Embed Size (px)
Citation preview
Joana Ramalho1,2
Renato Hoffmann Nunes1,3
Mauricio Castillo1
1University of North Carolina, Chapel Hill, NC 2Centro Hospitalar de Lisboa Central, Lisbon, Portugal
3Santa Casa de Misericórdia de São Paulo, Brazil
eEdE-235
The authors have no disclosures.
Review the clinical presentations, pathophysiologic mechanisms & magnetic resonance imaging findings of myelopathies that have underlying metabolic and/or toxic etiologies.
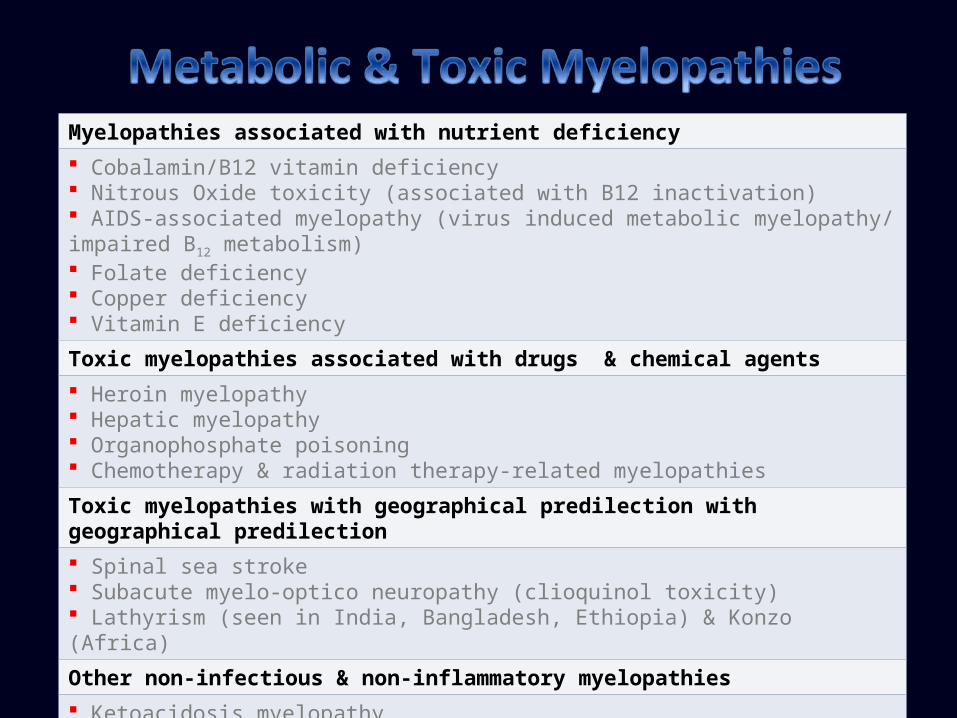
Myelopathies associated with nutrient deficiency Cobalamin/B12 vitamin deficiency Nitrous Oxide toxicity (associated with B12 inactivation) AIDS-associated myelopathy (virus induced metabolic myelopathy/ impaired B12 metabolism) Folate deficiency Copper deficiency Vitamin E deficiency
Toxic myelopathies associated with drugs & chemical agents Heroin myelopathy Hepatic myelopathy Organophosphate poisoning Chemotherapy & radiation therapy-related myelopathies
Toxic myelopathies with geographical predilection with geographical predilection Spinal sea stroke Subacute myelo-optico neuropathy (clioquinol toxicity) Lathyrism (seen in India, Bangladesh, Ethiopia) & Konzo (Africa)
Other non-infectious & non-inflammatory myelopathies Ketoacidosis myelopathy Spinal cord decompression illness Surfer’s myelopathy
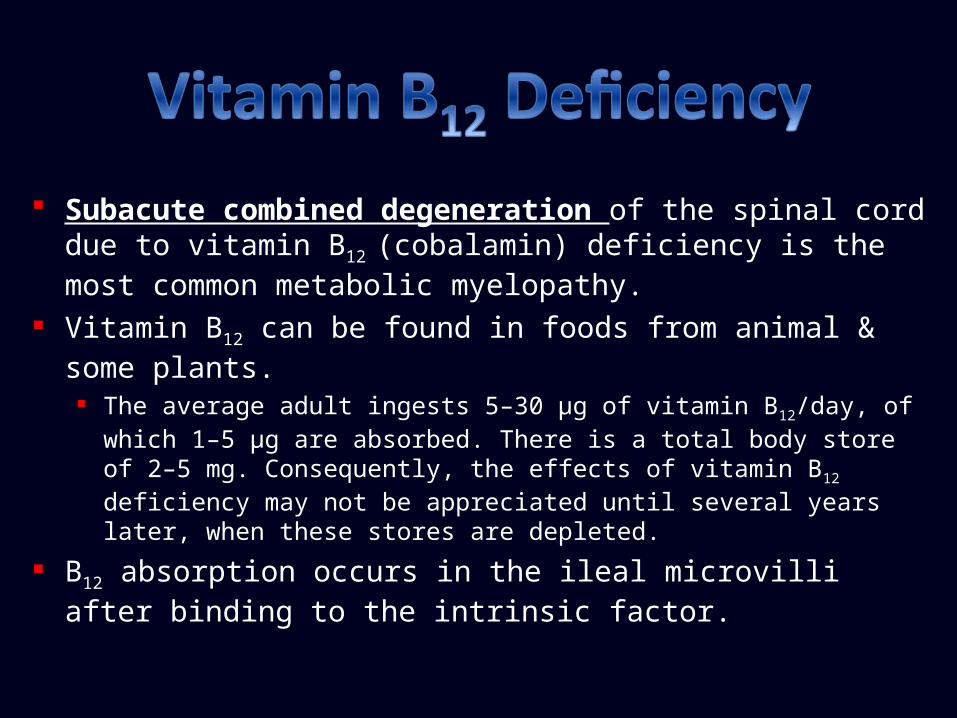
Subacute combined degeneration of the spinal cord due to vitamin B12 (cobalamin) deficiency is the most common metabolic myelopathy.
Vitamin B12 can be found in foods from animal & some plants. The average adult ingests 5–30 μg of vitamin B12/day, of which 1–5 μg are
absorbed. There is a total body store of 2–5 mg. Consequently, the effects of vitamin B12 deficiency may not be appreciated until several years later, when these stores are depleted.
B12 absorption occurs in the ileal microvilli after binding to the intrinsic factor.
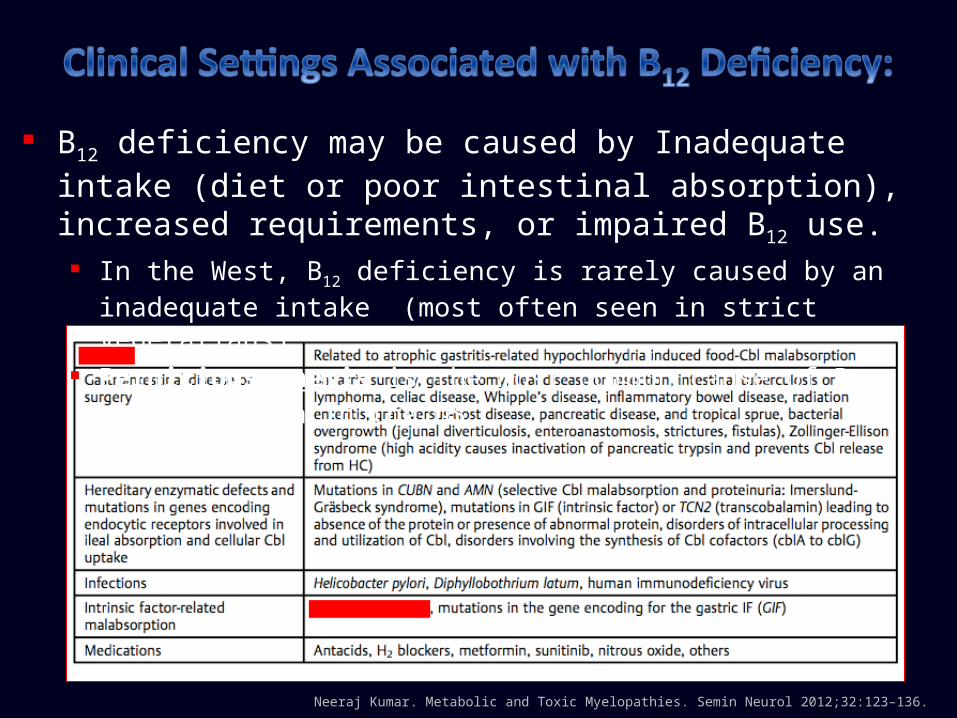
Neeraj Kumar. Metabolic and Toxic Myelopathies. Semin Neurol 2012;32:123–136.
B12 deficiency may be caused by Inadequate intake (diet or poor intestinal absorption), increased requirements, or impaired B12 use. In the West, B12 deficiency is rarely caused by an inadequate intake (most
often seen in strict vegetarians). Pernicious anemia is the most common cause of B12 malabsorption in the US.
Vitamin B12 is a required coenzyme for methylation of homocysteine into methionine & tetrahydrofolate:
Tetrahydrofolate is necessary for normal DNA synthesis. Methionine is converted to S-adenosylmethionine which is necessary for
methylation of myelin sheath phospholipids. Failure of this reaction results in elevated levels of methylmalonic acid & reduced myelin basic protein methylation with fragile myelin susceptible to demyelination & vacuolization.
Diagnosis is made by low serum B12 or if the B12 is borderline, by elevated homocysteine & methylmalonic acid. Hematological changes like megaloblastic anemia are not reliable markers.
Clinical manifestations of vitamin B12 deficiency:
Neurologic manifestations (may be the earliest & often the only manifestation of B12 deficiency): Myelopathy (subacute combined degeneration):
Numbness, weakness, & paresthesia of the extremities primarily affects the lower extremities, is often symmetric, & progresses in a distal-to-proximal manner. Later, this myelopathy progresses to unsteady gait, poor coordination, sensory deficits, & bowel or bladder dysfunction. Physical examination: signs of dorsal column involvement include loss of position & vibration sense/ataxia. Lateral column involvement includes spasticity, hyperreflexia, & positive Babinski sign. Involvement of the spinothalamic tracts with sensory level may also be present.
Peripheral neuropathy and/or optic neuropathy may be seen. Psychiatric manifestations
Cognitive impairment. Personality & mood changes with depression & psychosis.
Hematologic manifestations Megaloblastic anemia or megaloblastic marrow changes. Pancytopenia (leukopenia, thrombocytopenia).
Pathology findings: Demyelination involving the dorsal columns, predominately in the lower
cervical & upper thoracic regions which may extend symmetrically in the cranial-caudal directions & into lateral columns. If uncontrolled, it may advance to other long fiber tracts.
Imaging findings: T2 Hyperintensity that involves the dorsal columns.
Axial images: bilateral paired areas of T2 hyperintensity seen as an “inverted V” or “inverted rabbit ears” in the location of the dorsal columns.
Lateral column involvement & enhancement may occur. Cord atrophy is seen in stages. Brain MRI may show confluent areas of abnormal T2 signal intensity in
white matter.
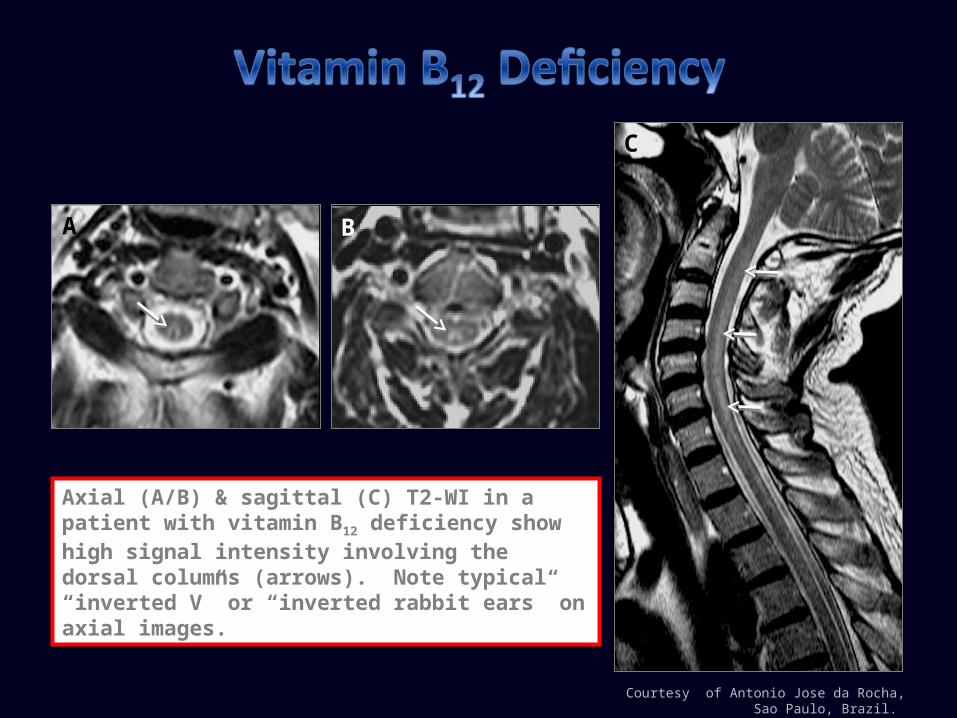
Courtesy of Antonio Jose da Rocha, Sao Paulo, Brazil.
Axial (A/B) & sagittal (C) T2-WI in a patient with vitamin B12 deficiency show high signal intensity involving the dorsal columns (arrows). Note typical “inverted V” or “inverted rabbit ears” on axial images.
A B
C
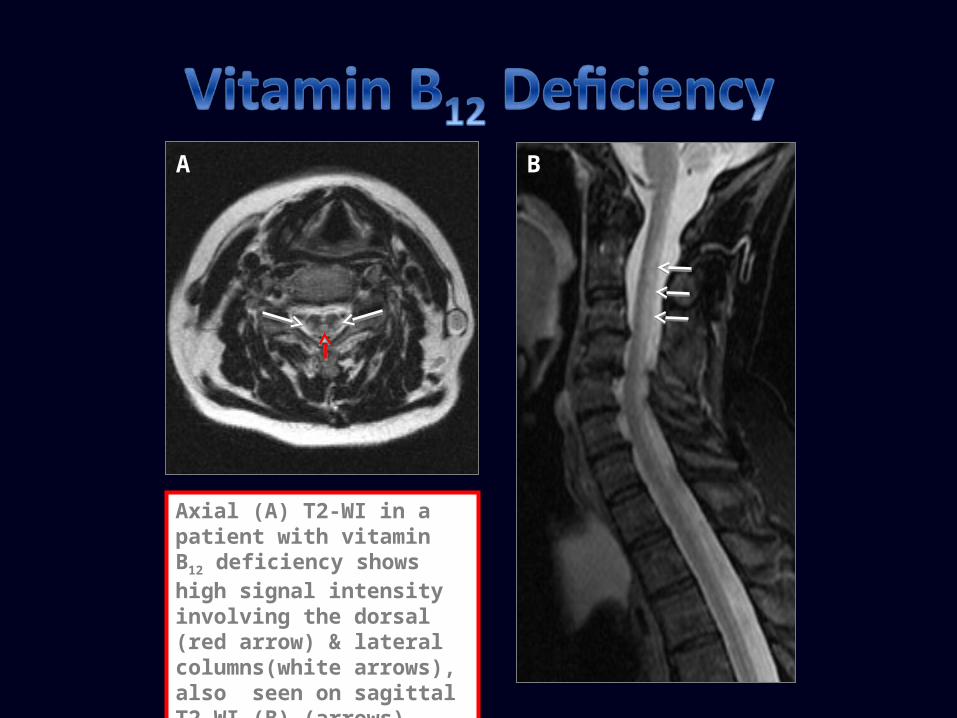
Axial (A) T2-WI in a patient with vitamin B12 deficiency shows high signal intensity involving the dorsal (red arrow) & lateral columns(white arrows), also seen on sagittal T2-WI (B) (arrows).
A B
Prognosis: B12 deficiency is treated with B12 intramuscular injections, continued monthly for life.Spine & brain MRI findings may resolve within a few months after starting therapy. Degree of recovery is inversely proportional to symptom duration/severity & early detection is necessary for full recovery.
Nitrous oxide (N2O or “laughing gas”) is a commonly used inhalational anesthetic agent that is abused because of its euphoriant properties.
N2O irreversibly oxidizes active Vitamin B12 to inactive cobalamin which once inactivated requires 3–4 days to recover.
Healthy individuals have sufficient stores to compensate but there is no reserve in patients with undiagnosed vitamin B12 deficiency.
Myeloneuropathy due to N2O should be considered in patients who develop neurologic symptoms following surgical and/or dental procedures - ‘‘anesthesia paresthetica’’. Signs & symptoms appear relatively rapidly with N2O toxicity but may
be delayed up to 2 months after the acute exposure.
Courtesy of Antonio Jose da Rocha, Sao Paulo, Brazil.
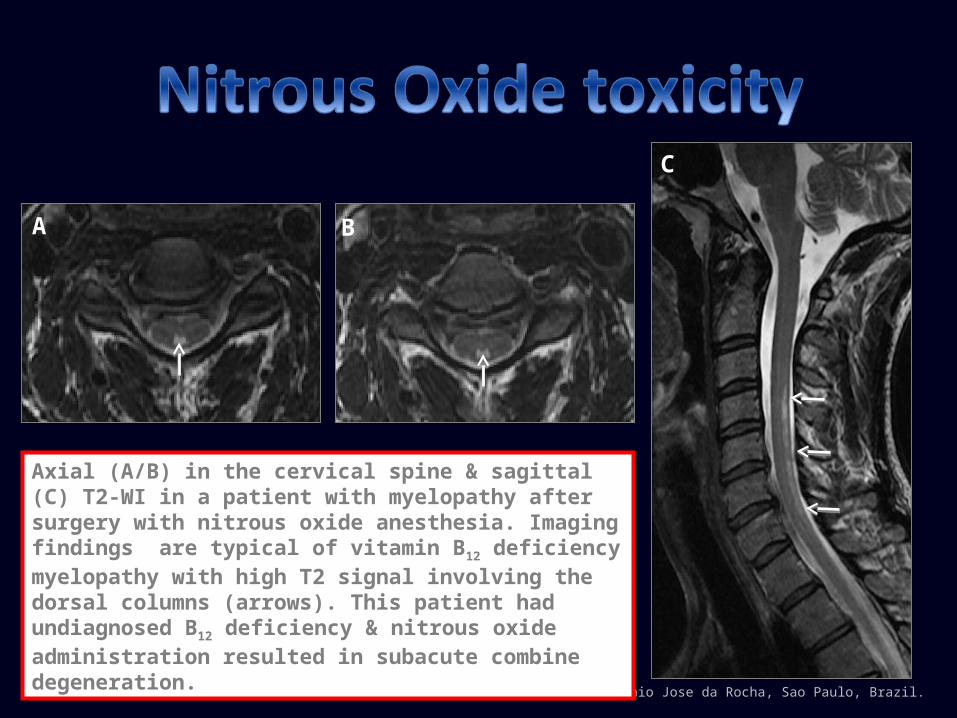
Axial (A/B) in the cervical spine & sagittal (C) T2-WI in a patient with myelopathy after surgery with nitrous oxide anesthesia. Imaging findings are typical of vitamin B12 deficiency myelopathy with high T2 signal involving the dorsal columns (arrows). This patient had undiagnosed B12 deficiency & nitrous oxide administration resulted in subacute combine degeneration.
A B
C
Clinical symptoms, MRI findings & histopathology of AIDS associated myelopathy resembles that of subacute combined degeneration.
The cause of vacuolar myelopathy in these patients is not known: Increased prevalence of B12 deficiency has been recognized in human
immunodeficiency virus (HIV) infected patients with neurologic symptoms, but its precise significance is unclear.
Impairment in methylation pathways related or not to viral infection of the spinal cord has been proposed.
Most common manifestation of folate deficiency is myelopathy or myeloneuropathy resembling subacute combined degeneration seen with B12 deficiency.
As with B12, folate acts as an important cofactor in DNA synthesis & methylation pathways.
Folate is a water-soluble B vitamin present in fresh green vegetables, citrus fruits, legumes, & liver.
Its deficiency results from: Reduced intake of folate-rich products, impaired absorption or increased
folate metabolism (genetic defects). It is commonly associated with alcoholism, gastrointestinal disease, & drugs
such as methotrexate & trimethoprim.
Clinical manifestations of folate deficiency: For unclear reasons, neurologic & hematologic manifestations due to folate deficiency, though similar to those seen with B12 deficiency are rare, mild, & controversial.
Neurologic manifestations (subacute combine degeneration): Myelopathy Peripheral neuropathy Optic neuropathy
Psychiatric manifestations Cognitive or or behavioral manifestations
Hematologic manifestations (not always present) Megaloblastic anemia and/or megaloblastic marrow changes (indistinguishable from the anemia seen in B12 deficiency).
Generally coexists with other nutrient deficiencies. Attribution of neurologic manifestations to pure folate deficiency requires
exclusion of other potential causes.
Diagnosis: Serum folate 2.5 - 5 μg/L - suggests mildly compromised folate status. Erythrocyte folate is more reliable than plasma folate because its levels are
less affected by short-term fluctuations in intake. Homocysteine levels are typically elevated in patients with clinically
significant folate deficiency.
Early diagnosis & treatment is required before neurological manifestations become irreversible.
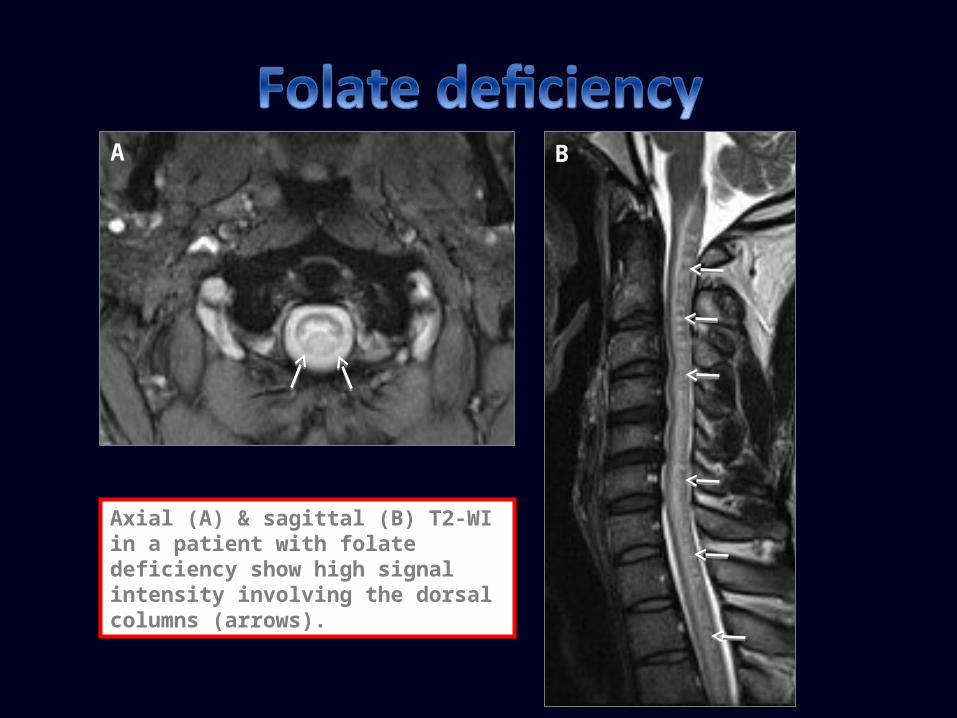
Axial (A) & sagittal (B) T2-WI in a patient with folate deficiency show high signal intensity involving the dorsal columns (arrows).
A B
Acquired Cu deficiency may cause myelopathy or myeloneuropathy that resembles subacute combined degeneration.
Cause of acquired Cu deficiency is often unknown: Acquired dietary Cu deficiency is rare. Most common known cause is history of gastric surgery (may not manifest for
decades). Excess zinc ingestion can also cause Cu deficiency Enteropathies associated with malabsorption like cystic fibrosis, sprue, bacterial
overgrowth, &inflammatory bowel disease have also been reported. Cu &B12 deficiencies may coexist. Diagnosis:
Decrease serum Cu or ceruloplasmin & 24-h urinary Cu excretion. Changes in serum Cu usually parallel ceruloplasmin concentration.
Clinical manifestations of Cu deficiency:
Neurologic & hematologic manifestations are similar to those seen with B12 deficiency:Neurologic manifestations (subacute combine degeneration):
Myelopathy - spastic gait & prominent sensory ataxia. Peripheral neuropathy is common. Optic neuropathy may be present.
Hematologic manifestations (common, but not always present) Anemia & neutropenia (hallmark of Cu deficiency) .
MRI findings: Most common: high T2 signal involving dorsal columns. Cervical cord is most
commonly affected, contrast enhancement is usually not present. Pyramidal tract signal changes, extension to the brainstem & involvement of
lateral columns has been reported. Prognosis:
Cu supplementation resolves anemia/neutropenia promptly & completely; may prevent neurological deterioration.
Recovery of neurological signs/symptoms is variable. Improvement is often subjective & involves sensory symptoms.
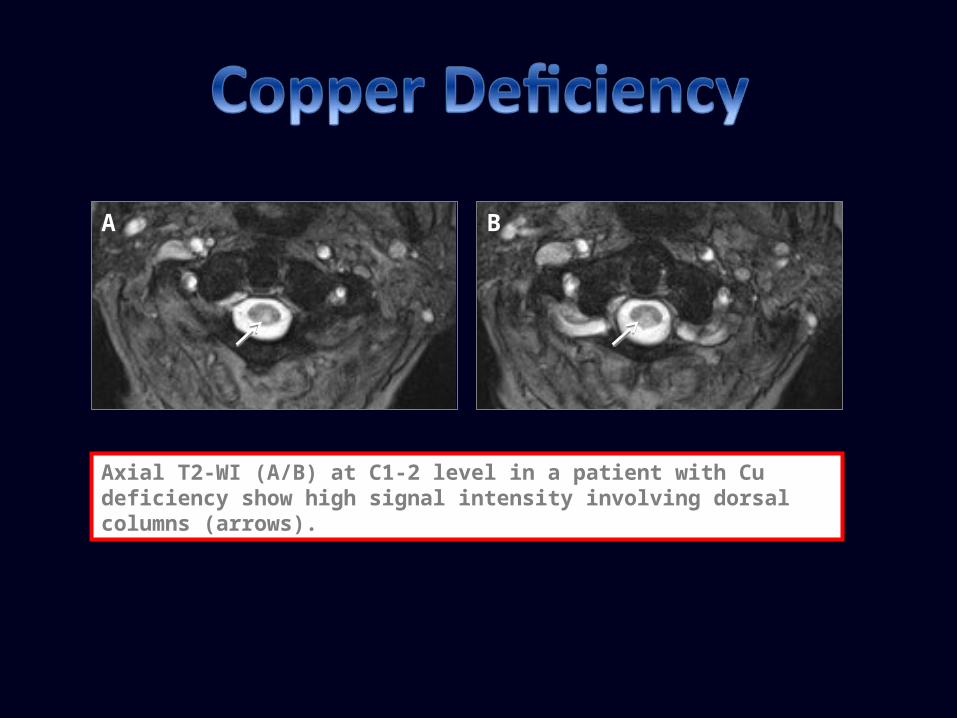
Axial T2-WI (A/B) at C1-2 level in a patient with Cu deficiency show high signal intensity involving dorsal columns (arrows).
A B
Vitamin E is an antioxidant preventing peroxidation of membrane fatty acids.
In adults, is most often associated with malabsorption syndromes (celiac disease, cystic fibrosis, cholestasis) & other intestinal disorders. Diagnosis is based on low serum vitamin E levels frequently
undetectable in patients with neurologic manifestations. Deficiency may also result from genetic defects in
alphatocopherol transfer protein, abetalipoproteinemia, or defects in chylomicron synthesis & secretion. In these cases, genetic testing is necessary.
Vitamin E deficiency may coexist with Cu deficiency.
Clinical manifestations of Vit E deficiency: Neurologic manifestations (subacute combine degeneration):
Progressive spinocerebellar syndrome with corticospinal tract dysfunction & peripheral neuropathy. Dorsal column dysfunction, with loss of position/vibration & ataxia. Pigmented retinopathy, myopathy, movement disorders, & gaze palsies. Phenotype is similar to that of Friedreich’s ataxia.
MRI findings: spinal cord hyperintense T2-WI signal in posterior columns.
Replacement of vitamin E is treatment of choice stopping progression. Improvement of neurologic symptoms/signs in severe cases may not occur.
Acute myelopathy is a recognized complication of heroin abuse by either inhalation of heroin vapor (“chasing the dragon”) or intravenous use.
Pathophysiologic mechanisms: Embolism of adulterants, vasculitis, direct toxicity, or hypersensitivity
reaction. Border-zone infarctions resulting from hypotension related to drug.
MRI show: Cord high T2-WI & FLAIR in posterior & lateral columns. Similar lesions in pontomedullary region & in ventral pons. Cord swelling & gadolinium enhancement resembling transverse myelitis.
Hepatic myelopathy (or portosystemic myelopathy) is a rare complication of chronic liver disease &s associated with cirrhosis and/or extensive portosystemic shunting.
Its hallmark is progressive spastic paraparesis: Sensory disturbances, upper limb involvement, & sphincter dysfunction are minimal
or absent. Preceding portosystemic encephalopathy may occur.
Pathophysiology is unknown but probably related to ammonia or other metabolites bypassing the liver.
There is symmetric demyelination of the lateral corticospinal tracts & less common the ventral pyramidal tracts, posterior columns, & spinocerebellar tracts.
MRI: high pallidal signal on T1-WI & symmetric demyelination of lateral corticospinal tracts, posterior columns & spinocerebellar tracts in the spine.
No particular treatment is effective. Variable results have been reported following liver transplantation.
Organophosphates are components of various pesticides & available in many home settings.
Signs/symptoms of acute toxicity are due to acetylcholinesterase inhibition & resulting muscarinic & nicotinic dysfunctions.
Myelopathic symptoms occur late in the course of the disease. MRI shows spinal cord atrophy in late stages. Measurement of cholinesterase activity in red blood cells
confirms diagnosis. Pralidoxime is the specific antidote & is used in conjunction with
atropine in acute stages.
Chemotherapy agents, such as cisplatin, cladarabine, doxorubicin, vincristine, cytosine arabinoside, & intrathecal methotrexate may cause myelopathy related to the agent itself or to preservatives & diluents used.
Radiation myelopathy is considered as another toxic type of myelopathy &t may occur months-to-years following irradiation of the spinal cord.
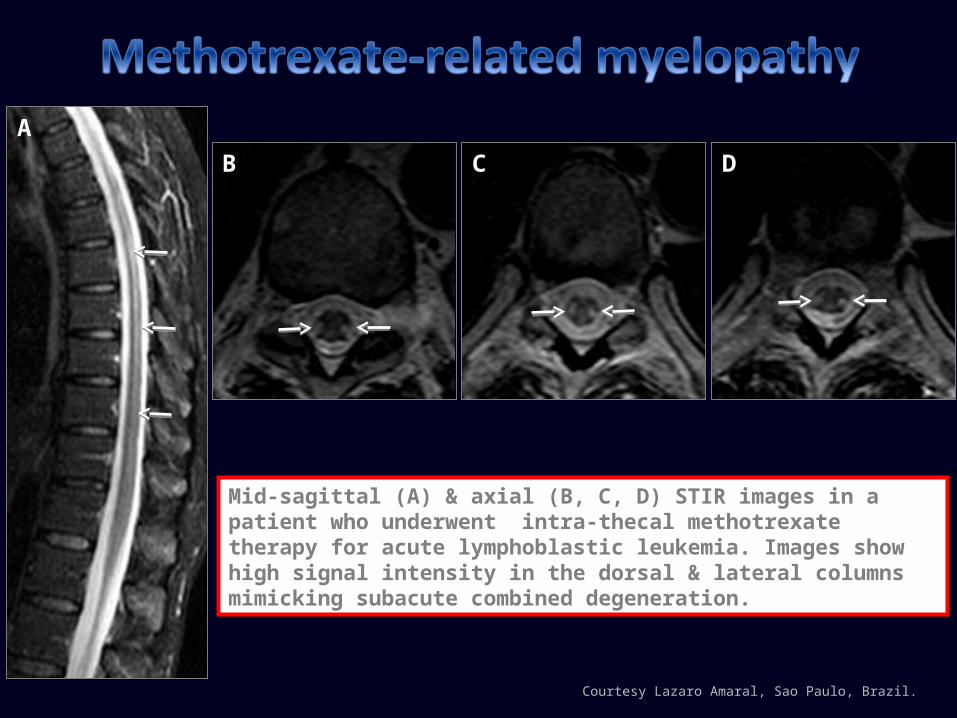
Mid-sagittal (A) & axial (B, C, D) STIR images in a patient who underwent intra-thecal methotrexate therapy for acute lymphoblastic leukemia. Images show high signal intensity in the dorsal & lateral columns mimicking subacute combined degeneration.
Courtesy Lazaro Amaral, Sao Paulo, Brazil.
AB DC
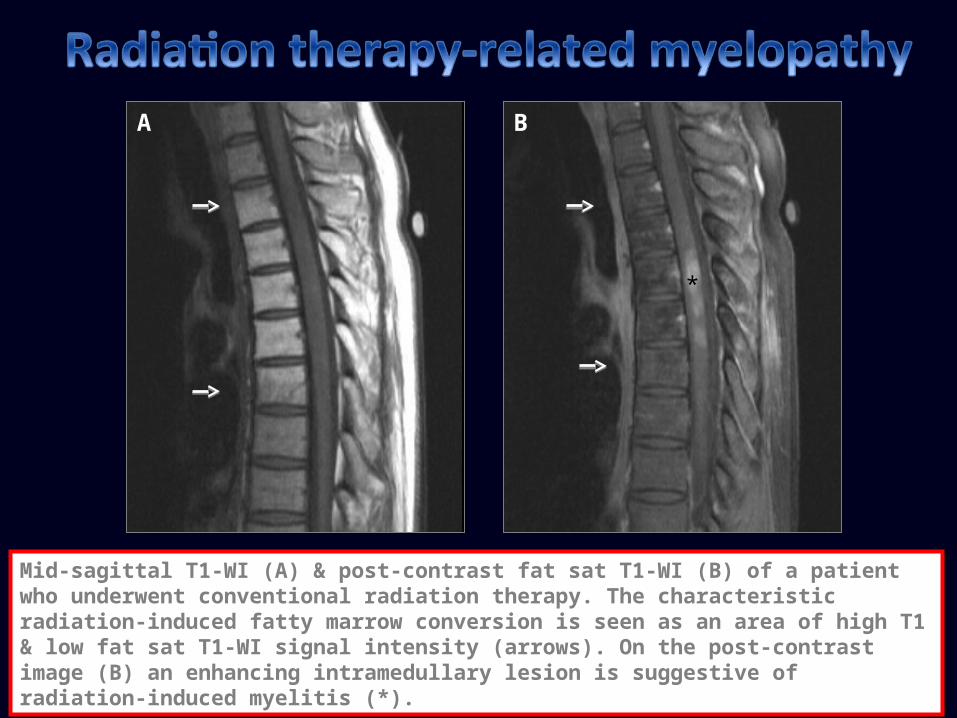
Mid-sagittal T1-WI (A) & post-contrast fat sat T1-WI (B) of a patient who underwent conventional radiation therapy. The characteristic radiation-induced fatty marrow conversion is seen as an area of high T1 & low fat sat T1-WI signal intensity (arrows). On the post-contrast image (B) an enhancing intramedullary lesion is suggestive of radiation-induced myelitis (*).
*
A B
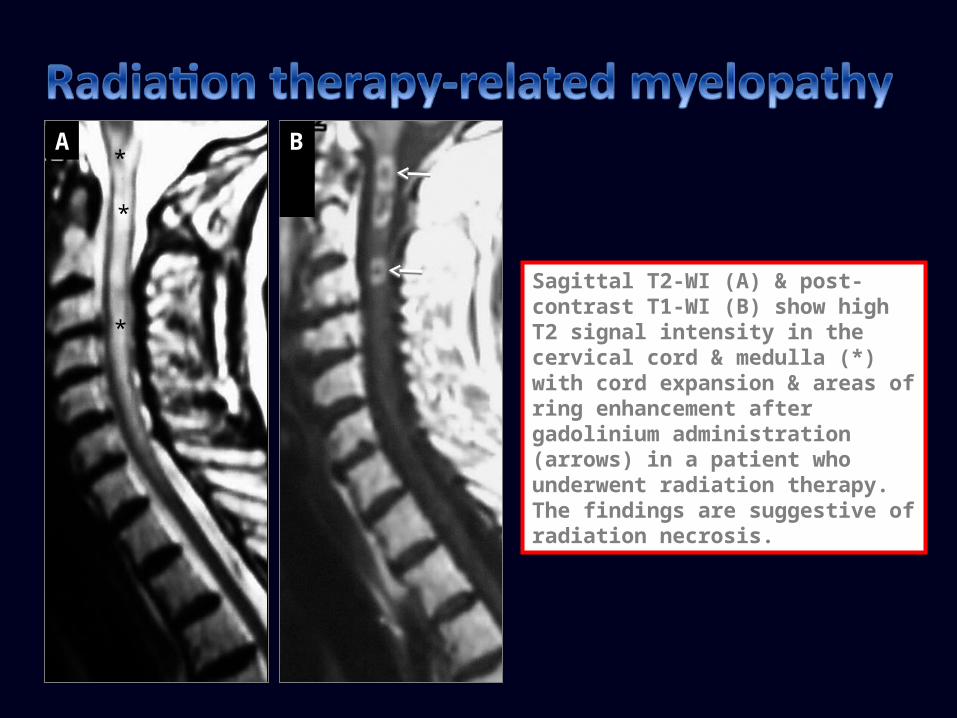
Sagittal T2-WI (A) & post-contrast T1-WI (B) show high T2 signal intensity in the cervical cord & medulla (*) with cord expansion & areas of ring enhancement after gadolinium administration (arrows) in a patient who underwent radiation therapy. The findings are suggestive of radiation necrosis.
*
*
A B
*
Brainstem & spinal cord infarcts have been reported in healthy patients following contact with water in the beaches of North Carolina & Virginia.
Jellyfish toxins have been proposed as the cause but the mechanism of neural tissue damage & distribution of lesions involving only the spinal cord and/or brainstem but sparing the brain is not known: Toxins may change membrane voltages & potentials leading to nerve
depolarization or may affect passage of calcium & sodium across excitable cell membranes.
Damage to the spinal cord may not be direct but due to systemic hypotension.
MRI: High T2-WI signal intensity in the anterior 2/3s of the cord with
restricted diffusion. Spinal cord infarctions have poor prognosis with little chance of recovery.
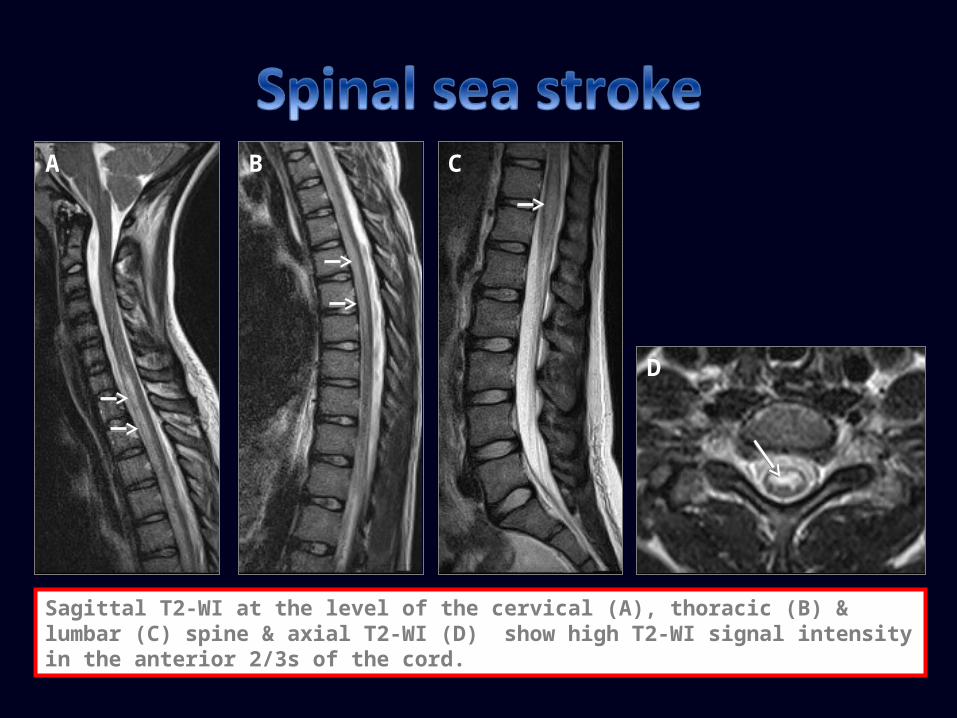
Sagittal T2-WI at the level of the cervical (A), thoracic (B) & lumbar (C) spine & axial T2-WI (D) show high T2-WI signal intensity in the anterior 2/3s of the cord.
A B
D
C
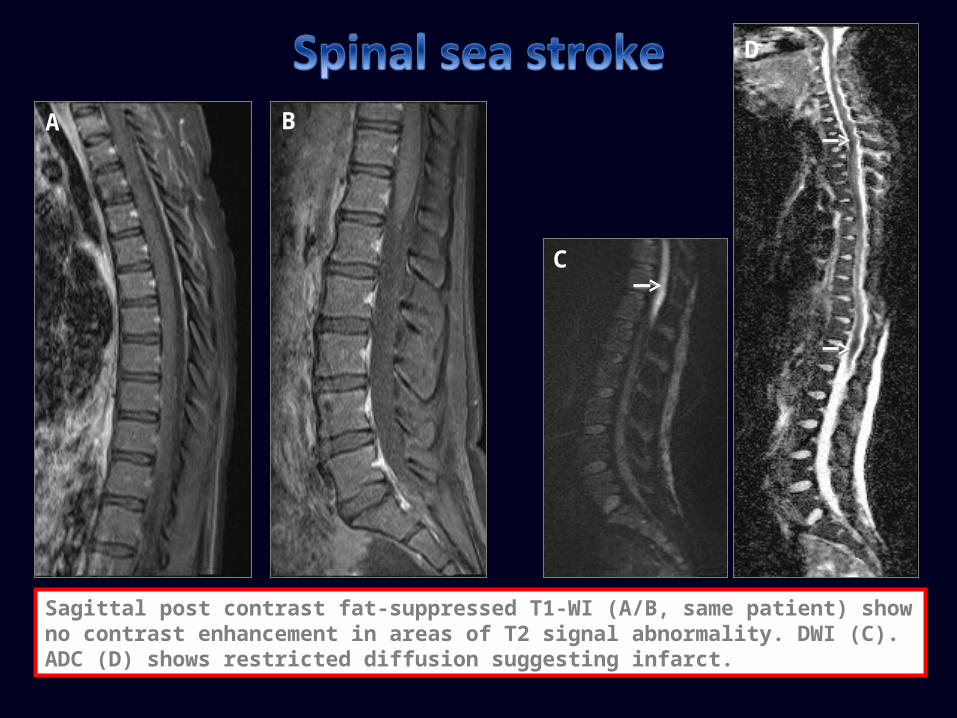
Sagittal post contrast fat-suppressed T1-WI (A/B, same patient) show no contrast enhancement in areas of T2 signal abnormality. DWI (C). ADC (D) shows restricted diffusion suggesting infarct.
A B
D
C
Clioquinol (iodochlorhydroxyquin) is an antifungal- antiprotozoal drug.
Clioquinol's use has been restricted or discontinued in some countries due to an event in Japan where >10,000 people developed subacute myelo-optic neuropathy.
Mechanism by which it causes this disease is not known: Clioquinol is a Cu-zinc chelate antibiotic & identification of a
myelopathy resulting from acquired copper deficiency has led to the speculation that clioquinol-induced neurotoxicity may be a consequence of Cu deficiency.
Lathyrism is a self-limiting neurotoxic disorde endemic in Bangladesh, India, & Ethiopia.
Presents as a subacute or insidious onset spastic paraparesis in patients who consume the environmentally tolerant legume lathyrus sativus (grass pea or chick pea) as a dietary staple.Typical is a lurching scissoring gait characterized by patients walking on the balls of their feet. In severely affected individuals, pyramidal signs may be present in the upper limbs. Lower limb sensory symptoms may occur but sensory signs are rare.
Toxin is probably Beta-N-oxalyl-amino-L-alanine (L-BOAA) an excitotoxic amino acid present in lathyrus sativus.
No typical MRI findings have been described.
Konzo is a tropical myelopathy seen in Africa resulting from weeks of high dietary cyanide exposure due to consumption of insufficiently processed cassava.
Clinically: Abrupt onset of spastic non-progressive paraparesis. Absence of sensory or autonomic disturbances. Upper limbs & visual pathways may be involved. Years of cassava consumption are implicated in a syndrome
of slowly progressive ataxia, peripheral neuropathy, & optic atrophy.
No typical MRI findings have been described.
Cerebral & spinal cord edema & infarction are rare complications of diabetic ketoacidosis. There are no existing theories to explain the mechanism of spinal cord edema/infacrt due to the rarity of reported cases:
Systemic hypotension & hypoxia? Rapid changes in serum osmolarity? Disseminated intravascular coagulation? Thrombosis secondary to dehydration, hemoconcentration & hyperviscosity?
MRI may show spinal cord edema and/or infarcts & atrophy in late stages.
Courtesy Antonio Jose da Rocha, Sao Paulo, Brazil.
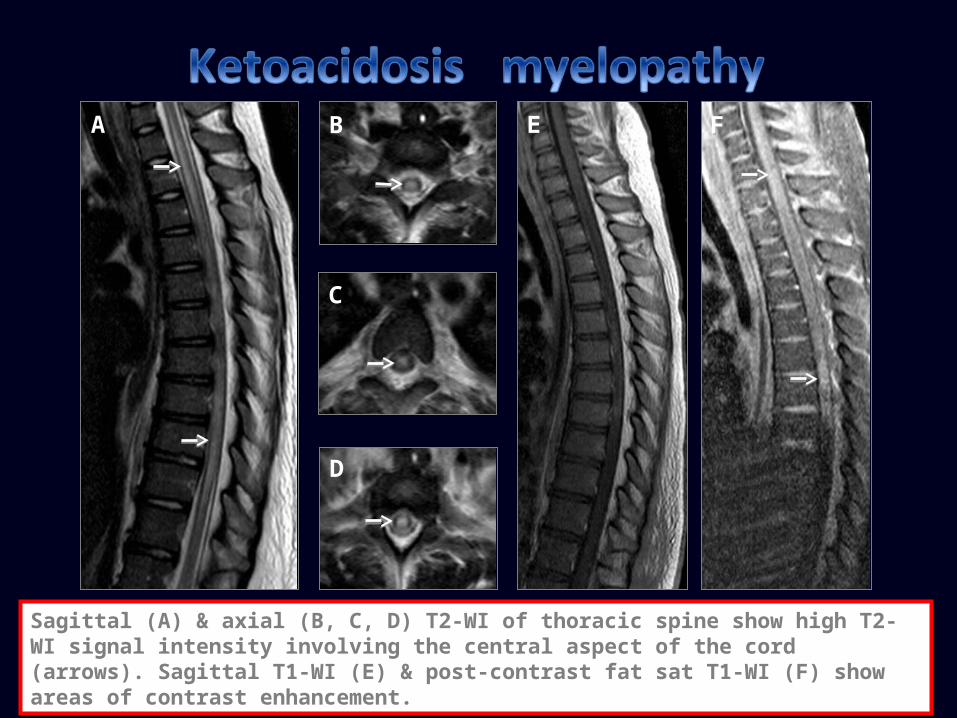
Sagittal (A) & axial (B, C, D) T2-WI of thoracic spine show high T2-WI signal intensity involving the central aspect of the cord (arrows). Sagittal T1-WI (E) & post-contrast fat sat T1-WI (F) show areas of contrast enhancement.
A B
D
C
E F
A clinical syndrome caused by alterations in environmental pressure resulting in liberation of inert gas bubbles in tissues or blood. Type I: joint pain, skin marbling, small patchy hemorrhages, & lymphatic
obstruction Type II: CNS involvement.
Cerebral: results from arterial gas embolism. Spinal cord: results from bubble embolization in epidural vertebral
venous system causing congestion & venous cord infarct. Spinal cord involvement accounts for 77% of CNS diving injuries. Recovery of CNS may be incomplete.
Hyperbaric oxygen therapy is main treatment.
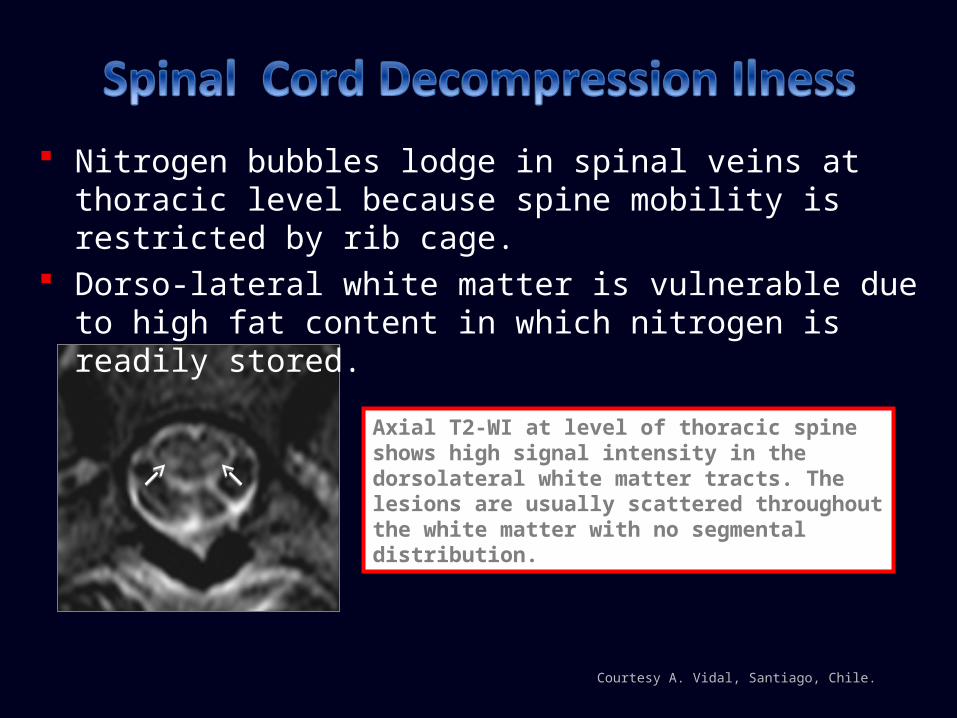
Nitrogen bubbles lodge in spinal veins at thoracic level because spine mobility is restricted by rib cage.
Dorso-lateral white matter is vulnerable due to high fat content in which nitrogen is readily stored.
Axial T2-WI at level of thoracic spine shows high signal intensity in the dorsolateral white matter tracts. The lesions are usually scattered throughout the white matter with no segmental distribution.
Courtesy A. Vidal, Santiago, Chile.
Is a rare non-traumatic injury occurring in novice surfers who lay prone on a surfboard with the lumbar spine hyperextended for prolonged periods of time.
It is preceded by back discomfort followed by acute myelopathy with variable motor-sensory involvement & urinary incontinence.
Etiology: Arterial insufficiency from hyperextension of lumbar spine? Venous
hypertension associated with obstruction of inferior vena cava? Fibrocartilagenous embolism from the nucleus pulposus into radicular spinal cord arteries? Avulsion of perforating arteries?
MRI: central cord T2 high signal extending from mid-thoracic region to conus without contrast enhancement.
No treatment is available, recovery is variable.
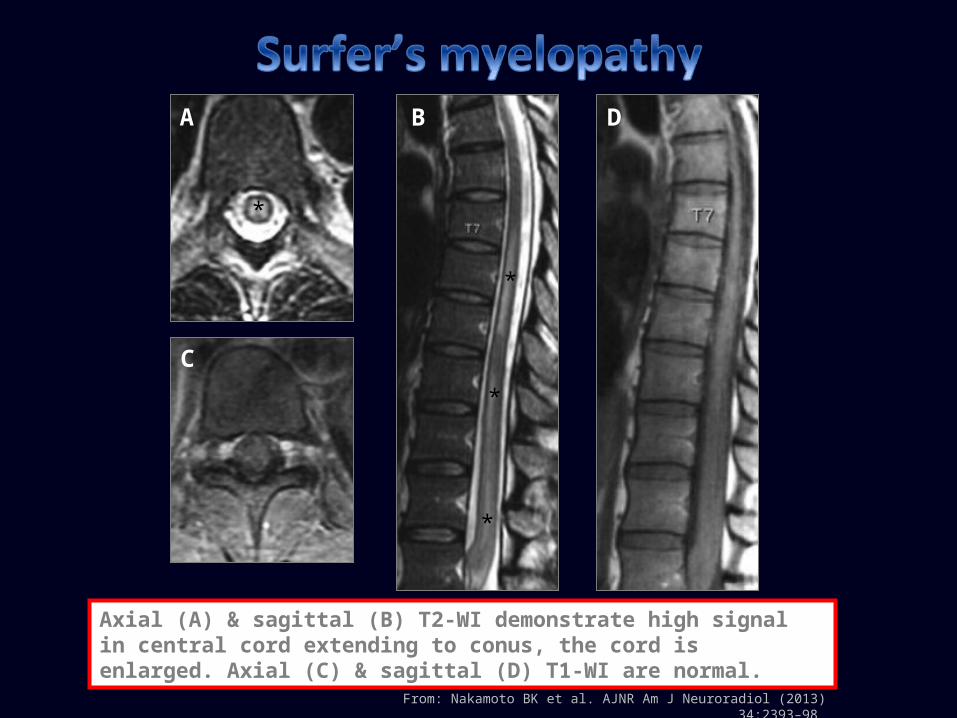
From: Nakamoto BK et al. AJNR Am J Neuroradiol (2013) 34:2393–98
Axial (A) & sagittal (B) T2-WI demonstrate high signal in central cord extending to conus, the cord is enlarged. Axial (C) & sagittal (D) T1-WI are normal.
A B D
C
*
*
*
*
Toxic & metabolic myelopathies are rare & have clinical, neuropathologic & imaging features in common as follows: Variable degrees of peripheral nerve and/or optic nerve
involvement. Preferential involvement of dorsal columns and/or corticospinal
tracts. Biopsy is rarely performed thus diagnosis & management rely on
patient’s history, physical examination, laboratory results & imaging findings.
Familiarity with these entities may lead to accurate diagnosis with successful identification of the underlying cause & appropriate treatment to revert or prevent progression of neurological symptoms.
Kumar N. Metabolic and Toxic Myelopathies. Semin Neurol (2012) 32:123–136. Schwendimann RN. Metabolic, Nutritional, and Toxic Myelopathies. Neurol Clin (2013) 31: 207–218. Kumar N. Myelopathy. Semin Neurol (2010) 30: 38–43. Naidich MJ and Ho SU. Case 87: Subacute Combined Degeneration. Radiology (2005) 237: 101–105. Sen A and Chandrasekhar K. Spina; MR imaging in Vitamin B12 deficiency: Case series; differential diagnosis of
symmetrical posterior spinal cord lesions. Ann Indian Acad Neurol (2012) 15:255-8. Chong J, Di Rocco A, Tagliati M, et al. MR Findings in AIDS-Associated Myelopathy. AJNR Am J Neuroradiol (1999) 20:
1412–1416 Okada A, Koike H, Nakamura T, et al. Slowly progressive folate-deficiency myelopathy: Report of a case. Journal of the
Neurological Sciences (2014) 336: 273–275. Kumar N. Copper Deficiency Myelopathy (Human Swayback). Mayo Clin Proc. (2006) 81(10): 1371-1384. Gosavi T, Diong CP, and Lim SH. Methotrexate-induced myelopathy mimicking subacute combined degeneration of the
spinal cord. Case Reports / Journal of Clinical Neuroscience (2013) 20: 1025–1026. Yi Y, Kang HJ, Shin HY, et al. Progressive Myelopathy Mimicking Subacute Combined Degeneration After Intrathecal
Chemotherapy. Journal of Child Neurology (2015) 30(2): 246-249. Chiang F and Castillo M. Seastrokes: A New Threat for North Carolina Swimmers? A Case Report. The Neuroradiology
Journal (2014) 27: 499-502. Christodoulidou M and Selmi F. Severe diabetic ketoacidosis leading to cardiac failure, pulmonary oedema and spinal
cord oedema resulting in tetraplegia. BMJ Case Reports (2012) 1-3. Blatteau JE, Gempp E, Simon O, et al. Prognostic Factors of Spinal Cord Decompression Sickness in Recreational Diving:
Retrospective and Multicentric Analysis of 279 Cases. Neurocrit Care (2011) 15: 120–127. Nakamoto BK, Siu AM, Hashiba KA, et al. Surfer’s Myelopathy: A Radiologic Study of 23 Cases. AJNR Am J Neuroradiol
(2013) 34: 2393–98.