Embed Size (px)
Citation preview

JOSE RONILO G JUANGCO MD MPH
Department of Preventive and Community MedicineUERMMMC
Learning Objectives
At the end of the lecture the students should be able to
bull differentiate among the different epidemiologic study designs being used on medical research
bull know the advantages and disadvantages of the different study designs
bull decide on what particular research design is best suited for their research proposal042123 2
REVIEW
042123 3
1 What are the two types of epidemiological studies
2 What are the two types of Observational Studies
3 What are the types of Descriptive Studies
4 What types of Descriptive designs may also be classified as analytical
5 What are the types of analytical designs
6 What are the types of Cohort Studies7 What are the types of Experimental
Studies
042123 4
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 5
Types of Studies
A Experimental - study factor is manipulated by the investigator
Typesbull Laboratory versus real world
B Observational - no manipulation of study factor by the investigator1 Descriptive versus Analytic2 Retrospective versus Prospective
042123 6
A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
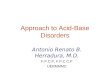
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Learning Objectives
At the end of the lecture the students should be able to
bull differentiate among the different epidemiologic study designs being used on medical research
bull know the advantages and disadvantages of the different study designs
bull decide on what particular research design is best suited for their research proposal042123 2
REVIEW
042123 3
1 What are the two types of epidemiological studies
2 What are the two types of Observational Studies
3 What are the types of Descriptive Studies
4 What types of Descriptive designs may also be classified as analytical
5 What are the types of analytical designs
6 What are the types of Cohort Studies7 What are the types of Experimental
Studies
042123 4
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 5
Types of Studies
A Experimental - study factor is manipulated by the investigator
Typesbull Laboratory versus real world
B Observational - no manipulation of study factor by the investigator1 Descriptive versus Analytic2 Retrospective versus Prospective
042123 6
A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

REVIEW
042123 3
1 What are the two types of epidemiological studies
2 What are the two types of Observational Studies
3 What are the types of Descriptive Studies
4 What types of Descriptive designs may also be classified as analytical
5 What are the types of analytical designs
6 What are the types of Cohort Studies7 What are the types of Experimental
Studies
042123 4
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 5
Types of Studies
A Experimental - study factor is manipulated by the investigator
Typesbull Laboratory versus real world
B Observational - no manipulation of study factor by the investigator1 Descriptive versus Analytic2 Retrospective versus Prospective
042123 6
A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

5 What are the types of analytical designs
6 What are the types of Cohort Studies7 What are the types of Experimental
Studies
042123 4
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 5
Types of Studies
A Experimental - study factor is manipulated by the investigator
Typesbull Laboratory versus real world
B Observational - no manipulation of study factor by the investigator1 Descriptive versus Analytic2 Retrospective versus Prospective
042123 6
A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 5
Types of Studies
A Experimental - study factor is manipulated by the investigator
Typesbull Laboratory versus real world
B Observational - no manipulation of study factor by the investigator1 Descriptive versus Analytic2 Retrospective versus Prospective
042123 6
A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Types of Studies
A Experimental - study factor is manipulated by the investigator
Typesbull Laboratory versus real world
B Observational - no manipulation of study factor by the investigator1 Descriptive versus Analytic2 Retrospective versus Prospective
042123 6
A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

A-Case report
bull Descriptionbull Is a brief objective report of clinical
characteristic or outcome from a single clinical subject or event
bull Study question bull It is commonly used to report unusual
or unexpected eventsbull Examples
bull A report of advanced diabetic retinopathy in a patient with no other clinical evidence of diabetes
-042123 7
Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Strengths and limitation
bull No statistical analysis or comparative group
bull It provides the first report of
unexpected event hypotheses for testing and definition of issue for further study but the results are rarely generalized
042123 8
B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

B-Case series report
-Descriptionbull An objective report of a clinical
characteristic or outcome from a group of clinical subjects
-Study question bull Report new disease or health
related problem -Examples bull The identification of several
children with birth defects who were born to mothers who took thalidomide during pregnancy
-042123 9
Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Strength and limitation
bull Control or comparison group is not included bull Generalization of the results is limited
because the selection of study subjects is unrepresentative
bull This study design has case selection bias and lacks statistical validity
042123 10
bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull When the goal of research is to test a hypothesis about the relationship between variables
bull No manipulation of variablesbull Variables must have values along a
numeric scalebull Different ways to describe
relationshipshellip042123 11
bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull Increase in the values of one variable is associated with increase in the second variable
042123 12
bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull Increase in the value of one variable is associated with decrease in the second variable
042123 13
bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull Increase in the value of one variable is associated with both increase and decrease of the second variable
042123 14
bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull 1048708 There is no relationship between two variables
042123 15
bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull Observations are collected and a Pearson correlational coefficient (r) is computed to specify the nature of the relationship between variables
-1 0 +1
042123 16
Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Cross-Sectional Study ndashPrevalence Study
bull Cross-Sectional Studies measure existing disease and current exposure levels
bull This study analyzes data collected on a group of subjects at one time rather than over a period of time
042123 17
Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Strength and Limitations
bull It is quick cheap and easy
bull True rates are determined (the prevalence)
bull Can study multiple exposure and multiple diseases
042123 18
Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Strength and Limitations
bull Impractical for rare diseasesbull Not useful for establishing causal
relationships It does not allow us to answer the question which came first (which caused which)
bull Data are particularly susceptible to distortion through the introduction of bias into the research during sampling questionnaire and interviewing042123 19
APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

APPROACH
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 20
CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

CASE CONTROL
042123 21
EXPOSED
NOT EXPOSED
NOT EXPOSED
EXPOSED
CASES(+) DISEASE
CONTROL(-) DISEASE
POPULATION
TIMETIME
DIRECTION OF STUDY
Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Purpose
bull Descriptive bull Describe the risk factor profile for an
outcome
bull Analytic bull Analyze associations between outcome
and risk factors
bull How do we analyze the data
ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

ANALYSIS OF CASE-CONTROL STUDY
ODDS RATIO ndash the measure of association between the factorpredictor and the outcome
= ODDS OF Case being exposed ODDS OF Control being
exposed
Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Doll and Hillrsquos Data
Lung cancer patients Controls TotalSmokers 647 622 1269Non-smokers 2 27 29Total 649 649 1298
Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Cases Controls
Exposed
Not Exposed
a b
c d
OR = a x d b x c
Using Doll amp Hillrsquos dataOR = 647 x 27 = 1404 622 x 2
Note the odds ratio of the Doll amp Hill data shows
clearly how much smoking increases the risk of lung
cancer
Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Interpretation
bull OR = 1 no association
bull ORgt 1 presence of association more factor among cases vs controls
bull ORlt1 presence of inverse association
lesser factor in cases compared to controls
Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Bias in data collection
bull The study is unmasked ( since the presence or absence of disease is known to the subject and the observer)
bull Recall bias may also occur because exposure to risk factor is often dependent on memory of subjects
042123 27
Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Bias in the selection of subjects
- (Non-representativeness of cases) since a case control study is not population ndash based study (Berkson Fallacy)
042123 28
Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Berkson Fallacy
bull As example suppose a collector has 1000 postage stamps of which 300 are pretty and 100 are rare with 30 being both pretty and rare 10 of all her stamps are rare and 10 of her pretty stamps are rare so prettiness tells nothing about rarity She puts the 370 stamps which are pretty or rare on display Just over 27 of the stamps on display are rare but still only 10 of the pretty stamps on display are rare (and 100 of the 70 not-pretty stamps on display are rare) If an observer only considers stamps on display he will observe a spurious negative relationship between prettiness and rarity as a result of the selection bias (that is not-prettiness strongly indicates rarity in the display but not in the total collection)042123 29
Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Disadvantage
bull Data Qualitybull Data with inadequate detail questionable
reliability or use a different standard to judge disease severity
bull Otherbull Capable of studying only one outcome at a
timebull Cannot calculate prevalence or incidencebull Subject to confounding factors bull Cannot prove contributory cause042123 30
COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

COHORT
042123 31
DISEASEDISEASEDISEASEDISEASEEXPOSUREEXPOSUREEXPOSUREEXPOSURE
TIMETIME
DIRECTION OF STUDYDIRECTION OF STUDY
Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Concurrent Cohort Study (Prospective)
TimePresent 2025
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
Cancer
No Cancer
Cancer
No Cancer
Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Nonconcurrent Cohort Study (Historical)
Time1985 2010
Defined Population
Fertilizer Exposure
No Fertilizer Exposure
No Cancer
Cancer
No Cancer
Cancer
ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

ANALYSIS OF COHORT STUDIES
RELATIVE RISK- measures the strength of
relationship or the association between the factorpredictors and the outcome
= Incidence Rate of outcome in EXPOSED
IR outcome in UNEXPOSED GRP
Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Cohort Study
(+) diseas
e
(-) diseas
e(+)
exposure
A B A + B
(-) exposu
re
C D C + D
A + C B + D
Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Cohort Study
Incidence Rates
bull exposed IRexposed = A divide (A + B)
bull unexposed IRunexposed = C divide (C + D)
Relative Risk (RR)
bull RR = (IRexposed) divide (IRunexposed)
bull RR = [A divide (A + B)] divide [C divide (C + D)]
Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Relative risk
bull 1 No difference in outcome between 2 groups
bull lt 1 Less risk of developing outcomebull gt 1 Higher risk of developing outcome
042123 37
bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull Low probability of selection and recall bias
bull Provide the probability of estimating the attributable risk
bull More conclusive results
bull Inefficient for rare diseases
bull Not always feasible
bull Long term follow up
bull Require a large sample size
bull High Cost
042123 38
Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Experimental
bull Therapeutic Trialbull Field Trialbull Community Trial
042123 39
Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Selected Concepts The Design of Trials
1 The control group 2 Randomization 3 Admissibility criteria4 Outcome
ascertainment5 Ethics
The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

The Need for Controls
bull Placebo effect ndash inert substances are associated with improvement
bull Hawthorne effect ndashobservation improves behavior
bull Conditions improve on their own over time
bull Use of a proper control group neutralizes all these effects
Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Element 2 Randomization
bull Groups must not differ with respect to relevant characteristics other than the exposure being studied
bull Otherwise results can be confounded by extraneous factors that lurk in the background
bull Randomization encourage the balancing of measured and unmeasured potential confounders neutralizing their effects
Randomization is the second leading principle of experimentation
Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Exp
erim
enta
l Des
ign
timeStudy begins here (baseline point)
Studypopulation
Intervention
Control
outcome
no outcome
outcome
no outcome
baselinefuture
RANDOMIZATION
Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Element 3 Admissibility Criteria
bull Restriction of subjects to those with uniform characteristics
bull Types of admissibility criteriabull Person place and time bull Prior conditions (eg having or
lacking a particular condition)bull Risk factor restriction (non-
smokers)
Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Element 4 Outcome Ascertainment
bull Outcome ascertainment validity and reproducibility
bull Blinding balances inaccuracies
bull Of course blinding is not always possible
Accurate outcome ascertainment is the third principle
Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Types
bull Single blindWhen the subjects do not know whether they belong to the treatment or the control group
bull Double blind When both the subject and the researcher has no knowledge
bull Triple blindWhen this knowledge is not known by all the three parties the subject the researcher and the statistician
042123 46
5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

5 Ethics = Equipoise
bull A condition of equipoise (balanced doubt) must exist for a human experiment can take place
bull You cannot knowingly expose a participant to known harm
bull You cannot knowingly withhold a known benefit
bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

bull Ability to assign the independent variable
bull Ability to randomize subjects to random and control
bull Ability to control confounding variable
bull Ability to replicate findings
bull Difficulty of extrapolation
bull Ethical problemsbull Non representability
of samples
042123 48
Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Clinical Trial
There are several variations on the randomized trial design that can substantially increase efficiency under the right circumstances
bull matched-pair randomizationbull time-series designbull cross-over design
Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Clinical Trial
Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Clinical Trial
How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

How do we Analyze Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For positive outcomebull RR lt 1 treatment is harmfulbull RR = 1 no significant difference bull RR gt 1 treatment is beneficial
Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Clinical Trial
Relative Risk (RR)
bull RR = (RiskTreatment) divide (RiskControl)
For negative outcomebull RR lt 1 treatment is beneficialbull RR = 1 no significant difference bull RR gt 1 treatment is harmful
Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Measures of treatment derived benefit
Absolute Risk Reduction (ARR) =Risk exposed ndash Risk unexposed
Relative Risk Reduction (RRR) =Risk exposed ndash Risk unexposed
Risk exposed
Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Basic Arithmetic
bull Suppose you have $2 and I have $1bull Absolute comparison made by
subtractionbull $2 ndash $1 = $1bull ldquoI have $1 more than yourdquo (in absolute terms)
bull Relative comparison made by divisionbull $2 divide $1 = 2 [unit-free]bull ldquoI have twice as much as yourdquo (relatively
speaking)
Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Basic Arithmetic
bull Suppose the 5-year risk of diseaseIn smokers is 2 per 100 In nonsmokers is 1 per 100
bull Absolute contrast (Risk Difference) (2 per 100) ndash (1 per 100) = 1 per 100There is one addition case per 100 exposures
bull Relative contrast (Risk Ratio) (2 per 100) divide (1 per 100) = 2The exposure doubled risk (equivalently there is a
100 increase in risk in relative terms)
Apply this scheme to risk estimates
Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

Preventive Measure
Disease
+ -
+ a b a+b
- c d c+d
a+c b+d
Disease Rate in Experimental Group
P1 = aa+c
Disease Rate in Control Group
P2 = bb+d
Protective Value = P2- P1P2
How do we analyze Prophylactic Trial
In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

In Summary
bull OBSERVATIONALbull Descriptive
bullCase ReportbullCase SeriesbullEcologicalbullCross Sectional
bull AnalyticalbullCase ControlbullCohort
bull EXPERIMENTALbull Clinical Trials
(RCT)bullTherapeutic Trial
bull Field TrialbullPrevention
bull Community TrialbullIntervention
042123 58
042123 59

042123 59