Embed Size (px)
Citation preview

JONATHAN MANT, MD; ABDALLAH AL-MOHAMMAD, MD; SHARON SWAIN, BA, PHD; AND PHILIPPE LARAMEE,DC,MSC, FOR THE
GUIDELINE DEVELOPMENT GROUP
CHRIS FONTIMAYOR MS-IIIMERCER UNIVERSITYSCHOOL OF MEDICINEDR. RAHIMI9/9/2011
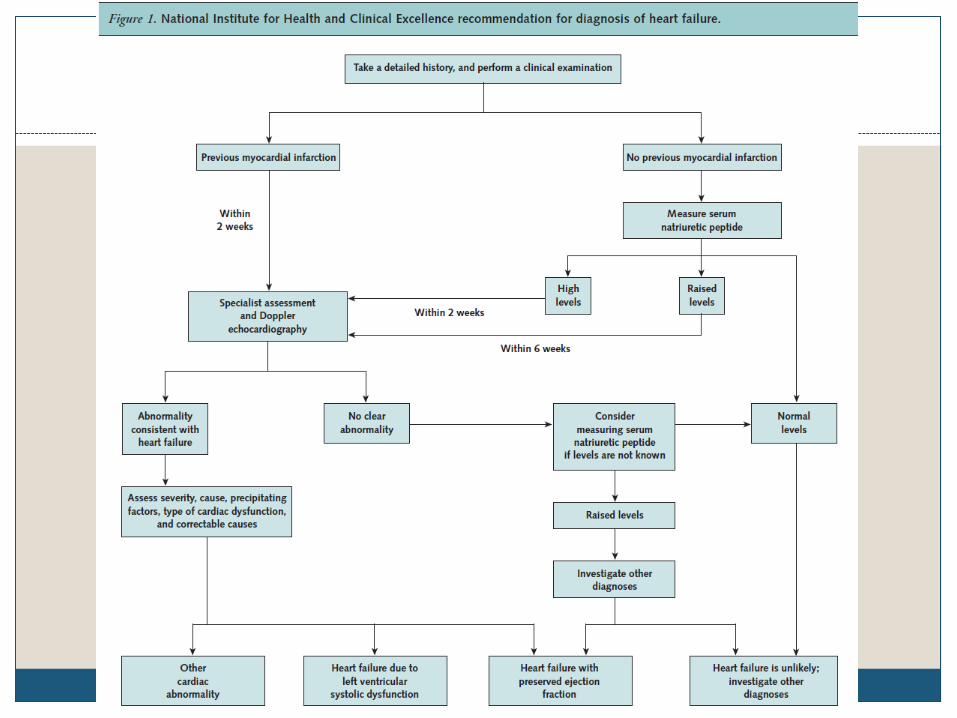
Management of Chronic Heart Failure in Adults: Synopsis of the National Institute
for Health and Clinical Excellence Guideline

Heart Failure (HF)
A common clinical syndrome representing the end-stage of a number of different cardiac diseases
Result of any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood
Two types Systolic Dysfunction Diastolic Dysfunction

Heart Failure
Symptoms – dyspnea, orthopnea, paroxysmal nocturnal dyspnea, nocturnal cough, confusion and memory loss in advanced stages, diaphoresis and cool extremities at rest
New York Heart Association (NYHA) Classification Class I – symptoms only with vigorous activities Class II – symptoms with moderate exertion Class III – symptoms with normal daily activities Class IV – symptoms at rest

National Institute for Health and Clinical Excellence (NICE)
Develops clinical practice guidelines for the National Health Service of England and Wales
First guideline on HF in 2003Target population: Non-pregnant adults with
symptoms of chronic HFExclusion: Patients with acute HF or acute
exacerbations of chronic HF Updated every 3 years
Literature searches for new evidence, warnings from licensing agencies , and major changes in costs
Actively seek out the views of health care professionals and patients

Guideline Development Process
Guideline development group (GDG)– general practitioners, specialist nurses, a consultant physician, consultant cardiologists, and 2 members representing patients and caregivers
Clinical question Literature review Evidence grading


High Quality Evidence for Pharmacologic Therapy
ACE inhibitors and ß-blockers reduce morbidity and increase survival in patients with left ventricular systolic dysfunction
No difference exists between selective ß-blockers (ie metoprolol) and nonselective ß-blockers (ie carvedilol) on the combined end point of mortality and hospitalization
Combination therapy of ARBs and ACE inhibitors increases risk of hyperkalemia
Adding ARB to ACE inhibitor and ß-blocker reduces the mortality and hospitalization caused by HF
Invasive Therapy Recommendations
Patients who are at any stage of HF with left ventricular systolic dysfunction should be considered for an implantable cardioverter-defibrillator (ICD)
Criteria Sustained ventricular tachycardia or non-sustained
ventricular tachycardia that is inducible on electrophysiology testing if the left ventricular ejection fraction (LVEF) is less than 35%
QRS of duration of 120 ms or longer if the LVEF is less than 30%

Rehabilitation
Moderate quality evidence shows that exercise rehab reduces hospital admissions for HF and increases long-term quality of life
GDG recommends supervised group exercise programs with psychological and educational components

Monitoring Patients With HF
Moderate quality evidence Therapy guided by serum natriuretic peptide levels
results in a reduction of hospitalizations due to HF Therapy guided by serum natriuretic peptide levels
reduces mortality in persons younger than 75 Cost effective analysis demonstrated that
serial serum natriuretic peptide monitoring was cost effective when used by specialists
Significant heterogeneity of evidence for the use of telemonitoring in decreasing hospitalizations GDG has no recommendation for telemonitoring

New Evidence Since the Implementation of the 2010 NICE guideline
EMPHASIS-HF Study (Epleronone in Mild Patients Hospitalization and Survival Study in Heart Failure) Significant reductions in hospitalization and mortality
when epleronone therapy is started in patients hospitalized during the preceding 6 months or with persistent moderate elevation of serum natriuretic peptide levels (BNP≥250 ng/L)
SHIƒT (Systolic Heart Failure Treatment with the Iƒ Inhibitor Ivabradine Trial) Ivabradine, Iƒ channel blocker in SA node, significantly
reduces unplanned hospitalization and mortality in patients with HF due to left ventricular systolic dysfunction whose HR remains higher than 70bpm

Discussion
NICE guidelines are broadly consistent with other international guidelines (ESC and AHA)
Benefits Earlier diagnosis Better management
Decreased morbidity and mortality Cost-effective

Level of Evidence











![Mant preventivo [autoguardado]](https://img.pdfslide.net/doc/110x75/556513d5d8b42a1a1d8b4bf5/mant-preventivo-autoguardado.jpg)



![De Mant]El Reparatioi\](https://img.pdfslide.net/doc/110x75/5571f3b949795947648e7da7/de-mantel-reparatioi.jpg)









![Seryice Mant]Al](https://img.pdfslide.net/doc/110x75/54a14bf8ac7959ea688b4665/seryice-mantal.jpg)



