Embed Size (px)
Citation preview

Joe Kutzin
Es coordinador de financiamiento en salud en la Organización Mundial de laSalud (OMS). Obtuvo su Maestría en Economía del Desarrollo en laUniversidad de Boston en 1985 y recibió un Doctorado Honorario de laUniversidad Semmelweis en Budapest en 2012. Es un economista de la saludque comenzó su carrera en Jamaica y ahora cuenta con más de 30 años deexperiencia en reformas de sistemas de salud, trabajando en países deÁfrica, Asia, el Caribe y Europa. Ha estado en la OMS durante más de 20años, prestando servicios en la sede central, en Kirguistán como asesor depolíticas del Ministerio de Salud, y en Copenhague y Barcelona como Asesorde la Región de Europa en Financiamiento en Salud. Fue colaborador delInforme sobre la salud en el mundo 2010 en el área de financiamiento de lacobertura universal y ha publicado numerosos artículos conceptuales yempíricos sobre financiamiento de la salud y Cobertura Universal, incluidocomo autor principal de un capítulo sobre lecciones aprendidas de laexperiencia con reformas financieras para avanzar hacia la CoberturaUniversal. El equipo que dirige en la OMS brinda orientación, servicios deasesoramiento sobre políticas, desarrollo de capacidades y trabajo técnicosobre compras estratégicas, monitoreo y seguimiento de gastos en salud ycuestiones de (des)alineación entre el financiamiento de la salud y la gestiónfinanciera del sector público.
Coordinador, Política de Financiamiento de la Salud, Organización Mundial de la Salud (OMS), Ginebra Suiza

Financing reforms for Universal Health Coverage: from theory to practice
Joseph Kutzin | Coordinator, Health Financing | Health
Systems Governance and Financingwww.who.int
VIII Congreso de Economía de la Salud de América Latina y el Caribe y en el VI Congreso de la Asociación
Colombiana de Economía de la SaludMedellin, Colombia. 1-3 October 2018

Need for core concepts to set direction for where we want to go (normative), and understand from where we are starting (positive) and explore options
• Draws on (a) thinking like a health economist, and (b) early thinking from LA (functional approach from Frenk, Londono and Frenk)
Operationalizing UHC – moving towards
Health financing functional approach
Guiding principles – health economics and what we know from practice
Overview/outline

Fis
cal co
nte
xt
Three pillars for approaching health financing policy
Desc
rip
tive
fram
ew
ork
Po
licy
ob
ject
ives
Health financing policy analysis and
viable options for reform
Starting point, direction, and reality check
Where should
we go?
(normative)
Where are we
starting from?
(positive)
What kind of vehicle
can we afford to get
us there? How far and
how fast?
(sustainability)

Normative: operationalizing UHC as a basis for public policy

All countries should seek to ensure that their
populations get the health services they need,
of good quality, without fear of the financial
consequences of paying for these services.
UHC as a normative proposition
Difficult if not impossible to have a sensible public policy discussion without consensus around what it is you are trying to achieve

Operationalize UHC as a direction, not a destination
• Reduce the gap between need and utilization (equity)
• Improve quality
• Improve financial protection
But even if this is accepted, normative question for each country remains: by how much to make these improvements, and at what cost? Answers to these depend on what is socially/politically acceptable – not something that an international agency can answer for a country.
Assuming general agreement on the basic normative proposition…

Coverage as a “right” (of citizenship, residence) rather than as just an employee benefit
• Critically important implications for choices on revenue sources and the basis for entitlement
Unit of analysis: system, not scheme
• Effects of a “scheme” is not of interest per se; what matters is the effect on UHC goals considered at level of the entire system and population
• Critical in the context of segmentation
An explicitly political agenda…because it involves redistribution
Public policy implications of this normative proposition

Positive: Health financing from a functional perspective
How to think about health
financing and the instruments of
reform

Functional approach to health systems
• Frenk (1995). “Comprehensive policy analysis for health system reform.” Health Policy 32: 257-277
• Londoño and Frenk (1997). “Structured pluralism: towards an innovative model for health system reform in Latin America.” Health Policy 41:1-36
Emerged in response to the segmented health systems within the region
• Perhaps a first example of thinking that went “from scheme to system”
Intellectual roots

Policy/political question:
•Why not organize the system by function rather than social group?
Technical response
• Functional description of health systems
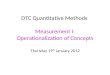
It was a response to the segmented health systems of Latin America
Adapted from Frenk (1995)
Upper
incomePoor
Insured
Functions
Delivery
Financing
Stewardship
Uninsured
Ministry of
Health
Social
security
Private
sector
SOCIAL GROUPS

Applied to change thinking about health financing: from labels to functions
Revenue raising
Pooling
Purchasing
Benefits and co-payments
“National Health System”
“Social Health Insurance System”
“Mixed Systems”
Classifications or models Functions and policies
Understand systems (and reform options) in
terms of functions, not labels or models
Are German citizens more insured than British citizens, just
because they call their system “insurance”?

All systems can be analyzed in this way
C o v e r a g e
Source/
revenue
Pooling
Purchasing
Provision
Population
General tax revenues
of each Oblast
C o v e r a g e
USSR: duplication
Rayons Oblast
Local
Gov’t
Local
Gov’t
Local
Gov’t
MOH
MOH
MOH
poor middle rich
LA: segmentation
General
taxation
MOH
MOH
uninsured
MOH
Voluntary
contribution
VHI and OOPS
SHI
SHI
Payroll
taxation
SHI insured
SHI
SHI

Health financing for UHC: guiding principles derived from
theory (especially applied micro) and practice

Goal: move towards UHC
• Equity in use, quality, financial protection
• Assessed at the level of the system/population, not scheme and beneficiaries
Starting point:
• Existing health financing system, understood in functional terms, not models or labels
• Key contextual constraints (especially fiscal and public administrative structure)
Overall: separate ends and means
Combine normative and positive with theory and evidence

Even though broad UHC goals are shared by all…
• Specific manifestations of problems vary, so how the goals should be operationalized will vary as well
• Every country already has a health financing system, so starting point for each country is unique
•Mix of fiscal and other contextual factors also unique
But this should not be interpreted to mean that “anything goes” – we have learned a few things over past 30 years (or more)
• Some “do’s” and “don’ts” in health financing policy
•We can avoid repeating mistakes made by others
Message following WHR2010: the path to UHC should be home-grown

1. Focus on compulsory funding sources: move
towards predominant reliance on public funding
for UHC (tax, including mandatory contributions)
2. Reduce fragmentation to enhance re-
distributional capacity (more prepayment, fewer
prepayment schemes) and reduce administrative
duplication
3. Move towards strategic purchasing to align
funding and incentives with promised services,
promote efficiency and accountability, and
manage expenditure growth to sustain progress
WHO health financing: 3 policy principles to guide health financing reform(ers)

From theory
• Arrow (1963). “Uncertainty and the welfare economics
of medical care.” American Economic Review 53:941–
973.
• Akerlof (1970). “The market for “lemons": quality
uncertainty and the market mechanism.” Quarterly Journal of Economics 84:488-500.
We can’t ignore adverse selection and supplier-
induced demand
What do theory and health economists tell us?

Fuchs (1996). “What every philosopher should know about health economics.” Proceedings of the American Philosophical Society 140:186-196
• Section titled “Two necessary and sufficient conditions for universal coverage” (WHR 2010 in 3 paragraphs)
• Compulsion (funding from some type of tax, with the entire population in the pool)
• Subsidization (for those unable to contribute)
Grounded in understanding of adverse selection, backed by global evidence
Raising revenues for UHC: the Fuchs conditions

No country has made much progress by relying on voluntary prepayment/individual contributions
• Private voluntary health insurance, community-based health insurance, or informal sector contributions to national schemes
• We can’t just wish away adverse selection
In countries with large informal sectors, this will tend to mean reliance on general budget revenues to scale up coverage on a non-contributory basis (e.g. SIS in Peru, Seguro Popular in Mexico)
Revenue sources

Historical legacy in many countries which led
to “inequity by design”
Some relevant experiences from Europe and
elsewhere highlight that progressive change is
possible, even if politically difficult
Pool fragmentation: a critical issue for the region and beyond

Consolidation (merging)
• Baltic and Scandinavian countries and Poland in the 1990s (geographic consolidation of insurance funds or sub-national “purchasing” units)
• Turkey merged different public insurance schemes into one (formerly for different population groups)
Equalization (create a pool among the pools)
• Consumer choice among competing SHI funds (e.g. Czech, Germany, Netherlands), with risk-adjusted capitation to reduce risk of strategic pooling by insurers
• Balance (again, risk-adjusted) per capita resource base of non-competing territorial pools (e.g. UK, Sweden, Poland)
How European countries responded to multiple pools to mitigate fragmentation

Went for multiple insurers in early 90s (post USSR collapse)
Funding arrangements
• Employer-employee contributions
• Budget transfers on behalf of non-working people
Risk selection behavior by insurers led to financial problems for company that served most of population (elderly, non-working)
Introduced limited and crude risk-adjustment in 1994, but problems remained for many years
Reducing fragmentedpooling in a multi-payersystem: the Czech reforms

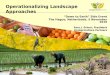
Incomplete pooling
•Only 60% of contributions subjected to
adjustment, together with budget transfers
Crude methods: insurers received 3x as much
per enrollee for persons over 60 years old
Risk adjustment before reforms introduced

OPPORTUNITIES FOR CREAM SKIMMING IN THE CZECH SYSTEM
BEFORE INTRODUCTION OF THE NEW RISK-ADJUSTMENT MECHANISM
Source: VZP; insurers’ annual reports
CZK in 2002
0
5 000
10 000
15 000
20 000
25 000
30 000
35 000
40 000
0 20 40 60 80
Average annualhealth care cost
Annual income per
economically non-
active insured
Age

Created one national pool
•100% of contributions subjected to adjustment,
together with budget transfers
Increased the sophistication of the risk
adjustment method
•36 age/sex categories, ex post partial
compensation of expensive cases
Risk adjustment reformsphased in over 2004-06 period

Pooling arrangements in Czech Republic prior to reform
Insured population
Co
ver
age
contracts
Source
Pooling
Purchasing
Provision
Population
Central budget revenues
(on behalf of non-working population)Payroll taxes
Health care providers
VZP
redistribution mechanism
other health insurers
40%60%

A virtual single pool createdby the 2003 reforms
Insured population
Co
ver
age
contracts
Source
Pooling
Purchasing
Provision
Population
Central budget revenues
(on behalf of non-working population)Payroll taxes
Health care providers
VZP
redistribution mechanism
other health insurers

3rd principle: you can’t just spend your way to UHC
Efficiency is central, but it won’t just happen by magic
Theory, again
• In well-functioning markets, unmanaged interactions between buyers and sellers would lead to an efficient result. But we don’t go for diagnostic tests or hip replacements because they are on sale…
• From Arrow and those who followed, e.g.
• Labelle, R, G Stoddart, T Rice (1994). “A re-examination of the meaning and importance of supplier-induced demand.” Journal of Health Economics 13:347-68.
• Fahs, MC (1992). “Physician response to the United Mine Workers' cost-sharing program: the other side of the coin.” Health Services Research 27:25-45.

Influencing provider behavioris key to drive efficiency gains and sustain progress
Strategic purchasing: linking payment to data on provider performance and the health needs of the population they serve
•Moving away from extremes of unmanaged fee-for-service or input-based line budgets with no provider autonomy
Recognizing and regulating out the potential for conflict-of-interest that can magnify consequences of supplier-induced demand (e.g. physician-owned diagnostic centers)

Fahs 1992 study in US (Pennsylvania):
• physician practice with two groups of insured patients
• Cost-sharing introduced for one, and their use fell
• In response, intensity of use by the other group of patients increased
China vs Thailand
• Both greatly increased public spending and affiliation to health insurance programs
• In Thailand, service use and financial protection improved due to coherent provider payment policies that managed spending growth.
• NOT the case in China
Supplier-induced demand and payment systems (evidence confirms theory)

Chinese Public Hospitals: “perfect alignment” of wrong incentives
All staff of the hospital are investors in the CT
scanner with objective to maximize its use
Source of slide: Prof. Winnie Yip

Final reflections

The analysis of how key interactions (patient-provider, person-insurer) deviate from standard market assumptions is at the core of key policy messages that are borne out by real-world experience
Practical application to health systems, particularly in Latin America, has helped us to move from models to functions, and from schemes to system
Health economics offers relevant insights

Public funding matters
• No country has made significant progress towards UHC without predominant reliance on some form of tax or compulsory contribution, due to reality of adverse selection
Reducing fragmentation is critical for both equity and efficiency objectives
• In particular to deal with a segmented context
• No one size fits all – countries have had success and failure with “single payer” and competition within a managed compulsory insurance market: implementation, not model
Towards more strategic purchasing
• Essential for system purchaser(s) to actively manage the allocation of resources to providers – it won’t just happen
And key messages for policy