Embed Size (px)
Citation preview

Jordan University of Science & TechnologyJordan University of Science & TechnologyJordan University of Science & TechnologyJordan University of Science & Technology
Faculty of EngineeringFaculty of EngineeringFaculty of EngineeringFaculty of Engineering
Department of Biomedical EngineeringDepartment of Biomedical EngineeringDepartment of Biomedical EngineeringDepartment of Biomedical Engineering
Experiment TitleExperiment TitleExperiment TitleExperiment Title PagePagePagePage
PART ONE:PART ONE:PART ONE:PART ONE: BenchBenchBenchBench ExperimentsExperimentsExperimentsExperiments Experiment # 1: Experiment # 1: Experiment # 1: Experiment # 1: Human HeartHuman HeartHuman HeartHuman Heart……………………………………………………………………………………………………………………………………………………………………………….…….…….……. 2222
Experiment # 2: Experiment # 2: Experiment # 2: Experiment # 2: Human SpirometryHuman SpirometryHuman SpirometryHuman Spirometry………………………………………...………………………………………...………………………………………...………………………………………... 11111111
Experiment # 3: Human Muscle…...Experiment # 3: Human Muscle…...Experiment # 3: Human Muscle…...Experiment # 3: Human Muscle…...……………………………………………………………………………………………………………………………………………………………… 22226666 Experiment # 4: Safety AnalyzerExperiment # 4: Safety AnalyzerExperiment # 4: Safety AnalyzerExperiment # 4: Safety Analyzer…………………………………………….…………………………………………….…………………………………………….……………………………………………. 33332222
Experiment # Experiment # Experiment # Experiment # 5: Pulmonary Function Test.……...5: Pulmonary Function Test.……...5: Pulmonary Function Test.……...5: Pulmonary Function Test.……...…………………….........…………………….........…………………….........……………………......... 41414141
Experiment # Experiment # Experiment # Experiment # 6: Audiome6: Audiome6: Audiome6: Audiomettttry ………………………………………………..ry ………………………………………………..ry ………………………………………………..ry ……………………………………………….. 44448888
Experiment # Experiment # Experiment # Experiment # 7: Gait Analysis……………………….....................................7: Gait Analysis……………………….....................................7: Gait Analysis……………………….....................................7: Gait Analysis………………………..................................... 56565656 PART TWO: Lab view ExperimentsPART TWO: Lab view ExperimentsPART TWO: Lab view ExperimentsPART TWO: Lab view Experiments
Prepared and Edited by: Dr.Prepared and Edited by: Dr.Prepared and Edited by: Dr.Prepared and Edited by: Dr.Ruba Khnouf andRuba Khnouf andRuba Khnouf andRuba Khnouf and Eng. Shereen Haddad Eng. Shereen Haddad Eng. Shereen Haddad Eng. Shereen Haddad
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 2
Experiment #1: Human HeartExperiment #1: Human HeartExperiment #1: Human HeartExperiment #1: Human Heart
Part A: ElectrocardioPart A: ElectrocardioPart A: ElectrocardioPart A: Electrocardiogram and Peripheral Circulationgram and Peripheral Circulationgram and Peripheral Circulationgram and Peripheral Circulation ObjectivesObjectivesObjectivesObjectives
• To learn the functions of LabScribe software and the IWX214 unit that are used
for recording, transforming, measuring, and displaying data. • To record a single lead ECG and the pulse wave in the finger of a subject
simulataneously.
• To demonstrate the time delay that occurs between the electrical events in the heart and mechanical events in the circulatory system.
• To examine the effects of temperature on peripheral circulation.
BackgroundBackgroundBackgroundBackground
The cardiac cycle involves the sequential contractions of the atria and the ventricles
which are triggered by action potentials in the myocardial cells. The combined electrical activity of the myocardial cells produces electrical currents that spread
through the body fluids. These currents are large and detectable by recording through
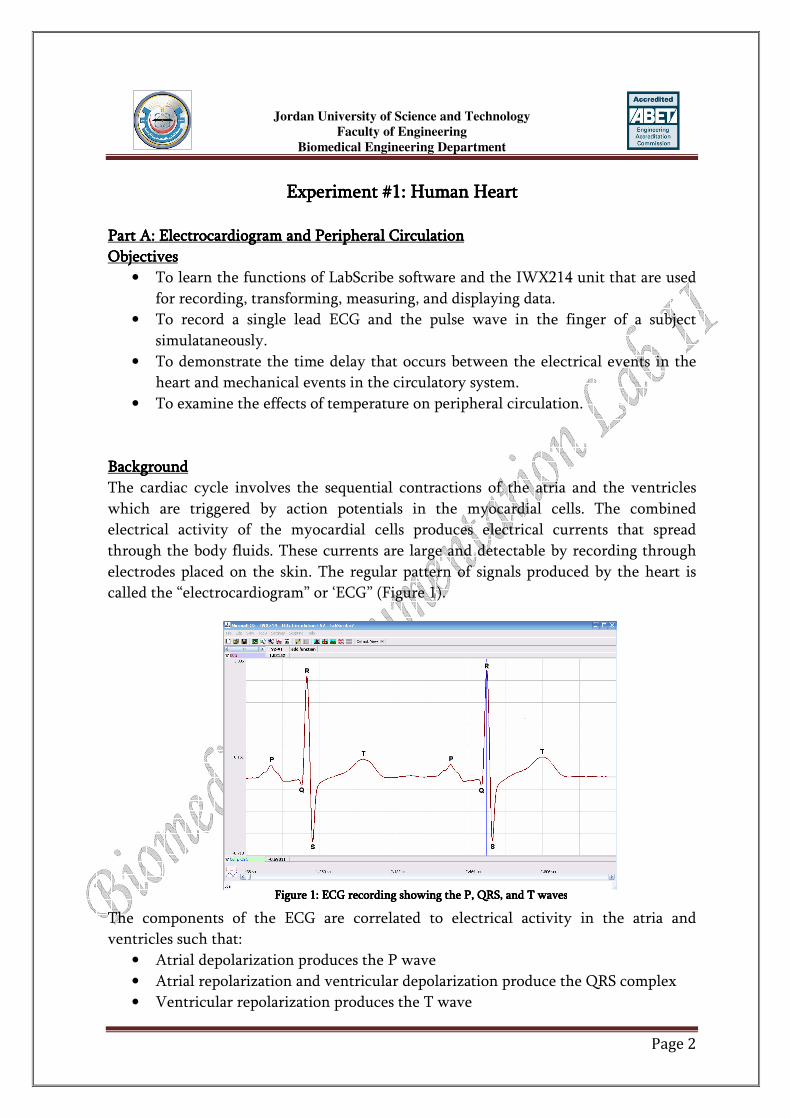
electrodes placed on the skin. The regular pattern of signals produced by the heart is called the “electrocardiogram” or ‘ECG” (Figure 1).
The components of the ECG are correlated to electrical activity in the atria and ventricles such that:
• Atrial depolarization produces the P wave
• Atrial repolarization and ventricular depolarization produce the QRS complex • Ventricular repolarization produces the T wave
Figure 1: ECG recording showing the P, QRS, and T wavesFigure 1: ECG recording showing the P, QRS, and T wavesFigure 1: ECG recording showing the P, QRS, and T wavesFigure 1: ECG recording showing the P, QRS, and T waves

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 3
The depolarization of the myocardial cells in the ventricle causes the ventricles to
contract and force blood into the major arteries of the circulatory system in a pulsatile
manner. The pulses of blood moving in arteries can be recorded using a device known as a “plethysmograph”.
EqEqEqEquipment Requireduipment Requireduipment Requireduipment Required
• PC Computer
• IWX/214 data acquisition unit • USB cable
• IWX/214 power supply
• C-AAMI-504 ECG cable and electrode lead wires
• PT-104 Pulse plethysmograph • Alcohol swabs
• Disposable ECG electrodes
IWX/214 SetupIWX/214 SetupIWX/214 SetupIWX/214 Setup
• Place the IWX/214 on the bench, close to the computer.
• Check the location of the USB port and the power socket on the IWX/214. • Use the USB cable to connect the computer to the USB port on the rear panel of
the IWX/214.
• Plug the power supply for the IWX/214 into the electrical outlet. Insert the plug on the end of the power supply cable into the labeled socket on the rear of the
IWX/214. Use the power switch to turn on the unit. Confirm that the red power
light is on.
Start the SoftwareStart the SoftwareStart the SoftwareStart the Software
Click on the LabScribe LabScribe LabScribe LabScribe shortcut on the computer’s desktop to open the program. If a
shortcut is not available, click on the Windows Start menuWindows Start menuWindows Start menuWindows Start menu, move the cursor to All All All All ProgramsProgramsProgramsPrograms and then to the listing for iWorxiWorxiWorxiWorx. Select LabScribeLabScribeLabScribeLabScribe from the iWorx submenuiWorx submenuiWorx submenuiWorx submenu.
The LabScribe Main windowMain windowMain windowMain window will appear
as the program opens. 1. On the Main windowMain windowMain windowMain window, pull down the Settings menuSettings menuSettings menuSettings menu and select Load GroupLoad GroupLoad GroupLoad Group.
2. Locate the folder that contains the settings group, IPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrp. Select this
group and click OpenOpenOpenOpen. 3. Pull down the Settings menuSettings menuSettings menuSettings menu again. Select the ECGECGECGECG----CirculationCirculationCirculationCirculation----LS2LS2LS2LS2 settings file.
4. After a short time, LabScribe will appear on the computer screen as configured
by the ECGECGECGECG----CirculationCirculationCirculationCirculation----LS2 LS2 LS2 LS2 settings.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 4
ECG Cable and Pulse Transducer SetupECG Cable and Pulse Transducer SetupECG Cable and Pulse Transducer SetupECG Cable and Pulse Transducer Setup
1. Locate the PT-104 pulse plethysmograph and C-AAMI-504 ECG cable and
electrode lead wires in the iWorx kit. 2. Plug the DIN8 connector to the PT-104 into the Channel 3 input of the
IWX/214.
3. Insert the black AAMI connector on the end of the ECG cable into the isolated inputs of Channels 1 and 2 of the IWX/214.
4. Insert the connectors on the red, black, and green electrode lead wires into the
matching sockets on the lead pedestal of the ECG cable. 5. Instruct the subject to remove all jewelry from their wrists and ankles.
6. Use an alcohol swab to clean and scrub a region with little or no hair, on the
inside of the subject’s right wrist. Let the area dry.
7. Remove a disposable ECG electrode from its plastic shield, and apply the electrode to the scrubbed area on the wrist.
8. Repeat Steps 6 and 7 for the inside of the left wrist and the inside of the right
ankle. 9. Snap the lead wires onto the electrodes, so that:
• The red (+1) lead is attached to the right wrist
• The black (-1) lead is connected to the left wrist • The green (C or ground) lead is connected to the right leg.
10. Place the plethysmograph on the volar surface (where the fingerprints are
located) of the distal segment of the subject’s middle finger, and wrap the Velcrotm strap around the end of the finger to attach the unit firmly in place.
11. Instruct the subject to sit quietly with their hands in their lap. If the subject
moves, the ECG trace will move off the top or bottom of the screen. If the
subject moves any muscles in the arms or upper body, electromyograms (EMGs) from the muscles will appear on the ECG recording as noise.
The ECG and the Pulse in a RestingThe ECG and the Pulse in a RestingThe ECG and the Pulse in a RestingThe ECG and the Pulse in a Resting SubjectSubjectSubjectSubject ProcedProcedProcedProcedure:ure:ure:ure:
1. Click on the Record button, located on the upper right side of the LabScribe
Main window. The signal should begin scrolling across the screen. 2. Click on the AutoScaleAutoScaleAutoScaleAutoScale button at the upper margin of the ECG, Pulse, and Pulse
Integral channels.
3. When you have a suitable trace, type <Subject’s Name><Subject’s Name><Subject’s Name><Subject’s Name> Resting ECG/PulseResting ECG/PulseResting ECG/PulseResting ECG/Pulse in the Mark boxMark boxMark boxMark box to the right of the Mark buttonMark buttonMark buttonMark button. Press the EnterEnterEnterEnter key on the
keyboard to attach the comment to the data. Record for a minute or two.
4. Click StopStopStopStop to halt recording.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 5
5. Select Save AsSave AsSave AsSave As in the File menuFile menuFile menuFile menu, type a name for the file. Choose a destination on
the computer in which to save the file, like your lab group folder). Designate the
file type as *.iwxdata*.iwxdata*.iwxdata*.iwxdata. Click on the SaveSaveSaveSave button to save the data file. Data AnalysisData AnalysisData AnalysisData Analysis
1. Scroll through the recording and find a section of data with five or six exemplary
ECG/pulse cycles in succession. 2. Use the Display TimeDisplay TimeDisplay TimeDisplay Time icons to adjust the Display TimeDisplay TimeDisplay TimeDisplay Time of the Main windowMain windowMain windowMain window to
show at least four complete ECG/Pulse cycles on the Main windowMain windowMain windowMain window. Four
adjacent ECG/Pulse cycles can also be selected by: • Placing the cursors on either side of a group of four complete ECG/Pulse
cycles.
• Clicking the Zoom between CursorsZoom between CursorsZoom between CursorsZoom between Cursors button on the LabScribe toolbar to
expand the segment with the four selected ECG/Pulse cycles to the width of the Main windowMain windowMain windowMain window.
3. Click on the Analysis windowAnalysis windowAnalysis windowAnalysis window icon in the toolbar or select AnalysisAnalysisAnalysisAnalysis from the
Windows menuWindows menuWindows menuWindows menu to transfer the data displayed in the Main windowMain windowMain windowMain window to Analysis Analysis Analysis Analysis windowwindowwindowwindow.
4. Look at the Function Table Function Table Function Table Function Table that is above the uppermost channel displayed in the
Analysis Analysis Analysis Analysis window. The names of the mathematical functions used in the analysis, V2V2V2V2----V1 V1 V1 V1 and T2T2T2T2----T1T1T1T1, appear in this table. The values for V2V2V2V2----V1 V1 V1 V1 and T2T2T2T2----T1 T1 T1 T1 from
each channel are seen in the table across the top margin of each channel. In this
exercise will only need to record the values for T2T2T2T2----T1T1T1T1. 5. Once the cursors are placed in the correct positions for determining the time
intervals on each ECG/Pulse cycle, the values of the time intervals can be
recorded in the on-line notebook of LabScribe by typing their names and values
directly into the JournalJournalJournalJournal, or on a separate data table. 6. Use the mouse to click on and drag the cursors to specific points on the
ECG/Pulse recording to measure the following:
• The beat periodbeat periodbeat periodbeat period, which is the time interval between two adjacent R waves. To measure the beat period, place one cursor on the peak of a R wave and the
second cursor on the peak of the adjacent R wave. The value for T2T2T2T2----T1 T1 T1 T1 on the
ECG ECG ECG ECG channel is the beat period. Measure the beat period for two additional pairs of R waves.
• The RRRR----Pulse intervalPulse intervalPulse intervalPulse interval, which is the time interval between the peak of the R wave
and the peak of the pulse wave that follows the R wave. To measure this interval, place one cursor on the peak of a R wave and the second cursor on the
peak of the pulse wave to its right. The value for T2T2T2T2----T1 T1 T1 T1 on any channel is this
interval. Measure this interval for two additional ECG/Pulse cycles. 7. Calculate the following values::::
• The average beat period, in seconds/beat.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 6
• The heart rate, which is expressed in beats per minute and calculated from
the average beat period by using the following equation:
• The average RRRR----Pulse intervalPulse intervalPulse intervalPulse interval.
Part Part Part Part BBBB: : : : TheTheTheThe Electrocardiogram and HeartElectrocardiogram and HeartElectrocardiogram and HeartElectrocardiogram and Heart SoundsSoundsSoundsSounds
ObjectivesObjectivesObjectivesObjectives • To measure the ECG in a resting individual.
• To study the phasing of heart sounds to the ECG
BackgroundBackgroundBackgroundBackground
Blood enters the arterial system from the ventricles of the heart in a pulsatile manner.
However, when blood is leaving the arterial system through the capillaries, it flows in a continuous manner. Between contractions, when the heart is relaxed and blood is not
being pumped into the arterial system, there is still enough pressure in the arterial
system to move blood along the arteries. The pressure in the arterial system exists because the elasticity of the arteries allow them to
distend and recoil and function as a pressure reservoir. When the ventricles contract,
the pressure of the blood inside the ventricles increases to close the atrioventricular valves. Further contraction increases the
ventricular pressure until it exceeds the arterial pressure. At this point, when the
arterial pressure is at its lowest point during the cardiac cycle (called diastolic pressure)
the semilunar valves are forced open, and blood flows into the artery. Blood entering the arterial system inflates the arteries a little and increases blood pressure to a
maximum, which is the systolic pressure.
The “lub” sound occurs during the early phase of ventricular contraction and is produced by closing of the atrioventricular valves, which prevents blood flow into the
atria. When the ventricles relax, the blood pressure drops below what is in the artery
and the semilunar valves close, producing the “dub” sound.
Equipment RequiredEquipment RequiredEquipment RequiredEquipment Required
• PC Computer • IWX/214 data acquisition unit
• USB cable
• IWX/214 power supply

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 7
• C-AAMI-504 ECG cable and electrode lead wires
• EM-100 Event marker
• Stethoscope • Alcohol swabs
• Disposable ECG electrodes
Start the SoftwareStart the SoftwareStart the SoftwareStart the Software
Click on the LabScribe LabScribe LabScribe LabScribe shortcut on the computer’s desktop to open the program. If a shortcut is not available, click on the WindoWindoWindoWindows Start menuws Start menuws Start menuws Start menu, move the cursor to All All All All
ProgramsProgramsProgramsPrograms and then to the listing for iWorxiWorxiWorxiWorx. Select LabScribeLabScribeLabScribeLabScribe from the iWorx submenuiWorx submenuiWorx submenuiWorx submenu.
The LabScribe Main windowMain windowMain windowMain window will appear
as the program opens. 1. On the Main windowMain windowMain windowMain window, pull down the Settings menuSettings menuSettings menuSettings menu and select Load GroupLoad GroupLoad GroupLoad Group.
2. Locate the folder that contains the settings group, IPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrp. Select this
group and click OpenOpenOpenOpen. 3. Pull down the Settings menuSettings menuSettings menuSettings menu again. Select the ECGECGECGECG----Heart SoundsHeart SoundsHeart SoundsHeart Sounds----LS2LS2LS2LS2 settings
file.
4. After a short time, LabScribe will appear on the computer screen as configured by the ECGECGECGECG----Heart SoundsHeart SoundsHeart SoundsHeart Sounds----LS2LS2LS2LS2 settings.
ECG Cable and Pulse Transducer SetupECG Cable and Pulse Transducer SetupECG Cable and Pulse Transducer SetupECG Cable and Pulse Transducer Setup 1. Locate the EM-100 event marker and C-AAMI-504 ECG cable and electrode
lead wires in the iWorx kit.
2. Plug the DIN8 connector to the EM-100 into the Channel 3 input of the
IWX/214. 3. Insert the black AAMI connector on the end of the ECG cable into the isolated
inputs of Channels 1 and 2 of the IWX/214.
4. Insert the connectors on the red, black, and green electrode lead wires into the matching sockets on the lead pedestal of the ECG cable.
5. Instruct the subject to remove all jewelry from their wrists and ankles.
6. Use an alcohol swab to clean and scrub a region with little or no hair, on the inside of the subject’s right wrist. Let the area dry.
7. Remove a disposable ECG electrode from its plastic shield, and apply the
electrode to the scrubbed area on the wrist. 8. Repeat Steps 6 and 7 for the inside of the left wrist and the inside of the right
ankle.
9. Snap the lead wires onto the electrodes, so that: • The red (+1) lead is attached to the right wrist
• The black (-1) lead is connected to the left wrist

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 8
• The green (C or ground) lead is connected to the right leg.
10. Instruct the subject to sit quietly with their hands in their lap. If the subject
moves, the ECG trace will move off the top or bottom of the screen. If the subject moves any muscles in the arms or upper body, electromyograms (EMGs)
from the muscles will appear on the ECG recording as noise.
Exercise #1: Exercise #1: Exercise #1: Exercise #1: The ECG in a RestingThe ECG in a RestingThe ECG in a RestingThe ECG in a Resting SubjectSubjectSubjectSubject
Procedure:Procedure:Procedure:Procedure: 1. Click on the Record button, located on the upper right side of the LabScribe
Main window. The signal should begin scrolling across the screen.
2. Click on the AutoScaleAutoScaleAutoScaleAutoScale button at the upper margin of the ECG, Pulse, and Pulse
Integral channels. 3. When you have a suitable trace, type <Subject’s Name><Subject’s Name><Subject’s Name><Subject’s Name> Resting Resting Resting Resting ECG/PulseECG/PulseECG/PulseECG/Pulse in
the Mark boxMark boxMark boxMark box to the right of the Mark buttonMark buttonMark buttonMark button. Press the EnterEnterEnterEnter key on the
keyboard to attach the comment to the data. Record for a minute or two. 4. Click StopStopStopStop to halt recording.
5. Select Save AsSave AsSave AsSave As in the File menuFile menuFile menuFile menu, type a name for the file. Choose a destination on
the computer in which to save the file, like your lab group folder). Designate the file type as *.iwxdata*.iwxdata*.iwxdata*.iwxdata. Click on the SaveSaveSaveSave button to save the data file.
Data AnalysisData AnalysisData AnalysisData Analysis 1. Scroll through the recording and find a section of data with four to six good ECG
cycles in succession.
2. Use the Display Time Display Time Display Time Display Time icons to adjust the Display Time Display Time Display Time Display Time of the Main window Main window Main window Main window to
show at least four complete ECG cycles on the Main windowMain windowMain windowMain window. Four adjacent ECG cycles can also be selected by:
• Placing the cursors on either side of a group of four complete ECG cycles.
• Clicking the Zoom between Cursors Zoom between Cursors Zoom between Cursors Zoom between Cursors button on the LabScribe toolbar to expand the segment with the four selected ECG cycles to the width of the
Main windowMain windowMain windowMain window.
3. Click on the Analysis window Analysis window Analysis window Analysis window icon in the toolbar or select AnalAnalAnalAnalysis ysis ysis ysis from the Windows menu Windows menu Windows menu Windows menu to transfer the data displayed in the Main window Main window Main window Main window to the
Analysis windowAnalysis windowAnalysis windowAnalysis window.
4. Look at the Function Table Function Table Function Table Function Table that is above the uppermost channel displayed in the Analysis Analysis Analysis Analysis window. The names of the mathematical functions used in the analysis,
V2V2V2V2----V1 V1 V1 V1 and T2T2T2T2----T1T1T1T1, appear in this table. The values for V2V2V2V2----V1 V1 V1 V1 and T2T2T2T2----T1T1T1T1 from
each channel are seen in the table across the top margin of each channel. 5. Once the cursors are placed in the correct positions for determining the
amplitudes and the beat period on each ECG cycle, the values of these

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 9
amplitudes and the time interval can be recorded in LabScribe by typing their
names and values directly into the JournalJournalJournalJournal, or on a separate data table.
6. Use the mouse to click on and drag the cursors to specific points on the ECG recording to measure the following:
• The RRRR----wave amplitudewave amplitudewave amplitudewave amplitude. To measure the R wave amplitude, place one cursor on
the Q wave that precedes the R wave and the second cursor on the peak of the R wave. The value for V2V2V2V2----V1 V1 V1 V1 on the ECG ECG ECG ECG channel is this amplitude. Measure the
amplitudes of two additional R waves.
• The PPPP----wave amplitudewave amplitudewave amplitudewave amplitude. To measure the P wave amplitude, place one cursor on the baseline that precedes the P wave and the second cursor on the peak of the P
wave. The value for V2V2V2V2----V1 V1 V1 V1 on the ECG ECG ECG ECG channel is this amplitude. Measure the
amplitudes of two additional P waves.
• The TTTT----wave amplitudewave amplitudewave amplitudewave amplitude. To measure the T wave amplitude, place one cursor on the baseline that precedes a P wave and the second cursor on the peak of the T
wave that is in the same cycle as that P wave. The value for V2V2V2V2----V1 V1 V1 V1 on the ECGECGECGECG
channel is this amplitude. Measure the amplitudes of two additional T waves.
Exercise #2: Exercise #2: Exercise #2: Exercise #2: The ECG The ECG The ECG The ECG and Heart Soundsand Heart Soundsand Heart Soundsand Heart Sounds ProcedureProcedureProcedureProcedure
1. Place the head of the stethoscope on the left side of the subject’s chest and listen
for the heart sounds. Move the stethoscope head to different positions until heart sounds are heard clearly. Heart sounds can also be heard by placing the
stethoscope over the arteries in the neck.
2. Click on the Record Record Record Record button. Hold the stethoscope head on the subject’s chest
with one hand and the event marker in the other. Press the event marker when you hear the “lub”, or first heart sound, and release it when you hear the “dub”,
or second heart sound.
3. After recording for twenty seconds, click Stop Stop Stop Stop to halt recording. 4. Select Save Save Save Save in the File File File File menu on the LabScribe window
Data AnalysisData AnalysisData AnalysisData Analysis 1. Scroll through the recording and find a section of data with four to six
exemplary ECG waveforms and consistent responses on the event marker
channel, in succession. 2. Use the Display Time Display Time Display Time Display Time icons to adjust the Display Time Display Time Display Time Display Time of the Main window Main window Main window Main window to
show at least our complete ECG/heart sound cycles on the Main windowMain windowMain windowMain window. Four
adjacent ECG/heart sound cycles can also be selected by: • Placing the cursors on either side of a group of four complete ECG/heart
sound cycles; and clicking the Zoom between Cursors Zoom between Cursors Zoom between Cursors Zoom between Cursors button on the

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 10
LabScribe toolbar to expand the segment with the four selected ECG/heart
sound cycles to the width of the Main windowMain windowMain windowMain window.
• Click on the Analysis window Analysis window Analysis window Analysis window icon in the toolbar or select Analysis Analysis Analysis Analysis from the Windows menu Windows menu Windows menu Windows menu to transfer the data displayed in the Main window Main window Main window Main window to the
Analysis windowAnalysis windowAnalysis windowAnalysis window.
3. Once the cursors are placed in the correct positions for determining the time intervals on each ECG cycle, the values of these intervals can be recorded by
typing their names and values directly into the JournalJournalJournalJournal, or on a separate data
table. 4. Use the mouse to click on and drag the cursors to specific points on the ECG
recording to measure the following:
• The RRRR----Lub IntervalLub IntervalLub IntervalLub Interval, which is the time interval between the peak of a R wave
and the onset of the event mark. The onset of the event mark indicates the occurrence of the first heart sound or “lub”. Record the value for T2T2T2T2----T1 T1 T1 T1 of
either channel. Measure this time interval for two additional ECG cycles.
• The TTTT----Dub IntervalDub IntervalDub IntervalDub Interval, which is the time interval between the peak of a T wave and the offset of the event mark. The offset of the event mark indicates the
occurrence of the second heart sound or “dub”. Record the value for T2T2T2T2----T1 T1 T1 T1 of
either channel. Measure this time interval for two additional ECG cycles. 5. Calculate the following values and type your results into the JournalJournalJournalJournal
• The average R-Lub interval.
• The average T-Dub interval.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 11
Experiment #Experiment #Experiment #Experiment #2222: : : : Human SpirometryHuman SpirometryHuman SpirometryHuman Spirometry
Part A: Part A: Part A: Part A: Breathing Parameters Breathing Parameters Breathing Parameters Breathing Parameters at Rest and After Exerciseat Rest and After Exerciseat Rest and After Exerciseat Rest and After Exercise ObjectivesObjectivesObjectivesObjectives
• Measure the breathing parameters at rest
• Measure the breathing parameters after exercise
BackgroundBackgroundBackgroundBackground The amount of air that moves in or out of the lungs during any one breathing cycle is
called the tidal volume. After normal inspiration, it is possible to breathe in additional
air—this is called the inspiratory reserve volume. Similarly, after a normal expiration, it
is possible to exhale additional air from the lungs—this is the expiratory reserve volume. Even if the expiratory reserve volume is fully expelled from the lungs, there is
still a volume of air in the lungs, called the residual volume, that cannot be exhaled. The
residual volume has low oxygen and high carbon dioxide concentrations. Upon inhalation, fresh air mixes with stale air from the residual volume to create air in the
alveoli that still has oxygen and carbon dioxide concentrations that facilitate the
diffusion of O2 into and CO2 out of the capillaries. The respiration center in the medulla insures that gaseous exchange at the lung matches the requirements of the body. During
times of increased demand, the tidal volume can be increased, using some of the reserve
lung volumes to bring more fresh air into the body. In addition, the rate of breathing and the rate of air movement in and out of the lungs can be changed.
Equipment RequiredEquipment RequiredEquipment RequiredEquipment Required • PC Computer
• IWX/214 data acquisition unit
• USB cable
• IWX/214 power supply • SP-304 Spirometer
• FH-300 Spirometer flow head and plastic tubes
Start the SoftwareStart the SoftwareStart the SoftwareStart the Software
1. Click on the LabScribe shortcut on the computer’s desktop to open the program. If a shortcut is not available, click on the Windows Start menuStart menuStart menuStart menu, move the cursor
to All ProgramsAll ProgramsAll ProgramsAll Programs and then to the listing for iWorxiWorxiWorxiWorx. Select LabScribe LabScribe LabScribe LabScribe from the
iWorx submenuiWorx submenuiWorx submenuiWorx submenu. The LabScribe MainMainMainMain window window window window will appear as the program opens. 2. On the Main windowMain windowMain windowMain window, pull down the Settings menu Settings menu Settings menu Settings menu and select Load Group.Load Group.Load Group.Load Group.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 12
3. Locate the folder that contains the settings group, IPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrp. Select this
group and click OpenOpenOpenOpen.
4. Pull down the Settings menu Settings menu Settings menu Settings menu again. Select the BreathingBreathingBreathingBreathing---- RestRestRestRest----ExerciseExerciseExerciseExercise----LS2 LS2 LS2 LS2 settings file.
5. After a short time, LabScribe will appear on the computer screen as configured
by the BreathingBreathingBreathingBreathing----RestRestRestRest----ExerciseExerciseExerciseExercise----LS2LS2LS2LS2 settings. Spirometer SetupSpirometer SetupSpirometer SetupSpirometer Setup
1. Locate the SP-304 spirometer, the FH-300, and the airflow tubing in the iWorx
kit. 2. Firmly push the two air flow tubes onto the two outlets on the FH-300 flow
head.
3. Firmly push the other ends of the two air flow tubes onto the two outlets on the
SP-304 spirometer unit. 4. Plug the DIN8 connector to the SP-304 spirometer into the Channel 4 input of
the IWX/214.
Before StartingBefore StartingBefore StartingBefore Starting
1. Please read the procedures for each exercise completely before beginning the
experiment. You should have a good understanding of how to perform these exercises before making recordings.
2. The spirometer will monitor breathing from a subject. It is important that the
subject is healthy and has no history of respiratory or cardiovascular problems. 3. On the flow head, the outlets connected to the airflow tubing should always be
pointed up to avoid problems with condensation developing within the tubing.
4. To reduce turbulence within the flowhead, place a disposable cardboard mouthpiece that contains a screen, over the opening of the flowhead.
5. Use a clip to prevent air from entering or leaving the nose as the subject is
breathing. Air that passes through the nose is not included in the volume
measurements and causes errors in these values. 6. The settings file, BreathingBreathingBreathingBreathing----RestRestRestRest----ExerciseExerciseExerciseExercise----LS2LS2LS2LS2, programs LabScribe to record the
breathing of the subject on the Air Flow channAir Flow channAir Flow channAir Flow channelelelel. The computed function used
on the VolumeVolumeVolumeVolume channel converts the data recorded on the Air FlowAir FlowAir FlowAir Flow channel to lung volume measurements.
7. Enter the calibration voltage of your SP-304 spirometer into the Spirometry Spirometry Spirometry Spirometry
computed function used on the VolumeVolumeVolumeVolume channel: • Click on the words Spirometry (AirFlow)Spirometry (AirFlow)Spirometry (AirFlow)Spirometry (AirFlow), that are next to the title of the
Volume Volume Volume Volume channel, to open the computed function pullcomputed function pullcomputed function pullcomputed function pull----down menudown menudown menudown menu.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 13
• Select Setup Setup Setup Setup from this pull-down menu to open the Spirometer Calibration Spirometer Calibration Spirometer Calibration Spirometer Calibration
Dialog windowDialog windowDialog windowDialog window.
• Enter the calibration voltagecalibration voltagecalibration voltagecalibration voltage, that is listed on the label of your SP-304 spirometer unit, into the equation that sets the calibration voltage equal to
one liter of lung volume.
• Make sure the reset time reset time reset time reset time is set to 60 sec60 sec60 sec60 sec, and the first 5 seconds 5 seconds 5 seconds 5 seconds of the recording are used to zero the baseline of the Volume Volume Volume Volume channel. Click OKOKOKOK.
8. Allow the SP-304 to warm up for 10 minutes before recording for the first time.
9. When spirometry data is recorded in the conventional manner, inhalation is always displayed as an upward deflection. To determine if the subject is
breathing through the correct end of the flow head.
• Click on the Save to Disk Save to Disk Save to Disk Save to Disk button in the lower left corner of the Main window Main window Main window Main window to
switch the LabScribe software into Preview modePreview modePreview modePreview mode. When LabScribe is in Preview modePreview modePreview modePreview mode, there is a red X red X red X red X across the SaSaSaSave to Disk ve to Disk ve to Disk ve to Disk button. In Preview modePreview modePreview modePreview mode,
the iWorx recording system works without recording data on the hard drive or
any other storage media which allows a subject to become comfortable with breathing through a spirometer.
• Click on the Preview Preview Preview Preview
button. Have the subject inhale through the spirometer flowhead. Click on the AutoScale AutoScale AutoScale AutoScale button at the upper margin of the Air Flow Air Flow Air Flow Air Flow and Volume Volume Volume Volume channels. If
the flowhead is oriented properly, the traces on the Air Flow Air Flow Air Flow Air Flow and Volume Volume Volume Volume
channels will go up during inhalation. If the traces onthese channels go down during inhalation, have the subject breathe through the other end of the
flowhead, or reverse the positions of the airflow tubes at the outlets of the
flowhead.
10. Click on the Stop Stop Stop Stop button. 11. Before proceeding to the actual exercises, make sure the LabScribe software in
set to Record modeRecord modeRecord modeRecord mode. Click on the Save to Disk Save to Disk Save to Disk Save to Disk button, in the lower left corner of
the MainMainMainMain windowwindowwindowwindow, to change LabScribe from Preview Preview Preview Preview mode to Record Record Record Record mode. When LabScribe is in Record Record Record Record mode, there is a green arrow green arrow green arrow green arrow on the Save to Disk Save to Disk Save to Disk Save to Disk
button.
Exercise #1: Breathing while Exercise #1: Breathing while Exercise #1: Breathing while Exercise #1: Breathing while RestingRestingRestingResting (While Sitting)(While Sitting)(While Sitting)(While Sitting)
Procedure:Procedure:Procedure:Procedure: 1. Instruct the subject to:
• Sit quietly and become accustomed to breathing through the spirometer
flowhead. • Breathe normally before any recordings are made.
• Hold the flowhead so that its outlets are pointed up.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 14
• Remove the flowhead from his or her mouth and hold it at the mouth level in a
position that prevents a breath from moving through the flowhead.
2. Type <Subject’s Name> Resting <Subject’s Name> Resting <Subject’s Name> Resting <Subject’s Name> Resting in the Mark box Mark box Mark box Mark box that is to the right of the Mark Mark Mark Mark button.
3. Click on the Record Record Record Record button. After waiting five seconds for the Volume Volume Volume Volume channel
to zero, have the subject place the flowhead in his or her mouth and begin breathing. Press the Enter Enter Enter Enter key on the keyboard to mark the recording.
4. Click the AutAutAutAutoScale oScale oScale oScale buttons of the Air Flow Air Flow Air Flow Air Flow and VolumeVolumeVolumeVolume channels. Notice the
slowly moving wave on the VolumeVolumeVolumeVolume channel. Record five breaths, which normally takes about forty-five seconds to record. Every sixty seconds into the
recording, the baseline of the Volume Volume Volume Volume channel automatically resets itself to zero,
which has no impact on the data being recorded.
5. Type Forced Forced Forced Forced in the Mark boxMark boxMark boxMark box. Press the Enter Enter Enter Enter key on the keyboard as the subject inhales as deeply as possible. After reaching his or her maximum inhalation
volume, the subject should exhale as quickly and as completely as possible.
6. After the forced exhalation is complete, the subject should continue to breathe normally through the spirometer for five breath cycles.
7. Click Stop Stop Stop Stop to halt recording.
8. Select Save As Save As Save As Save As in the File File File File menumenumenumenu, type a name for the file. Choose a destination on the computer in which to save the file, like your lab group folder). Designate the
file type as
*.iwxdata*.iwxdata*.iwxdata*.iwxdata. Click on the Save Save Save Save button to save the data file.
Data AnalysisData AnalysisData AnalysisData Analysis (Normal Breathing at Rest)(Normal Breathing at Rest)(Normal Breathing at Rest)(Normal Breathing at Rest) 1. Scroll through the recording and find the section of data recorded when the
subject was breathing while restingrestingrestingresting.
2. Use the Display Time Display Time Display Time Display Time icons to adjust the Display Time Display Time Display Time Display Time of the Main window Main window Main window Main window to show at least four complete breathing cycles on the Main windowMain windowMain windowMain window. Four adjacent
breathing cycles can also be selected by:
• Placing the cursors on either side of a group of four complete breathing cycles • Clicking the Zoom between Cursors Zoom between Cursors Zoom between Cursors Zoom between Cursors button on the LabScribe toolbar to expand
the four selected breathing cycles to the width of the Main windowMain windowMain windowMain window.
3. Click on the Analysis window Analysis window Analysis window Analysis window icon in the toolbar or select Analysis Analysis Analysis Analysis from the Windows menuWindows menuWindows menuWindows menu to transfer the data displayed in the Main window Main window Main window Main window to the
Analysis windowAnalysis windowAnalysis windowAnalysis window.
4. Look at the Function Table Function Table Function Table Function Table that is above the uppermost channel displayed in the AnalysisAnalysisAnalysisAnalysis window. The mathematical functions, V2V2V2V2----V1V1V1V1, Max_dv/dtMax_dv/dtMax_dv/dtMax_dv/dt, Min_dv/dtMin_dv/dtMin_dv/dtMin_dv/dt,
and T2T2T2T2----T1T1T1T1 should appear in this table. Values for V2V2V2V2----V1V1V1V1, Max_dv/dtMax_dv/dtMax_dv/dtMax_dv/dt, Min_dv/dtMin_dv/dtMin_dv/dtMin_dv/dt,

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 15
and T2T2T2T2----T1 T1 T1 T1 on each channel are seen in the table across the top margin of each
channel.
5. Minimize the height of the Air Flow channel Air Flow channel Air Flow channel Air Flow channel by clicking on the arrow to the left of the channel’s title to open the channel menuchannel menuchannel menuchannel menu. Select Minimize Minimize Minimize Minimize from this menu
to reduce the height of the channel display.
6. Maximize the height of the trace on the Volume channel Volume channel Volume channel Volume channel by clicking on the arrow to the left of the channel’s title to open the channel menuchannel menuchannel menuchannel menu. Select Scale Scale Scale Scale
from the menu and AutoScaleAutoScaleAutoScaleAutoScale from the Scale submenu Scale submenu Scale submenu Scale submenu to increase the height of
the data on that channel. 7. Once the cursors are placed in the correct positions for determining the volumes
and rates of each breath cycle, the values of the parameters in the Function Function Function Function
Table Table Table Table can be recorded in the on-line notebook of LabScribe by typing their
names and values directly into the JournalJournalJournalJournal. 8. On the Volume Volume Volume Volume channel, use the mouse to click on and drag the cursors to
specific points on the recording to measure the following volumes:
• Tidal Volume Tidal Volume Tidal Volume Tidal Volume (TVTVTVTV), which is the volume of air inhaled or exhaled during a normal breathing cycle. To measure the tidal volume of the subject during
breathing at rest, place one cursor in the trough prior to inhalation, and the
second cursor on the peak of the cycle. The value for the V2V2V2V2----V1 V1 V1 V1 function on the Volume channel Volume channel Volume channel Volume channel is the tidal volume.
• Maximum Inspiratory Flow RateMaximum Inspiratory Flow RateMaximum Inspiratory Flow RateMaximum Inspiratory Flow Rate, which is the maximum rate of air
movement during inhalation. To measure the maximum inspiratory flow rate of the subject during breathing at rest, leave the cursors in the same positions
used to measure the tidal volume. The value for the Max_dv/dtMax_dv/dtMax_dv/dtMax_dv/dt function on
the Volume channel Volume channel Volume channel Volume channel is the maximum inspiratory flow rate of that breath
cycle. • Maximum Expiratory Flow RateMaximum Expiratory Flow RateMaximum Expiratory Flow RateMaximum Expiratory Flow Rate, which is the maximum rate of air
movement during exhalation. To measure the maximum expiratory flow rate
of the subject during breathing at rest, place one cursor on the peak of the breath cycle, and the second cursor in the trough to the right of that peak.
The value for the Min_dv/dt Min_dv/dt Min_dv/dt Min_dv/dt function on the Volume channel Volume channel Volume channel Volume channel is the
maximum expiratory flow rate of that breath cycle. This function is used since the exhalation portion of the breath cycle has a negative slope.
• Breath PeriodBreath PeriodBreath PeriodBreath Period, which is the duration of each breathing cycle. To measure the
breath period of the subject during breathing at rest, place one cursor on a peak of a breath cycle, and the second cursor on the peak of an adjacent
cycle. The value for T2T2T2T2----T1 T1 T1 T1 on the Volume channel Volume channel Volume channel Volume channel is the period of that
breath cycle.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 16
9. Repeat the measurements of tidal volume, maximum inspiratory flow rate,
maximum expiratory flow rate, and breath period on two additional normal
breath cycles. 10. Average the three values obtained for each parameter....
11. Record the means for the tidal volume, rates, and breath period.
12. Calculate the normal breathing rate of the subject at rest using the following equation:
13. Multiply the mean tidal volume by the breathing rate to calculate the volume of
air passing in and out of the resting subject’s lungs each minute. 14. Record the values for these calculations.
Data AnalysisData AnalysisData AnalysisData Analysis (Forced Expiration at Rest)(Forced Expiration at Rest)(Forced Expiration at Rest)(Forced Expiration at Rest) 1. Use the slider or the arrows on the scroll bar, at the bottom of the AnaAnaAnaAnalysis lysis lysis lysis
window, to position data recorded when the subject exhaled with maximum
force in the window.
2. Use the Display Time Display Time Display Time Display Time icons to adjust the Display Time Display Time Display Time Display Time of the Analysis window Analysis window Analysis window Analysis window to show the forced expiration curve and the two normal breaths, that occur before
the force expiration curve, on the same window. These breathing cycles can also
be selected by: • Placing the cursors on either side of the group of appropriate breathing cycles.
• Clicking the Zoom between Cursors Zoom between Cursors Zoom between Cursors Zoom between Cursors button on the LabScribe toolbar to expand
the selected breathing cycles to the width of the Main windowMain windowMain windowMain window. 3. Place the cursors on the forced expiration data displayed on the Volume Volume Volume Volume channel
to measure the following volumes and rates using the V2V2V2V2----V1V1V1V1, T2T2T2T2----T1T1T1T1, Max_dv/dtMax_dv/dtMax_dv/dtMax_dv/dt,
and Min_dv/dtMin_dv/dtMin_dv/dtMin_dv/dt functions. The volumes and rates that you will measure: • Tidal Volume Tidal Volume Tidal Volume Tidal Volume (TVTVTVTV), by placing one cursor in the trough before the inhalation
segment of the resting breath and the second cursor on the peak of that resting
breath cycle. The value for the V2V2V2V2----V1V1V1V1 function on the Volume chanVolume chanVolume chanVolume channel nel nel nel is the
tidal volume. • Inspiratory Reserve Volume Inspiratory Reserve Volume Inspiratory Reserve Volume Inspiratory Reserve Volume (IRVIRVIRVIRV), by placing one cursor on the peak of the
normal breath prior to the maximum inhalation and the second cursor on the
peak of the forced breath cycle. The value for the V2V2V2V2----V1 V1 V1 V1 function on the VolumeVolumeVolumeVolume cccchannel hannel hannel hannel is the inspiratory reserve volume.
• Forced Inspiratory Flow RateForced Inspiratory Flow RateForced Inspiratory Flow RateForced Inspiratory Flow Rate, by keeping the cursors in the same positions used
for measuring IRVIRVIRVIRV. The value for the Max_dv/dt Max_dv/dt Max_dv/dt Max_dv/dt function on the Volume Volume Volume Volume channel channel channel channel is the forced inspiratory flow rate.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 17
• Forced Vital CapaciForced Vital CapaciForced Vital CapaciForced Vital Capacity ty ty ty (FVCFVCFVCFVC), by placing one cursor on the peak of the forced
breath cycle and the second cursor on the flat line after the subject has expelled
all the air from his or her lungs. The value for the V2V2V2V2----V1 V1 V1 V1 function on the VolumeVolumeVolumeVolume channel channel channel channel is the forced vital capacity.
• Forced Expiratory Flow RateForced Expiratory Flow RateForced Expiratory Flow RateForced Expiratory Flow Rate, by keeping the cursors in the same positions used
for measuring VCVCVCVC.The value for the Min_dv/dt Min_dv/dt Min_dv/dt Min_dv/dt function on the Volume channel Volume channel Volume channel Volume channel is the forced expiratory flow rate.
• Expiratory Reserve Volume Expiratory Reserve Volume Expiratory Reserve Volume Expiratory Reserve Volume (ERVERVERVERV), by placing one cursor in the trough before
maximal inhalation and the second cursor on the flat line after subject has expelled all the air from his or her lungs. The value for the V2V2V2V2----V1 V1 V1 V1 function on
the VolumeVolumeVolumeVolume channel channel channel channel is the expiratory reserve volume.
• Forced Expiratory Volume at 1 SForced Expiratory Volume at 1 SForced Expiratory Volume at 1 SForced Expiratory Volume at 1 Second econd econd econd (FEV1FEV1FEV1FEV1), by placing one cursor on the
peak of the maximum breath cycle and the second cursor on the data point that is one second after the peak. Use the T2T2T2T2----T1 T1 T1 T1 function to determine the data point
that is one second after the peak. The value for the VVVV2222----V1 V1 V1 V1 function on the
Volume channel Volume channel Volume channel Volume channel is the forced expiratory volume at one second. • Forced Expiratory Volume at 3 Seconds Forced Expiratory Volume at 3 Seconds Forced Expiratory Volume at 3 Seconds Forced Expiratory Volume at 3 Seconds (FEV3FEV3FEV3FEV3), by placing one cursor on the
peak of the maximum breath cycle and the second cursor on the data point that
is three seconds after the peak. Use the T2T2T2T2----T1 T1 T1 T1 function to determine the data point that is three seconds after the peak. The value for the V2V2V2V2----V1 V1 V1 V1 function on
the Volume channel Volume channel Volume channel Volume channel is the forced expiratory volume at three seconds.
4. Record these volumes and rates. 5. Calculate the subject’s FEV1/FVC ratio by dividing the subject’s FEV1 value by
his or her FVC value.
6. Calculate the subject’s FEV3/FVC ratio by dividing the subject’s FEV3 value by
his or her FVC value. 7. Compare the FEV1/FVC and FEV3/FVC ratios of the subject to the normal
values of 0.80 and 0.95, respectively, for young healthy adults. Both of these
ratios decrease with age. • In obstructive airway diseases, like asthma, bronchitis, or emphysema, both FVC
and FEV1 are reduced, and FEV1/FVC ratios are usually less than 0.70.
• In restrictive lung diseases, like fibrosis, FVC is reduced. But, because of the low compliance and high recoil of the lungs, the FEV1/FVC ratio may be normal
(~0.80) or greater than normal (>0.85).
8. Record the FEV1/FVC and FEV3/FVC ratios. 9. Record the volumes, rates, and ratios from your subject in the table being
compiled for all the subjects in the class.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 18
Exercise #2: Breathing Immediately after ExerciseExercise #2: Breathing Immediately after ExerciseExercise #2: Breathing Immediately after ExerciseExercise #2: Breathing Immediately after Exercise
Procedure:Procedure:Procedure:Procedure:
1. In this exercise, use the same healthy subject whose breathing parameters at rest were measured in Exercise 1.
2. Type After Exercise After Exercise After Exercise After Exercise in the Mark box Mark box Mark box Mark box to the right of the Mark Mark Mark Mark button.
3. The subject should exercise to sufficiently elevate breathing rate, but with minimal class disruption. Running up and down flights of stairs is a good
method. The subject should sit down after the exercise period.
4. Click on the Record Record Record Record button. After waiting five seconds for the Volume Volume Volume Volume channel to zero, have the subject place the flowhead in his or her mouth and begin
breathing. Press the Enter Enter Enter Enter key on the keyboard to mark the recording.
5. Click the AutoScale AutoScale AutoScale AutoScale buttons of the Air Flow Air Flow Air Flow Air Flow and VolumeVolumeVolumeVolume channels. Record at
least five breaths as the subject is recovering from exercise. Remember the baseline of the Volume Volume Volume Volume channel automatically resets every sixty seconds.
6. Type Forced Forced Forced Forced in the Mark boxMark boxMark boxMark box. Press the Enter Enter Enter Enter key on the keyboard as the subject
inhales as deeply as possible. After reaching his or her maximum inhalation volume, the subject should exhale as quickly and as completely as possible.
7. The subject should return to breathing as normally as possible through the
spirometer. 8. Click Stop Stop Stop Stop to halt recording.
9. Select Save As Save As Save As Save As in the File menuFile menuFile menuFile menu, type a name for the file. Choose a destination on
the computer in which to save the file, like your lab group folder). Designate the file type as *.*.*.*.iwxdataiwxdataiwxdataiwxdata. Click on the Save Save Save Save button to save the data file.
Data AnalysisData AnalysisData AnalysisData Analysis
Perform the same types of measurements on the data recorded in exercise #1.
Part Part Part Part BBBB: : : : Factors that Affect Breathing PatternsFactors that Affect Breathing PatternsFactors that Affect Breathing PatternsFactors that Affect Breathing Patterns
ObjectivesObjectivesObjectivesObjectives • Study any changes in breathing patterns due to standing.
• Study any changes in breathing patterns due to sitting up.
BackgroundBackgroundBackgroundBackground
The respiratory control center in the medulla is responsible for matching the amount of
O2 used and CO2 produced by tissues with the amount of O2 taken up and CO2 discharged by the lungs. Lung ventilation can be influenced by many factors, including
emotion, speech, disease, and body position. This latter factor was the focus of the last
exercise. In this experiment, students will examine how other factors, like concentrating on the completion of a task or sitting up quickly, influence breathing.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 19
Equipment RequiredEquipment RequiredEquipment RequiredEquipment Required
• PC Computer • IWX/214 data acquisition unit
• USB cable
• IWX/214 power supply • SP-304 Spirometer
• FH-300 Spirometer flow head and plastic tubes
• Needle and thread • 18-24” of plastic tubing that fits over the end of flowhead
Start the SoftwareStart the SoftwareStart the SoftwareStart the Software
1. Click on the LabScribe shortcut on the computer’s desktop to open the program.
If a shortcut is not available, click on the Windows Start menuStart menuStart menuStart menu, move the cursor to All ProgramsAll ProgramsAll ProgramsAll Programs and then to the listing for iWorxiWorxiWorxiWorx. Select LabScribe LabScribe LabScribe LabScribe from the
iWorx submenuiWorx submenuiWorx submenuiWorx submenu. The LabScribe Main window Main window Main window Main window will appear as the program opens.
2. On the Main windowMain windowMain windowMain window, pull down the Settings menu Settings menu Settings menu Settings menu and select Load Group.Load Group.Load Group.Load Group. 3. Locate the folder that contains the settings group, IPLMv4.IPLMv4.IPLMv4.IPLMv4.iwxgrpiwxgrpiwxgrpiwxgrp. Select this
group and click OpenOpenOpenOpen.
4. Pull down the Settings menu Settings menu Settings menu Settings menu again. Select the BreathingBreathingBreathingBreathing---- OtherFactorsOtherFactorsOtherFactorsOtherFactors----LS2 LS2 LS2 LS2 settings file.
5. After a short time, LabScribe will appear on the computer screen as configured
by the BreathingBreathingBreathingBreathing----OtherFactorsOtherFactorsOtherFactorsOtherFactors----LS2LS2LS2LS2 settings.
SSSSpirometer Setuppirometer Setuppirometer Setuppirometer Setup
1. Locate the SP-304 spirometer, the FH-300, the airflow tubing. 2. Firmly push the two air flow tubes onto the two outlets on the FH-300 flow
head.
3. Firmly push the other ends of the two air flow tubes onto the two outlets on the
SP-304 spirometer unit. 4. Plug the DIN8 connector to the SP-304 spirometer into the Channel 4input of
the iWX/214.
Before StartingBefore StartingBefore StartingBefore Starting
1. Please read the procedures for each exercise completely before beginning the
experiment. You should have a good understanding of how to perform these exercises before making recordings.
2. The spirometer will monitor breathing from a subject. It is important that the
subject is healthy and has no history of respiratory or cardiovascular problems.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 20
3. The outlets on the flow head should always be in the upright position to avoid
problems with condensation developing in the airflow tubes.
4. Turbulence in the flow head will produce a noisy signal. To reduce turbulence, the subject should place his or her lips around the outside of the opening of the
flowhead, or around the cardboard mouthpiece or bacterial filter attached to the
flowhead. 5. Use a clip to prevent air from entering or leaving the nose as the subject is
breathing. air that passes through the nose is not included in the volume
measurements and causes errors in these values. 6. The settings file, BreathingBreathingBreathingBreathing----OtherFactorsOtherFactorsOtherFactorsOtherFactors----LS2LS2LS2LS2, programs LabScribe to record the
breathing of the subject on the Air Flow channelAir Flow channelAir Flow channelAir Flow channel. A computed function is
programmed on the Volume channel Volume channel Volume channel Volume channel to convert the data recorded on the Air FloAir FloAir FloAir Flow w w w
channel to lung volume measurement. 7. Enter the calibration voltage of your SP-304 spirometer into the Spirometry Spirometry Spirometry Spirometry
computed function used on the VolumeVolumeVolumeVolume channel:
• Click on the words Spirometry (AirFlow)Spirometry (AirFlow)Spirometry (AirFlow)Spirometry (AirFlow), that are next to the title of the Volume Volume Volume Volume channel, to open the computed function pullcomputed function pullcomputed function pullcomputed function pull----down menudown menudown menudown menu.
• Select Setup Setup Setup Setup from this pull-down menu to open the Spirometer Calibration Spirometer Calibration Spirometer Calibration Spirometer Calibration
Dialog windowDialog windowDialog windowDialog window. • Enter the calibration voltagecalibration voltagecalibration voltagecalibration voltage, that is listed on the label of your SP-304
spirometer unit, into the equation that sets the calibration voltage equal to one
liter of lung volume. • Make sure the reset time reset time reset time reset time is set to 60 sec60 sec60 sec60 sec, and the first 5 seconds 5 seconds 5 seconds 5 seconds of the recording
are used to zero the baseline of the Volume Volume Volume Volume channel. Click OKOKOKOK.
8. Allow the SP-304 to warm up for 10 minutes before recording for the first time.
9. When spirometry data is recorded in the conventional manner, inhalation is always displayed as an upward deflection. To determine if the subject is breathing through
the correct end of the flow head.
• Click on the Save to Disk Save to Disk Save to Disk Save to Disk button in the lower left corner of the Main window Main window Main window Main window to switch the LabScribe software into Preview modePreview modePreview modePreview mode. When LabScribe is in
Preview modePreview modePreview modePreview mode, there is a red X red X red X red X cross the Save to Disk Save to Disk Save to Disk Save to Disk button. In Preview modePreview modePreview modePreview mode,
the iWorx recording system works without recording data on the hard drive or any other storage media which allows a subject to become comfortable with
breathing through a spirometer.
• Click on the Preview Preview Preview Preview button. Have the subject inhale through the spirometer flowhead. Click on the AutoScale AutoScale AutoScale AutoScale button at the upper margin of the Air Flow Air Flow Air Flow Air Flow
and Volume Volume Volume Volume channels. If the flowhead is oriented properly, the traces on the Air Air Air Air
Flow Flow Flow Flow and Volume Volume Volume Volume channels will go up during inhalation. If the traces on these channels go down during inhalation, have the subject breathe through the other

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 21
end of the flowhead, or reverse the positions of the airflow tubes at the outlets of
the flowhead.
10. Click on the Stop Stop Stop Stop button. 11. Before proceeding to the actual exercises, make sure the LabScribe software in set
to Record modeRecord modeRecord modeRecord mode. Click on the Save to Disk Save to Disk Save to Disk Save to Disk button, in the lower left corner of the
Main windowMain windowMain windowMain window, to change LabScribe from Preview Preview Preview Preview mode to Record Record Record Record mode. When LabScribe is in Record Record Record Record mode, there is a green arrow green arrow green arrow green arrow on the Save to Disk Save to Disk Save to Disk Save to Disk button.
Breathing While StandingBreathing While StandingBreathing While StandingBreathing While Standing
Repeat the same steps in Exercise 1 (BreaBreaBreaBreathing while thing while thing while thing while RestingRestingRestingResting (While Sitting)) (While Sitting)) (While Sitting)) (While Sitting)) while the
subject is standing.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 22
Experiment #Experiment #Experiment #Experiment #3333: : : : Human MuscleHuman MuscleHuman MuscleHuman Muscle
Part One: Grip Strength and Electromyogram (EMG) ActivityPart One: Grip Strength and Electromyogram (EMG) ActivityPart One: Grip Strength and Electromyogram (EMG) ActivityPart One: Grip Strength and Electromyogram (EMG) Activity
ObjectivesObjectivesObjectivesObjectives • Measure a subject’s grip strength and record EMG activity of the forearm
muscles used to generate the subject’s grip a by using a hand dynamometer for
the dominant and non-dominant forearms.. • Relate the EMG activity will be to the grip strength by plotting the maximum
grip strength as a function the area under the absolute integral of the EMG
activity during the muscle contraction. • Determine the rate of fatigue in the dominant and non-dominant forearms.
BackgroundBackgroundBackgroundBackground
A motor unit is composed of a motor neuron and all the muscle fibers that are innervated by that motor neuron. In a persistent muscle contraction, multiple motor
units are firing repetitively throughout the contraction of the muscle. The strength of a
muscle contraction is related to the number of motor units in the muscle that are activated during the same time period. The electromyogram (EMG) recorded during the
muscle contraction is seen as a burst of spike-like signals, and the duration of the burst
is about equal to the duration of the muscle contraction. The strength of a striated muscle contraction is directly proportional to the amount of
electrical activity in the muscle. However, it is difficult to quantify the amount of
electrical activity in a muscle unless the raw EMG data is mathematically transformed. One of the most common transformations used is the integration of the absolute values
of the amplitudes of the EMG spikes. Through this transformation, it has been found
that the area under the graph of the absolute integral of the EMG is
linearly proportional to the strength of the muscle contraction.
Equipment RequiredEquipment RequiredEquipment RequiredEquipment Required • PC Computer
• IWX/214 data acquisition unit
• USB cable • IWX/214 power supply
• C-AAMI-504 ECG cable and electrode lead wires
• Disposable electrodes • FT-325 Hand Dynamometer
• Alcohol swabs

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 23
• Bathroom scale and 5 or 6 textbooks
• String
• Metric Ruler
Start the SoftwareStart the SoftwareStart the SoftwareStart the Software
1. Click on the LabScribe shortcut on the computer’s desktop to open the program. If a shortcut is not available, click on the Windows Start menuStart menuStart menuStart menu, move the cursor to
All ProgramsAll ProgramsAll ProgramsAll Programs and then to the listing for iWorxiWorxiWorxiWorx. Select LabScribe LabScribe LabScribe LabScribe from the iWorx iWorx iWorx iWorx
submenusubmenusubmenusubmenu. The LabScribe Main window Main window Main window Main window will appear as the program opens. 2. On the Main windowMain windowMain windowMain window, pull down the Settings menu Settings menu Settings menu Settings menu and select Load Group.Load Group.Load Group.Load Group.
3. Locate the folder that contains the settings group, IPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrp. Select this group
and click OpenOpenOpenOpen.
4. Pull down the Settings menu Settings menu Settings menu Settings menu again. Select the EMGGripStrengthEMGGripStrengthEMGGripStrengthEMGGripStrength----LS2 LS2 LS2 LS2 settings file. 5. After a short time, LabScribe will appear on the computer screen as configured by
the EMGEMGEMGEMG----GripStrengthGripStrengthGripStrengthGripStrength----LS2LS2LS2LS2 settings. EMG Cable and Hand Dynamometer SetupEMG Cable and Hand Dynamometer SetupEMG Cable and Hand Dynamometer SetupEMG Cable and Hand Dynamometer Setup 1. Locate the C-AAMI-504 EMG cable and electrode lead wires and FT-325 hand
dynamometer in the iWorx kit.
2. Plug the DIN8 connector to the FT-325 hand dynamometer into the Channel 3 input of the IWX/214.
3. Insert the black AAMI connector on the end of the EMG cable into the isolated
inputs of Channels 1 and 2 of the IWX/214. 4. Insert the connectors on the red, black, and green electrode lead wires into the
matching sockets on the lead pedestal of the EMG cable.
5. The subject should remove all jewelry from their wrists. For the first exercises in this lab, record EMGs and muscle forces from the subject’s dominant arm, the arm
used most often.
6. Use an alcohol swab to clean and scrub three regions on the inside of the subject’s
dominant forearm where the electrodes will be placed. One area is near the wrist, the second is in the middle of the forearm, and the third area is about 2 inches from
the elbow.
7. Let the areas dry before attaching the electrodes. 8. Remove the plastic disk from a disposable electrode and apply it to one of the
scrubbed areas. Repeat for the other two areas.
9. Snap the lead wires onto the electrodes, so that: • the red “+1” lead is attached to the electrode near the elbow.
• the black “-1” lead is attached to the electrode in the middle of the forearm.
• the green “C” lead (the ground) is attached to the electrode on the wrist.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 24
Calibrating the Hand DynamometerCalibrating the Hand DynamometerCalibrating the Hand DynamometerCalibrating the Hand Dynamometer
1. Collect 5 textbooks. Weigh the stack of books on the bathroom scale. Record the
weight of the stack in kilograms (kg) in the JournalJournalJournalJournal. To open the JournalJournalJournalJournal, click on the JournJournJournJournal al al al button in the LabScribe toolbar. Use the keyboard to type the weight of the
stack in the Journal Journal Journal Journal window.
2. Lay the hand dynamometer down on the bench top. Click the Record Record Record Record button on the LabScribe Main Main Main Main window and record for ten seconds.
3. Continue to record as you stack the textbooks on the bulb of the hand dynamometer.
Record for an additional ten seconds after the last book is placed on the stack. Click the Stop Stop Stop Stop button.
4. Click the AutoScale AutoScale AutoScale AutoScale button on the Muscle Force Muscle Force Muscle Force Muscle Force channel. Use the Double Display Double Display Double Display Double Display
Time Time Time Time icon to adjust the Display Time Display Time Display Time Display Time of the Main window Main window Main window Main window to display the force
recording before and after the books were placed on the hand dynamometer. 5. Click on the Double Cursors button Double Cursors button Double Cursors button Double Cursors button on the LabScribe toolbar. Place one cursor on
the force recording made before the books were placed on the bulb. Place the other
cursor on the recording after the books were placed on the bulb. 6. Open the Channel Menu Channel Menu Channel Menu Channel Menu of the Muscle Force Muscle Force Muscle Force Muscle Force channel by clicking on the down arrow down arrow down arrow down arrow
to the left of the channels’s title. Select Units Units Units Units from this menu and Simple Simple Simple Simple from the
submenu to open the Simple Units Conversion dialogue windowSimple Units Conversion dialogue windowSimple Units Conversion dialogue windowSimple Units Conversion dialogue window. 7. Put check marks in the boxes next to Apply Units to new data Apply Units to new data Apply Units to new data Apply Units to new data and Apply Units to all Apply Units to all Apply Units to all Apply Units to all
blocksblocksblocksblocks. Click on the Units Off button Units Off button Units Off button Units Off button to remove any prior units conversion from this
channel. 8. In the middle of the window is an array of four boxes. For each cursor, the value in
the box on the left is the voltage at the position of the cursor on the recording
window. In the box on the right, enter the value of the unit that equals the voltage on the left:
• For Cursor 1, type zero (0) zero (0) zero (0) zero (0) in the box on the right. this cursor is on the portion
of the recording when no weight was placed on top of the hand dynamometer.
• For Cursor 2, type the weight of the stack of books in the box on the right • Type the name of the unit, kilogram kilogram kilogram kilogram or kgkgkgkg, in the Unit NameUnit NameUnit NameUnit Name box. Click the OK OK OK OK
button.
Exercise#Exercise#Exercise#Exercise#1: EMG Intensity and Force in Dominant Arm1: EMG Intensity and Force in Dominant Arm1: EMG Intensity and Force in Dominant Arm1: EMG Intensity and Force in Dominant Arm
ProcedureProcedureProcedureProcedure
1. The subject should sit quietly with his or her dominant forearm resting on the table top. Explain the procedure to the subject. The subject will squeeze his or her fist
around the hand dynamometer four times, each contraction is two seconds long

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 25
followed by two seconds of relaxation. Each successive contraction should be
approximately two, three, and four times stronger than the first contraction.
2. Type Increasing Grip ForceIncreasing Grip ForceIncreasing Grip ForceIncreasing Grip Force----Dominant Dominant Dominant Dominant in the Mark box Mark box Mark box Mark box to the right of the Mark Mark Mark Mark buttonbuttonbuttonbutton. Click the Record button Record button Record button Record button to begin the recording; then, press the Enter Enter Enter Enter key
on the keyboard to mark the beginning of the recording. After the recording is
marked, tell the subject to begin squeezing the hand dynamometer following the procedure outlined in the step above.
3. In the relaxation period after the last contraction, click the Stop Stop Stop Stop button.
4. Click the AutoScale buttons AutoScale buttons AutoScale buttons AutoScale buttons for the EMGEMGEMGEMG, Muscle Muscle Muscle Muscle ForceForceForceForce, and EMG Integral EMG Integral EMG Integral EMG Integral channels.
5. Select Save As Save As Save As Save As in the File menuFile menuFile menuFile menu, type a name for the file. Choose a destination on
the computer in which to save the file, like your lab group folder). Designate the
file type as *.iwxdata*.iwxdata*.iwxdata*.iwxdata. Click on the Save Save Save Save button to save the data file.
Data AnalysisData AnalysisData AnalysisData Analysis 1. Use the Display Time Display Time Display Time Display Time icons to adjust the Display Time Display Time Display Time Display Time of the Main window Main window Main window Main window to show
the four progressive muscle contractions on the Main windowMain windowMain windowMain window. The four
contractions can also be selected by: • Placing the cursors on either side of a group of four contractions; and clicking
the Zoom between Cursors Zoom between Cursors Zoom between Cursors Zoom between Cursors button on the LabScribe toolbar to expand the
segment with the four contractions to the width of the Main windowMain windowMain windowMain window. 2. Click on the Analysis window Analysis window Analysis window Analysis window icon in the toolbar or select Analysis Analysis Analysis Analysis from the
Windows menu Windows menu Windows menu Windows menu to transfer the data displayed in the Main window Main window Main window Main window to the Analysis.Analysis.Analysis.Analysis.
3. Look at the Function Table Function Table Function Table Function Table that is above the uppermost channel displayed in the
Analysis Analysis Analysis Analysis window. The mathematical functions, Abs. AreaAbs. AreaAbs. AreaAbs. Area, V2V2V2V2----V1V1V1V1, and T2T2T2T2----T1 T1 T1 T1 should appear in this table. The values for Abs. AreaAbs. AreaAbs. AreaAbs. Area, V2V2V2V2----V1V1V1V1, and T2T2T2T2----T1 T1 T1 T1 on each
channel are seen in the table across the top margin of each channel.
4. Once the cursors are placed in the correct positions for measuring the absolute areas under the muscle contraction and the corresponding EMG activity, the values
for the areas can be recorded in the on-line notebook of LabScribe by typing the
names and values directly into the JournalJournalJournalJournal. 5. Use the mouse to click on and drag the cursors to the beginning and end of the first
muscle contraction. The values for Abs. Area Abs. Area Abs. Area Abs. Area on the EMG EMG EMG EMG and Muscle channels Muscle channels Muscle channels Muscle channels are
the relative amount of the electrical activity causing the contraction and relative strength of the muscle, respectively. Record the values for these areas in the Journal Journal Journal Journal
using the one of the techniques described earlier in this exercise....
6. Repeat Steps 4, 5, and 6 for the other three muscle contractions recorded in this exercise.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 26
7. Use a piece of string and a metric ruler to measure the circumference of the
dominant forearm at approximately 3 centimeters below the elbow. Record this
value in the Journal.Journal.Journal.Journal. 8. Select Save Save Save Save from the File menuFile menuFile menuFile menu.
ExerciseExerciseExerciseExercise#### 2: EMG Intensity and Fatigue in2: EMG Intensity and Fatigue in2: EMG Intensity and Fatigue in2: EMG Intensity and Fatigue in Dominant ArmDominant ArmDominant ArmDominant Arm
ProcedureProcedureProcedureProcedure 1. The subject should sit quietly with his or her dominant forearm on the table top.
2. Explain the experimental procedure of this exercise to the subject:
• The subject will squeeze the bulb of the hand dynamometer as tightly and as long as possible in an attempt to fatigue the muscles of the forearm.
• As time passes, the subject’s muscle force will decrease, but a a rate that is
dependent on the fitness of the subject.
• When the subject’s muscle strength drops to a level that is below half of the subject’s maximum muscle force at the beginning of the recording, the recording
will be stopped. This could take as little as 20 or as long as a few minutes.
3. Type FatigueFatigueFatigueFatigue----Dominant Dominant Dominant Dominant in the Mark box Mark box Mark box Mark box to the right of the Mark buttonMark buttonMark buttonMark button. Click the Record Record Record Record button, followed by pressing the Enter Enter Enter Enter key on the keyboard. Record a
baseline for ten seconds, then instruct the subject to squeeze and hold the hand
dynamometer with as much force as possible. Continue to record. 4. Click the AutoScale buttons AutoScale buttons AutoScale buttons AutoScale buttons for the EMG EMG EMG EMG and MuscleMuscleMuscleMuscle Force Force Force Force channels.
5. When the subject’s muscle strength decreases to a level that is below 50% of the
maximum muscle strength that was recorded at the beginning of this exercise, instruct the subject to release the bulb. Click the Stop Stop Stop Stop button to halt the recording.
6. Select Save Save Save Save from the File menuFile menuFile menuFile menu.
Data AnalysisData AnalysisData AnalysisData Analysis 1. Use the Display Time Display Time Display Time Display Time icons to adjust the Display Time Display Time Display Time Display Time of the Main window Main window Main window Main window to show
the complete muscle fatigue recording on the Main windowMain windowMain windowMain window. The complete
recording can also be selected by: • Placing one cursor on the relaxation period just before the contraction and the
other cursor on the relaxation period just after the subject releases the hand
dynamometer. • Clicking the Zoom between Cursors Zoom between Cursors Zoom between Cursors Zoom between Cursors button on the LabScribe toolbar to expand
the muscle fatigue recording to the width of the Main windowMain windowMain windowMain window.
2. Click on the Analysis window Analysis window Analysis window Analysis window icon in the toolbar or select Analysis Analysis Analysis Analysis from the Windows menu Windows menu Windows menu Windows menu to transfer the data displayed in the Main window Main window Main window Main window to the Analysis Analysis Analysis Analysis
windowwindowwindowwindow.
3. Look at the Function Table Function Table Function Table Function Table that is above the uppermost channel displayed in the Analysis Analysis Analysis Analysis window. The mathematical functions, Abs. AreaAbs. AreaAbs. AreaAbs. Area, V2V2V2V2----V1V1V1V1, and T2T2T2T2----T1 T1 T1 T1

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 27
should appear in this table. The values for Abs. AreaAbs. AreaAbs. AreaAbs. Area, V2V2V2V2----V1V1V1V1, and T2T2T2T2----T1 T1 T1 T1 on each
channel are seen in the table across the top margin of each channel.
4. On the Muscle Force Muscle Force Muscle Force Muscle Force channel, use the mouse to click on and drag the cursors to specific points on the recording to measure the following:
• The maximum muscle forcemaximum muscle forcemaximum muscle forcemaximum muscle force. To measure this force, place one cursor on the
baseline before the muscle contraction and the second cursor on the peak muscle force near the beginning of the contraction. The value for V2V2V2V2----V1 V1 V1 V1 on the Muscle Muscle Muscle Muscle
ForForForForcececece channel is this amplitude.
• The halfhalfhalfhalf----max muscle forcemax muscle forcemax muscle forcemax muscle force. Divide the maximum muscle force by 2. • The halfhalfhalfhalf----max fatigue timemax fatigue timemax fatigue timemax fatigue time, which is the time it takes the muscle force to
decrease to 50% of the maximum during the fatigue experiment. Place one
cursor on the peak muscle force. Move the second cursor to the right of the peak
muscle force until the absolute value for V2V2V2V2----V1V1V1V1, seen on the Muscle Force Muscle Force Muscle Force Muscle Force channel, is equal to the half-max muscle force.
Exercise 3: EMG Intensity and Force in the NonExercise 3: EMG Intensity and Force in the NonExercise 3: EMG Intensity and Force in the NonExercise 3: EMG Intensity and Force in the Non---- Dominant ArmDominant ArmDominant ArmDominant Arm
ProceProceProceProceduredureduredure Follow the same directions used in Exercise 1 to record data from the subject’s non-dominant forearm.
Data AnalysisData AnalysisData AnalysisData Analysis
1. Analyze the data from the subject’s non-dominant forearm as it was done in Exercise 1.
2. Record the values for the parameters that were measured in the Journal Journal Journal Journal using the
one of the techniques described in Exercise 1.
3. Use a piece of string and a metric ruler to measure the circumference of the non-dominant forearm at approximately 3 centimeters below the elbow. Record this
value in the JournJournJournJournalalalal.
4. Select Save Save Save Save from the File menuFile menuFile menuFile menu.
Exercise 4: EMG Intensity and Fatigue in NonExercise 4: EMG Intensity and Fatigue in NonExercise 4: EMG Intensity and Fatigue in NonExercise 4: EMG Intensity and Fatigue in Non----Dominant ArmDominant ArmDominant ArmDominant Arm ProcedureProcedureProcedureProcedure
Follow the same directions used in Exercise 2 to record fatigue data from the subject’s
non-dominant forearm. Data AnalysisData AnalysisData AnalysisData Analysis
Analyze the fatigue data from the subject’s non-dominant forearm as it was done in
Exercise 2.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 28
PPPPart art art art TwoTwoTwoTwo: : : : ElectromyogramElectromyogramElectromyogramElectromyogram (EMG) Activity in Antagonistic(EMG) Activity in Antagonistic(EMG) Activity in Antagonistic(EMG) Activity in Antagonistic MusclesMusclesMusclesMuscles
ObjectivesObjectivesObjectivesObjectives
• To study the EMG activity in muscles that work in opposition to each other to
flex or extend the hand. • To study the EMG activity in muscles that lift weight by flexion or by extension
BackgroundBackgroundBackgroundBackground The movement of parts of the body is accomplished through a system of levers
composed of skeletal muscles and bones. In a lever, the muscle attached to the bone
provides the effort or force that moves the bone. As the muscle contracts and relaxes, the bone, functioning as the actual lever, rotates around a joint in the skeletal system. In
relation to the muscle, the bone, and the body part being moved, the joint is the fixed
point that functions as the fulcrum for the lever. The body part being moved is the load
in the lever.
All levers, including the ones in the body, can be categorized into one of three classes, which are based on the position of the fulcrum in relation to the positions of the effort
and the load:
• In First Class levers, the fulcrum is between the effort and the load, like on a see-saw. In the body, an example of this class is the extension of the forearm by the
triceps muscle.
• In Second Class levers, the load is between the effort and the fulcrum, like a
wheel barrow. In the body, an example of this class is standing on tiptoe by using the gastrocnemius muscle.
• In Third Class levers, the effort is between the fulcrum and the load, like
tweezers. In the body, an example is the flexion of the forearm by the biceps muscle.
Body parts are moved in different directions by muscles that act on the same bone from
different directions. A simple example is the movement of the forearm. When the

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 29
biceps muscle contracts, the forearm and the hand move toward the shoulder in a
motion called flexion. When the triceps muscle contracts, the forearm and hand move
away from the shoulder in a motion called extension. Since these two muscles move the forearm in different directions, they are antagonistic muscles. These muscles relax and
contract in a coordinated manner to place the forearm and hand in the desired position.
If the effort exerted on the bone by each muscle is equal in magnitude and opposite in direction, the forearm remains stationary. Antagonistic muscles do not need to belong
to the same class of lever to work in opposition. For example, the biceps and from two
different classes of levers. The biceps and triceps are different classes of levers; the biceps is part of a third class lever, and the triceps is part of a first class lever.
By recording the EMG activity in a muscle during the movement or positioning of a
body part, it can be determined if the muscle is involved. In this experiment, students will record EMG activity from muscles on the anterior and posterior sides of the
forearm to determine which ones are responsible for flexion and extension of the hand.
Recording of EMG activity from these muscles will also be done while a weight is lifted by the hand. In another exercise, students will record EMG activity from the anterior
and posterior sides of the lower leg to determine which muscles are active during
movements or positioning that are more complex, like leaning forward, standing on toes, or rocking on heels.
Equipment RequiredEquipment RequiredEquipment RequiredEquipment Required
• PC Computer
• IWX/214 data acquisition unit
• USB cable • IWX/214 power supply
• C-AAMI-504 ECG cable and electrode lead wires
• Disposable electrodes
• Alcohol swabs • Small weight
Start the SoftwareStart the SoftwareStart the SoftwareStart the Software 1. Click on the LabScribe shortcut on the computer’s desktop to open the program. If
a shortcut is not available, click on the Windows Start menuStart menuStart menuStart menu, move the cursor to
All ProgramsAll ProgramsAll ProgramsAll Programs and then to the listing for iWorxiWorxiWorxiWorx. Select LabScribe LabScribe LabScribe LabScribe from the iWorx iWorx iWorx iWorx submenusubmenusubmenusubmenu. The LabScribe Main window Main window Main window Main window will appear as the program opens.
2. On the Main windowMain windowMain windowMain window, pull down the Settings menu Settings menu Settings menu Settings menu and select Load Group.Load Group.Load Group.Load Group.
3. Locate the folder that contains the settings group, IPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrpIPLMv4.iwxgrp. Select this group and click OpenOpenOpenOpen.
4. Pull down the Settings menu Settings menu Settings menu Settings menu again. Select the AntagonstAntagonstAntagonstAntagonsticMusclesicMusclesicMusclesicMuscles----LS2 LS2 LS2 LS2 settings file.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 30
5. After a short time, LabScribe will appear on the computer screen as configured by
the AntagonsticMusclesAntagonsticMusclesAntagonsticMusclesAntagonsticMuscles----LS2 LS2 LS2 LS2 settings.
EMG Cable SetupEMG Cable SetupEMG Cable SetupEMG Cable Setup
1. Locate the C-AAMI-504 EMG cable and electrode lead wires in the iWorx kit. 2. Insert the black AAMI connector on the end of the EMG cable into the isolated
inputs of Channels 1 and 2 of the IWX/214.
3. Locate the muscles of the forearm over which the recording electrodes will be placed. Muscles can be located by flexing or extending the hand and noting the
areas of the forearm where the muscles are tense during these hand positions:
• One pair of recording electrodes will be placed over the flexor muscles on the anterior surface of the forearm. The first electrode in this pair will be placed
about 8 centimeters below the inside of the elbow and about 4 centimeters from
the medial margin of the forearm. The second electrode in this pair will be
placed about 8 centimeters below the other electrode along the midline of the anterior surface of the forearm.
• A second pair of electrodes will be placed over the extensor muscles on the
posterior surface of the forearm. The first electrode in this pair will be placed about 9 centimeters below the tip of the elbow along the midline of the posterior
surface of the forearm. The second electrode in this pair will be placed about 6
centimeters below the first electrode and about 3 centimeters from the lateral margin of the posterior surface of the forearm.
• A fifth electrode, used as the ground, is centered between the positions of the
four recording electrodes.
4. Use an alcohol swab to clean and scrub the areas where the electrodes will be
placed. Let the areas dry before attaching the electrodes.
5. Remove the plastic disk from a disposable electrode and apply it to one of the
scrubbed areas. Attach an electrode to each of the other areas.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 31
6. Snap the recording lead wires onto the electrodes, so that:
• the red “+1” lead is attached to the electrode on the anterior forearm that is
nearest the elbow. • the black “-1” lead is attached to the electrode on the anterior forearm closest to
the middle of the forearm.
• the white “+2” lead is attached to the electrode on the posterior forearm that is nearest the elbow.
• the brown “-2” lead is attached to the electrode on the posterior forearm closest
to the middle of the forearm. • the green “C” lead (the ground) is attached to the electrode in the center of the
box formed by the positions of the four recording electrodes.
Exercise Exercise Exercise Exercise 1111: : : : Antagonistic MusclesAntagonistic MusclesAntagonistic MusclesAntagonistic Muscles in Forearmin Forearmin Forearmin Forearm
ProcedureProcedureProcedureProcedure
1. Instruct the subject that he or she will be doing the following during this exercise: • Before the recording begins, the subject extends his or her arm in front of their
body with the palm facing upward. This position is defined as the neutralneutralneutralneutral
position.position.position.position. • Keep his or her hand open during the recording.
• Move his or her hand upward (flexion) from the neutral position as far as
possible and hold it in this position for four seconds. • Return the hand to the neutral position for four seconds.
• Move the hand downward (extension) as far as possible and hold it in this
position for four seconds. • Return the hand to the neutral position for at least two seconds.
• Repeat this cycle of flexion and extension two more times while recording.
2. Before the starting the recording, type Neutral in the Mark box to the right of the
Mark button. Instruct the subject to place his or her hand in the neutral position.
3. Click the Record button in the upper right corner of the LabScribe Main window. Either click on the Mark button or press the Enter key on the keyboard to label the
recording. 4. While the subject’s hand is in the neutral position, type Flexion in the Mark box.
When the subject flexes his or her hand, click on the Mark button or press the Enter key on the keyboard to label the recording.
5. While the subject’s hand is in the flexed position, type Neutral in the Mark box.
When the subject returns his or her hand to the neutral position, click on the Mark button or press the Enter key on the keyboard to label the recording.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 32
6. While the subject’s hand is in the neutral position, type Extension in the Mark box.
When the subject extends his or her hand, click on the Mark button or press the
Enter key on the keyboard to label the recording. 7. Repeat Steps 2 through 6 two more times.
8. When the last cycle is completed, click the Stop button.
9. Click Auto Scale on all channels to amplify signals. 10. Select Save As in the File menu, type a name for the file.
Data AnalysisData AnalysisData AnalysisData Analysis 1. Scroll through the recording and find the section of data recorded while the subject
was flexing and extending his or her hand.
2. Use the Display Time icons to adjust the Display Time of the Main window so all three flexion-extension cycles appear on the Main window. The three flexion-
extension cycles can also be selected by:
• Placing the cursors on either side of the three adjacent cycles.
• Clicking the Zoom between Cursors button on the LabScribe toolbar to expand the segment with the three cycles to the width of the Main window.
3. Click on the Analysis window Analysis window Analysis window Analysis window icon in the toolbar or select Analysis Analysis Analysis Analysis from the
Windows menu Windows menu Windows menu Windows menu to transfer the data displayed in the Main window Main window Main window Main window to the Analysis Analysis Analysis Analysis windowwindowwindowwindow.
4. Look at the Function Table that is above the uppermost channel displayed in the
Analysis window. The mathematical functions, Abs. Area, MaxAbs. Area, MaxAbs. Area, MaxAbs. Area, Max----Min, and T2Min, and T2Min, and T2Min, and T2----T1T1T1T1 should appear in this table. The values for Abs. Area, MaxAbs. Area, MaxAbs. Area, MaxAbs. Area, Max----Min, and T2Min, and T2Min, and T2Min, and T2----T1T1T1T1 on each
channel are seen in the table across the top margin of each channel.
5. Use the mouse to click on and drag the cursors to the onset and offset of the EMG burst during the first flexion. The values for Abs. Area, MaxAbs. Area, MaxAbs. Area, MaxAbs. Area, Max---- Min, and T2Min, and T2Min, and T2Min, and T2----T1T1T1T1 on
the Anterior channelAnterior channelAnterior channelAnterior channel are the relative amounts of the EMG activity, the differences
between maximum and minimum EMG amplitudes, and the durations of the EMG
burst in the anterior muscle group during the flexion. The values for these parameters, listed in the table above the Posterior channelPosterior channelPosterior channelPosterior channel, are the same properties
from the posterior muscle group during the same flexion.
6. Use the mouse to move the cursors to onset and offset of the next EMG burst, which is the first burst that occurs during extension. Measure and record the values
for Abs. Area, MaxAbs. Area, MaxAbs. Area, MaxAbs. Area, Max----Min, and T2Min, and T2Min, and T2Min, and T2----T1T1T1T1 from both groups of muscles during this
extension. 7. Measure the Abs.Area, MaxAbs.Area, MaxAbs.Area, MaxAbs.Area, Max----Min, and T2Min, and T2Min, and T2Min, and T2----T1T1T1T1 for the EMG bursts from the anterior
and posterior muscles from the remaining flexions and extensions.
8. Average the values for each parameter taken from the anterior muscles during flexion. Find the average for each parameter from the anterior muscles during
extension. Also, find the averages for the parameters from the posterior muscles

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 33
during flexion and during extension. Enter the averages for each parameter, from
each muscle group during flexion and during extension.
Exercise Exercise Exercise Exercise 2222: : : : Antagonistic MusclesAntagonistic MusclesAntagonistic MusclesAntagonistic Muscles Doing WorkDoing WorkDoing WorkDoing Work
ProcedureProcedureProcedureProcedure
1. Use the same experimental setup used in Exercise 1. 2. Instruct the subject to rest his or her forearm, with the electrodes, on a flat surface
with the palm up.
3. Place a weight (2-3kg) in the palm of the subject’s hand. 4. Click Record. Record the EMG activity from the muscles of the forearm as the
subject lifts the weight by the flexion. The subject should raise and hold the weight
up for four seconds and then return the weight to the table top for four seconds. Repeat this cycle two more times.
5. Click Stop to halt the recording.
6. Instruct the subject to rest his or her forearm on a flats surface with the palm down.
7. Have the subject grip the same weight (2-3kg). 8. Click Record. Record the EMG activity from the muscles of the forearm as the
subject lifts the weight by extension. The subject should raise and hold the weight
up for four seconds and then return the weight to the table top for four seconds. Repeat this cycle two more times.
9. Click Stop to halt the recording.
10. Select Save in the File menu.
Data AnalysisData AnalysisData AnalysisData Analysis
1. Scroll through the recording and find the section of data recorded while the subject
was lifting a weight by flexion and extension.
2. Use the same procedures used in Exercise 1 to measure and record the Abs. Area, Abs. Area, Abs. Area, Abs. Area, MaxMaxMaxMax----Min, and T2Min, and T2Min, and T2Min, and T2----T1 T1 T1 T1 from each muscle group while the weight was lifted by
flexion and by extension.
3. Average the values for each parameter taken from the anterior muscles while weight was lifted by flexion. Find the average for each parameter from the anterior
muscles while weight was lifted by flexion. Also, find the averages for the
parameters from the posterior muscles while weight was lifted by flexion and by extension. Enter the means for each parameter, from each muscle group during
flexion and during extension.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 34
Experiment # Experiment # Experiment # Experiment # 4444: Safety Analyzer
ObjectiveObjectiveObjectiveObjectivessss:
• To understand the principles involved in performing electrical safety
measurements on medical devices. • To perform acceptance tests on medical devices using an electrical
safety analyzer that include main voltage, dual lead voltage, current
consumption, insulation resistance, protective earth resistance, earth leakage current, enclosure leakage current , patient leakage current,
…etc.
Equipment RequiredEquipment RequiredEquipment RequiredEquipment Required::::
• International safety analyzer • Oscilloscope
• Lead selector
• ECG cable • Medical Kit (ECG)
BackgroundBackgroundBackgroundBackground::::
Commercially available instruments called Electrical-Safety Analyzers are available for
testing both medical-facility power systems and medical appliances. These analyzers range in complexity from simple conversion boxes used with any voltage-ohmmeter to
computerized automatic measurement systems. The features to consider are accuracy,
ease of use, testing time, and cost. The analyzers also reduce errors caused by incorrect
test setups and reduce the risk of shock to person performing tests such as applying line voltage to patient leads to test isolations.
Adequate electrical safety in health-care facilities can be achieved at moderate cost by combining a good power-distribution system, careful selection of well-designed
equipment, periodic testing of power systems and equipment, and a modest training
program for medical personnel. For an electrical accident to occur, current of sufficient magnitude must flow through the body of the victim in such a way that it impairs the functioning of vital organs.
The Physiological effect of electrical current:

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 35
• The physiological effect of the current depends not only on their
magnitude but also on the current pathway through the body, which in turn depend on the location of the contact.
• The effect of small current applied directly to the heart is often referred to as microshock
• Electric current can affect the tissue in two different ways:
1. The electrical energy dissipated in the tissue resistance can
cause a temperature increase, if high enough, tissue damage can occur.
2. An extraneous electric current of sufficient magnitude can cause local voltages that can trigger action potential and stimulate nerves, the stimulation of motor nerves or muscles causes contraction of muscle fiber In the muscles or muscle group
There are three methods of accident prevention:
1. Reliable Grounding design: The design and construction of equipment,
excluding self-powered equipment, should insure that all external parts, surfaces, and shields, exclusive of antenna and transmission line
terminals, are at ground potential at all times during normal operation. A
point on the electrically conductive chassis or equipment frame should serve as the common tie point for static and safety grounding.
2. Reduction of Leakage current: Leakage current is that current which
flows through the equipment conductive paths to a solidly grounded
source. The equipment leakage current should not exceed 3.5 milliamperes dc or rms.
3. Double insulation of equipment.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 36
Front PanelFront PanelFront PanelFront Panel
AAAA Applied Part Terminal: The jacks allow direct connection to banana jacks, or 4mm-to-
alligator adapters provided
BBBB Red Input Terminal : Single test lead connection CCCC Black Input Terminal: Used for dual lead testing in combination with red test lead.
D D D D Green Input Terminal: Protective Earth of Device Under Test
EEEE Power Outlet: Allows standard power plug connection of the Device Under Test. 120V @ 15A or 240V @ 15A maximum
FFFF On-Off Switch
Comparable Terminology: International and United StatesComparable Terminology: International and United StatesComparable Terminology: International and United StatesComparable Terminology: International and United States
INTERNATIONAL/IECINTERNATIONAL/IECINTERNATIONAL/IECINTERNATIONAL/IEC U.S./AAMIU.S./AAMIU.S./AAMIU.S./AAMI
L1 Neutral L2 Hot
Earth Ground
Mains Line Voltage Applied Parts Patient Leads
Enclosure/Case Chassis
Protective Earth Ground Wire
Earth Leakage Current Leakage in Ground Wire Enclosure Leakage Chassis Leakage
Patient Leakage Lead Leakage
Patient Auxiliary Leakage between Patient Leads Mains on Applied Parts Lead Isolation
Insulation Resistance Dielectric Strength or Insulation Resistance
between Hot and Neutral to Ground
Earth Resistance Ground Wire Resistance
Keys Used to Enter DeKeys Used to Enter DeKeys Used to Enter DeKeys Used to Enter Device Control Numbersvice Control Numbersvice Control Numbersvice Control Numbers
0 Volts0 Volts0 Volts0 Volts: In single lead mode, displays mains voltage.
In dual lead mode, displays voltage between RED and BLACK test leads.
1 Current:1 Current:1 Current:1 Current: Measures the current consumption (in amperes) flowing in the L2 of the
device under test. 2 In2 In2 In2 Insulation: sulation: sulation: sulation: Tests insulation resistance (mains to case or applied parts to case).

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 37
3 Protective Earth Resistance: 3 Protective Earth Resistance: 3 Protective Earth Resistance: 3 Protective Earth Resistance: Measures the earth resistance using a 1A test
current (unless 10A or 25A is selected) using the RED test lead attached to the DUT
Protective Earth terminal or enclosure. The front panel outlet power is turned off off off off for this test.
* Note: Note: Note: Note: Calibrate the test leads if performing a protective earth resistance test for the
first time with a unit or when using a new set of leads. Also calibrate the leads if the unit does not read zero when the test lead is connected between the RED and GREEN
input jacks and a measurement is taken.
4 4 4 4 Earth LeakageEarth LeakageEarth LeakageEarth Leakage: easured between the DUT “Protective Earth” terminal and the “Protective Earth” terminal of the 601PRO.
5 5 5 5 Enclosure Leakage: Enclosure Leakage: Enclosure Leakage: Enclosure Leakage: In single-lead mode, measures the enclosure leakage (RED test
lead to DUT protective earth on the 601PRO).
6666 Patient Leakage: Patient Leakage: Patient Leakage: Patient Leakage: Measures the patient leakage current (applied part to earth). 7 Mains on Applied Part Leakage: 7 Mains on Applied Part Leakage: 7 Mains on Applied Part Leakage: 7 Mains on Applied Part Leakage: Applies 110% mains voltage to selected applied part
and measures leakage to earth in both normal and reverse polarity. Does not apply to
patient auxiliary selections. 8 Patient Auxiliary Current: 8 Patient Auxiliary Current: 8 Patient Auxiliary Current: 8 Patient Auxiliary Current: Measures the leakage and biasing current between applied
parts.
ProcProcProcProcedureedureedureedure::::
Part 1:
1. Connect the power cable of oscilloscope to the safety analyzer machine. At this
time make sure that safety machine in OFF status.
2. Turn ON the safety test machine. Wait until the safety analyzer tests itself.
When the test is successfully completed, "Main Menu" appears on the screen.
3. Select (System Setup) Key, Select (setup function). Then select test standard key
The select test standard option allows you to choose among IEC 601-1,VDE 701-
1, VDE 751-1, HEL 95, IEC 1010, AAMI, AS/NZS 3551. 4. At this part choose IEC 601-1.
Note : To enable /disable the test standards that appear at the Main Menu, press Utilities at the Main menu , then More then Enable standards. Press Yes
5. At the enable test standard once the selection is made, the system will automatically return to the main menu where the selected standard is displayed.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 38
6. In order to record the testing times do the following.
Selecting the class/Type:
The class /Type selection sets the type of equipment that is being tested. This affects the
limits for the protective earth resistance, insulation resistance, and earth leakage.
The class / type should be set to the instrument classification and type before testing.
What is the class and the type of the oscilloscope?
1. On the main menu under class/type menu enter the type and the class of the
oscilloscope.
2. Press view present setting key. View present setting allows you to inspect all the
entered data. If the entered data are true continue with the following.
3. Press (0) key, main voltage test and lead voltage test.
a. The main voltage test measures and displays the mains voltages from L1
to Earth, L2 to Earth, and L1 to L2.
b. The main voltage test appears on the display L1-Earth = ………
L2-Earth = ………
L1-L2 = ……….
4. Press key (1), Current Consumption Test and Turn on the scope. The current
consumption test is displayed and the test begins immediately.
Current consumption = ………..
5. Press on soft key 1 toggle the device polarity from normal to off to reverse
(Earth, L2). Current consumption = ………..
6. Toggle the device outlet from Earth to No Earth by pressing on key (2). (Normal Polarity, L2)
Current consumption = ………..
7. Toggle the device out let from L2 to No L2. (Normal Polarity, Earth)
Current consumption = ………..
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 39
Did the current value change, why? 8. The insulation Resistance testsinsulation Resistance testsinsulation Resistance testsinsulation Resistance tests measure (in Megohms) the resistance from the
device outlet L1 and L2 to device earth .The measurement is taken with a test
voltage of 500 Volts Dc. The test will not begin until start test is pressed Insulation resistance = ………
Do we need very high input resistance, why?
9. Attach the red lead for the safety machine to any conductive part of the
oscilloscope.
10. Press shortcut key 3. The protective earth resistance test is displayed.
11. Press soft key 3 to select a test current (1 AMP), the selected test current is
displayed in the upper right corner of the display
Protective earth resistance for 1 AMP = ……………
12. Select a test current (25 AMP), the selected test current is displayed in the upper right corner of the display
Protective earth resistance for 25 AMP = ……………
13. In order to measure earth leakage current, from the main menu press short key
(4), the earth leakage test appears on the display and the test begins
immediately:
a. soft key 1 toggles the device polarity from normal to off to reverse.
(Earth, L2) b. soft key 2 toggles the device outlet from Earth to no Earth. (Normal
Polarity, L2)
c. soft key 3 toggles the device from L2 to no L2. (Normal Polarity, Earth)
14. Now, record the output for all the conditions above.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 40
15. To measure the Enclosure leakage current connect the red lead terminal to the
safety analyzer machine (on the red front point) and attach it to any metal part
in the oscilloscope.
16. Press key (5) on the main menu
a. Soft key 1 toggles the device outlet polarity from normal to off to reverse,
or reverse to off to normal. (Earth, L2)
b. Soft key 2 toggles the device outlet from Earth to no Earth. (Normal Polarity, L2)
c. Soft key 3 toggles the device outlet from L2 to no L2. (Normal Polarity,
Earth)
17. Now , record the data for all above conditions
Are all values the same? Why?
18. Shutdown safety analyzer machine by pressing (Off) key, then remove the
power cable for the oscilloscope.
Part 2:
19. Connect the power cable for the medical kit to the safety analyzer, then power
on the machine.
20. Repeat steps from 1 to 7.
21. Press key (2). Record the insulation resistance as in step 8. Attach the ECG
applied parts to safety analyzer machine then press soft key (2) to change the test to AP insulation resistance. The unit will beep repeatedly as long as the test
is active. Press soft key (4) to toggle between all applied parts .
a. ALL – CASE ……. b. RA – CASE ………
c. RL - CASE ………
d. LA - CASE ………. e. LL – CASE ……….
Is their any deference between the measured values? if yes, why?
22. Repeat step (10), then record the data.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 41
23. Repeat step (12), then toggle soft key (4) in order to change from AP to earth
and from No AP to earth. Record all the results.
24. Repeat step (14), also toggle soft key from AP to No AP, then record all the
outputs.
25. Patient leakage current is measured between a selected applied part and main
earth. The following outlet conditions apply when performing this test: a. Normal polarity, earth open, Outlet ON
b. Normal polarity, L2 Open, Outlet ON
c. Reversed Polarity, Outlet ON
d. Reversed Polarity, Earth Open, Outlet ON e. Reversed Polarity, L2 Open, outlet ON.
26. To perform patient leakage current test , from the main menu press short cut Key (6). The patient leakage test is displayed, and the test begins immediately.
Record the output for the following cases:
a. All To Earth (RMS) = ……… b. RA To Earth (RMS) = ………..
c. RL To Earth (RMS) = …………
d. LA To Earth (RMS) = ……….. e. LL To Earth (RMS) = ………..
27. Mains on applied part test applies a test voltage, which is 110 of the mains
voltage, through a limiting resistance, to selected applied part terminal. Current measurements are then taken between the selected part and earth
.measurements are taken with test voltage (110 of mains) to applied parts in the
normal and reverse polarity conditions as indicated on the display. The following outlet conditions apply when performing the Mains on applied part
test:
Normal polarity
Reversed Polarity
27. Attach the red terminal lead to a conductive part on the device enclosure. Press
short key (7). The Mains applied Part test is displayed .then select the desired
outlet configuration and applied part to test using the following Keys: Soft key (1) takes one pair of readings and displays the result, Soft Key (3) toggles the
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 42
device outlet polarity from Normal To device OFF to Reverse Polarity, or refers
to device OFF to normal Polarity.
28. Now, record the following:
a. All To Earth = …….
b. Ra To Earth = …….. c. Rl To Earth = ……..
d. La to Earth = ………
e. LL To Earth = ……. (Note : on each item press start key to begin the test )
29. Patient auxiliary Current Tests are measured between any selected ECG jack and
the remaining Selected ECG jack. The following outlet conditions apply when performing this test
a. Normal Polarity, earth open, outlet ON
b. Normal Polarity, L2 Open, Outlet ON c. Reverse Polarity, outlet ON
d. Reverse Polarity, earth open, Outlet ON
e. Reversed Polarity, L2 open, Outlet ON
30. From the Main menu press shortcut Key (8), the Patient auxiliary Current test is
displayed, and the test begins immediately. The display is updated until another test is selected.
31. Toggle between soft keys (1,2,3,4) and record all data. Including the following:
a. Ra to All (RMs) = ……
b. Rl to All (RMS) = ……
c. LL to All (RMS) = …… d. La to All (RMS) = ……

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 43
Experiment #Experiment #Experiment #Experiment #5555: : : : Pulmonary Function Test
Objectives:Objectives:Objectives:Objectives:
• To understand and analyze different respiratory parameters VC, FVC, and MVV. • Understand how to prepare PFT patient data.
• To study the effect of exercise on respiratory parameters.
Equipment Required:Equipment Required:Equipment Required:Equipment Required:
• USB serial port • Spirobank II • Computer
• Mouthpiece
• Nose clip
BackgroundBackgroundBackgroundBackground::::
Background:
Pulmonary function testing (PFT) is one of the basic tools for evaluating patient’s
respiratory status. Pulmonary function tests are tests performed to make measurements
of how your lungs and airways function. Results from pulmonary function tests enable your physician to evaluate your breathing, make diagnosis, recommend treatment and
follow your progress.
PFT is used for the following reason:
1. Screening for the presence of obstructive and restrictive diseases
2. Evaluating the patient's condition for weaning from a ventilator. If the patient on a ventilator can demonstrate a vital capacity (VC) of 10 - 15
ml/Kg of body weight, it is generally thought that there is enough
ventilatory reserve to permit (try) weaning and extubation. 3. Documenting the progression of pulmonary disease - restrictive or
obstructive
4. Documenting the effectiveness of therapeutic intervention

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 44
Terminology and Definitions:
• Total Lung Capacity (TLC):Total Lung Capacity (TLC):Total Lung Capacity (TLC):Total Lung Capacity (TLC): the volume of air in lungs during a maximal effort of inhalation.
• Functional Residual Capacity (FRC): Functional Residual Capacity (FRC): Functional Residual Capacity (FRC): Functional Residual Capacity (FRC): the volume of air in lungs when the
respiratory muscles are inactive and relaxed. • Residual Volume (RV):Residual Volume (RV):Residual Volume (RV):Residual Volume (RV): the volume of air remaining in lungs after a maximal
effort of exhalation.
• VitalVitalVitalVital capacitycapacitycapacitycapacity (VC):(VC):(VC):(VC): the maximum volume of air that can be expired slowly after a full inspiratory effort.
• Forced Vital Capacity (FVForced Vital Capacity (FVForced Vital Capacity (FVForced Vital Capacity (FVC):C):C):C): measured by taking the deepest possible breath,
this is the volume of air which can be forcibly and maximally exhaled out of the
lungs until no more can be expired. This value is critically important in the diagnosis of obstructive and restrictive diseases.
• Forced Expiratory Volume in One Second (FEV1):Forced Expiratory Volume in One Second (FEV1):Forced Expiratory Volume in One Second (FEV1):Forced Expiratory Volume in One Second (FEV1): the volume of air which can
be forcibly exhaled from the lungs in the first second of a forced expiratory maneuver. This PFT value is critically important in the diagnosis of obstructive
and restrictive diseases.
• FEV1/FVC FEV1/FVC FEV1/FVC FEV1/FVC ---- FEV1 Percent (FEV1%):FEV1 Percent (FEV1%):FEV1 Percent (FEV1%):FEV1 Percent (FEV1%): - This number is the ratio of FEV1 to FVC - it indicates what percentage of the total FVC was expelled from the lungs
during the first second of forced exhalation - this number is called FEV1%,
%FEV1 or FEV1/FVC ratio. This PFT value is critically important in the diagnosis of obstructive and restrictive diseases.
• Maximal Voluntary Ventilation (MVV):Maximal Voluntary Ventilation (MVV):Maximal Voluntary Ventilation (MVV):Maximal Voluntary Ventilation (MVV): - this value is determined by
breath in and out as rapidly and fully as possible for 12 -15 seconds. This
test parameter reflects the status of the respiratory muscles, compliance of the thorax-lung complex, and airway resistance.
• Dynamic Lung Volumes and Flow Rates:Dynamic Lung Volumes and Flow Rates:Dynamic Lung Volumes and Flow Rates:Dynamic Lung Volumes and Flow Rates: Dynamic lung volumes reflect
the caliber and integrity of the airways. Spirometry records lung volume against time during an FVC maneuver. It's mainly expressed by (FEV1)
(%FVC), (MVV).
• FlowFlowFlowFlow----Volume Loop:Volume Loop:Volume Loop:Volume Loop: The flow-volume loop is generated by continuously recording flow and volume with an electronic spirometer during a forced
inspiratory and expiratory VC maneuver. The shape of the loop reflects
the status of the lung volumes and airways throughout the respiratory cycle. Characteristic changes occur in restrictive and in obstructive
disorders. The loop is especially helpful in detecting laryngeal and
tracheal lesions. It can distinguish between fixed obstruction (e.g., tracheal stenosis) and variable obstruction (e.g., tracheomalacia, vocal

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 45
cord paralysis) of the upper airway. The figure below illustrates some
characteristic flow-volume loop abnormalities.
Obstructive lung disorders
The most common disorders are: asthma, chronic obstructive bronchitis, emphysema, and cystic fibrosis.
These disorders are all characterized by low expiratory airflow as measured by low
FEV1. The low FEV1 is due to narrowing of the airways with increased airflow resistance.
The patient with obstructive lung disease has a smaller flow-volume-loop than that of a normal subject - performed as a forced vital capacity maneuver The RV of the patient is
2.4 l or twice as high as that of the healthy individual, because of air trapping (a large
volume of trapped air).
Flow through the tubular passageways of the lung can be reduced for a number of
reasons:
• Narrowing of the airways due to bronchial smooth muscle contraction as
is the case in asthma
• Narrowing of the airways due to inflammation and swelling of bronchial mucosa as is the case in bronchitis
• Material inside the bronchial passageways physically obstructing the flow
of air as is the case in excessive mucus plugging, inhalation of foreign objects or the presence of pushing and invasive tumors
• Destruction of lung tissue with the loss of elasticity and hence the loss of
the external support of the airways as is the case in emphysema • External compression of the airways by tumors and trauma
ProcedurProcedurProcedurProcedureeee::::
Using Computer Pulmonary Function Test Software “winspiroPRO” and the Recording
of VC ,FVC and MVV
1. Insert a mouthpiece into the protruding part of the turbine
2. Fit the nose clip onto the nose of the subject to ensure that cannot escape through
the nostrils. 3. Hold Spirobank at either end using both hands.
4. Open the winspiroPRO software.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 46
5.Open window Patient and after
6. Insert the required fields to create a new patient (Code -
Surname - First name - Date of birth - Gender - Ethnic Group) in the following windows
7. Then click and the Visit Card opens, insert or c
on
f
ir
m
the visit details ( date, height and weight)
8.
FVC TestFVC TestFVC TestFVC Test 9. Click on the FVC icon from the following icons to start the test.
10. Breath at rest for few moments. When ready to start inspire inspire inspire inspire
slowlyslowlyslowlyslowly as much air as possible. 11. Make a complete expiration as fastfastfastfast as possible, then with the mouthpiece always
held firmly in the mouth, complete the cycle by inspiring again as quicklyquicklyquicklyquickly as possible.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 47
Note: Note: Note: Note: After inspiring slowly and deeply, the following expiration must be made with After inspiring slowly and deeply, the following expiration must be made with After inspiring slowly and deeply, the following expiration must be made with After inspiring slowly and deeply, the following expiration must be made with the maximum effort by expiring all air as fast as possible.the maximum effort by expiring all air as fast as possible.the maximum effort by expiring all air as fast as possible.the maximum effort by expiring all air as fast as possible. After 6 seconds of expiration the instrument will emit a contiAfter 6 seconds of expiration the instrument will emit a contiAfter 6 seconds of expiration the instrument will emit a contiAfter 6 seconds of expiration the instrument will emit a continuous beep, this helps nuous beep, this helps nuous beep, this helps nuous beep, this helps the user to understand when the minimum expiry time has been reached.the user to understand when the minimum expiry time has been reached.the user to understand when the minimum expiry time has been reached.the user to understand when the minimum expiry time has been reached.
12. Record FVC, FEV1 and PEF.
13. Repeat the measurement three times and choose the beast values.
• The FVC may be calculated as:
( ) ( )
( ) ( )
0.058 0.025 4.24 for male
0.0453 0.024 2.852 for female
FVC Hc A
FVC Hc A
= − −
= − −
Where Hc and A stand for the height and age, respectively
VC TestVC TestVC TestVC Test 1. Start the Slow Vital Capacity test by carrying out several complete breaths at
rest.
2. After three or four such breaths a beep will sound to confirm that the ventilator
profile has been measured. 3. After the beep inspire inspire inspire inspire slowlyslowlyslowlyslowly as much air as possible and then expire slowly expire slowly expire slowly expire slowly as
mush air as possible. This is the Expiratory Slow Vital Capacity (VC or EVC).
4. Record VC. 5. Repeat the measurement three times and choose the beast one.
MVVMVVMVVMVV TestTestTestTest When participating in sports such as running, one is often required to use maximum
voluntary ventilation (MVV). The individual is inhaling and exhaling more deeply and
at more rapid rate. Normal respiratory rate is in the order of 11-18 times/min. During MVV activity the respiratory rate is likely to be 30 or more times/min. MVV value
depends directly on gender and height and indirectly on age, for people in their
twenties with average height and weight, males produce an MVV value of 160-170
L/min and females average 120 L/min. MVV may be estimated according to the following equation: ( ) ( ) malesfor 9.37816.019.1 −− AHc
( ) ( )1.004 0.685 48.7 for femalesHc A− −

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 48
Also, it’s possible to estimate its value from FEV1
MVV =135 FEV (l/m).
1. Start the test by carrying out a series of forced inspirations and expirations with the
maximum possible amplitude.
2. The suggested frequency is 30 breaths/min. 3. The test will terminate automatically after 12 seconds.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 49
Experiment #Experiment #Experiment #Experiment #6666: : : : Audiometry
OOOObjectivesbjectivesbjectivesbjectives::::
•••• To evaluate the audibility threshold by using an electronic audiometer. •••• To compile an audiometric graph
EEEEquipment quipment quipment quipment RRRRequiredequiredequiredequired::::
•••• Digital Multimeter
•••• Electronic Audiometer •••• Power Supply base unit
•••• Headphones.
BackgroundBackgroundBackgroundBackground::::
Hearing Process:
Hearing occurs when sound waves are conducted to the nerves of the inner ear and
from there to the brain. Sound waves can travel to the inner ear by air conduction
(through the ear canal, eardrum, and bones of the middle ear) or bone conduction (through the bones around and behind the ear).
Definition:
An audiology exam tests your ability to hear sounds. Sounds vary according to the
intensity (volume or loudness) and the tone (the speed of sound wave vibrations).
Audiometry is the testing of hearing ability. Typically, audiometric tests determine a
subject’s hearing levels, but may also measure ability to discriminate between different sound intensities, recognize pitch, or distinguish speech from background noise.
Acoustic reflex and otoacoustic emissions may also be measured. Results of audiometric
tests are used to diagnose hearing loss or diseases of the ear.
An equal-loudness contour is a measure of sound pressure (dB SPL), over the frequency
spectrum, for which a listener perceives a constant loudness. The unit of measurement
for loudness levels is the phon, and by definition two sine waves that have equal phons are equally loud.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 50
The human’s auditory system is sensitive to frequencies from 20 Hz to a maximum of
around 20,000 Hz, although the hearing range decreases with age. Within this range,
the human ear is most sensitive between 1 and 5 kHz, largely due to the resonance of the ear canal and the transfer function of the ossicles of the middle ear.
Threshold of Hearing:
INTENSITY of sound is measured in decibels (dB):
• A whisper is about 20 dB
• Loud music (some concerts) is around 80 to 120 dB • A jet engine is about 140 to 180 dB
Usually, sounds greater than 85 dB can cause hearing loss in a few hours. Louder sounds can cause immediate pain, and hearing loss can develop in a very short time.
TONE of sound is measured in cycles per second (cps) or Hertz:
• Low bass tones range around 50 to 60 Hz
• Shrill, high-pitched tones range around 10,000 Hz or higher
The normal range of human hearing is about 20 Hz to 20,000 Hz, and some animals can
hear up to about 50,000 Hz.
The measured threshold of hearing curve shows that the sound intensity required to be
heard is quite different for different frequencies. The standard threshold of hearing at
1000 Hz is nominally taken to be 0 dB, but the actual curves show the measured threshold at 1000 Hz to be about 4 dB. There is marked discrimination against low
frequencies so that about 60 dB is required to be heard at 30 Hz. The maximum
sensitivity at about 3500 to 4000 Hz is related to the resonance of the auditory canal.
Pure Tone Audiometry::::
It is typical to do this testing with pure tones by providing calibrated tones to a person via earphones, allowing that person to increase the level until it can just be heard.
Various strategies are used, but pure tone audiometry with tones starting at about 125
Hz and increasing by octaves, half-octaves, or third-octaves to about 8000 Hz is typical. Hearing tests of right and left ears are generally done independently. The results of such
tests are summarized in audiograms.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 51
Audiogram Showing Presbycusis::::
The progressive loss of high frequency sensitivity with aging is typical, and is called presbycusis. The loss of the high frequencies can make it difficult to understand speech,
since the intelligible differences in speech sounds are often in the range above 2000 Hz.
Audiograms Showing Hearing Loss::::
Audiograms can help with the diagnosis of various types of hearing disorders. Specific geometries of curves are found to be typical of presbycusis, and a characteristic notch in
the hearing curve may be the signature of damage by a sudden loud sound like a
gunshot or a firecracker explosion close to the ear.
In this experiment, an electronic audiometer will be used. It is made up of the following
blocks:
1111.... Low frequency signal generatorLow frequency signal generatorLow frequency signal generatorLow frequency signal generator
To carry out the audiometer we need a low frequency generator able to provide in output a perfectly sinusoidal wave with a very low distortion and a
constant amplitude on the whole audio range about from 20 to 25,000 Hz. The
generator has to allow to vary the output frequency by tuning on reference frequencies, for example 100 – 200 – 400 – 800 – 1,000 – 2,000 – 4,000 – 6,000
– 8,000 Hz.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 52
Sinusoidal waveform generator
This selection is made through the knob of selector S1 and a finer regulation is carried
out through trimmer R3.The oscillator is made up of three stages of operational
amplifiers at very low noise (N1A-N1B-N2A); to trigger this oscillator it is necessary to pick up the LF signal from the output of the third stage (N2A) and apply it to the input
of switch S1.The output of the first operation N1A is connected to switch S1 which
allows us to get with the second operational N1B and the double potentiometer R3 all the acoustic frequencies required by the audiometer.
The capacitors present on the five positions of the switch S1 block 1 are the same as the ones present on switch S1 block 2 as well as the resistance of the double potentiometer
R3 is the same (22k Ω).
The frequency of the output sinusoidal wave is determined by the product of the
capacity and of the resistance respectively selected through switch S1 and trimmer R3.
The frequency is calculated by using the following formula:
F= 1/6.28 R CF= 1/6.28 R CF= 1/6.28 R CF= 1/6.28 R C

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 53
2222.... Variable gain output amplifierVariable gain output amplifierVariable gain output amplifierVariable gain output amplifier
The generator is connected to an output stage which has the purpose of piloting the earphones; such an output stage is made up of a manual amplitude regulator,
an operational and a deviator.
3333.... Measure block and logarithmic display of the emitted sound levelMeasure block and logarithmic display of the emitted sound levelMeasure block and logarithmic display of the emitted sound levelMeasure block and logarithmic display of the emitted sound level
To measure and display the intensity of the emitted sound signal, it is necessary to use a logarithmic meter. This meter behaves as a comparator which compares
a fixed voltage level in input with a scale of logarithmic levels. Since the signal
emitted by the generator is sinusoidal, to measure its intensity it is necessary to rectify the signal itself.
The block which deals with “rectifying” the signal, is made up of the double
half-wave rectifying stage composed by the two operational amplifiers N4 and
N5.The direct voltage present on terminal 26 of N5A is applied to the non-inverting terminal 29 of the operational N5B and picked up by terminal 30 to be
applied to the Audio Level at LED diodes. The audio level is the most complex
part of the whole circuit; it is made up of five integrated circuits LM324 containing each one four operational amplifiers. By connecting all the non-
inverting inputs to a resistive divider of 36 resistances, we get a comparator of 19
levels at discrete components. The comparator outputs pilot 19 LED diodes, each one of which lights up with a variation of the input voltage of 1 dB.The
criticality of this logarithmic comparator is due to the fact that an error of the
lighting up level of the first LED diode (0 dB) reflects in an error of logarithmic type as to the lighting up level of the other LED diodes.
4444.... Stereo earphones with selectorStereo earphones with selectorStereo earphones with selectorStereo earphones with selector
It transforms the electric signal in acoustic signal by allowing to select the ear under
test.
PPPProcedurerocedurerocedurerocedure: : : :
1. Supply the circuit. 2. Turn trimmer R17 fully counter clockwise
3. Set switch S1 to 2
4. Turn trimmer R3 fully clockwise (minimum frequency) 5. Insert the jack of the stereo headphones in the AUDIO OUT connector.
6. Set selector S2 to LEFT (L).
7. Connect the digital multimeter between terminal 10 and ground.
Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 54
8. Adjust trimmer R3 until getting a frequency of about 100 Hz.
9. Adjust the volume (R17) until the student (patient under test) can hear the
sound in the headphones. 10. Write down in Table 1 the corresponding Audio Level in dB.
11. Turn trimmer R17 fully counter clockwise.
12. Set switch S1 to 2. 13. Turn trimmer R3 until getting an output frequency of about 200 Hz.
14. Adjust the volume until the student (patient under test) can hear the sound in
the headphones. 15. Write down in table 1 the corresponding Audio Level in dB .
16. Repeat from step 19 to step 23 for all the frequencies shown in table 1.
17. By using the values shown in the table, draw on logarithmic panel the
audiometric graph relative to the left ear of the student (patient under test). 18. Move switch S2 to RIGHT (R).
19. Repeat the procedure you have already carried out for the left ear.
20. Graph the left audio level and the right audio level versus the frequency. 21. Compare the obtained graphs.
22. Comment such results as to the studied theory.
23. Turn off the circuit.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 55
Table 1Table 1Table 1Table 1
Sound Sound Sound Sound
FrequencyFrequencyFrequencyFrequency [Hz][Hz][Hz][Hz]
SelectorSelectorSelectorSelector S1 positionS1 positionS1 positionS1 position
Left Audio LevelLeft Audio LevelLeft Audio LevelLeft Audio Level [dB][dB][dB][dB]
Right Audio LevelRight Audio LevelRight Audio LevelRight Audio Level [dB][dB][dB][dB]
20 1
50 1
100 2
200 2
500 3
1000 3
2000 4
3000 4
4000 4
5000 4
6000 4
7000 5
8000 5
9000 5
10000 5
11000 5
12000 5
13000 5
14000 5
15000 5
16000 5
17000 5
18000 5
19000 5
20000 5

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 56
Experiment #Experiment #Experiment #Experiment #7777:::: Gait Analysis
ObjectiveObjectiveObjectiveObjectivessss::::
• Learn how to record foot-floor contact data from footswitches.
• Learn how to calculate gait parameters from this data.
Equipment Required:Equipment Required:Equipment Required:Equipment Required:
• Computer • Footswitches
• Two leg belts for attaching wireless transmitters to lower legs
• Left leg and right leg wireless transmitters • Receiver with USB cable
BackgroundBackgroundBackgroundBackground::::
Gait analysis is a process of quantification and interpretation of human locomotion. The
study of gait analysis allows diagnosis processes to be made, as well as permitting future developments in rehabilitation engineering. Gait analysis is widely used in professional
sports training to optimize and improve athletic performance.
Gait analysis provides the patient with what gait experts refer to as 'Dynamic Testing' - testing during movement, thus allowing the dysfunction to occur in a near natural state, while under controlled testing conditions. By studying the motion of the lower
extremities, combined with the forces exerted upon those extremities, gait experts are usually able to identify the source of pain and thus the real cause of the pain and/or dysfunction. Very often, treatment using other methods means treating symptoms of the dysfunction and lengthy trial end error because identification of the true source of the problem cannot occur without continuous movement or exertion of the lower
extremity. Gait Analysis allows for such movement and exertion of the lower
extremities, and thus the source of the dysfunction/pain can usually be identified.
Walking is the most convenient way to travel short distances. Free joint mobility and
appropriate muscle force increases walking efficiency. As the body moves forward, one limb typically provides support while the other limb is advanced in preparation for its
role as the support limb. The gait cycle in its simplest form is comprised of stance and
swing phases. The stance phase further is subdivided into 3 segments, including initial
double stance, single limb stance, and terminal double limb stance.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 57
Each double stance period accounts for 10% of the gait cycle, while each single stance
typically represents 40%, thus the stance phase of each limb represents 60% of the limbs
gait cycle. The swing phase for the same limb is the remaining 40% of the gait cycle.
A stride is the equivalent of a gait cycle. The duration of a stride is the interval between
sequential initial floor contacts by the same limb. A step is recognized as the interval between sequential floor contacts by the two limbs. Two steps make up each gait cycle,
which is roughly symmetric in normal individuals.
Gait Cycle Phases:
Stance phase 60%
• Heel Strike (HS)
• Foot Flat (FF) • MidStance (MS)
• Heel Off (HO)
• Toe Off (TO)
Swing Phase 40%
• Initial Swing
• MidSwing
• Late Swing
A consistent sequence of motions is performed at each of the lower extremity joints
during locomotion. Stance is comprised of 5 gait phases (Heel strike, Foot flat, MidStance, Heel off, and Toe-off), with the remaining 3 phases occurring during swing.
Figure (1) shows the five gait phases of the stance phase.
The first two phases of the Stance phase occur during initial double support. These
phases include initial contact and the loading response. Initial contact often is referred
to as heel strike. The joint motion during this phase allows the transfer of weight onto
the new stance phase leg while attenuating shock, preserving gait velocity, and maintaining stability.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 58
Figure (1): Heel strike, Foot flat, MidStance, Heel off, and Toe-off
ProcedureProcedureProcedureProcedure::::
1. Setting Up the Measured Walkway: Select a convenient walking area at
least 10 meters long. A distance of 2 meters should be available before
and after the measured walkway. This distance is necessary to enable the patient to accelerate before, and decelerate after the Walkway Length for
capturing Trial data. The default Distance of the Walkway Length is 6.0
meters.
2. Attaching the Footswitches to the Patient: Footswitches are the sensors
of the Stride Analyzer System. The Footswitches are worn as insoles in the patient's shoes. Contact areas within each Footswitch must be
positioned under the appropriate weight-bearing areas of each foot for
the Heel, 5th Metatarsal, 1st Metatarsal, and Great Toe to capture timing data when these areas of the foot are bearing weight and are not bearing
weight.
• Place the proper sized insole Footswitches in the patient's shoes. • The heel section should be positioned to correspond to the
patient's Heel and the forefoot section should be positioned to
correspond to the patient's Metatarsal Heads and Great Toe.

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 59
3. Connecting the Wireless Transmitters to the Footswitches and Patient:
Each Footswitch is connected to a Transmitter by a thin cable. The
adjustable leg belt overlaps and fastens around the leg of the patient, and
the Transmitter is attached to outside of the leg belt with Velcro.
Positioning of Leg Belt and Transmitters
4. Connecting the Receiver to PC: The Receiver is used to transfer Footswitch Data from the wireless Transmitters to the Stride Analyzer
software via a USB port on the computer. Connect one end of the USB
Cable into the Receiver and the other end into the USB port on the computer.
5. Recording and Saving Patient Trial Data:
• Select File | Add New Patient

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 60
• Enter patient information in the dialog box shown above. Use the TAB
key to advance to the next field. Three fields are required: Patient I.D., Last Name, and Birth Date. After clicking the OK button, the patient's
name will appear in the program title bar near the top of the window.
• Select View | Acquire Trial
• Instruct the patient to start walking two meters before the Beginning Mark of the measured walkway (acceleration).
• As the patient crosses the Beginning Mark of the walkway, Press the
Space Bar or Click Start Recording. • Instruct the patient to continue walking two meters after the Ending
Mark of the measured walkway (deceleration).
• As the patient crosses the Ending Mark of the walkway, Press the Space Bar or Click Stop Recording.
• Once reviewed, all Trail data file(s) can be either saved to the current
Database by clicking on Save and Close, or deleted by clicking Cancel and Close. Both Save and Cancel close the Acquire New Trials and Real Time
Footswitches screens.
6. Analyzing Saved Trials from the Database:
To view the gait parameters and reports for Trials saved within the Current
Database folder, select View | Select TrialView | Select TrialView | Select TrialView | Select Trial, then Double-click on the desired Trial
Name.
Stride Characteristics:Stride Characteristics:Stride Characteristics:Stride Characteristics:

Jordan University of Science and Technology
Faculty of Engineering
Biomedical Engineering Department
Page 61
Velocity (m/min)
Cadence (Steps/min)
Stride Length (m) Gait Cycle (sec)
Swing (%GC)
Stance (%GC)