Embed Size (px)
Citation preview
Jordan Anderson, SPT
developed by Dr. Kenzo Kase in 1979 to have qualities similar to human skin
allows 50-60% longitudinal stretch of resting length (does not stretch horizontally)
about the same thickness of the epidermis polymer elastic strands wrapped in cotton
fibers, heat-activated acrylic adhesive can be worn for 3-5 days before
reapplication is needed
Skin provides gentle stimulation to sensory
receptors during movement to activate the descending inhibitory system and decrease pain (Gate Control Theory)
or affects both acute sensory experience from
small afferents and prolonged sense of pain from the neural matrix (Neuromatrix Theory)
Circulation and Lymph “opens up” superficial lymphatic channels
by lifting the endothelial cells of the dermis they are connected to by anchoring filaments
allows decreased pressure of these vessels, encouraging more fluid flow to remove inflammatory substances from the area
muscle taping produces the same effect for deeper lymphatic vessels
Fascia minimizes fascial contraction following
acute soft tissue injury helps reorganize alignment of fibers during
chronic injuryby reducing pain and increasing circulation
via previously mentioned methods
Muscle takes advantage of neural control of
movement by assisting the Golgi Tendon Organs in sensation of muscle length and tension to protect them from excessive force
Joint reduces strain on joint ligaments to inhibit
the protective excitatory reflex and provide proper proprioception of the injured joint, which allows more appropriate movement
Application TechniquesApplication Techniques
“Recoiling” Mechanical correction; provides positional stimulation
through skin; use 50-75% stretch
“Holding” Fascia correction; gathers fascia to provide proper tissue
alignment; use 25-50% stretch
“Lifting” Space correction; reduces pressure around the affected
area be increasing space; use 25-50% stretch
“Pressure” Ligament/Tendon correction; increase stimulation of
mechanoreceptors for proprioception; use 50-75% stretch
“Spring” Functional correction; provides sensory stimulation to
either inhibit or enhance a motion; use 50-100% stretch
“Channeling” Lymphatic correction; channels fluid to nearest lymph duct
by decreasing pressure under the taped area; use 0-15% stretch

Jae-Yong Shim, Hye-Ree Lee, Duk-Chul Lee 22 male New Zealand White rabbits were put under
anesthesia and had a cannula inserted into a lymphatic vessel in the lower left hind leg
lymph flow rate was measured for 4 separate protocols: rate without passive exercise, rate with passive exercise, rate according to tape area with passive exercise, and rate according to tape site with passive exercise (each protocol included tape and no-tape conditions)
statistically significant increase in lymph flow rate was found for: taping vs no taping with passive exercise, increasing area of tape, and applying tape to upper or whole leg vs no tape
Han-Ju Tsai, Hsiu-Chuan Hung, Jing-Lan Yang, Chiun-Sheng Huang, Jau-Yih Tsauo
41 patients were separated into 2 groups: 1. standard decongestive lymphatic therapy with pneumatic compression, and 2. modified decongestive lymphatic therapy (bandage replaced with Kinesio Tape) with pneumatic compression
each patient completed a 4-week control period, 4-week intervention period, and 3-month follow-up; measurements were taken for water displacement, arm circumference, water composition, self-rated symptom severity (fullness, tightness, discomfort), quality of life, and response to bandage or tape
statistically significant improvement after the intervention period was found for: water displacement, circumference, water composition, and all 3 self-rated symptoms in the bandage group; but only forearm circumference, water composition, and all 3 self-rated symptoms in the KT group
statistical significance for between-group outcomes were not mentioned
patient acceptance of KT was more than that of the bandage and those in the KT group reported increased ease-of-use, longer use, and more comfort and convenience than those in the bandage group
Javier González-Iglesias, César Fernández-de-las-Peñas, Joshua Cleland, Peter Huijbregts, Maria del Rosario Gutiérrez-Vega
41 patients with a diagnosis of cervical whiplash-associated-disorders due to a MVA were randomly assigned to a therapeutic Kinesio Tape group or a sham Kinesio Tape group
measurements for neck pain, Neck Disability Index, and cervical range of motion (flexion, extension, right and left rotation, and right and left lateral flexion) were taken before tape application, immediately post-application, and 24 hours post-application
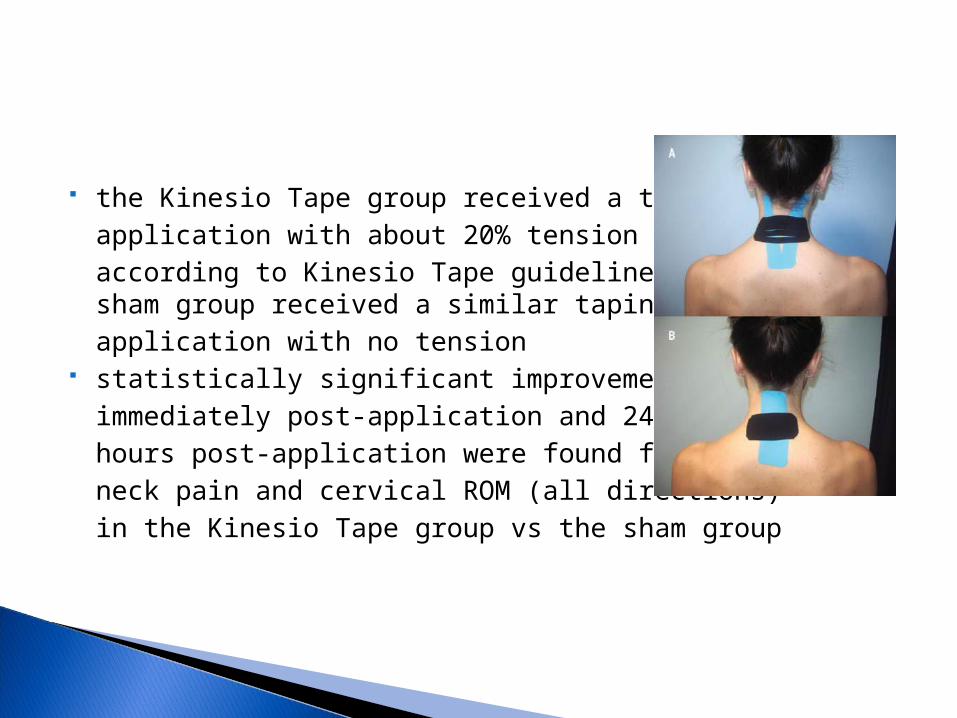
the Kinesio Tape group received a taping application with about 20% tension according to Kinesio Tape guidelines, the sham group received a similar taping application with no tension
statistically significant improvements immediately post-application and 24 hours post-application were found for: neck pain and cervical ROM (all directions) in the Kinesio Tape group vs the sham group
Manuel Saavedra-Hernández, Adelaida M. Castro-Sánchez, Manuel Arroyo-Morales, Joshua A. Cleland, Inmaculada C. Lara-Palomo, César Fernández-de-las-Peñas
80 patients with mechanical idiopathic neck pain were randomly assigned to either the Kinesio Tape group or the Manipulation group
measurements for neck pain, Neck Disability Index, and cervical range of motion (flexion, extension, right and left rotation, and right and left lateral flexion) were taken at baseline and 7 days post-treatment
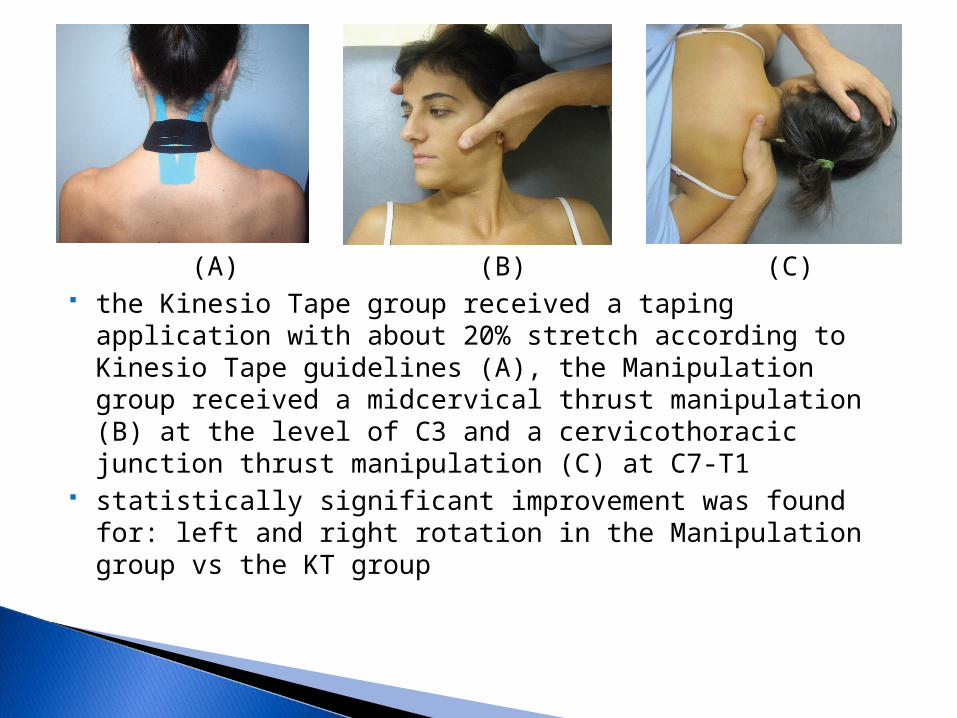
(A) (B) (C) the Kinesio Tape group received a taping application with
about 20% stretch according to Kinesio Tape guidelines (A), the Manipulation group received a midcervical thrust manipulation (B) at the level of C3 and a cervicothoracic junction thrust manipulation (C) at C7-T1
statistically significant improvement was found for: left and right rotation in the Manipulation group vs the KT group
Yin-Hsin Hsu, Wen-Yin Chen, Hsiu-Chen Lin, Wendy T.J. Wang, Yi-Fen Shih
17 baseball players with shoulder impingement syndrome were randomly assigned to one of two groups; each group received both Kinesio Tape and placebo tape (3M nonelastic) application, but in opposite order, over the lower trapezius
measurements were taken for scapular motion, EMG activity of the upper and lower trapezius and serratus anterior, and lower trapezius strength at baseline and after application of each taping condition
statistically significant difference between taping conditions was found for: increased lower trapezius EMG activity for KT
vs placebo tape from 60-30˚ of scaption (lowering)
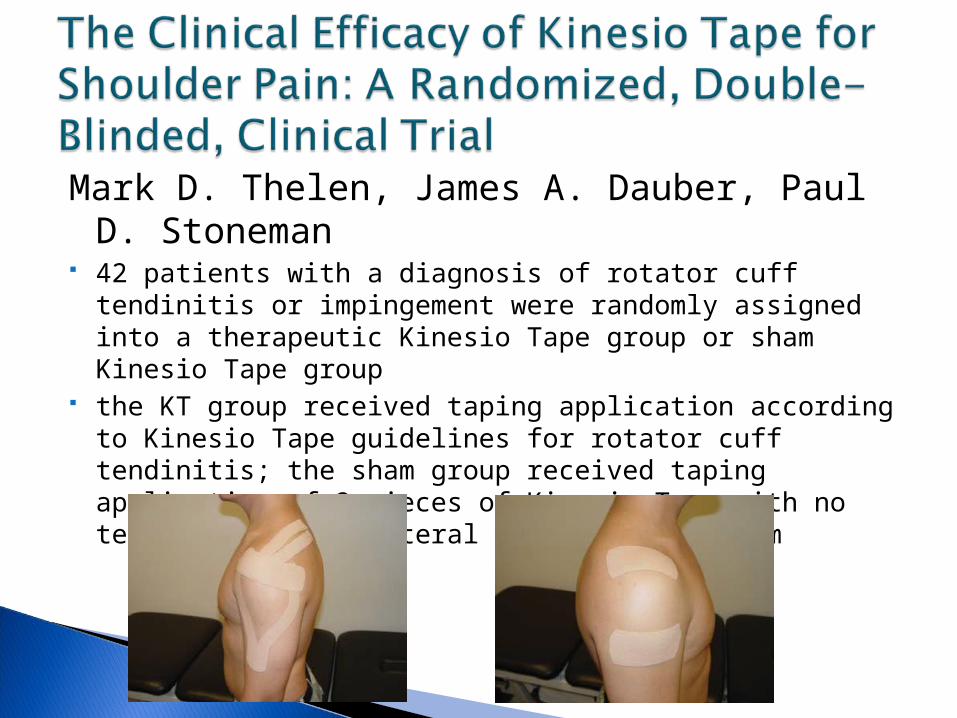
Mark D. Thelen, James A. Dauber, Paul D. Stoneman
42 patients with a diagnosis of rotator cuff tendinitis or impingement were randomly assigned into a therapeutic Kinesio Tape group or sham Kinesio Tape group
the KT group received taping application according to Kinesio Tape guidelines for rotator cuff tendinitis; the sham group received taping application of 2 pieces of Kinesio Tape with no tension over the lateral upper and mid- arm
measurements were taken for pain-free active range of motion, pain level, and Shoulder Pain and Disability Index at baseline, immediately after application (except the SPADI), 3 day follow-up, and 6 day follow-up
patients wore the tape for 48-72 hours, came in for their 3 day follow-up, received a re-application of tape, wore it for another 48-72 hours, and came in for their final follow-up
statistically significant changes were found for: increased pain-free shoulder abduction in the KT group vs sham group immediately post-application, improved SPADI scores for both groups at the 3 day follow-up, and improvement in all outcome measures for both groups at the 6 day follow-up
P.L. Chen, W.H. Hong, C.H. Lin, W.C. Chen 15 women with PFPS and 10 healthy women were all
evaluated for ground reaction forces (GRFs) and EMG activity (timing and ratio) of the vastus medialis and lateralis
each group received a taping application for the VMO and VL according to Kinesio Tape guidelines, the same application using nonelastic athletic tape, and a no tape condition; all participants then completed a stair-stepping task (ascencding and descending)
statistically significant differences were found for: decreased GRF during descending stairs for KT vs no tape in subjects with PFPS and increased VMO/VL ratio for KT vs no tape in subjects with PFPS
Travis Halseth, John W. McChesney, Mark DeBeliso, Ross Vaughn, Jeff Lien
30 patients were randomly assigned to a taping or no-tape condition first; all participants completed both conditions; taping application was for a lateral ankle sprain according to Kinesio Tape guidelines
patients sat with their bare foot on a moveable platform, were blindfolded, and wore earphones playing white noise; the platform was passively moved into a randomly-generated angle (plantarflexion and inversion with 20 degrees PF), held for 5 seconds, and returned to neutral, the patient then performed 5 trials of recreating each position
no statistically significant differences were found between conditions
Kristin Briem, Hrefna Eythorsdottir, Ragnheidur G. Magnusdottir, Runar Palmarsson, Tinna Runarsdottir, Thorarinn Sveinsson
51 male athletes received the Star Excursion Balance test, the top 15 and bottom 15 scores were used for the study
participants stood on one foot on a balance board while a 10-kg weight was dropped onto the posterolateral edge of the board; EMG for mean and peak muscle activity of the fibularis longus was recorded for 3 trials of each condition (Kinesio Tape, nonelastic athletic tape, and no tape)
statistically significant difference (increase) in mean muscle activation was found at 500ms for the unstable vs stable group and overall for the athletic tape vs no tape group
Shim JY, Lee HR, Lee DC. The use of elastic adhesive tape to promote lymphatic flow in the rabbit hind leg. Yonsei Medical Journal 2003; 44(6): 1045-1052.
Tsai HJ, Hung HC, Yang JL, Huang CS, Tsauo JY. Could Kinesio tape replace the bandage in decongestive lymphatic therapy for breast-cancer-related lymphedema? A pilot study. Support Care Cancer 2009; 17: 1353-1360.
González-Iglesias J, Fernández-de-las-Penas C, Cleland J, Huijbregts P, Gutiérrez-Vega M. Short-term effects of cervical Kinesio taping on pain and cervical range of motion in patients with acute whiplash injury: A randomized clinical trial. JOSPT 2009; 39(7): 515-521.
Saavedra-Hernández M, Castro-Sánchez AM, Arroyo-Morales M, Cleland JA, Lara-Palomo IC, Fernández-de-las-Penas C. Short-term effects of Kinesio taping versus cervical thrust manipulation in patients with mechanical neck pain: A randomized clinical trial. JOSPT 2012; 42(8): 724-730.
Hsu YH, Chen WY, Lin HC, Wang WTJ, Shih YF. The effects of taping on scapular kinematics and muscle performance in baseball players with shoulder impingement syndrome. Journal of Electromyography and Kinesiology 2009; 19: 1092-1099.
Thelen MD, Dauber JA, Stoneman PD. The clinical efficacy of Kinesio tape for shoulder pain: A randomized, double-blinded, clinical trial. JOSPT 2008; 38(7): 389-395.
Chen PL, Hong WH, Lin CH, Chen WC. Biomechanics effects of Kinesio taping for persons with patellofemoral pain syndrome during stair climbing. Biomed 2008; 21: 395-397.
Halseth T, McChesney JW, DeBeliso M, Vaughn R, Lien J. The effects of Kinesio taping on proprioception at the ankle. JSSM 2004; 3:1-7.
Briem K, Eythörsdöttir H, Magnúsdóttir RG, Pálmarsson R, Rúnarsdöttir T, Sveinsson T. Effects of Kinesio tape compared with nonelastic sports tape and the untaped ankle during a sudden inversion perturbation in male athletes. JOSPT 2011; 41(5): 328-335.
Kase K, Wallis J, Kase T (2003). Clinical Therapeutic Applications of the Kinesio Taping Method (2nd ed.). Tokyo, Japan: Ken Ikai Co. Ltd.
Hancock D. Scientific Explanation of Kinesio® Tex Tape. Obtained from: http://hitechtherapy.ipcoweb.com/user_images/kinesiotex/scientific_explanation_kinesiotex.pdf
ResourcesResources