Embed Size (px)
Citation preview

Joseph S. Coselli, M.D.Joseph S. Coselli, M.D.Vice Chair, Department of Surgery
Professor, Chief, and Cullen Foundation Endowed Chair
Division of Cardiothoracic SurgeryDivision of Cardiothoracic Surgery
Baylor College of Medicine
The Houston Aortic Symposium: Frontiers in Cardiovascular DiseasesHouston, Texas • Friday, February 24, 2017Houston, Texas • Friday, February 24, 2017

Me dtronic, Inc PI ClinicalTrialsConsultant
Vascute k ConsultantVascute kTe rum o
ConsultantPI ClinicalTrialsRoy altie sCose llib ranch e d graft
W L Gore &Associate s
PI ClinicalTrialsConsultant
Bolton Me dical PI ClinicalTrialsBolton Me dical PI ClinicalTrials



• Estimated 10.4 cases per• Estimated 10.4 cases per100,000 per year Clouse et al JAMA 1998
• Without repair patients remain• Without repair patients remainat risk of aortic dissection,rupture, or bothrupture, or both Repair indicated if symptomatic
Or if a diameter-based thresholdof repair is reachedof repair is reached
> 5.5 cm in chronic dissection
> 6.0 cm for aneurysm without > 6.0 cm for aneurysm withoutaortic dissection
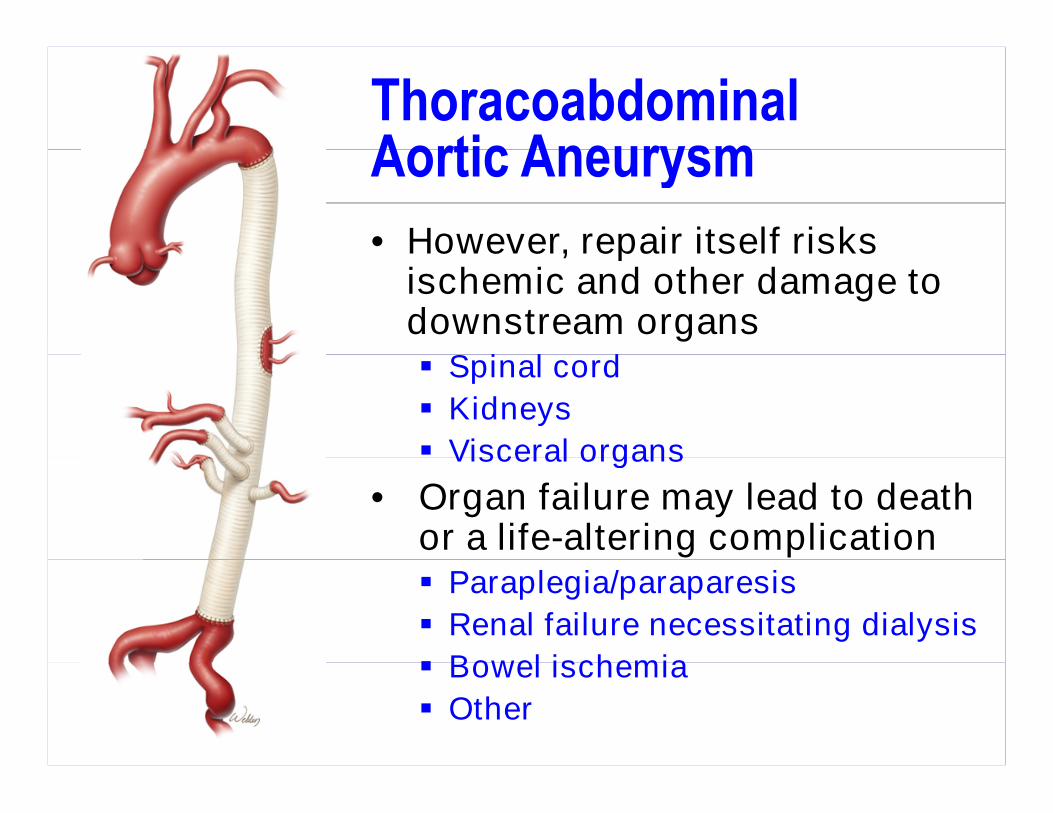
• However, repair itself risks• However, repair itself risksischemic and other damage todownstream organs Spinal cord Spinal cord
Kidneys
Visceral organs Visceral organs
• Organ failure may lead to deathor a life-altering complication Paraplegia/paraparesis
Renal failure necessitating dialysis
Bowel ischemia Bowel ischemia
Other

Thoracoabdominal Aortic Aneurysms:Survival with Non-operative Management
From Date of Diagnosis
From Date of AdmissionFrom Date of Admission
Crawford & DeNatale 1986TAAA: Observations Regarding the Natural Course of Disease

Crawford –1509 TAAA repairsSvensson et al. J Vasc Surg 1993Svensson et al. J Vasc Surg 1993
Lifetime Experience
31-year experience31-year experience1960 to 1991 n (%)
Early death 123 (8%)
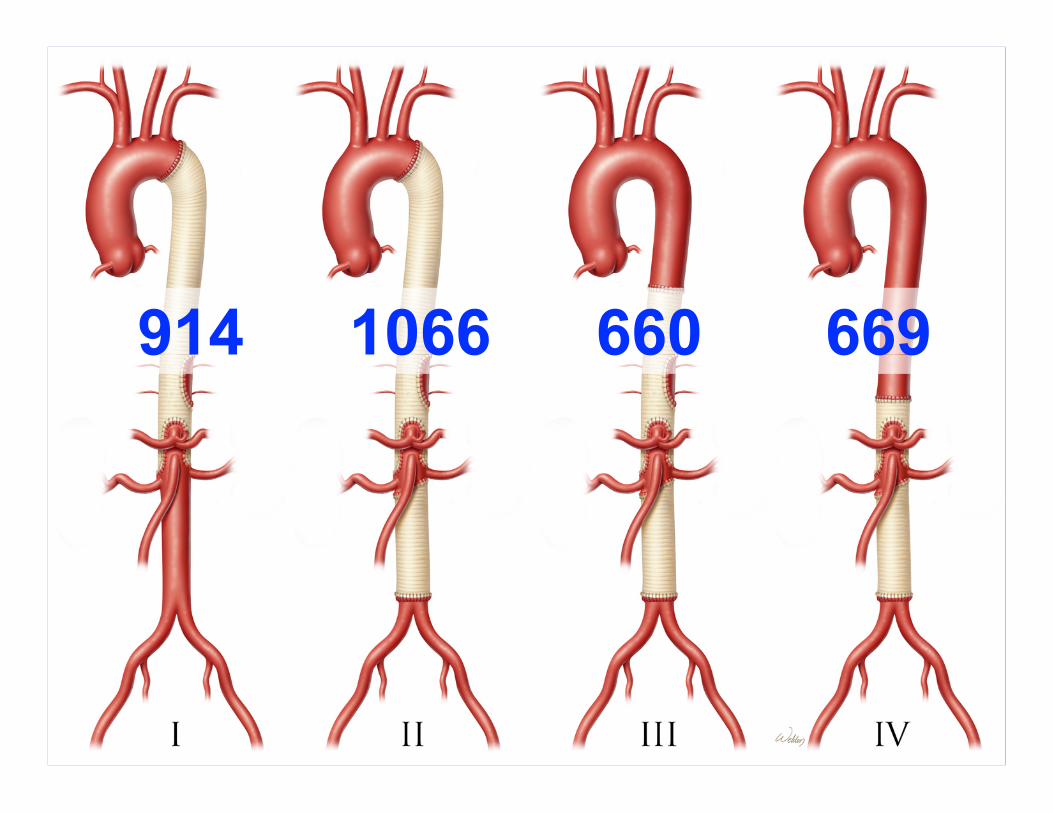
I → 378 patients
Paraplegia/-esis 234 (16%)
Renal dialysis 136 (9%)
GI complications 101 (7%)II → 442 patients
III → 343 patients
IV → 346 patients
GI complications 101 (7%)
Svensson, Crawford, Hess, Coselli, SafiJVasc S u rg1993;17:357-70.
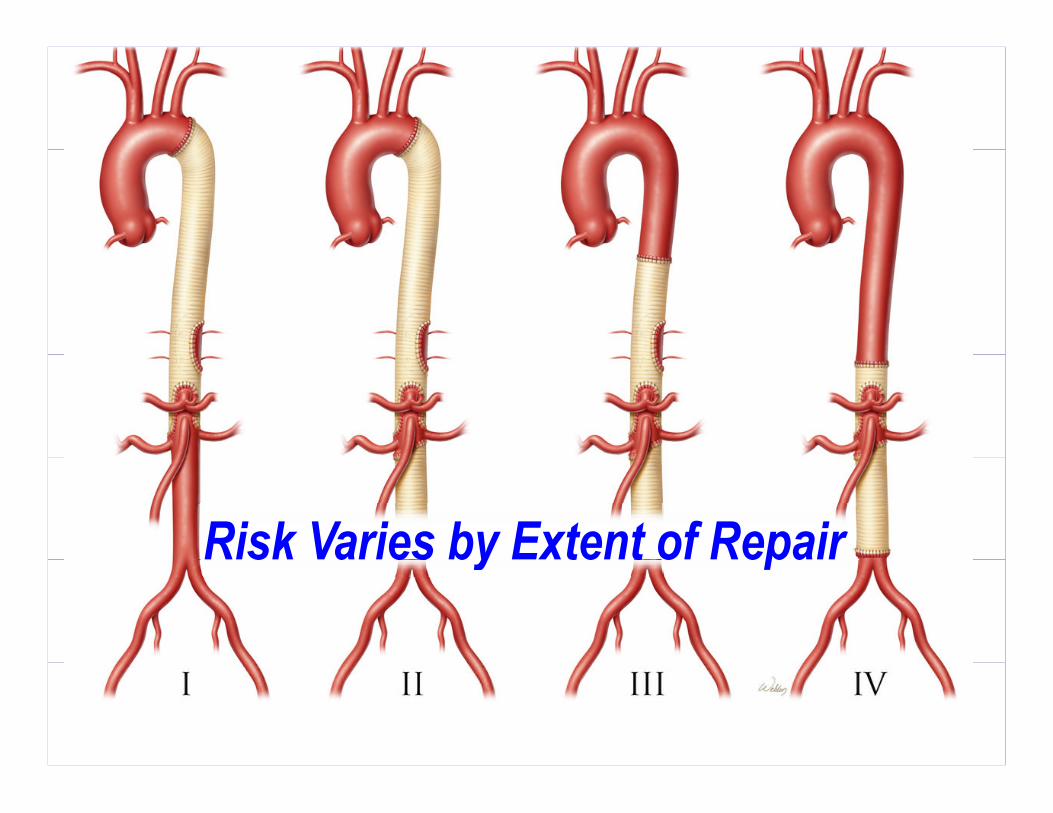
RiskVaries by ExtentofRepairRiskVaries by ExtentofRepair

All extents
• Moderate heparinization• Moderate heparinization
• Permissive mild hypothermia
• Aggressive reattachment ofsegmental arteriessegmental arteries
• Cold renal perfusion wheneverrenal ostia can be accessedrenal ostia can be accessed
• Expeditious repair
Extent I and II repairsExtent I and II repairs
• Cerebrospinal fluid drainage
• Left heart bypass• Left heart bypass
• Selective celiac/SMA perfusion



Left Heart Bypass
Left inferiorpulmonary vein
Distal descendingthoracic aorta


Reattachment of ICAs

Cold Renal Perfusion
9-Fr Pruitt catheters9-Fr Pruitt cathetersLR + 12.5 g/L Mannitol
+ 125 mg/L methylprednisolone

Selective Visceral Perfusion
9-Fr Pruitt catheters200-300 mL/min

Stent




B ranc hed grafts avoid latervisc eralpatc haneu rysmsvisc eralpatc haneu rysms
Red u c es native aortictissu e in M arfan synd rome
Usefu lifvisc eralarteries Usefu lifvisc eralarteriesare wid ely d isplac ed , su c has is c ommon in c hronicaortic d issec tion





Outcomes of 3309ThoracoabdominalOutcomes of 3309Thoracoabdominal
Aortic Aneurysm Repairs?Aortic Aneurysm Repairs
Coselli et al JTCVS 2016
95th Annual Meeting, American Association of Thoracic Surgery (AATS)95th Annual Meeting, American Association of Thoracic Surgery (AATS)Plenary Scientific Session: Abstract 1
Seattle, Washington • Monday, April 27, 2015

October 1986 to December 2014October 1986 to December 2014
Study Enrollment• Clinical research protocol• Clinical research protocol
approved by Baylor College ofMedicine in 2006Medicine in 2006
• Prospective data from 2006
• Retrospective data before 2006• Retrospective data before 2006
• Single-practice seriesCosellli et alOutcom e sof 3309 th oracoab dom inalaortic ane ury sm re p airsaortic ane ury sm re p airsJ Th orac Cardiovasc Surg2016;151:1323-38.

Coselli Experience
~30 year experience
3309 open TAAA repairsCoselli Experience
~30 year experience1986 to 2014 n (%)
Operative death 249 (7.5%)Operative death 249 (7.5%)
30-day death 159 (4.8%)
Permanent paraplegia 97 (2.9%)Permanent paraplegia 97 (2.9%)
Permanent paraparesis 81 (2.4%)
Renal failure (dialysis) 189 (5.7%)Renal failure (dialysis) 189 (5.7%)
Gastrointestinal ischemia 31 (0.9%)

3309 TAAA RepairsSelect Rates of Operative MortalitySelect Rates of Operative Mortality
Early DeathS u bgrou ps ofinterest n
Early Deathn (%) P
Patients ≤ 50 y 439 14 (3.2%) <.001
Patients > 79 y 193 37 (19.2%) <.001
Connective tissue disorder 330 10 (3.0%) .001
Chronic aortic dissection 1020 58 (5.7%) .007Chronic aortic dissection 1020 58 (5.7%) .007
Rupture 170 37 (21.8%) <.001
Prior aortic repair 858 70 (8.2%) .4Prior aortic repair 858 70 (8.2%) .4
Elective repair 2586 161 (6.2%) <.001
Urgent or emergent repair 723 88 (12.2%) <.001Urgent or emergent repair 723 88 (12.2%) <.001

Thoracoabdominal Aortic Aneurysms:Predictors: Multivariate Analysis
O perative M ortality RRR p value
Predictors: Multivariate Analysis
O perative M ortality RRR p value
Age (by inc reasingyear) 1.05 <.001
Clamp time (by inc reasingmin) 1.01 <.001Clamp time (by inc reasingmin) 1.01 <.001
Rupture 2.38 <.001
Renal insufficiency 1.98 .02Renal insufficiency 1.98 .02
Symptomatic aneurysm 1.62 .004
Endarterectomy, stent, or bypass 1.46 <.001Endarterectomy, stent, or bypass 1.46 <.001
Extent IV repair 0.50 0.001

0.17
3309 TAAA Repair: Risk of Operative Death
0.13
0.17
Age
Endarterectomy/stenting/bypass
Symptoms
0.11
0.13Symptoms
Renal insufficiency
Rupture
Symptoms + renal insufficiency
0.06
0.090.09Symptoms + renal insufficiency
0.06
Probability
Coselli et al 2016 JTCVS
10 20 30 40 50 60 70 80 90
Age at time of repair

O c tober1 9 8 6 to D ec ember2 0 1 4O c tober1 9 8 6 to D ec ember2 0 1 4
Gap of ≥ 50 Date 1 Date 2 Sequential cases without paraplegia1 Oct 1991 May 1992 69
2 May 1992 Nov 1992 512 May 1992 Nov 1992 51
3 July 1993 Apr 1995 261
4 Apr 1995 Oct 1995 92
5 Sep 1996 May 1997 1175 Sep 1996 May 1997 117
6 Apr 1998 Feb 1999 113
7 Feb 1999 May 1999 51
8 May 2000 Aug 2000 608 May 2000 Aug 2000 60
9 Dec 2000 Apr 2001 53
10 Feb 2002 July 2002 84
11 July 2002 Feb 2003 10211 July 2002 Feb 2003 102
12 Nov 2003 Apr 2004 65
13 June 2004 Dec 2004 62
14 Jan 2007 Dec 2007 9014 Jan 2007 Dec 2007 90
15 Dec 2010 May 2011 50
16 Mar 2014 Dec 2014 67

3470 Open ThoracoabdominalAortic Aneurysm RepairsAortic Aneurysm RepairsRepairs performed between 1 9 8 6 and Janu ary 2 0 1 7
P atientC harac teristic s n (%)P atientC harac teristic s n (%)Median age, y [IQR]; range 12 y to 92 67 [59-73]
Connective tissue disorder 357 (10%)
Marfan syndrome 313 (9%)
Aortic dissection involving distal aorta 1225 (35%)Aortic dissection involving distal aorta 1225 (35%)
Acute or subacute dissection 171 (5%)
Chronic dissection 1051 (30%)Chronic dissection 1051 (30%)
Symptomatic 2220 (64%)
Rupture 179 (5%)Rupture 179 (5%)

3470 Open ThoracoabdominalAortic Aneurysm Repairs
O perative D etails n (%)
Aortic Aneurysm RepairsRepairs performed between 1 9 8 6 and Janu ary 2 0 1 7
O perative D etails n (%)Elective repair 2696 (78%)
Urgent repair 463 (13%)
Emergent repair 311 (9%)
Reoperation* 848 (24%)
Reverse elephant trunk 84 (2%)
Completion elephant trunk 152 (4%)Completion elephant trunk 152 (4%)
Clamping proximal to theleft subclavian artery (LSCA)
553 (16%)left subclavian artery (LSCA)
*Prior open descending thoracic, thoracoabdominal, or abdominal aortic repair

27% 33% 20% 20%

3470 Open ThoracoabdominalAortic Aneurysm Repairs
Use ofO perative A d ju nc ts n (%)
Aortic Aneurysm RepairsRepairs performed between 1 9 8 6 and Janu ary 2 0 1 7
Use ofO perative A d ju nc ts n (%)Left heart bypass (distal aortic perfusion) 1566 (45%)
Hypothermic circulatory arrest 57 (2%)
Cerebrospinal fluid drainage 1641 (47%)
Cold renal perfusion 2048 (59%)
Selective visceral perfusion 833 (24%)

3470 Open ThoracoabdominalAortic Aneurysm Repairs
A d d itionalP roc ed u res n (%)
Aortic Aneurysm RepairsRepairs performed between 1 9 8 6 and Janu ary 2 0 1 7
A d d itionalP roc ed u res n (%)Reattachment of intercostal arteries 1669 (48%)
Management of visceral/renal arteries
Endarterectomy 904 (26%)
Stenting 287 (8%)
Bypass 913 (26%)
Use of a 4-branched TAAA graft 193 (6%)Use of a 4-branched TAAA graft 193 (6%)
Any visceral/renal artery procedure 1463 (42%)

3470 Open ThoracoabdominalAortic Aneurysm Repairs
Early O u tc omes n (%)
Aortic Aneurysm RepairsRepairs performed between 1 9 8 6 and Janu ary 2 0 1 7
Early O u tc omes n (%)Operative mortality 268 (8%)
30-day death 177 (5%)
Persistent*
Paraplegia 103 (3%)
Paraparesis 82 (2%)
Stroke 81 (2%)Stroke 81 (2%)
Renal failure necessitating dialysis 198 (6%)
Adverse event (composite endpoint) 504 (15%)Adverse event (composite endpoint) 504 (15%)
*Persisting to the time of hospital discharge or early death

3 4 7 0 TA A A RepairsEarly O u tc omes by ExtentofRepair
OperativeMortality
AdverseEvent
PersistentParaplegia
Early O u tc omes by ExtentofRepair
ExtentMortality
n (%)Eventn (%)
Paraplegian (%)
I 55 (6%) 103 (11%) 13 (2%)I(n=946)
55 (6%) 103 (11%) 13 (2%)
II(n=1130)
114 (10%) 217 (19 %) 53 (5%)(n=1130)
114 (10%) 217 (19 %) 53 (5%)
III(n=692)
58 (8%) 115 (17%) 31 (5%)
IV(n=702)
41 (6%) 69 (10%) 6 (1%)
Total 268 (8%) 504 (15%) 103 (3%)Total(n=3470)
268 (8%) 504 (15%) 103 (3%)

• Much work remains to be done• Much work remains to be done
• Contemporary TAAA open repair yields• Contemporary TAAA open repair yieldsgood-to-excellent outcomes inexperienced centersexperienced centers
• Variety of adjuncts have lowered risk in• Variety of adjuncts have lowered risk incontemporary practice
www.notretired yet.c om





























