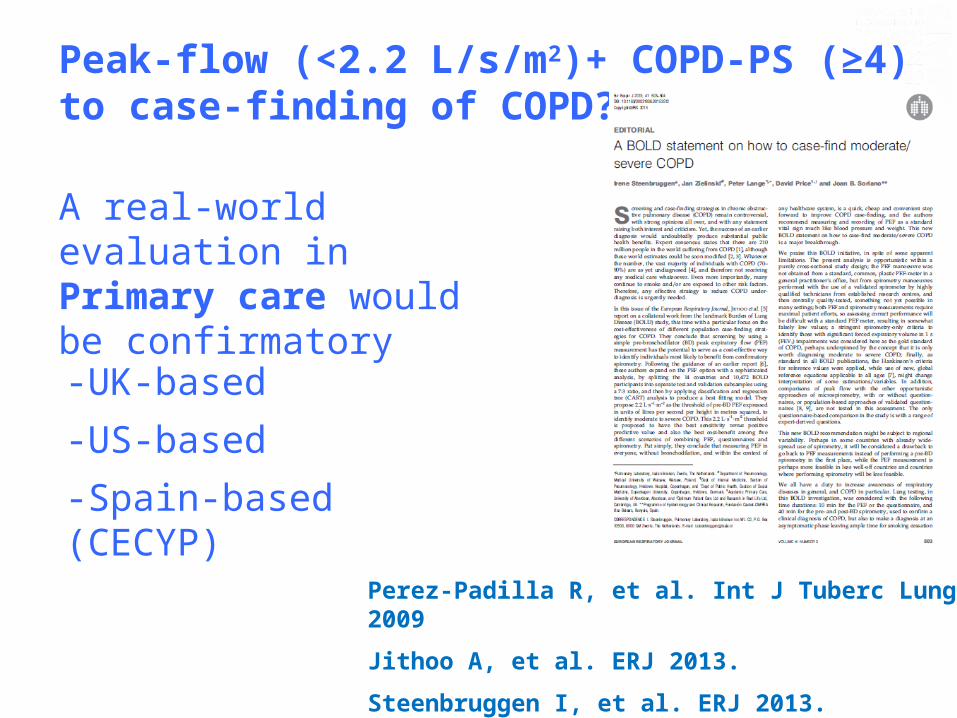
Peak-flow (<2.2 L/s/m2)+ COPD-PS (≥4)to case-finding of COPD?
Perez-Padilla R, et al. Int J Tuberc Lung Dis 2009
Jithoo A, et al. ERJ 2013.
Steenbruggen I, et al. ERJ 2013.
A real-world evaluation in Primary care would be confirmatory
-UK-based
-US-based
-Spain-based (CECYP)
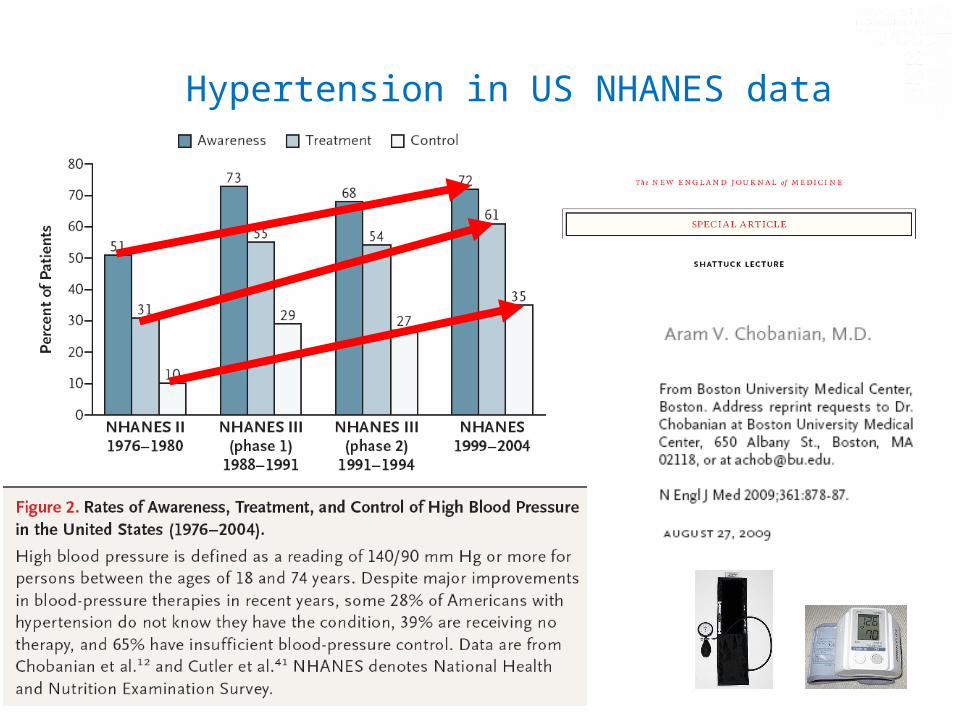
Hypertension in US NHANES data

Spirometer vs. Sphygmomanometer
COPD vs. Hypertension
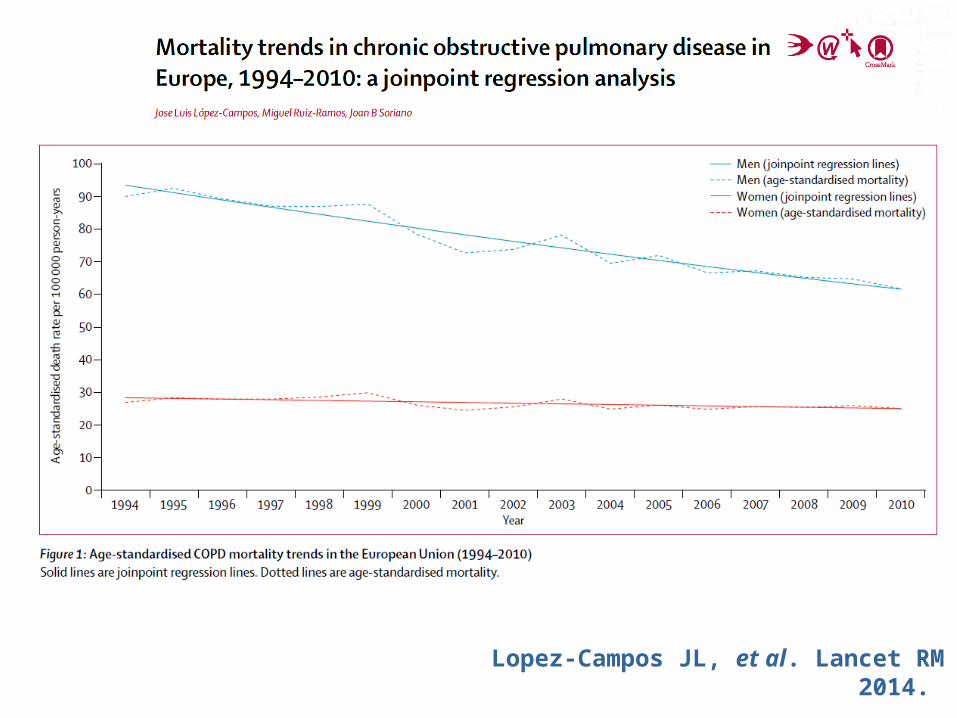
Lopez-Campos JL, et al. Lancet RM 2014.
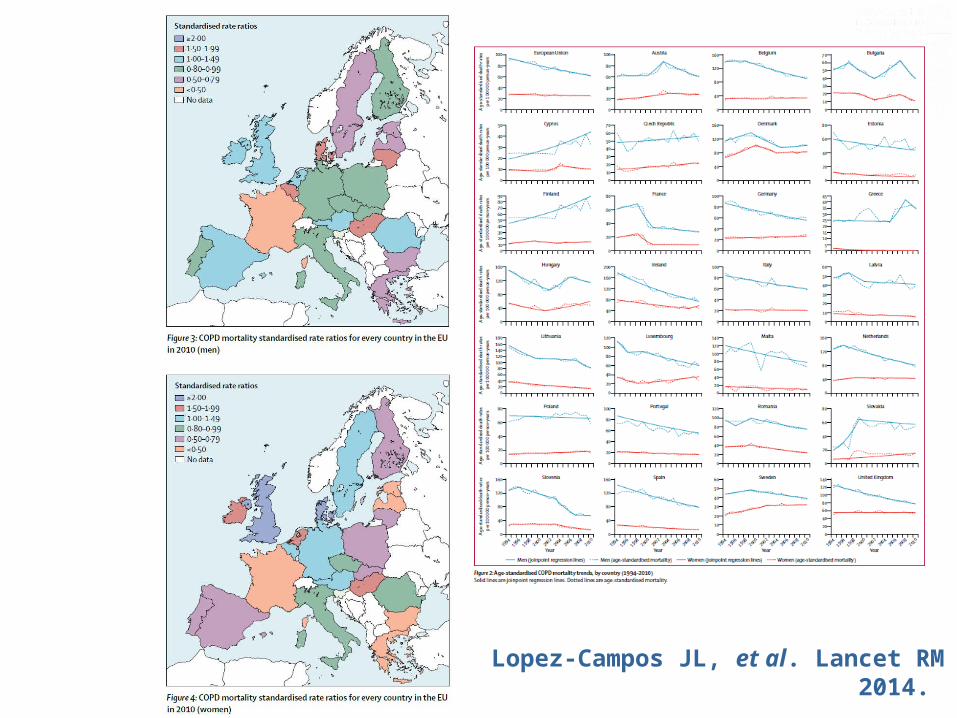
Lopez-Campos JL, et al. Lancet RM 2014.

° El infradiagnóstico de la EPOC es universalmente elevado
° Una gran diversidad de opciones de cribado y detección de casos ya están disponibles: cuándo, dónde y cómo
° Una mayor implementación de la espirometría de calidad podría / debería ayudar a reducir la carga de enfermedad futura de la EPOC.
CONCLUSIONES
SOLUCIONES° !La Persistencia Paga! ° Mantenimiento/ Solicitud/
Interpretación de la espirometría de alta calidad° ¿Cómo ?: herramientas y técnicos
capacitados y validados ° ¿Cuándo?: todos los días ° ¿Dónde?: siempre que sea posible





























